
Abstract
Purpose.
To investigate the correlation between periventricular leukomalacia (PVL) and retinopathy of prematurity (ROP), which are complications of perinatal and postnatal hypoxic-ischemic insults in premature infants.
Methods
In this retrospective case series study, from 1996 to 2008, after excluding cases with follow-up of less than 3 months, we reviewed medical charts of babies who had gestational age (GA) less than 30 weeks or birthweight (BW) less than 2000 g. A total of 195 patients were diagnosed with ROP and/or PVL and were enrolled in this analysis. We investigated the correlation between ROP and PVL with Pearson chi-square test and evaluated BW, GA, and Apgar scores at 1 minute and 5 minutes after birth as risk factors by independent t test.
Results
There were no significant differences in the prevalence of PVL between patients who received ROP treatment and those who did not receive ROP treatment. The BW was significantly lower in patients with PVL than in patients without PVL. Gestational age, BW, and Apgar scores significantly differed between patients who did and did not receive retinal treatment for ROP.
Conclusions
Periventricular leukomalacia did not increase the severity of ROP or requirement of ROP treatment. Birthweight, GA, and Apgar scores were the principal factors that determined the necessity of ROP treatment.
Introduction
Tremendous progress in perinatal and neonatal treatment has led to a clear increase in the survival of premature low birthweight (BW) infants (1). However, several studies confirm that these children are at increased risk for major and minor neurologic disabilities, poor cognitive performance, and visual impairment (1), all of which may affect their future quality of life. The main causes of visual impairment in premature children are retinopathy of prematurity (ROP) and periventricular leukomalacia (PVL) (2).
Retinopathy of prematurity is a major cause of blindness in children in the developing and developed world despite the availability of surgical treatment for the late stages of the disease. Retinopathy of prematurity is associated with excessive oxygen use (6), as initially observed in the nursery and then confirmed in animal studies (3-5). It is a biphasic disease that is characterized by an initial phase of blood vessel loss and a second phase of vessel proliferation (7). Premature infants have incompletely vascularized retinas with a peripheral avascular zone. At a postmenstrual age of approximately 30–32 weeks, the absence of an adequate vascular system leads to tissue hypoxia. Subsequently, hypoxia-induced retinal neovascularization develops at the junction between the vascularized and avascular zones of the retina. Over time, this pathologic growth of blood vessels causes fibrous scarring that extends from the retina to the vitreous gel and the lens. Retraction of this scar tissue can separate the retina from the retinal pigment epithelium, resulting in retinal detachment and often, in blindness (7). The eye and the developing visual system are both susceptible to hypoxic-ischemic damage in utero (8). In many countries, PVL is a major cause of visual impairment in premature children (2). Periventricular leukomalacia is a condition in which hypoxic ischaemic damage of the periventricular white matter causes diverse clinical manifestations, including spastic diplegia (9, 10), mental retardation (10, 11), and visual impairments (12, 13). The combination of reduced systemic blood pressure and impaired vascular autoregulation of cerebral circulation decreases perfusion in the premature infant brain. Lowered cerebral perfusion contributes to defective tissue oxygenation, resulting in hypoxic-ischemic brain injury (8).
Periventricular leukomalacia and ROP are thought to result from ischemia and are common complications of preterm birth. Therefore, we wondered whether the interruption of blood flow to the immature brain, which contributes to hypoxic-ischemic brain injury, might also decrease the immature retinal perfusion because of a common source of blood supply and cause retinal ischemia; this may deteriorate the hypoxic status and increase the severity of ROP after use of oxygen. Few studies have investigated the aforementioned correlation. Ng et al (14) reported that cerebral hypoperfusion, the basis of PVL, might exacerbate the already ischemic retina and be a major contributing factor to severe acute ROP in some infants. However, no study has investigated whether the occurrence of PVL influences the severity of ROP. Therefore, the purpose of the present study was to investigate whether the insult mediating cerebral ischaemia increases the necessity of ROP treatment.
Methods
A computer search was performed for patients evaluated at the Ophthalmology Department, Kaohsiung Chang Gung Memorial Hospital, Taiwan, from 1996 to 2008 and coded as retrolental fibroplasia or periventricular leukomalacia. We reviewed the medical records for babies who were born at a gestational age (GA) of less than 30 weeks or had a BW less than 2000 g. Only 388 cases were screened because of missing or wrong codes in medical charts. This review was approved by the Chang Gung Memorial Hospital Institutional Review Board (IRB no. 97-1690B).
