
Abstract
Keywords
Constraint-induced movement therapy (CIMT) is a high-duration, 2- to 3-wk intervention targeting the paretic upper extremity (UE). During CIMT, paretic UE use is encouraged through restriction of the nonparetic UE using two primary strategies: (1) Distributed protocols consist of supervised paretic UE therapy sessions lasting up to 6 hr per weekday for 2 to 3 wk, and (2) traditional protocols involve forced paretic UE use during most waking hours over 2 to 3 wk. CIMT using these strategies has been shown to increase paretic UE use and movement in adults (Wolf et al., 2006) and children (Taub, Ramey, DeLuca, & Echols, 2004).
Despite its promise, concerns have been reported about CIMT’s feasibility and clinical application in adult populations. For example, in adult CIMT trials, low compliance associated with wearing the constraint for the prescribed amount of time (Blanton & Wolf, 1999; Ploughman & Corbett, 2004) and fatigue that diminished patients’ ability to complete the clinical protocol (Kaplon, Prettyman, Kushi, & Winstein, 2007; van der Lee et al., 1999) have been reported. Similar misgivings have emerged from pediatric constraint-induced movement therapy (pCIMT) studies (Glover, Mateer, Yoell, & Speed, 2002; Walker & Pink, 2009), including concerns about patient and family adherence, the human resources needed to administer pCIMT, reimbursement for treatment, and the temporal demands placed on patients’ families. However, although occupational therapists tend to focus heavily on UE functional restitution, no study has formally examined occupational therapists’ opinions of pCIMT or variations in these opinions when the duration of the UE practice components is modified. Such information is fundamental to cost-effective, appropriate pCIMT implementation.
Our overall goal was to facilitate development of feasible, well-tolerated CIMT protocols for clinical and scientific use. As a first step toward attainment of this goal, this study examined pediatric occupational therapists’ opinions of the feasibility of two published pCIMT protocols that have established efficacy but vary markedly in their treatment duration and frequency. On the basis of findings in the adult CIMT literature (Page, Levine, Sisto, Bond, & Johnston, 2002) and the speech therapy literature (Page & Wallace, 2014), we hypothesized that occupational therapists would hold more favorable opinions about the clinical feasibility and compliance associated with distributed pCIMT protocols.
Method
Participants
The population of potential respondents was identified from a public directory of licensed occupational therapists that was obtained from a state licensure board for occupational therapy in the midwestern United States. To be eligible, participants had to be a licensed occupational therapist working with pediatric clients at least 50% of the time and identified in the directory as working in one or more of the following practice categories: school systems; early intervention; health system or hospital-based outpatient facility or clinic; subacute or rehabilitation facility, unit, or clinic; acute care hospital; or private practice. Because of the implementation challenges with CIMT, it was not expected that many clinicians would be administering CIMT in their clinics. Thus, therapists were not required to have personal experience using CIMT to be eligible to participate. Applying these criteria, the study population comprised 2,723 licensed occupational therapists.
Instrument
After obtaining local ethics board approval, the instrument was sent to all population members by email; it consisted of a cover letter and a link to the online survey. The cover letter detailed the study purpose, pCIMT attributes and efficacy, required language for expedited survey studies (e.g., information about participant confidentiality), and contact information for the research team. The letter also informed recipients that response to the survey constituted informed consent. Three weeks later, a follow-up email was sent that reminded nonrespondents of the survey opportunity.
The survey, which was modified from adult CIMT opinion research (Page et al., 2002), consisted of three sections. The first section contained the following screening question: “Do you work with pediatric patients at least 50% of the time?” If participants responded no, their participation was complete; if they responded yes, they were invited to complete the rest of the survey. The second survey section consisted of seven demographic and baseline questions (e.g., age, practice setting, years of experience) and two questions about whether respondents had used a CIMT protocol with their pediatric patients and whether they had read any literature about pCIMT.
