
Abstract
Purpose
To compare demographic and clinical data, systemic disease association, visual prognosis, and complications found in childhood and adult onset of intermediate uveitis (IU).
Methods
Retrospective cohort study of 287 patients with IU: 122 (42.5%) children at onset (<16 years), 165 (57.5%) adults. The data were entered on a computer-based standardized data entry form for statistical analysis. Student t test was used regarding differences in means. To assess significance of differences in proportions, we used the χ 2 test, but when the population in the subgroup was ≤5 patients, we used the Fisher exact test (p<0.05 were deemed to be statistically significant and as reported were not corrected for multiple testing and so should be viewed as nominal).
Results
A total of 61% of childhood-onset cases occurred in boys (44% in the adult group), while adult onset was more common in women (56% vs 39%) (p = 0.004, odds ratio [OR] 2.06). Regardless of the onset age, IU was frequently bilateral and idiopathic. The most frequent complication was cystoid macular edema (27.5%, p = 0.469, OR 0.85), which was also the most frequent cause of visual loss. Optic disc edema was more prevalent in children (15.5% vs 9.2%; p = 0.027, OR 1.81), ocular hypertension in adults (15.6% vs 7.5%, p = 0.007, OR 0.44). A total of 25 patients had non-idiopathic IU. A total of 14 patients had multiple sclerosis.
Conclusions
Intermediate uveitis was mostly idiopathic and bilateral in both groups. Visual prognosis was good and it was not age-related. Childhood onset was more frequent in boys, adult onset in women. Endocrinal factors could be involved.
Introduction
Intermediate uveitis (IU) is a chronic intraocular inflammation primarily involving pars plana ciliaris, peripheral retina, and anterior vitreous (1). Whereas IU affects children and young adults more frequently, it is observed in all ages (2, 3). The onset is typically in childhood or early adolescence. It seems that the onset age of ocular inflammation has a bimodal pattern, with a first peak between 5 and 15 years and a second peak between 25 and 35 years (4). Onset after 40 years is uncommon. Giles (2) described a more aggressive anterior segment inflammation in children with IU than in adults. Giles (2) and Hogan et al (5) reported the most prevalent occurrence of severe posterior complications such as papillitis and neovascularization in children with IU vs in adults. Concerning visual acuity (VA), the data of Malinowski et al (6) suggest that age was not significantly related to final visual outcome, while Guest et al (7) reported a worse VA both at initial diagnosis and at follow-up in childhood-onset IU vs cases presenting in adulthood.
In the literature, most retrospective studies of IU reported data involving both children and adults.
The aim of our study was to compare childhood-onset and adult-onset IU in a large cohort of patients referred to a tertiary eye center in Italy with particular regards to the clinical features, associated systemic diseases, complications, and visual prognosis.
Methods
We reviewed all clinical charts of patients referred to a tertiary referral uveitis center from January 1, 1995, to December 31, 2010.
The inclusion criterion was diagnosis of IU according to the diagnostic criteria of International Uveitis Study Group (8). A retrospective and descriptive study of 287 patients (520 eyes) was performed. Of these, 122 patients (226 eyes) were children at onset, aged 16 years or under (minimum 3–maximum 16 years), and 165 patients (294 eyes) were adults, aged 17 years or older at onset (minimum 17–maximum 72 years).
After the initial presentation, 104 children (191 eyes) and 125 adults (227 eyes) underwent successive examinations and had available follow-up data. Media follow-up duration was respectively 40.5 months (range 1–239) and 31.7 months (range 1–171).
For each patient, we considered the age at first visit, the age at onset of uveitis, the laterality of uveitis, the ocular complications, the visual loss, and any possible associated systemic disease.
