
Abstract
This systematic review describes the published evidence related to the effectiveness of frequency modulation (FM) devices in improving academic outcomes in children with auditory processing difficulties. The Preferred Reporting Items for Systematic Reviews and Meta-Analyses standards were used to identify articles published between January 2003 and March 2014. The Cochrane Population, Intervention, Control, Outcome, Study Design approach and the American Occupational Therapy Association process forms were used to guide the article selection and evaluation process. Of the 83 articles screened, 7 matched the systematic review inclusion criteria. Findings were consistently positive, although limitations were identified. Results of this review indicate moderate support for the use of FM devices to improve children’s ability to listen and attend in the classroom and mixed evidence to improve specific academic performance areas. FM technology should be considered for school-age children with auditory processing impairments who are receiving occupational therapy services to improve functioning in the school setting.
Most classrooms in the United States rely on oral communication for academic and social interaction; directions are read aloud, questions are answered verbally, and lectures are used to deliver educational content (Yang & Bradley, 2009). This style of instruction relies heavily on the student’s ability to decode and process auditory information efficiently and effectively. Classroom noise and poor classroom acoustics have a detrimental effect on students’ learning, specifically the ability to accurately perceive speech and attend during auditory instruction (Dockrell & Shield, 2012; Klatte, Bergström, & Lachmann, 2013).
Classroom noise can be internal (e.g., children talking, humming of projection systems, materials shifting) and external (e.g., lawn equipment, street traffic, children on the playground, students in the hallway) and may interfere with a student’s ability to process relevant aspects of acoustic signals (Shield & Dockrell, 2008). The negative effects of classroom noise are further exacerbated by reverberation, or the extended presence of a sound caused by reflection against surfaces such as desks or chairs (American Speech–Language–Hearing Association [ASHA], 2005). Longer reverberation time may lead to cognitive fatigue and greater distraction during academic instruction (Kjellberg, 2004). Although classroom noise and reverberation may affect all children, the negative outcomes appear to be particularly salient for children with learning disorders and other special needs (Bradlow, Kraus, & Hayes, 2003; Shield & Dockrell, 2008).
Auditory processing disorder (APD) is frequently diagnosed in school-age children. Its primary symptom is difficulty identifying or discriminating sounds despite having normal peripheral hearing; poor ability to understand speech in noise is the most common manifestation (Dawes & Bishop, 2009). Children with APD may have difficulty with academic tasks that involve dichotic listening (i.e., processing sounds from more than one speaker), processing rapid speech, or integrating binaural input (Johnston, John, Kreisman, Hall, & Crandell, 2009). Children with APD often have diminished skills in reading and writing and impairments in attention and concentration.
Unsurprisingly, APD is widely diagnosed in children with learning disabilities (Dawes & Bishop, 2009). Warrier, Johnson, Hayes, Nichol, and Kraus (2004) demonstrated that children with learning problems exhibit neural timing abnormalities such that their neurophysiological representation of speech sounds becomes distorted in the presence of background noise. Similarly, people with dyslexia have been shown to have temporal auditory processing and figure ground alterations (Oliveira, Murphy, & Schochat, 2013; Soares, Sanches, Alves, Carvallo, & Cárnio, 2013), as well as asynchrony between auditory and visual processing speeds (Sela, 2014). Reading and spelling tasks in particular have been shown to be influenced by classroom babble in children receiving special education services (Shield & Dockrell, 2008). Other school-age populations may also present with auditory processing problems and secondarily be influenced negatively by background noise and reverberation; these populations include children with attention deficit hyperactivity disorder (ADHD), autism spectrum disorder (ASD), or other disorders with known impairments in central auditory processing (Bailey, 2012; Chermak, Hall, & Musiek, 1999; Edgar et al., 2014; Rance, Saunders, Carew, Johansson, & Tan, 2014; Tierney, Kurtz, & Souders, 2012).
Although guidelines for classroom acoustics have been established by ASHA (2005), classrooms in the United States rarely meet these criteria (Acoustical Society of America, 2014). This finding suggests that other strategies may need to be used for children to perform optimally in the classroom environment. Environmentally based strategies focused on modifying acoustics are a feasible and potentially high-impact option and an area of expertise of occupational therapy practitioners. Frequency modulation (FM) devices are one possible option to implement these modifications.
