
Abstract
Purpose
To compare visual function after implantation of multifocal Lentis comfort LS-313 MF 15 (group 1) or Lentis M plus LS-313 MF 30 (group 2) intraocular lenses (IOLs).
Methods
Patients between 49 and 76 years of age who received monocular cataract surgery with multifocal IOL implantation were analyzed. Patients were evaluated preoperatively and for 5 months postoperatively for distance, intermediate, and near visual acuities, and static photopic and mesopic contrast sensitivity. A satisfaction questionnaire was administered 5 months after surgery.
Results
Group 1 comprised 21 eyes and group 2 contained 34 eyes. Both groups had a statistically significant improvement in uncorrected and corrected distance visual acuities postoperatively (p<0.01). Uncorrected visual near acuity at 40 cm was better in group 2 (1 month: p = 0.013; 5 months: p = 0.051). Uncorrected intermediate visual acuity at 70 cm was better in group 1 (1 month: p = 0.060; 5 months: p = 0.044). No significant differences in contrast sensitivity were observed between the groups. Glare and halo symptoms were better in group 1 (glare: p = 0.044; halo: p = 0.029).
Conclusions
Inferior sector-shaped, near-addition IOLs with lower add powers (+1.5 D) provide good vision over longer working distances and show fewer glare and halo symptoms.
Introduction
Visual performance after cataract surgery is highly dependent on the type of intraocular lens (IOL) implanted. Recent design advances in IOLs have resulted in very good visual outcomes after cataract surgery. From this development, cataract patients have high expectations of visual quality after cataract surgery, including spectacle independence. The most recent IOL models are aimed at restoring not only distance but also intermediate and near visual function. Multifocal IOLs have been developed to provide patients with an IOL with more than 1 focal point, enabling good visual acuity at more than one distance. The Lentis Mplus (Oculentis GmbH, Berlin, Germany) is an IOL that provides multifocality by using a refractive, rotationally asymmetric design (1). Segmented, asymmetric (also termed “zonal”) refractive multifocal IOLs have shown better contrast sensitivity and intermediate vision outcomes than those of diffractive multifocal IOLs (2, 3). The Lentis Mplus (Oculentis GmbH) included an inferior surface-embedded segment with an addition of +3.00 D for near vision. The recently introduced Lentis Mplus LS-313 MF 15 also has rotational asymmetry, but with a near add of +1.50 D. This design may provide an optimal visual outcome at near and intermediate distances with lower incidence of optical side effects.
Alió et al (4) reported a comparison between +3.00 D LS-312 IOLs and +1.5 D LS-312 IOLs in 2011, but the Mplus model had a c-loop design before modification. The modified plate haptic LS-313lens, presented in Venter et al (5), showed less tilting. After that study, only the plate haptic LS-313 IOL has been used. To our knowledge, there have been no direct comparisons reported among plate haptic LS-313 IOLs, +1.5 D IOLs, and +3.0 D IOLs. In this study, we evaluated near, intermediate, and distance visual outcomes of low add power multifocal IOLs. These outcomes were compared with an earlier +3.00 D-add near segment-embedded IOL model.
Methods
Patients
This study was approved by the institutional review board of the University of Ulsan College of Medicine, Asan Medical Center, Seoul, South Korea. After being fully informed of the details and possible risks of the surgical procedure, all patients provided written informed consent. Exclusion criteria included previous ocular surgery or trauma and the presence of corneal opacities, fundus abnormalities, glaucoma, uveitis, amblyopia, systemic disease, or posterior capsule rupture during cataract surgery. All subjects underwent standard-of-care senile cataract extraction with multifocal IOL implantation with an add power of +1.5 D (LS-313MF15; Oculentis GmbH, group 1) or +3.0 D (LS-313 MF 30; Oculentis GmbH, group 2) at the University of Ulsan College of Medicine.
Surgical technique
Phacoemulsification surgery was performed using topical anesthesia (0.5% proparacaine hydrochloride). The same surgeon (H.T.) performed all of the operations. All patients had undergone phacoemulsification and the implantation of a foldable IOL using a 2.2-mm biplanar clear corneal incision. Incision locations were selected according to the steep corneal axis, which was evaluated using keratometric power analysis. First, when selecting the incision, a perpendicular groove incision was made approximately 0.2 mm anterior to the edge of the limbal vessels using a 2.2-mm disposable blade. The IOL was implanted into the capsular bag using a Monarch II injector with a C-cartridge (Alcon Laboratories, Inc., Fort Worth, TX, USA). The residual ophthalmic viscosurgical device was removed from behind the IOL and anterior chamber. The anterior chamber was reformed, and stromal hydration of the main incisions was performed.
Patient examinations
Postoperative evaluations were performed 1 and 5 months after cataract surgery. All subjects underwent measurement of monocular uncorrected distance visual acuity (UDVA) and manifest refraction (MR) values. Monocular uncorrected near visual acuity (UNVA) was also measured using a Rosenbaum near vision card at 40 cm. Monocular uncorrected intermediate visual acuity (UIVA) was measured at 70 cm. Contrast sensitivity under photopic and mesopic conditions was measured using a vision contrast sensitivity test (Vistech Consultants, Inc., Hartford, CT). Finally, 5 months after surgery, the subjects were asked to complete a questionnaire regarding overall satisfaction following surgery, presence of visual symptoms, and spectacle dependence for near and far vision. Overall satisfaction was assessed using the 5-point Likert scale (1 = very dissatisfied; 2 = dissatisfied; 3 = neither satisfied nor dissatisfied; 4 = satisfied; 5 = very satisfied).