At the first visit, patients, or their parents, filled out a detailed questionnaire concerning the history and peculiar features of the present illness and, furthermore, any other possible ocular or systemic disease. The patients were examined at each visit by the same physician. Each patient underwent a full ophthalmologic examination that included VA check using Snellen charts or E charts, slit-lamp biomicroscopy, fundus examination using bilateral indirect ophthalmoscope, and, in cooperative patients, intraocular pressure (IOP) measurement using the Goldmann applanation tonometer. Each patient underwent routine laboratory examinations including a complete blood cell count, erythrocyte sedimentation rate, urinalysis, and serum biochemical analysis. According to the clinical history and the characteristics of uveitis, other serologic and immunologic tests (e.g., autoantibodies, serum angiotensin-converting enzyme, antibodies to infective agents, human leukocyte antigen I and II class typing) and instrumental examinations (e.g., fluorescein and indocyanine green angiography, ultrasonography, Stratus optical coherence tomography [OCT scanner with version 3.0 software; Carl Zeiss Meditec, Oberkochen, Germany], electrophysiologic tests, and visual fields tests) were performed. If necessary, imaging studies, such as chest radiography, joint radiography, or computed tomography or magnetic resonance imaging study of head and orbits, were requested. Association of IU with systemic diseases was confirmed by clinical features, laboratory and diagnostic tests, and specialized consultations (“tailored approach procedure”). When a specific cause of ocular inflammation was not found, we defined idiopathic IU. Complications included edema of optic disk, cataract, ocular hypertension, retinoschisis, cystoid macular edema (CME), vitreous bleeding, and retinal detachment. Cataract was defined as the presence of 1+ nuclear sclerosis or 1+ cortical change or trace posterior subcapsular changes. Ocular hypertension was defined as IOP elevation >21 mm Hg and hypotony was defined as an IOP <5 mm Hg. Cystoid macular edema was defined as the presence of macular thickening with or without cyst formation that was seen by clinical examination. Only patients with fundus suspicious characteristics of CME and drastic visual loss underwent Stratus OCT. After diagnosis of CME with OCT, the patients underwent the examination every 3 months, to assess the response to treatment. Patients with visual loss despite therapy underwent OCT before 3 months. Central foveal thickness to establish the diagnosis of macular edema was defined as ≥252 microns. Band keratopathy and posterior synechiae were diagnosed by slit-lamp examination. We investigated the topical and systemic therapy and ocular surgery performed during the follow-up. The study was undertaken in accordance with the tenets of the declaration of Helsinki and institutional review board approval was obtained. Descriptive and frequency distributions were obtained overall and separately for children (patients ≤16 years) and adults (patients >16 years). Data on patients were entered on a computer-based standardized data entry form for statistical analysis. Student t test was used regarding differences in means. To assess significance of differences in proportions we used the χ2 test when the population in the subgroup was >5 patients and Fisher exact test when each subgroup involved 5 or fewer patients. p Values <0.05 were deemed to be statistically significant and as reported were not corrected for multiple testing and so should be viewed as nominal.
Results
Among 4,882 patients with uveitis seen at our Ocular Immunovirology Service from January 1, 1995, to December 31, 2010, 287 patients had IU (6%). Of these, 43% (122 patients) showed IU onset during pediatric age (≤ 16 yeas) and the other 57% (165 patients) showed IU onset in adulthood (>16 years).
The demographic and clinical characteristics of the study population are shown in Table I. The distribution of the age at presentation by decile is shown in Figure 1.
Characteristics of Patients with Intermediate Uveitis a
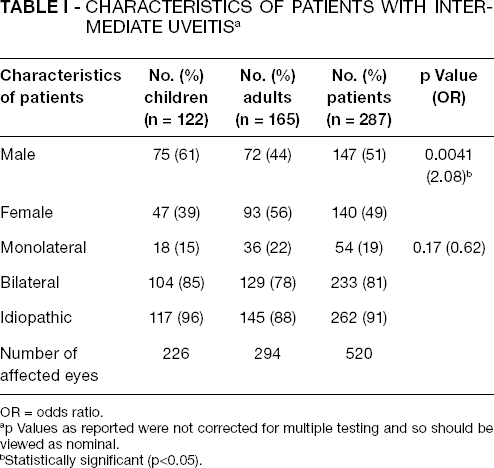
OR = odds ratio.
p Values as reported were not corrected for multiple testing and so should be viewed as nominal.
Statistically significant (p<0.05).
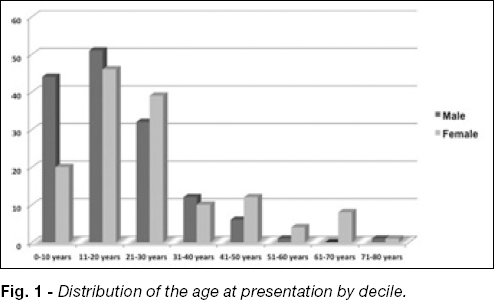
Distribution of the age at presentation by decile.
Our study group included 147 male (51.2%) and 140 female (48.8%) patients. The sex ratio in each group is different, because childhood IU was more prevalent in male patients (61% vs 44%), while adult IU was more prevalent in female patients (56% vs 39%) (p = 0.004; odds ratio [OR] 2.06).
