
Abstract
Purpose
To determine the effect of intravitreal bevacizumab on retrobulbar blood flow of patients with diabetic macular edema.
Methods
Peak systolic velocity, end-diastolic velocity, resistance, and pulsatility indices of central retinal artery (CRA), nasal posterior ciliary artery (NPCA), temporal posterior ciliary artery (TPCA), and ophthalmic artery (OA) were assessed by color Doppler ultrasonography in injected and uninjected eyes of 37 patients at baseline and at day 1 and day 7 after the injection.
Results
At day 1 after the injection, peak systolic and end diastolic velocities of the CRA and NPCA in the injected eyes and peak systolic velocity of NPCA in the uninjected eyes decreased significantly (p<0.05, p = 0.025, respectively). Peak systolic and end diastolic velocities were not significantly different in the injected and uninjected eyes at day 7 after the injection (p>0.05). In the injected eyes, there was no significant change in resistance and pulsatility indices (p>0.05), but a decrease in resistance index of NPCA and resistance and pulsatility indices of TPCA occurred in uninjected eyes at day 7 after the injection (p = 0.016, p = 0.023, and p = 0.025, respectively).
Conclusions
Intravitreal bevacizumab affects retrobulbar blood flow in injected and uninjected eyes of patients with diabetic macular edema.
Introduction
Diabetic retinopathy (DR) is the leading cause of vision loss in the working population all around the world. Diabetic macular edema (DME) is the most common cause of visual impairment in patients with DR and is an important public health problem (1). In recent years, intravitreal anti-vascular endothelial growth factor (VEGF) agents have demonstrated positive visual and anatomical results in patients with DME (2–6). Bevacizumab is a full-length humanized monoclonal antibody that binds all VEGF-A isoforms. Due to the crucial role of VEGF in the development of DR and DME and cost-effective profile of bevacizumab, it has been used frequently as an off-label agent in the management of DME.
Although intravitreal bevacizumab (IVB) has been shown to be safe in most previous studies, there are studies reporting the worsening of preexisting retinal ischemia in patients with DR after IVB injection (7, 8). Adverse vascular events including central retinal artery (CRA) occlusion, branch retinal artery occlusion, central retinal vein occlusion, branch retinal vein occlusion, retinal capillary occlusion with resultant macular ischemia, conversion of nonischemic central retinal vein occlusion to the ischemic form and anterior ischemic optic neuropathy, and ocular ischemic syndrome have been reported following IVB (9–16). The exact mechanism of these adverse vascular events is not clear, but they may be related to the vasoconstrictive effect of anti-VEGF agents or an increase in intraocular pressure (IOP) (17, 18).
The ischemic vascular events may be even more devastating in the setting of ischemic retinal vascular diseases, like DR. Retinal hypoxia, as demonstrated by capillary dropout, is well-known in patients with DR. As demonstrated in previous studies, both retinal and choroidal circulation are affected in diabetic patients with or without DR (19). Decreased blood flow velocity and increased resistance index (RI) of ophthalmic artery (OA) and CRA were reported in patients with proliferative DR (20). Despite widespread use of anti-VEGF agents, in the setting of already deteriorated ocular circulation in patients with DR, their effects on retrobulbar blood flow merit further investigation.
To our knowledge, there is no study evaluating the effect of IVB on retrobulbar blood flow in patients with DME. Our purpose was to show the short-term effect of IVB on retrobulbar blood flow parameters in the injected and uninjected fellow eyes of patients with DME using color Doppler imaging.
Materials and Methods
Thirty-seven patients treated with IVB for DME were assessed prospectively. Informed consent was obtained from all patients and the study was approved by the local ethics committee and carried out in accordance with the Declaration of Helsinki.
Patients with previous intraocular surgery and intravitreal injection within the past 3 months, retinal vein occlusion, retinal artery occlusion, optic neuropathy, glaucoma, macular dystrophy, intraocular inflammatory disorder, retinal detachment, hypertensive retinopathy, IOP more than 21 mm Hg during the study period, or coronary artery disease were excluded from the study.
All patients underwent a complete ophthalmic examination including best-corrected visual acuity, examination of the anterior and posterior segments, measurement of IOP by applanation tonometry, fluorescein angiography, and optical coherence tomography.
The injection procedure constituted 1.25 mg/0.05 mL injection of bevacizumab (Altuzan, Roche Diagnostics GmbH, Mannheim, Germany) through pars plana, 4 mm away from the limbus, under sterile conditions in the operating room.