The third section began with the following instructions:
Constraint-induced movement therapy (CIMT) is a new treatment for use with children with hemiplegic cerebral palsy. The main components of CIMT include restraining the unaffected limb and using repetition and structured activity to improve the function of the affected limb. Modifications have been made to the typical CIMT protocol by requiring less time in constraint and therapy. Initial research indicates that both protocols described below improve the use and function of the affected arm. Please note: You do not have to have prior experience with CIMT to participate. We are interested in your professional opinions regarding the feasibility of implementing either of the following two protocols in your clinical environment with the children and families you see.
Immediately below these instructions, a table was presented summarizing the parameters of two contrasting pCIMT protocols. Protocol A (Taub et al., 2004) involved restraint worn 24 hr/day on the nonparetic UE and in-clinic, therapist-supervised practice sessions administered 7 days/wk for 6 hr/day over the course of 3 wk. Protocol B (Glover et al., 2002) comprised restraint on the nonparetic UE worn 2 hr/day; practice by clients of activities using the paretic UE 2 hr/day for 6 days/wk with parent or caregiver supervision; and in-clinic, therapist-supervised practice sessions 1 day/wk for 2 hr over the course of 8 wk. Using a Likert scale anchored by high concern and no concern, the first two items asked participants to indicate their level of concern about seven facets of the feasibility of Protocol A and Protocol B:
Length of time child has to wear cast on functioning arm, either 24 hr/day for 3 wk (Protocol A) or 2 hr/day for 8 wk (Protocol B)
Ability to provide occupational therapy services either 7 days/wk for 6 hr/day (Protocol A) or 1 day/wk for 2 hr (Protocol B)
Expectation of third-party reimbursement or ability to fund therapy time and materials
Safety of child when wearing constraint (full-arm fiberglass cast)
Child’s frustration level during performance of daily tasks
Child’s ability to participate in therapy 6 hr/day, 7 days/wk (Protocol A) or in caregiver-led activities 2 hr/day, 6 days/wk (Protocol B)
Caregiver’s or family’s ability to adhere to protocol.
The final two survey questions asked participants how they would rate the feasibility of Protocol A and Protocol B in their practice environment using a Likert scale ranging from high feasibility to not feasible.
Data Analyses
Quantitative data were downloaded from the online survey tool into Microsoft Excel Version 2010 (Microsoft, Inc., Seattle). Data were coded and double entered into Excel worksheets. Next, descriptive statistics were applied to analyze therapists’ opinions regarding the two CIMT protocols.
Results
Demographics
The surveys were transmitted by email to all 2,723 population members meeting study criteria, and we received 274 completed surveys (10.1% response rate). Two respondents were excluded post hoc because they did not work in a pediatric environment at least 50% of the time. Therefore, the final sample comprised 272 participants. All participants in the sample completed all survey items. Participant demographics are listed in Table 1.
Participant Demographics (N = 274)
Note. — = not applicable.
Participants were permitted to indicate more than one diagnosis.
Participants who provided two or more responses for primary setting were excluded from the total count. However, participants were allowed to indicate more than one secondary practice setting.
Survey Outcomes
The majority of respondents reported moderate or high concerns about every facet of Protocol A. As shown in Figure 1a, 75.3% held moderate or high concerns about the length of time a child would have to wear a cast, 97.8% held moderate or high concerns about their ability to provide occupational therapy services 7 days/wk, 86.0% reported moderate or high concerns about third-party reimbursement, 61.4% held moderate or high concerns about the child’s safety while wearing the cast for the time required, 78.7% had moderate or high concerns about the child’s frustration while attempting daily tasks, 94.3% reported moderate or high concerns about the child’s ability to participate in the required duration of therapy, and 87.5% had moderate or high concerns about the family’s or caregiver’s ability to fully adhere to Protocol A.