Frequency modulation is a wireless sound transmission method used to optimize the listening environment by improving the signal-to-noise ratio and minimizing the effects of reverberation. FM devices consist of two main parts, a radio transmitter and a radio receiver. Speech signals are detected by a lapel microphone worn by the speaker or teacher, then transmitted by radio waves to a receiver worn by the listener (personal system) or a loudspeaker placed close to the listener (classroom system). The FM unit allows the speaker’s voice to predominate while reducing background noise (Chisolm, Noe, McArdle, & Abrams, 2007).
Personal FM devices are well documented as an evidence-based strategy for people who have hearing impairments or difficulty hearing over distance (Fitzpatrick et al., 2010; Schafer, Huynh, Romine, & Jimenez, 2013; Schafer & Thibodeau, 2006; Thibodeau, 2010). Recent literature has also begun to show the benefits of FM devices for children without hearing impairments but with other auditory processing concerns. School-based occupational therapy practitioners are often called on to collaborate with educational teams regarding strategies to improve academic performance for students with various sensory processing problems. Therefore, practitioners may be involved in clinical decisions related to implementation of FM devices for students on their caseload. The purpose of this systematic review was to determine whether FM devices are associated with improved academic outcomes in children and adolescents ages 5–21 yr with auditory processing concerns but without primary hearing impairments to support evidence-based practice.
Method
Before initiating a literature search, we established a protocol using the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (Moher, Liberati, Tetzlaff, & Altman, 2009). We strategically searched four databases—PubMed, Web of Science, CINAHL, and the Cochrane Database of Systematic Reviews—and did a secondary selection of articles based on a review of references in relevant articles. Following PRISMA guidelines, we reviewed the titles of all articles for appropriateness, then reviewed relevant abstracts and appraised full-text articles. Selection was based on preestablished inclusion and exclusion criteria. Two authors independently reviewed abstracts and full-text articles and generated concordance rates. A third author was available to settle disagreements; any discrepancies were discussed and resolved through consensus.
The search strategy was initiated using the following Population, Intervention, Control, Outcome, Study Design (PICOS) question: Are FM assistive listening devices effective in improving academic outcomes in school-age children with auditory processing disorders but without a primary hearing impairment? Search terms included assistive listening device, FM device, and FM system. Only articles published between January 2003 and March 2014 were considered; nonelectronic sources of literature and articles written in a language other than English were not considered. Specific search limits for each database are presented in Table 1.
Database Search Limits
The population was defined as children and adolescents ages 5–21 with a diagnosed or suspected auditory processing disorder but without primary hearing loss. Children with disorders such as ASD, ADHD, and learning disabilities, which are known to have accompanying auditory processing deficits, were included. Children with cochlear implants, hearing aids, or other types of corrective hearing devices were not considered.
To meet the inclusion criteria for intervention, each publication needed to report on the use of a personal FM device or classroom FM system lasting a total of 4 wk or more. Studies using infrared sound field systems were not included, nor were studies in which the assistive listening device used was not clearly described as using FM. No comparative intervention or population was required.
The studies included were required to assess academic outcomes including (but not limited to) improved sound discrimination in the classroom, reading scores, general academic performance, phonological awareness, speech perception, and attention. All publications were required to include a description of assessments used to measure outcomes and statistical procedures used for determining changes in performance.
Standards established by the National Guideline Clearinghouse and accepted by the American Occupational Therapy Association (AOTA, 2014b) for assessing levels of evidence were used to evaluate the study design quality of the articles reviewed (Figure 1). Only studies with a Level III rating or above were included. Therefore, studies that used a case-series design or a poor-quality cohort or case-control design or that consisted of expert opinion without explicit critical appraisal were excluded.