Neonatal fundus examinations and cranial transfontanelle scans were performed by experienced ophthalmologists and pediatricians, respectively. The stage of ROP was determined according to the guidelines of the International Classification of Retinopathy of Prematurity (ICROP; 2005 revision) (15). In this classification, stage 0 is defined as immature blood vessels that end without any demarcation. Stage 1 has a flat demarcation line between the vascular and avascular retina. Stage 2 has an elevated demarcation line. Stage 3 has an elevated demarcation line with neovascularization along the ridge. Stage 4 is partial retinal detachment. Stage 5 is total retinal detachment (16). Retinopathy of prematurity staging was determined at the initial screening, before therapy, and at the end of the study. The indication for ROP treatment was determined according to the Cryotherapy for ROP (CRYO-ROP) trial as threshold disease (17) from 1996 to 2003 and the Early Treatment for Retinopathy of Prematurity (ET-ROP) as type 1 ROP (18) since 2003. Eyes that received ROP treatment were classified as severe ROP, and eyes with spontaneously regressed ROP were classified as mild ROP.
Neonatal standard sagittal and coronal transfontanelle ultrasonograms were obtained at least 2 times in the first month of life according to the health status of these patients, and PVL(+) was defined as the formation of cysts in periventricular areas on coronal and sagittal views. Neonates who did not have any abnormal findings in the brain were included in the PVL(–) group.
Birth parameters, including GA, BW, gender, and Apgar scores at 1 and 5 minutes after birth, were assessed for all babies. We analyzed the correlation between PVL and ROP by Pearson chi-square test and compared the groups in terms of GA, BW, and Apgar score at 1 and 5 minutes after birth by independent t test to determine the role of PVL and the risk factors that necessitated ROP treatment in ROP patients. All p values were 2-sided, and a p value of less than 0.05 was considered statistically significant.
Results
Among all 388 screened cases, 80 patients received treatment for ROP, which is a treatment rate of 20.6%. After excluding those who had follow-ups of less than 3 months, 195 babies were included in the study to retrospectively examine the factors that correlated with ROP and PVL. Of the 195 patients, 78 (40%) were female and 117 (60%) were male. The mean follow-up period was 31 months (range 3 to 142 months). The averages of BW, GA, and Apgar score at 1 and 5 minutes after birth in the study population were 1165.56±386.7 g (range 530 to 2540 g), 28.38±2.73 weeks (range 25 to 38 weeks), 4.43±2.03 (range 0 to 9), and 6.64±1.71 (range 0 to 10), respectively.
PVL in premature babies cannot predict the necessity for ROP treatment
Of these 195 babies, 33 were diagnosed with PVL(+) and 162 with PVL(–); 80 babies received standard ROP treatment, and 115 were considered to have mild ROP. The prevalence of patients receiving ROP treatment (severe ROP) was 45.5% in the PVL(+) group and 40.1% in the PVL(–) group. The prevalence of PVL was 18.8% in the severe ROP group and 15.7% in the mild ROP group. Using Pearson chi-square test, we did not find a significant difference in the prevalence of ROP treatment and PVL (Tab. I).
CORRELATION BETWEEN ROP TREATMENT AND PVL
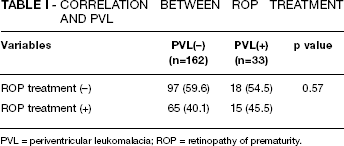
PVL = periventricular leukomalacia; ROP = retinopathy of prematurity.
Low BW is a risk factor for PVL
The averages of BW, GA, and Apgar score at 1 and 5 minutes after birth were 1058.52±290.73 g, 27.70 ± 2.48 weeks, 4.60±2.11, and 6.73±1.31 in the PVL(+) group, respectively, and 1187.36±400.71 g, 28.52 ± 2.77 weeks, 4.40±2.02, and 6.62±1.78 in the PVL(–) group, respectively. An independent t test showed that BW was significantly lower in patients with PVL than in those without PVL (p=0.035). No differences were noted in gender, GA, and Apgar scores at 1 and 5 minutes after birth between patients with or without PVL (Tab. II).
DIFFERENCES IN BW, GA, AND APGAR SCORES AFTER 1 min AND 5 min BETWEEN PATIENTS WITH AND WITHOUT PVL
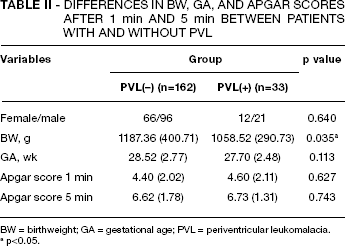
BW = birthweight; GA = gestational age; PVL = periventricular leukomalacia.
p<0.05.