Ultrasound imaging using color Doppler system (EZU-MT28-S1, Hitachi Medical, Tokyo, Japan) with a 4-MHz to 9-MHz linear array transducer was performed before the injection and at day 1 and day 7 after the injection by the same radiologist. All measurements were recorded at the same time of day (between 9 AM and 2 PM). Color Doppler imaging examination was carried out as described by Lieb et al (21) using a paraocular approach while the patients were in supine position. The OA, CRA, nasal posterior ciliary artery (NPCA), and temporal posterior ciliary artery (TPCA) were evaluated in all patients. Ocular blood flow indices of peak systolic velocity (PSV) and end diastolic velocity (EDV) were measured in both eyes. Pulsatility index (PI) and RI were calculated automatically by the scanner after measuring the systolic and diastolic blood flow velocities of each vessel.
Statistical analysis was done by SSPS statistical software (SPSS for Windows 10.0, Chicago, IL, USA). Comparisons were made using paired t tests. Data are expressed as mean ± standard deviation. Statistical significance was defined at a level of 5% (p<0.05).
Results
The mean age of the patients was 61.65 ± 10.02 (39–84) years. Of the 37 patients, 15 were men and 22 were women. There was no statistically significant difference between the injected and uninjected eyes regarding the baseline measures of ocular blood flow indices (PSV, EDV, RI, PI) for each vessel (all p>0.05).
The PSV and EDV in the CRA and NPCA decreased statistically significantly at day 1 after IVB in the injected eyes (p<0.05, p = 0.025, respectively) (Fig. 1, a and b). The PSV and EDV in the OA and TPCA also decreased slightly at day 1after the injection, but was not statistically significant (p>0.05). The difference between baseline and day 7 values for PSV and EDV was not also statistically significant in the 4 arteries (p>0.05). The RI and PI values of the 4 arteries did not show any significant change in each paired comparison in the injected eyes (all p>0.05) (Tab. I) (Fig. 2, a-d).
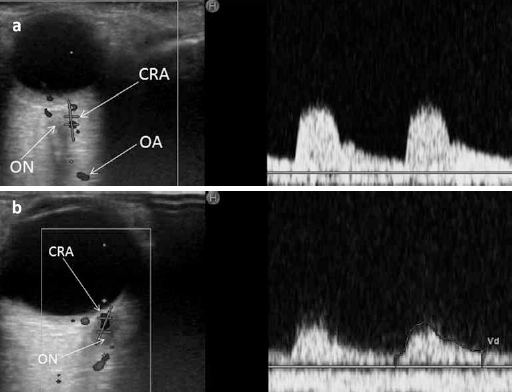
(a) Doppler analysis of the central retinal artery (CRA) in a patient with diabetic macular edema (DME) before intravitreal bevacizumab injection. (b) A significant decrease in peak systolic and end diastolic velocity of CRA occurred at day 1 after intravitreal bevacizumab injection. OA = ophthalmic artery; ON = optic nerve.
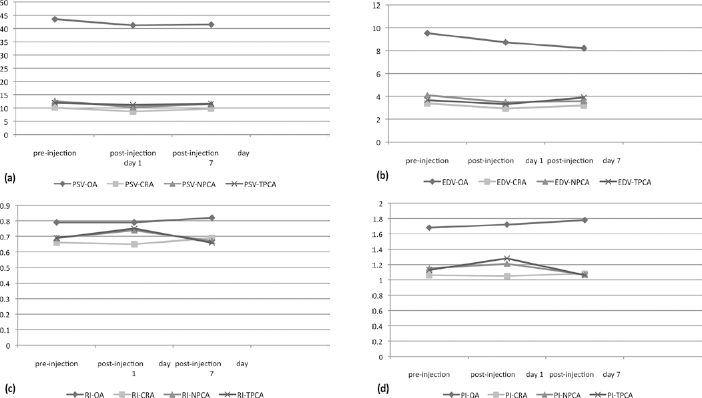
(a-d) Ocular blood flow parameter changes before and after intravitreal bevacizumab in all 4 arteries in the injected eyes.
Doppler parameters in the injected eyes
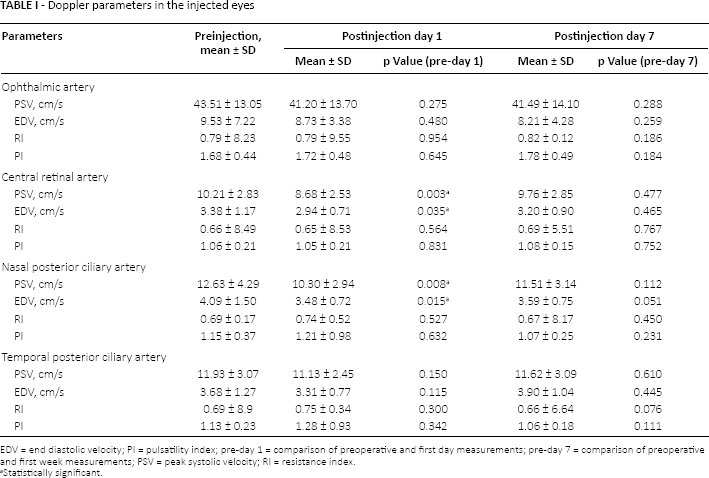
EDV = end diastolic velocity; PI = pulsatility index; pre-day 1 = comparison of preoperative and first day measurements; pre-day 7 = comparison of preoperative and first week measurements; PSV = peak systolic velocity; RI = resistance index.
statistically significant.