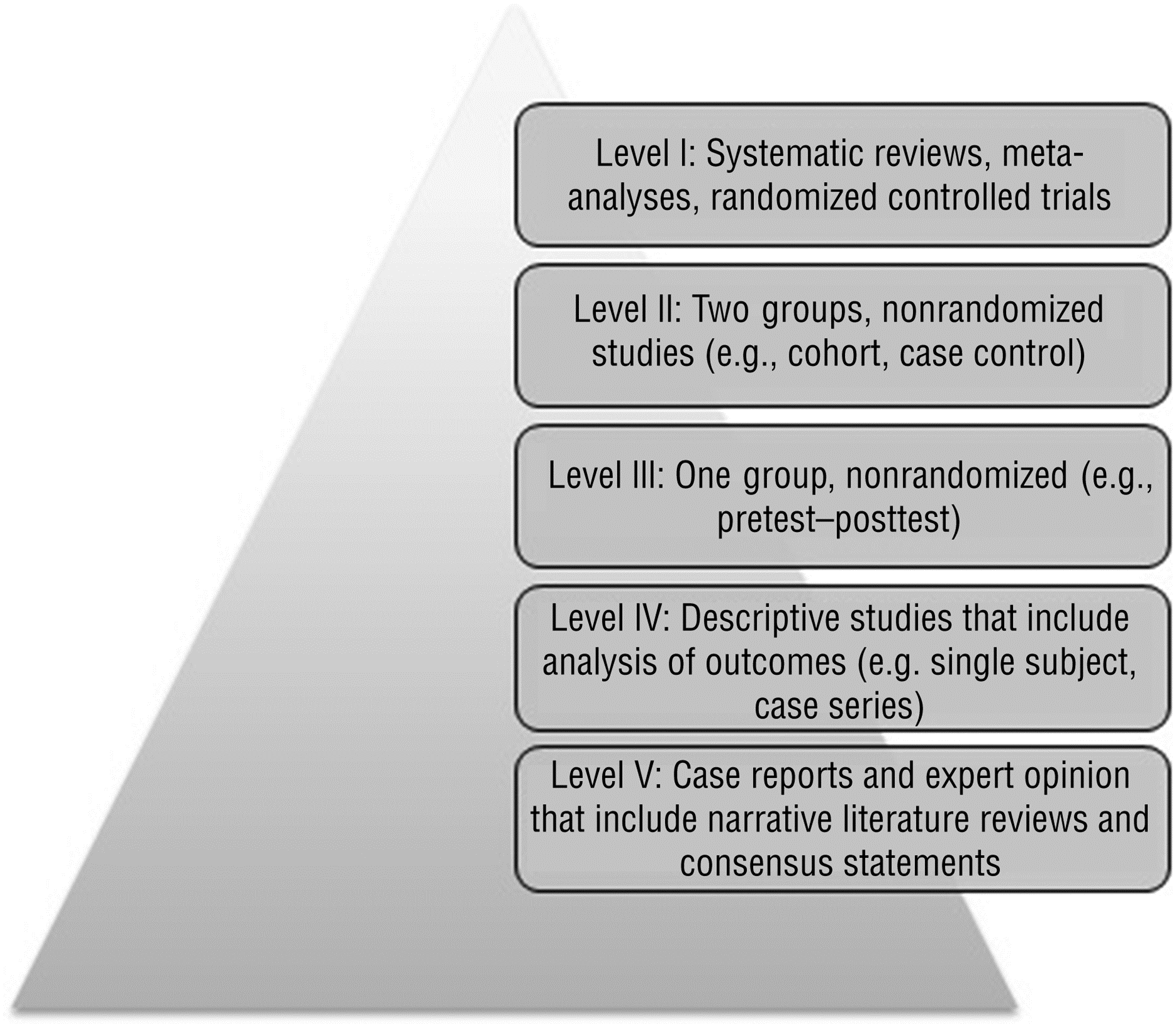
Levels of evidence (AOTA, 2014b).
Results
Initial search strategies of the four databases yielded 257 articles, with an additional 15 records identified through reference review and supplemental searches on key authors (Figure 2). After duplicates were removed and titles were screened for relevance, a total of 83 articles remained. Within the screened publications, randomized and nonrandomized experimental studies were represented, as were descriptive studies, narrative reviews, systematic reviews, and case reports. Of the 83 abstracts screened, 71 were excluded with reasons, whereas 7 appeared to match the PICOS inclusion criteria. An additional 5 articles did not have enough information in the abstract to justify exclusion, received the designation maybe, and were included in the next phase of the review.