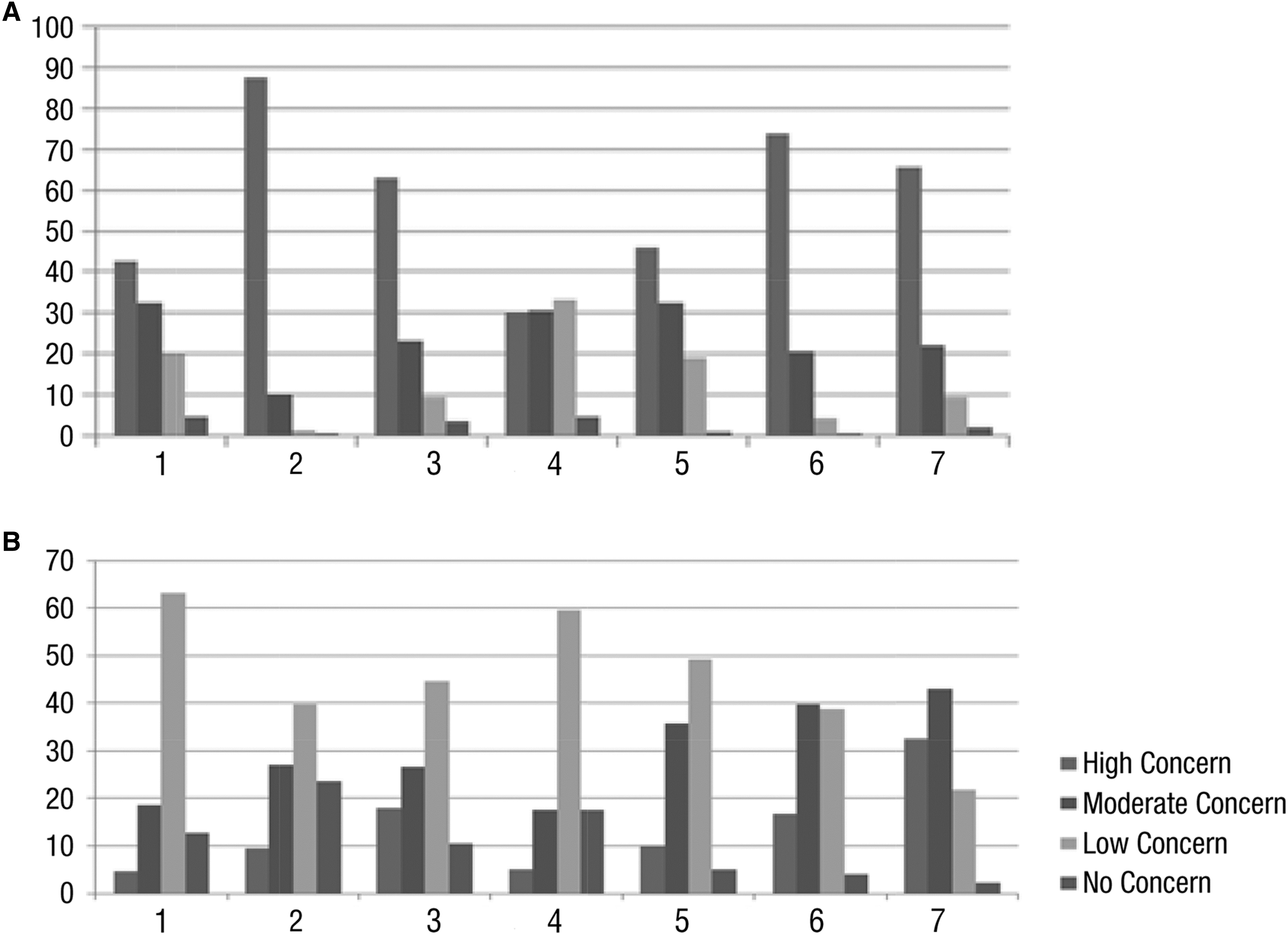
Therapists’ concerns about (A) Protocol A and (B) Protocol B.
In contrast, the only aspects of Protocol B about which a majority of respondents reported moderate to high concerns were the child’s ability to participate in 2 hr/day of therapy (56.6%) and the family’s or caregiver’s ability to fully adhere to Protocol B (75.6%; see Figure 1b). Five of Protocol B’s seven facets elicited low or no concerns.