BW, GA, and Apgar scores are risk factors for needing ROP treatment
To determine differences between patients who did and did not receive treatment for ROP, we measured GA, BW, and Apgar scores at 1 and 5 minutes after birth. The average GA, BW, and Apgar scores at 1 and 5 minutes after birth were 26.96±2.34 weeks, 984±270.72 g, 3.99±1.96, and 6.22±1.70 in patients requiring ROP treatment, respectively, and 29.28±2.48 weeks, 1273.93±385.47 g, 4.71±2.03, and 6.91±1.67 in patients who did not require ROP treatment, respectively. Compared with patients who did not receive ROP treatment, those who received ROP treatment had significantly lower GA (p<0.001), BW (p<0.001), and Apgar scores at 1 minute (p=0.017) and 5 minutes (p=0.007) after birth (Tab. III). No significant differences were found in the gender distribution between the 2 groups (Tab. III).
DIFFERENCES IN BW, GA, AND APGAR SCORES AFTER 1 min AND 5 min BETWEEN ROP PATIENTS WITH AND WITHOUT TREATMENT
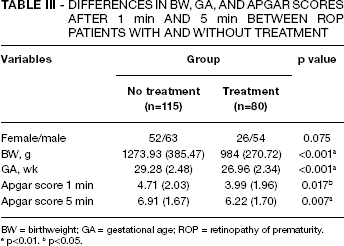
BW = birthweight; GA = gestational age; ROP = retinopathy of prematurity.
p<0.01.
p<0.05.
Discussion
Hypoxia-ischemia results in selective damage to various brain structures, depending on the developmental stage at which it occurs (19). Hypoxia-ischemia in the preterm human (gestational week 23-32) damages developing subcortical white matter, a condition known as PVL (20). Developmental immaturity of the cerebral vasculature is believed to account for this characteristic subcortical distribution (21), and cortical visual impairments are particularly common in infants with PVL. In 2005, Murata et al (22) reported potential antenatal and perinatal factors in the development of cystic PVL. They found that Apgar score, cord length, and indomethacin and magnesium sulphate use, but not BW (p=0.15), were associated with PVL. In our study, we only noted a significant difference in BW between the PVL(+) and PVL(–) groups. However, in our data, Apgar score did not increase the risk of PVL occurrence. We attribute this difference to the inclusion of only patients with lower BW (<1200 g) and Apgar scores (<5) in the analysis of Murata et al.
Retinopathy of prematurity is one of the leading causes of vision loss in children (23). With the rising rates of prematurity and improved survival, it is necessary to identify risk factors, perform ROP screening, and provide timely treatment and long-term follow-up for these babies. Currently, oxygen overuse and low GA/BW of the baby are major risk factors for ROP (24, 25). According to a joint statement from the American Academy of Ophthalmology and the American Association of Pediatric Ophthalmology and Strabismus (26), current screening guidelines recommend dilated examination by indirect ophthalmoscopy for all premature infants with a GA of less than 30 weeks or BW of less than 1500–2000 g. Therefore, we enrolled patients whose BW was less than 2000 g or whose GA was less than 30 weeks. In our study, a higher prevalence of ROP treatment (20.4%) was noted, probably because of missing or incorrect coding in the old medical category system, which resulted in mislaying some patients when the initial raw data were retrieved from this old system. Interestingly, other than BW and GA, we observed significant differences in Apgar score at 1 and 5 minutes after birth between patients who did and did not receive treatment for ROP. These findings suggested that in addition to BW and GA, Apgar scores at 1 and 5 minutes after birth are risk factors that increase the probability of requiring ROP treatment.
Both PVL and ROP are believed to result from ischemia insults. Ng et al (14) reported that PVL correlated with the severity of acute ROP because cerebral and ocular circulation arises from the internal carotid artery; therefore, an episode that causes hypoperfusion of the cerebral circulation that is sufficient to result in cerebral ischemia can also limit previously compromised ocular blood flow. In contrast, our results indicate that having PVL did not affect the severity of ROP. Our findings might have differed due to our larger patient sample size or because the pathophysiology of ROP and PVL differ: ROP is the result of postnatal post-hyperoxia-induced relative hypoxia, and PVL is caused by antenatal or perinatal hypoperfusion. Even though severe preceding cerebral hypoperfusion results in PVL, the disruption of blood flow is insufficient to affect the hypoxic status in retinas. Additionally, retinal circulation may be derived from not only the brain arteries but also other collaterals, which are assumed to decrease hypoxic retinal damage. Therefore, PVL does not correlate with the severity of ROP or the necessity of treatment for ROP.
The limitations of our study include the small sample size in the PVL(+) group, which led to no significant relevance of PVL in the severity of ROP. In addition, relatively short follow-up times resulted in inadequate data for evaluating retinal function. Further electrophysiologic studies are required to determine the final outcome of visual function in these patients.