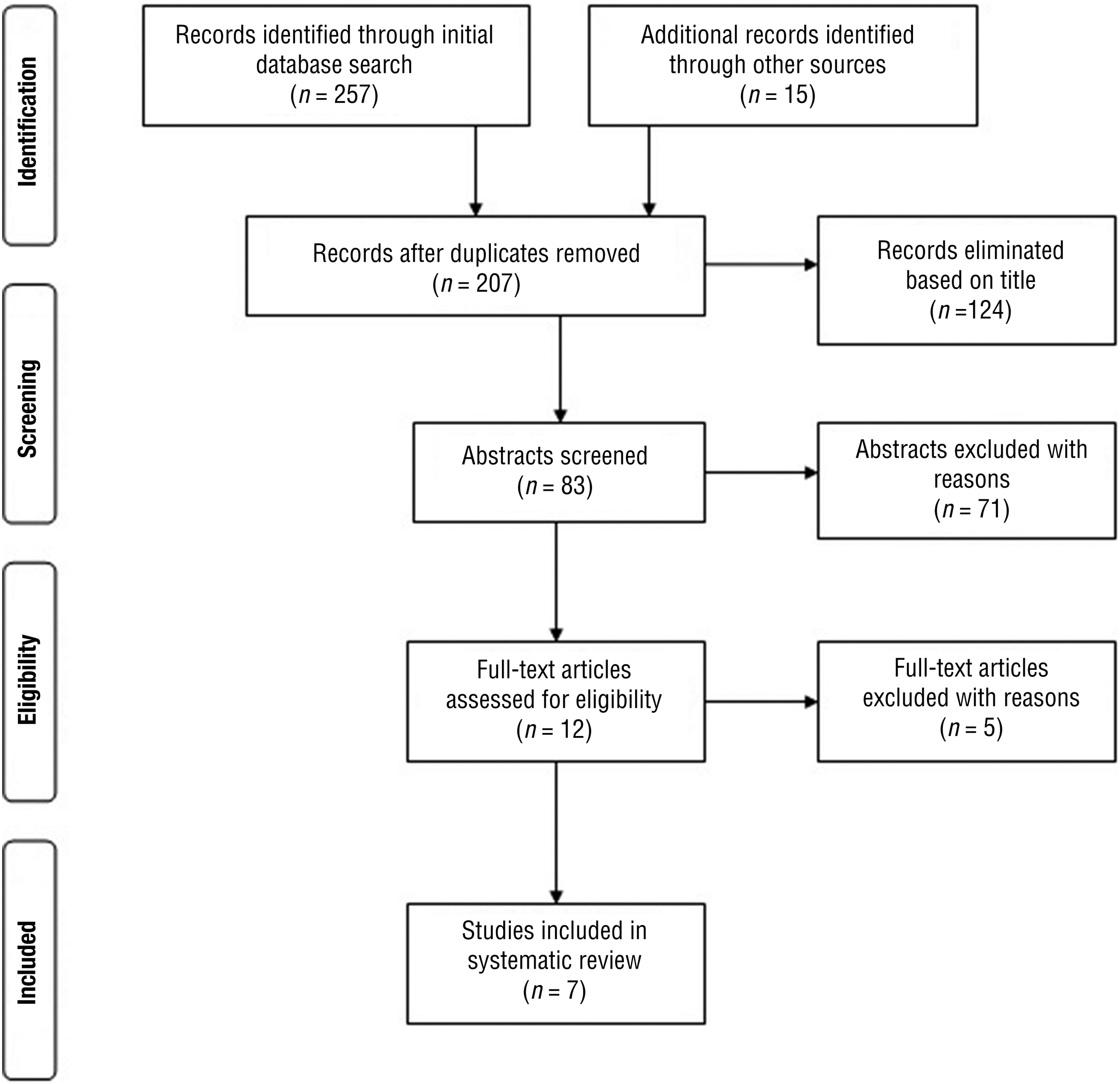
Preferred Reporting Items for Systematic Reviews and Meta-Analyses flow diagram of published literature search.
Interrater agreement was 91.6% for inclusion and exclusion decisions and 84.3% for level of evidence ratings. A comprehensive list of the reviewed abstracts with rationale for exclusion is presented in Supplemental Table 1 (available online at http://otjournal.net; navigate to this article, and click on “Supplemental”). On the basis of the established exclusion criteria, 63 studies were omitted because of population criteria (88.7%), 51 studies because of intervention criteria (71.8%), 39 studies because they did not use required outcome measures (54.9%), and 29 studies because they did not fit the criteria for study design (40.8%).