Overall, the majority of occupational therapy therapists responded that Protocol A had no clinical feasibility (66%; Figure 2a); impressions regarding Protocol B’s feasibility were more distributed, with 51.1% reporting moderate feasibility, 17.2% reporting high feasibility, and 20.4% reporting low feasibility (Figure 2b).
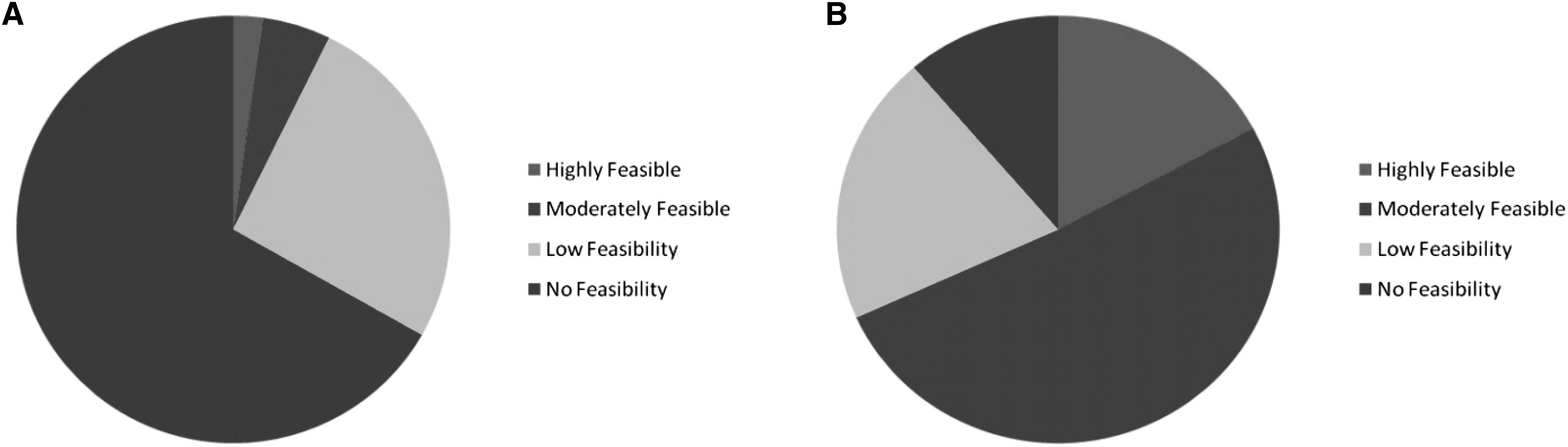
Therapists’ ratings of the feasibility of (A) Protocol A and (B) Protocol B.
We also asked participants about their familiarity with and use of pCIMT, although collecting this information was not a primary study aim. When asked whether they had read information or literature about pCIMT, 78% (n = 211) responded yes. However, when asked whether they had ever used pCIMT in any form with their patients, 69% (n = 188) reported that they had never used it.
Discussion
UE hemiparesis is a disabling impairment commonly exhibited after acquired brain injury in adult and pediatric populations. Although CIMT appears to increase paretic UE use and movement, concerns have emerged from CIMT clinical trials regarding its feasibility, impact on some participants, and participant compliance, especially among adults. Pediatrics is a traditional focus of occupational therapists, but until now no study has examined occupational therapists’ perspectives and concerns regarding pCIMT.
To accomplish the study purpose, we examined pediatric occupational therapists’ opinions of two published pCIMT protocols: (1) a higher duration pCIMT regimen requiring constant restraint of the nonparetic UE and participation in 7 hr/day treatment sessions over 3 wk (Protocol A) and (2) a lower duration regimen of UE practice sessions distributed over 8 wk (Protocol B). The majority of pediatric occupational therapists we surveyed had moderate to high concerns about every aspect of traditional pCIMT (Protocol A). The most prevalent concerns were about therapists’ ability to feasibly administer pCIMT in clinical environments and the reimbursement of services for this high-duration protocol; third-party reimbursement is a prerequisite for most rehabilitative service provision in the United States. Only 7.2% of respondents rated Protocol A as highly or moderately feasible. The child’s potential frustration with participation in daily tasks while wearing restraint for 24 hr/day was cited as a moderate or high concern among at least three-quarters of therapists. This concern is notable because pediatric UE hemiparesis is frequently accompanied by impairments in attention, frustration tolerance, and inhibition that might be exacerbated by the frustration a child could experience during Protocol A participation.