Among children, the mean age at onset of uveitis symptoms was 10.1 years (range 3–16 years; ±3.6), the mean age at time of the diagnosis of uveitis was 10.6 years (range 3–16 years; ±3.6), and the mean age at our first visit was 12.5 years (range 5–49; ±7.0). Among adults, the mean age was, respectively, 30.7 years (range 17–72; ± 13.4), 31.4 years (range 17–72; ±13.5), and 33.2 years (range 17–72; ±13.8).
Signs and symptoms at uveitis onset are reported in Table II: decreased VA (44% of children and 62% of adult IU) and floaters (30% of children and 51% of adult IU) were most reported in both groups (overall, respectively, 55% and 42%). A total of 27.9% of childhood IU was diagnosed during routine ophthalmologic examinations, while in adults this happened only in 6.7% of cases (p = 0.021; OR 2.18). Overall, incidental diagnosis occurs in 16% of IU cases.
Signs and Symptoms at Presentation a
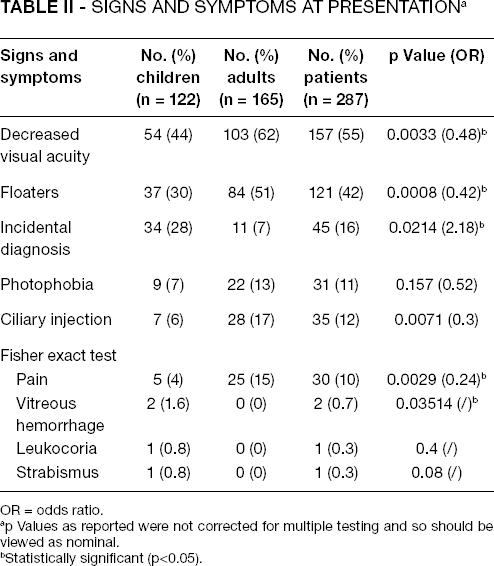
OR = odds ratio.
p Values as reported were not corrected for multiple testing and so should be viewed as nominal.
Statistically significant (p<0.05).
We described snowbanking in 426 of 520 eyes with IU (81.9%): 188 in children (83.2% of 226 eyes with childhood uveitis) and 238 in adults (80.9% of 294 eyes with adult uveitis).
Cystoid macular edema (25.7% in children vs 28.9% in adults) and cataract (19.9% vs 27.2%) were the most common complications associated with IU found in these patients (respectively, overall 27.5% and 24%), described in Table III. Comparing the prevalence of optic disc edema and ocular hypertension among children and adults, we found significantly more frequently optic disc edema in childhood IU (15.5% in children vs 9.2% in adults, p = 0.027; OR 1.81) and ocular hypertension in adult IU (15.6% in adults vs 7.5% in children, p = 0.007; OR 0.44). Overall, we found optic disc edema in 11.9% of IU and ocular hypertension in 12.1%. At onset of ocular inflammation, we found vitreous hemorrhage only among 4 of 226 pediatric eyes (1.6%) vs 0 of 165 adult eyes (p = 0.035; OR infinity). We did not find any case of anterior synechiae or decreased VA due to amblyopia.
Complications a
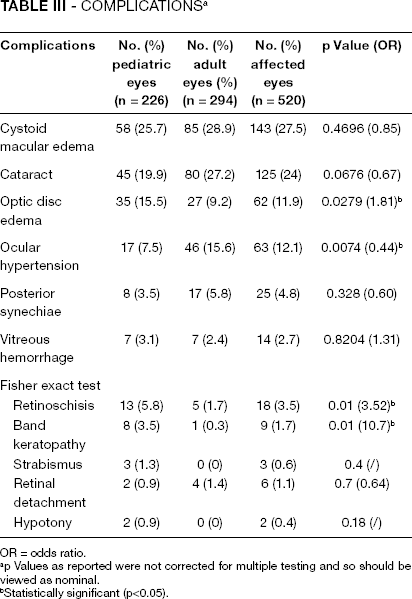
OR = odds ratio.
p Values as reported were not corrected for multiple testing and so should be viewed as nominal.
Statistically significant (p<0.05).