A total of 12 articles were assessed for eligibility through a full-text review. Each article was read by two of the three authors and evaluated using the preestablished inclusion and exclusion criteria and level of evidence rating. Interrater agreement was 100% for inclusion and exclusion criteria and 83% for evidence level ratings. Five articles did not meet inclusion criteria and were therefore excluded (Supplemental Table 2; available online at http://otjournal.net). Seven studies met all inclusion criteria: 1 article ranked at Level I (Sharma, Purdy, & Kelly, 2012), 4 ranked at level II (Hornickel, Zecker, Bradlow, & Kraus, 2012; Johnston et al., 2009; Schafer, Mathews, et al., 2013; Umat, Mukari, Ezan, & Din, 2011), and 2 ranked at Level III (Rance, Corben, Du Bourg, King, & Delatycki, 2010; Rance et al., 2014). Of the 7 included articles, all examined use of personal FM devices, and none reported outcomes for a classroom FM system. Supplemental Table 3 (available online at http://otjournal.net) identifies the characteristics of all seven articles meeting inclusion criteria, including all PICOS components.
Study Design
Of the 7 articles identified for an in-depth review, the study designs included 1 randomized controlled trial (RCT; Sharma et al., 2012) and 6 quasi-experimental studies. Of the 6 quasi-experimental studies, 2 used a within-groups (ABBA) design (Rance et al., 2010, 2014), 2 used a group comparison design with a typically developing control population (Johnston et al., 2009; Schafer, Mathews, et al., 2013), and 2 used a group comparison design with a diagnostic control group (Hornickel et al., 2012; Umat et al., 2011).
Statistical procedures used within these articles included paired t tests and analysis of variance models. Most articles reviewed used a p value of ≤.05 to identify statistically significant associations. However, Hornickel and colleagues (2012) set their α level at .10 for one-tailed t tests and at .05 for two-tailed t tests, whereas Sharma and colleagues (2012) established their α level at .01 for all analysis of variance models.
Population
A total of 211 participants were enrolled in the included studies, 187 with auditory processing impairments and 24 control participants without auditory processing impairments. Of the 187 children with auditory processing impairments, 118 had a primary diagnosis of APD, 38 were diagnosed with dyslexia, 17 had ASD, 10 were diagnosed with Friedreich’s ataxia, and 4 had ADHD. Approximately 68% of participants were male. The age range for most studies was 7–15 yr; however, 1 study included participants up to age 42 yr (Rance et al., 2010) and was included in the review because 50% of the participants were of school age. Two studies included only children from private specialty schools, which accounted for 93 of the 211 participants (44%).
Intervention
All 7 of the included articles reported using Phonak (Zurich, Switzerland) personal FM devices. In all 7 studies, FM receivers were fitted to participants binaurally. One study (Umat et al., 2011) also included a subgroup of children who wore unilateral receivers. The intensity and duration of intervention varied greatly among studies. The timeframe of the FM intervention varied from 4 wk to 8 mo. Four studies reported a short duration (4–6 wk; Rance et al., 2010, 2014; Schafer, Mathews, et al., 2013; Sharma et al., 2012), 1 an intermediate duration (12 wk; Umat et al., 2011), and 2 a longer duration (5–8 mo; Hornickel et al., 2012; Johnston et al., 2009).
All 7 studies recommended daily use of the FM devices during the school week. Three articles reported intervention lasting 4–6 hr/day (Hornickel et al., 2012; Rance et al., 2014; Umat et al., 2011), 1 article reported intervention lasting 1–5 hr per day (Rance et al., 2010), 1 article reported intervention lasting 45 min/day during reading and math only (Schafer, Mathews, et al., 2013), 1 article reported use of intervention only during lectures (no time amount specified; Johnston et al., 2009), and 1 article did not specify how many hours per day the FM device was worn (Sharma et al., 2012). All 7 studies indicated that the device was worn at school; only 1 specified that home use was encouraged but not directly measured (Johnston et al., 2009).