Participants’ opinions of Protocol A were unsurprising considering the marked departure from traditional rehabilitation protocols that this pCIMT version presents. Specifically, the duration that is used for Protocol A is not consistent with most inpatient or outpatient therapies or with what is reimbursed by most managed care providers. Moreover, the findings were consistent with concerns that have emerged from other reports regarding higher duration pCIMT protocols. For example, Walker and Pink (2009) reported that occupational therapists held concerns about the feasibility of pCIMT, including available resources, staff time, child participation, caregiver follow-through, and possibility for reimbursement, because of the high treatment duration. Similarly, Glover et al. (2002) found that some children exhibited discomfort and frustration when constrained and were at increased risk of falling or knocking objects over, especially when unsupervised. In a study of therapists providing CIMT to adults, 68% reported that CIMT would be very difficult or difficult to administer, that they were most concerned about clients not being able to adhere to the rigorous CIMT protocol, and that their facilities lacked the necessary resources to administer CIMT (Page et al., 2002).
In short, misgivings about the traditional form of pCIMT expressed in the current study closely resemble those reported in previous surveys regarding CIMT practice with adults and children. Collectively, these data add to a growing evidence base suggesting that a higher duration CIMT protocol, although efficacious, may result in logistical and patient-related challenges. This emerging body of evidence is notable, given that high-duration protocols similar to Protocol A are currently offered in several clinics across the United States. To address similar limitations in the adult literature, modified CIMT protocols that distribute the UE practice components over longer periods have been successfully tested in adult populations (e.g., Page, Levine, & Leonard, 2005; Page, Levine, Leonard, Szaflarski, & Kissela, 2008) with comparable efficacy to higher duration CIMT protocols (Fleet, Page, MacKay-Lyons, & Boe, 2014). Moreover, the clinical sessions associated with these protocols are being reimbursed using existing Current Procedural Terminology™ codes. Given the support for modified CIMT in the adult neurorehabilitation literature, and as an alternative to using camps and for-profit clinic models to accommodate the high number of hours associated with longer duration pCIMT iterations, it is likely that pediatric therapists could successfully integrate lower duration pCIMT protocols distributed over more weeks into routine clinical care.
Participants’ opinions of Protocol B differed markedly from their opinions of Protocol A. For example, >50% of respondents reported low or no concerns about five of the seven facets of Protocol B. Moreover, there was only one aspect of Protocol B with which >20% of participants cited high concern—that is, the caregiver’s or family’s ability to follow the protocol (32.5%). In contrast, >50% of participants reported high concerns about five of the seven facets of Protocol A. Furthermore, 17% of participants found Protocol B to be highly feasible, and 51% found it to be moderately feasible.
Although this study was the first to examine pediatric therapists’ opinions of distributed CIMT schedules, our findings are somewhat consistent with a previous survey regarding adult CIMT (Page et al., 2002) in which 83% of clients with stroke reported a preference for an alternative CIMT protocol, analogous to Protocol B, that provided the same benefits as a traditional CIMT regimen without its time-associated limitations (e.g., duration of practice sessions). The preference of therapists in our study for a more distributed pCIMT protocol also underscores a need elucidated by a Cochrane CIMT review in cerebral palsy, which suggested that the impact of varying intensities of this treatment should be examined (Hoare, Imms, Carey, & Wasiak, 2007).