In the uninjected fellow eyes of 37 patients, PSV of NPCA showed a statistically significant reduction (p<0.05), but the reduction of EDV of NPCA was not statistically significant at day 1 after the injection (p>0.05). Although there was a numerical reduction in PSV and EDV parameters of CRA (p = 0.05, p = 0.05, respectively), it did not reach a statistically significant level at day 1 after the injection. The PSV and EDV of OA and TPCA and RI and PI of the 4 arteries did not show significant difference at day 1 after the injection (all p>0.05). When compared with preinjection values, PSV and EDV of the 4 arteries were not statistically significantly different at day 7 after the injection (all p>0.05). The RI of NPCA and RI and PI of TPCA was reduced significantly at day 7 after the injection in the uninjected fellow eyes (p = 0.016, p = 0.023, and p = 0.025, respectively) (Tab. II) (Fig. 3, a-d).
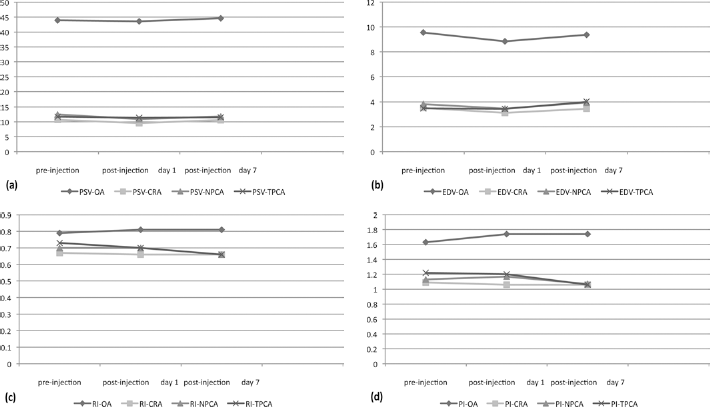
(a-d) Ocular blood flow parameter changes before and after intravitreal bevacizumab in all 4 arteries in the uninjected fellow eyes. CRA = central retinal artery; EDV = end diastolic velocity; NPCA = nasal posterior ciliary artery; OA = ophthalmic artery; PI = pulsatility index; PSV = peak systolic velocity; RI = resistance index; TPCA = temporal posterior ciliary artery.
Doppler parameters in the uninjected eyes of the patients
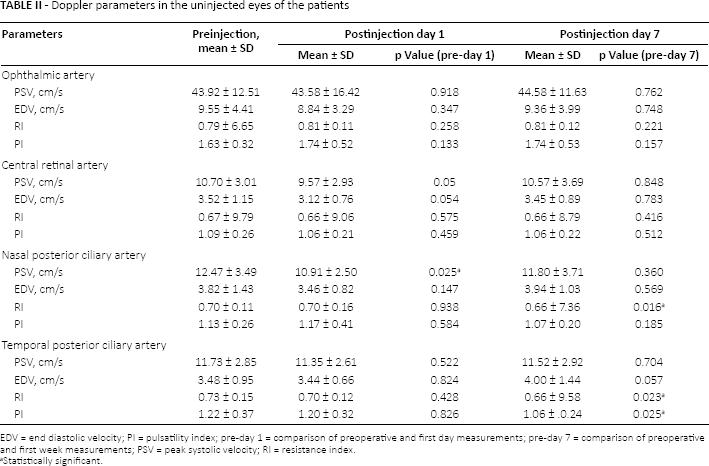
EDV = end diastolic velocity; PI = pulsatility index; pre-day 1 = comparison of preoperative and first day measurements; pre-day 7 = comparison of preoperative and first week measurements; PSV = peak systolic velocity; RI = resistance index.
Statistically significant.
Discussion
Vascular endothelial growth factor has been shown to be one of the main agents in the pathogenesis of many ophthalmologic disorders such as proliferative DR, DME, neovascular age-related macular degeneration, neovascularization secondary to central or branch retinal vein occlusion, and edema secondary to causes other than diabetes (17, 22–25). Anti-VEGF therapy has been established as an effective treatment of DME. Bevacizumab (Avastin) is one of the most commonly used anti-VEGF agents and despite the availability of anti-VEGF drugs specifically designed for intraocular use, significant off-label use of intravitreal bevacizumab persists for various neovascular ocular diseases like DME. Following extensive use of bevacizumab, some concerns about its side effects on the retrobulbar and systemic circulatory system were raised and supported by several thromboembolic accidents (12, 26). Soliman et al (17) and Tatlιpιnar et al (27) showed vasoconstriction of retinal vessels after IVB in patients with DME though the difference was not statistically significant. An acute visual acuity loss following IVB for DME has also been reported (28). However, the effect of IVB on retinal and choroidal hemodynamics has not yet been tested in patients with DME.