In all 7 studies, research staff fitted the FM devices and set volume levels. Although not consistently reported, research staff appeared to originate from a variety of academic departments, including otolaryngology, audiology, speech–language pathology, psychology, neurology, and speech and hearing sciences. Regular monitoring of the FM devices (e.g., checking volume levels, battery life, and general use) throughout the intervention was not always reported. Two studies noted daily monitoring by research staff (Schafer, Mathews, et al., 2013; Umat et al., 2011), and 1 study reported weekly monitoring by research staff (Hornickel et al., 2012). Only 1 study indicated that the students were trained to monitor their own devices and change batteries independently (Johnston et al., 2009).
Outcomes
Because children with auditory processing impairments are likely to have difficulty registering, recognizing, and processing verbal instructions in an academic setting, the primary outcome measure used in FM intervention studies is often speech perception and recognition. In this review, 6 of the 7 studies measured speech perception or recognition, or both, with 5 of the 6 studies demonstrating statistically significant improvements in these areas with FM use (Table 2). Tools used to measure speech perception and recognition included the Hearing in Noise Test, the Modified Bamford–Kowal–Bench Speech-in-Noise Test, the Abbreviated Profile of Hearing Aid Benefit, and auditory brainstem responses to speech. Changes in classroom behaviors associated with listening and attention were also measured in 3 studies (Johnston et al., 2009; Rance et al., 2014; Schafer, Mathews, et al., 2013), with improvements seen in all 3 under FM intervention conditions. Measures of classroom behaviors included direct observation of on-task versus off-task behavior and the Listening Inventory for Education, a teacher-report questionnaire.
Summary of Outcomes, by Evidence Level
Note. ↑ = statistically significant improvements in identified area; → = no change identified in this area; NA = not applicable (item not measured in study).
Academic performance was measured in 5 of the 7 studies considered in this review (Hornickel et al., 2012; Johnston et al., 2009; Schafer, Mathews, et al., 2013; Sharma et al., 2012; Umat et al., 2011). Positive changes were noted with FM use in the areas of reading (measured by the Woodcock–Johnson III); sentence recall (measured by the Clinical Evaluation of Language Fundamentals); nonword spelling and syllable segmentation (measured by the Queensland University Inventory of Literacy); and working memory, best learning, and retention of information (measured by the Rey Auditory Verbal Learning Test). These measures are all objective performance measures. No changes in academic performance were found when a parent- or teacher-report tool, the Screening Instruments For Targeting Educational Risk, was used to identify changes in academic performance after FM use (Johnston et al., 2009; Schafer, Mathews, et al., 2013).
Discussion
This systematic review found moderate evidence to suggest that personal FM devices for children with auditory processing impairments may be effective in improving academic outcomes related to speech perception and recognition in the classroom and classroom listening behaviors. On the basis of AOTA’s (2014a) Guidelines for Systematic Reviews, moderate evidence indicates that “one RCT or two or more studies with lower levels of evidence” (p. 4) demonstrate significant and positive outcomes for the intervention. Six of the studies included in the review had outcomes related to speech perception and recognition. Five studies (3 Level II and 2 Level III) demonstrated significant improvements, and 1 (Level I) study demonstrated no changes in speech perception and recognition. Three of the studies (2 Level II and 1 Level III) measured classroom listening behaviors; all 3 studies reported significant improvements when using the personal FM devices. Finally, 3 of 5 studies (1 Level I and 2 Level II) demonstrated significant improvements in specific areas of academic performance, whereas 2 studies demonstrated no improvements. Although support for improvements was found in the majority of the studies, the evidence is considered mixed for improving academic performance.
The lack of homogeneity in the measurement tools used and in the diagnostic conditions examined limits the ability to make in-depth comparisons or to summarize the findings across all studies. However, when objective, performance-based tools were used, findings consistently indicated improvements with use of FM devices across diagnostic groups. Therefore, on the basis of the results of the systematic review, occupational therapy practitioners may consider FM devices to be one of the possible classroom modifications suggested to educational teams to improve academic outcomes for students with auditory processing difficulties.