Visual acuity at initial examination and during follow-up did not differ with age. A total of 418 eyes underwent successive examinations: 191 with childhood IU and 227 with adult IU. Visual prognosis was good in both groups. In the childhood-onset group, at the end of the study (mean follow-up 40.5 months), 92.2% of eyes maintained a VA >20/50 (vs 90.6% at the beginning), 3.14% of eyes had a VA 20/50 or worse but better than 20/200 (vs 4.19% at the beginning), whereas a lower percentage had a VA ≤20/200 (4.7% vs 5.2% at the beginning). In the adult-onset patients, at the end of the study (mean follow-up 31.7 months), 89.9% of eyes maintained a VA >20/50 as at the beginning of the follow-up, 6.6% of eyes had a VA 20/50 or worse but better than 20/200 (vs 7.1% at the beginning), and 3.5% had a VA ≤20/200 (vs 3.1% at the beginning). Common causes for developing low vision were CME and cataract in both groups. Among children, 3 of 8 eyes with 20/200 or worse vision at the end of the study had CME. Other reasons for reduced vision were cataract (3 eyes), vitreous hemorrhage (3 eyes), retinal detachment (1 eye), and pathological myopia (1 eye). Among adults, 8 of 8 eyes with 20/50 or worse vision at the end of the study had CME. Other reasons for reduced vision in these 8 eyes were cataract in 4, age-related macular degeneration in 1, and ischemic papilledema in 1. These were not related to IU.
A total of 262 patients (91.3%) were classified as having idiopathic IU or pars planitis. None of these developed autoimmune systemic disease during the follow-up. The remaining 25 patients, 5 children and 20 adults, had non-idiopathic IU (as shown in Tab. IV). Fourteen patients—3 children (2.6% of pediatric group), 1 female and 2 male, and 11 adults (6.7% of adult group), 8 female and 3 male—had multiple sclerosis (MS). In this group, mean age at IU onset was 35.1 ± 17.5 years, while mean age at MS diagnosis was 27.2 ± 12.6 years. The ocular inflammation appeared simultaneously with the demyelinating disease in 7 patients (50%), while 5 patients (36%) developed intraocular inflammation after MS diagnosis. In 2 patients, a 16-year-old boy and a 41-year-old woman, ocular inflammation anticipated demyelinating disease (it appeared 10 years and 2 years before MS, respectively).
Etiology of Intermediate Uveitis
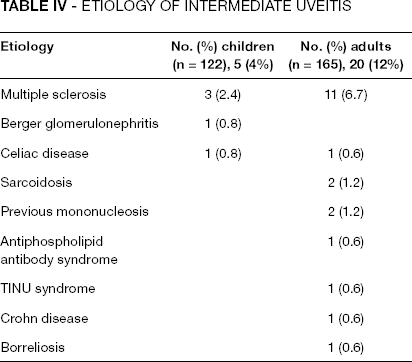
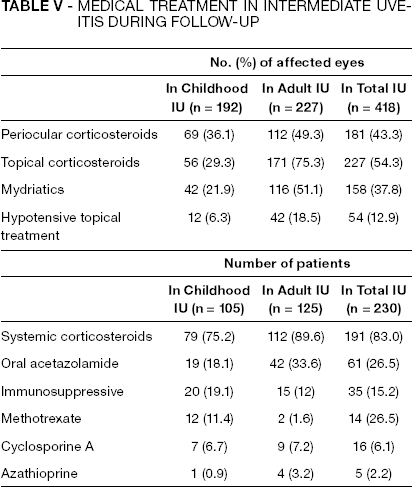
In the pediatric group, other cases of systemic illness with immunologic pathogenesis were Berger glomerulonephritis (1 case) and celiac disease (1 case). Among adults, there were 2 cases of sarcoidosis, 1 case of TINU syndrome, 1 case of Crohn disease, 1 case of antiphospholipid antibody syndrome, 1 case of borreliosis, and 2 cases of previous mononucleosis. The treatments used during follow-up are shown in Table V. Local treatments included periocular corticosteroids (181 eyes), topical corticosteroids (227 eyes), mydriatics (158 eyes), and hypotensive topical treatment (54 eyes), whereas systemic therapies included corticosteroids (191 patients), oral acetazolamide (61 patients), methotrexate (16 patients), cyclosporine A (16 patients), and azathioprine (1 patient). Most patients in both groups received oral steroids and only 20 children and 15 adults were treated with oral immunosuppressive drugs. Vitreoretinal surgery was necessary in 4 adults (4 eyes) in whom retinal detachment occurred. In the pediatric group, only 2 patients (2 eyes) required vitrectomy and cerclage.