Bevacizumab has 2 successive effects: vasoconstriction occurs very soon after injection (from minutes to hours), which is mediated mainly by nitric oxide (NO) and followed by a decrease in capillary density occurring from hours to a few days after injection. This capillary disappearance has been described in experimental murine models, not in humans. Nitric oxide is also important in retinal blood flow autoregulation and arteriolar tone maintenance. Another effect of bevacizumab is endothelial cell injury, which results in occlusion of choriocapillaris. At the first day of treatment, fibrin accumulates and patency is lost in some capillaries, and at day 2, endothelial cells undergo apoptosis and regression (29–32). In this study, we observed a reduction in retrobulbar blood flow velocities (BFV) of CRA and NPCA of the injected and NPCA of the uninjected eyes at day 1 after IVB. At the first week after the injection, BFV of CRA and NPCA were not statistically significantly different compared with preinjection values. The blood flow parameters of OA did not reveal any significant change in the injected and uninjected eyes of patients with DME after the injection.
Decreased BFV of CRA shows the effect of IVB on the vascular bed of the retina in the injected eyes. The retinal vasculature is the first vascular network that comes into contact with the intravitreal injected drug, therefore decreased BFV of CRA is not surprising in the injected eyes. Decreased BFV of NPCA may be explained by the effect of bevacizumab on the choroidal blood flow. There are some theories that may explain this issue. First, IVB was found to induce early reduction of choriocapillaris endothelial cell fenestration in rats (33). Second, bevacizumab may induce arterial thrombosis by exposing subendothelial procoagulant phospholipids inhibiting VEGF-induced endothelial regeneration (34). Bevacizumab may also reduce the production of NO and prostacyclin thus predisposing to thromboembolic events (35). The BFV in OA may reflect the effect of the drug on the entire orbit after its transretinal and scleral diffusion to deeper layers. It is well-known that large molecules can diffuse from the choroid to the periocular tissues. The amount of the drug may decrease and this may cause lesser effect in the OA than vessels feeding retina and choroid. The effect of the drug in the uninjected fellow eyes may be explained by the inhibition of VEGF in systemic circulation. In previous studies, it has been shown that bevacizumab may enter the systemic circulation (36). In this study, in the uninjected fellow eyes, the decrease in BFV of NPCA and CRA was more prominent than in OA. Therefore, the action of the drug may not be related to its concentration in the vessels as we expect greater concentration in OA than in NPCA and CRA in the uninjected eyes. This needs to be evaluated with further studies.
Decreased BFV of the arteries may not be related to IOP rise in the present study. We excluded patients from the study who had IOP more than 21 mm Hg during the study period, as measured at each visit. Also, the effect of acute IOP rise on retrobulbar hemodynamics can occur immediately after the intravitreal injection. As Wu and Evans (37) and Hollands et al (38) showed in previous studies, IOP generally tends to return to normal levels within 30 minutes after the intravitreal injection. In the present study, we evaluated the effect of IVB on retrobulbar hemodynamics at day 1 and at day 7 in patients with DME. We also found decreased BFV in the fellow uninjected eyes, despite no space-occupying effect of the drug, which is expected to cause IOP elevation.
Another surprising result of the present study is that the effect of IVB on blood flow parameters was more prominent on the first day and returned close to preoperative values by the end of the first week. In previous studies, retrobulbar blood flow after IVB was studied in neovascular age-related macular degeneration and the authors proposed that the effect was more prominent at the end of the first week owing to the half-life of the drug (9.8 days) and reduced to preinjection levels by the end of the first month (39, 40). We should also consider that, in the present study, participants were composed of patients with DR who already had affected ocular blood flow parameters. Possible mechanisms for this early change in retrobulbar blood flow merit further study.
In conclusion, a significant decrease in blood flow velocities occurred in retrobulbar circulation at day 1 after IVB and returned close to preinjection values by the end of the first week in injected and uninjected fellow eyes of patients with DME. Therefore, patients should be monitored for adverse effects of IVB on retrobulbar blood flow during the first week after the injection. Further studies with larger sample sizes are required to clarify the effect of IVB treatment on retrobulbar blood flow parameters in patients with DME.
Footnotes
Financial support: No financial support was received for this submission.
Conflict of interest: None of the authors has conflict of interest with this submission.