Collectively, the results of this study and the promise of modified CIMT protocols in recent work (e.g., Cope, Forst, Bibis, & Liu, 2008; Page et al., 2008; Wallen, Ziviani, Herbert, Evans, & Novak, 2008) suggest several future directions. First, researchers must formally examine the efficacy of modified pCIMT protocols using larger samples and randomized controlled methods, as suggested by the authors of the Cochrane review (Hoare et al., 2007). In addition, the specific pCIMT facets about which therapists cited concerns constitute areas of potential refinement through future research efforts. For example, dosing studies were not performed leading up to the Phase 3 CIMT trial in adults with stroke (Wolf et al., 2006) or the 7 hr/day pCIMT clinical protocol that is now used in some pediatric contexts (Taub et al., 2004). On the basis of findings in modified CIMT studies conducted thus far, it is likely that some pCIMT ingredients found to be less feasible (e.g., number of hours patients have to wear the constraint) constitute potential areas for future research, including dosing studies.
Aside from the practicalities of modified pCIMT protocols, the promise of more distributed practice schedules is supported by decades of learning research (Baddeley & Longman, 1978; Bourne & Archer, 1956; Ofen-Noy, Dudai, & Karni, 2003; Wright & Sabin, 2007), and such protocols are believed to positively affect motor memory consolidation (McGaugh, 2000). Only recently has some evidence supporting this precept been produced in the pediatric literature. For instance, results from a controlled trial (DeLuca, Case-Smith, Stevenson, & Ramey, 2012) and the 6-mo follow-up (Case-Smith, DeLuca, Stevenson, & Ramey, 2012) demonstrated that pCIMT protocols administered 3 hr/day and 6 hr/day were equally efficacious in increasing paretic UE use and function in the weeks and months after treatment. Findings in the adult literature reviewed previously (e.g., Page et al., 2008) have indicated that even shorter daily durations may also be efficacious in the pediatric population. These studies constitute positive steps forward in affirming more practical, scientifically grounded, and easy-to-use clinical pCIMT protocols.
In future research, it may be beneficial to control for level of therapist experience and years as a therapist as covariates. On the one hand, more recent graduates may possess more exposure to this work and hold more positive impressions of this and other contemporary UE rehabilitation protocols given their exposure during training. On the other hand, more experienced therapists may have similar familiarity from exposure to such protocols in the literature or professional conferences, but their enthusiasm may be tempered by time in the clinic or the feasibility of pediatric and adult CIMT as reported in the literature. Investigation of differences in the opinions of more and less experienced clinicians and the rationale for these differences constitutes a possible entry point for clinician education and training.
Although this study was the largest to examine occupational therapists’ opinions on pCIMT treatment in any population, our response rate was only about 10%. This rate compares unfavorably with mailed survey response rates advocated by several authors (Blair, Czaja, & Blair, 2014). However, we do not believe that the study findings are subject to nonresponse bias, given that our findings are highly congruent with those of other studies and given that the sample size was considerable despite the relatively low response rate.
Implications for Occupational Therapy Practice
The results of this study have the following implications for occupational therapy practice:
The majority of occupational therapists prefer shorter pCIMT protocols.
Most occupational therapists have moderate to severe concern with protocols lasting multiple days per week and that have moderate to high durations of several hours per day. Most of these therapists also reported that it is unlikely to highly unlikely that such protocols would be reimbursed under existing managed care rules and that clients would fully comply with the protocol parameters.
In adult populations, modified CIMT protocols are available on an outpatient basis and are efficacious. Given this finding in adult populations, pCIMT constitutes an area ripe for future investigation.
Conclusion
Occupational therapists’ concerns about traditional, higher duration pCIMT included its exceptional human resource needs, potential for patient frustration, potential difficulty with third-party reimbursement, and doubts about caregivers’ and families’ ability to comply with its high-duration demands. In contrast, they reported low or no concerns about a distributed pCIMT protocol that has shown efficacy, with 68% finding such a regimen to be highly or moderately feasible. The findings of this study are consistent with reports of CIMT trials in adult populations and provide support for the continued refinement of modified pCIMT regimens. To increase the feasibility of CIMT for therapists, children, and families, it is vital to develop a pCIMT protocol of the lowest duration that still produces lasting changes in paretic UE use and function.
Footnotes
Acknowledgments
We gratefully acknowledge the contributions of Jane Case-Smith, who reviewed and provided comments on early versions of this article.