Medical Treatment in Intermediate Uveitis During Follow-Up
Discussion
In this study, IU accounts for 6% of all uveitis cases observed in our center over a period of 16 years, in agreement with the previous reports (6, 9–11), and children represented 43% of the cases. In our study group, a higher percentage of patients were male (51.2%), confirming the data reported by Guest et al (7), in which the prevalence of males in all study groups is 65.4%. The higher percentage of males in the pediatric population has also been reported by other studies (12, 13). In contrast with the results of Guest et al, which describe a similar sex ratio in each group, in our study in childhood IU the percentage of males is significantly higher (61% vs 44%), while among adults, IU is more prevalent in women (56% vs 39%); this difference is statistically significant (p = 0.004). Estrogens in adult women may enhance inflammation, as in other autoimmune diseases. It is commonly observed that autoimmune disease develops in females more frequently than in than males, seemingly dependent not on chromosomal sexual factors, but on hormonal factors. Sex hormones (estrogens and androgens) influence both cell-mediated immunity and humoral immunity in different ways. Molecular mechanisms by which sex hormones modulate inflammation are not understood: proinflammatory effect has been proposed as well as anti-inflammatory activity. The hypothalamus-hypophysis-gonadal axis may be involved in autoimmune disorders (16) and the influence of hormones on inflammatory cytokines in autoimmune disorders and particularly uveitis remains to be investigated further. The relationship between IU and autoimmune diseases suggests in the heterogeneous pathogenesis of this ocular inflammation also an autoimmune pathogenesis. Histologic studies on eyes with idiopathic IU demonstrated that snowbanks, pars plana exudates, are fibroglial and vascular preretinal membranes including T-cell helper CD4+ (14, 15). T-cells are in fact the predominant cell type in the vitreous in IU and in particular 30%–90% of those cells are CD4+ (17). Intermediate uveitis was more frequently bilateral and idiopathic in the 2 subgroups, similarly to previous studies (7, 9, 18).
The most frequent associated disease was MS, observed in 14 patients (4.9% of all patients with IU). Data on association between IU and MS range between 3% and 27% in adults or in the whole population (13, 19, 20). Some studies suggested that the probability of MS or optic neuritis in patients with IU may be 20% higher for a period of 5 years after the uveitis onset, whereas IU did not always forecast MS because ocular inflammation could appear many years after neurologic symptoms (20). In our study, MS was diagnosed after the ocular inflammation in 2 cases, a 6-year-old boy and a 41-year-old woman, with a time from IU onset to the diagnosis of demyelinating disease of 10 years and 2 years, respectively. Malinowski et al (6) reported that 15% of patients with IU developed MS 5 years before the ocular inflammation; therefore, we underline the importance of neurologic monitoring during follow-up also in pediatric IU. An incidental diagnosis was more frequent in children than in adults (p = 0.02). This is probably due to lack of communication skills in children and also because of the frequently asymptomatic onset in childhood IU (21). The most important complication and the main cause of visual loss was CME both in children and the adult-onset group. In our study, CME was diagnosed in 27.5% of all eyes with IU, in agreement with previous studies, in which CME occurs in 28% to 52% (2, 21–23). From the data of our study, there is a statistically significant difference between the incidence of optic edema in childhood IU (15.5%) and in adult IU (9.7%) (p = 0.003). Hogan et al (24) reported posterior complications more frequently in children than in adults with intraocular inflammation. We underline that low-grade edema could only be detected by fluorescein angiography (FA) and only a small percentage of patients underwent FA; therefore, we found optic disc complications less frequently (15.5%) than reported by de Boer et al (71%) (22). Ocular hypertension occurs more frequently in adults than in children (p = 0.004).
Fourteen of the eyes with IU (2.7%) had no traumatic vitreous bleeding. At onset, this complication appeared only in children, in 4 eyes (1.77% of eyes with childhood IU). Lauer et al (25) reported more prevalent vitreous bleeding among children with IU due to the difficulties of children in communicating symptoms and also due to a more aggressive inflammation response with the consequent formation of fundus neovascularization. Concerning visual prognosis, there is no consensus in the literature about onset age correlation. Visual prognosis in patients with IU was good in our study and we did not observe significant differences between children and adults in the long-term visual outcome. Hogan et al (24) and Guest et al (7) noted an inverse correlation between age and severity of ocular inflammation, with greater severity in children. Dinning (26) showed data suggesting that older patients have more severe disease complicated by CME. In our study, long-term VA in childhood-onset and adult-onset disease was good and we observed no significant differences. In both groups, CME was the main cause of loss of VA, in accordance with the literature (2, 22).