Several limitations found in the studies reviewed limit the strength of the current knowledge base. First, many of the studies included in the review were of inadequate sample size to allow for multivariate statistical analysis of data and therefore used multiple t test comparisons. Use of multiple t tests, particularly without any type of statistical adjustment, increases the risk of Type I error (i.e., the likelihood of finding significance by chance). Second, the lack of randomization in 6 of 7 articles reviewed suggests that selection bias may also have been a factor, along with the potential for performance or detection bias because no studies reported use of blinding techniques (see Supplemental Table 4 for risk of bias ratings; available online at http://otjournal.net).
Limitations and Future Research
This review was limited to articles published in English and available in full text. Furthermore, we excluded studies with children who did not have auditory processing impairments but may also have benefited from the use of FM systems, such as children who are learning in English-speaking classrooms but speak English as a second language. Because the current review focused on the use of FM technology, articles were excluded that used other types of assistive listening technology, such as classroom infrared systems (also known as sound-field systems). Literature is available on the use of these systems and should be considered in future reviews.
Outcomes of this systematic review highlight the need for additional high-quality, highly powered studies on the use of FM technology to improve academic outcomes in children with auditory processing disorders and other neurodevelopmental disorders that have associated auditory processing impairments. The rigor of future studies can be improved by increasing sample size, including both diagnostic and nondiagnostic control groups; randomizing group assignment and concealing group allocation (to decrease selection bias); blinding participants and personnel (to decrease performance bias); using objective performance-based measures that have established reliability and validity; monitoring and recording the intensity and duration of device use; and using multivariate statistics for data analysis to reduce the likelihood of Type I statistical errors. Because none of the studies reviewed included children below age 7 yr, future studies (including future reviews) may consider including preschool and early school-age children because these ages are of primary importance for the development of foundational language, social, and reading abilities.
Implications for Occupational Therapy Practice
Almost a quarter of the occupational therapy workforce works in schools or with school-age children (AOTA, 2010). Part of the role of school-based occupational therapy practitioners is to support academic outcomes and social participation by promoting occupation within the classroom and other school environments. This systematic review has the following implications for occupational therapy practice:
FM technology is an evidence-based strategy to help children function in their school setting. FM technology may be useful in enhancing speech perception and recognition in school-based settings and may help improve classroom behaviors. Initial support is also provided for improvements in specific academic performance areas.
Because FM devices in the reviewed studies were set up and monitored by research staff from a variety of academic departments, it is not clear which clinical professionals would take the lead on FM system implementation in school settings. Likely the lead professionals will vary depending on the school and school system in question. Occupational therapy practitioners’ role may vary accordingly, with responsibilities ranging from simply suggesting device use at team meetings to taking the lead on purchasing FM systems for children within the school system and setting up plans for teacher and educator trainings and programs for device monitoring and technical support.
Whatever their role, occupational therapy practitioners work as part of a larger team of school-based professionals. Interdisciplinary collaboration is encouraged among occupational therapy practitioners, audiologists, speech–language pathologists, teachers, and other team members in implementing modifications such as FM technology to improve the learning environment.
Supplemental Materials
Supplementary material for Systematic Review of the Effectiveness of Frequency Modulation Devices in Improving Academic Outcomes in Children With Auditory Processing Difficulties
Supplementary material, sj-pdf-1-aot-10.5014_ajot.2016.016832.pdf for Systematic Review of the Effectiveness of Frequency Modulation Devices in Improving Academic Outcomes in Children With Auditory Processing Difficulties by Stacey Reynolds, Heather Miller Kuhaneck and Beth Pfeiffer in The American Journal of Occupational Therapy
Supplementary material for Systematic Review of the Effectiveness of Frequency Modulation Devices in Improving Academic Outcomes in Children With Auditory Processing Difficulties
Supplementary material, sj-pdf-2-aot-10.5014_ajot.2016.016832.pdf for Systematic Review of the Effectiveness of Frequency Modulation Devices in Improving Academic Outcomes in Children With Auditory Processing Difficulties by Stacey Reynolds, Heather Miller Kuhaneck and Beth Pfeiffer in The American Journal of Occupational Therapy
Footnotes
Acknowledgments
The authors acknowledge the Pediatric Research Interest and Mentoring Group (PRIME) for their collaboration and idea generation, which provided a launching point for this project. We also acknowledge the AOTA for supporting the PRIME and pediatric research in the profession.
*
Indicates studies that were systematically reviewed for this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.