Statistical analysis
Statistical analysis was performed using the SPSS software package for Windows (version 19.1, SPSS, Inc., Chicago, IL, USA). First, the normality of all data samples was evaluated using the Kolmogorov-Smirnov test. When parametric analysis was possible, the independent-sample t test for paired data was used. When parametric analysis was not possible, the Wilcoxon rank-sum test was used to assess the significance of differences between preoperative and postoperative status and the Mann-Whitney test for between-group comparisons. The chi-square test was used to compare responses to the subjective questionnaire. For all statistical tests, the level of significance was p<0.05.
Results
Fifty-five eyes of 55 patients were included in this study, with 21 eyes in group 1 (+1.5 D-add) and 34 in group 2 (+3.0 D-add). The preoperative patient and ocular characteristics of the 2 groups are summarized in Table I. There were no statistically significant between-group differences in age, corrected distance visual acuity (CDVA), sphere, cylinder, mean keratometry, or manifest refraction.
Preoperative demographic characteristics of the study patients
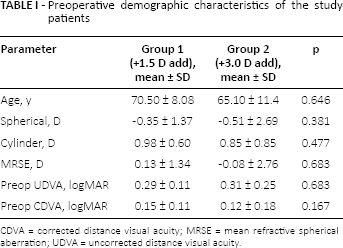
CDVA = corrected distance visual acuity; MRSE = mean refractive spherical aberration; UDVA = uncorrected distance visual acuity.
Visual acuity, refraction, and preferred reading distance
Table II lists the postoperative UDVA, UIVA, UNVA, and MR values. The mean 5-month postoperative uncorrected and distance-corrected visual acuity improved. No significant differences in the UDVA and CDVA were observed between the 2 groups. However, the UNVA at 40 cm was better in group 2 than in group 1 at 1 month (p = 0.013) after surgery. The UIVA at 70 cm was better in group 1 at 5 months (p = 0.044) after surgery. The preferred reading distance showed significant differences between the 2 groups: 43.31 cm for group 1 and 37.31 cm for group 2 at 5 months after the operation (p = 0.022).
Visual acuity, manifest refraction, and preferred reading distance for the study subjects with rotational near-sector multifocal intraocular lenses with add power of +1.50 D (group 1) and +3.00 D (group 2)
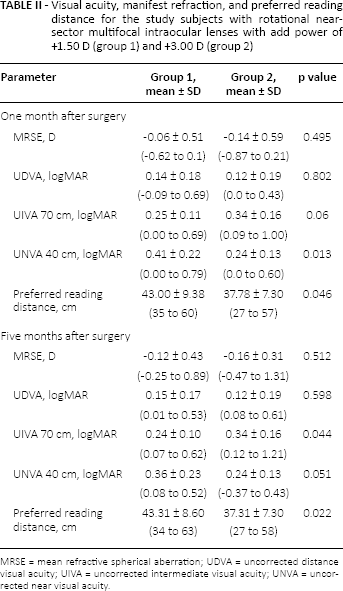
MRSE = mean refractive spherical aberration; UDVA = uncorrected distance visual acuity; UIVA = uncorrected intermediate visual acuity; UNVA = uncorrected near visual acuity.
Contrast sensitivity and defocus curve
Figure 1 shows the contrast sensitivity under photopic and mesopic conditions in the 2 groups. Both groups demonstrated good contrast sensitivity under both conditions. There were no statistically significant differences at any spatial frequency (p>0.05, Student t test). The depth of focus results are shown in Figure 2. The depth of focus curve in group 2 had double peaks with the 0 D and −3.0 D addition powers. Conversely, group 1 showed a smooth line instead of a double peak, implying a gradual decrease from distance to near vision, and better performance in intermediate vision.
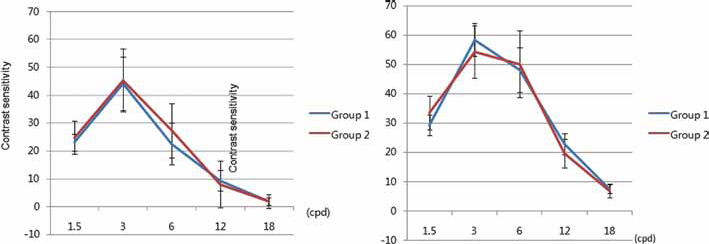
Contrast sensitivity (log values) under photopic (left) and mesopic (right) conditions in the 2 study groups. No significant differences were observed (Student t test, all p values >0.05).
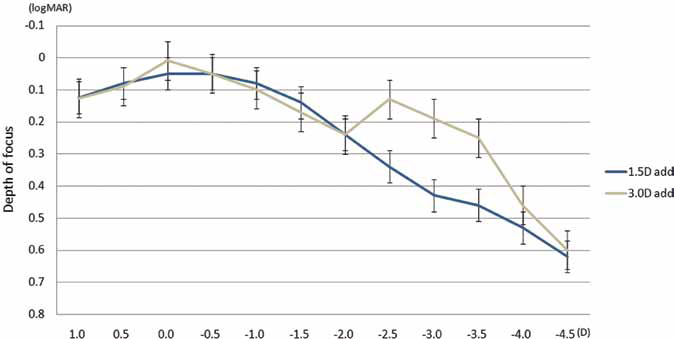
Depth of focus curve in eyes implanted with the +1.5 D-add Mplus intraocular lens (IOL) and +3.0 D-add Mplus intraocular IOL.
Patient satisfaction
Five months after surgery, all patients completed satisfaction questionnaires. The answers are summarized in Table III. Overall satisfaction after surgery showed no statistical difference between the 2 groups (p = 0.128). Interestingly, glare and halos symptoms were significantly lower in group 1 (p = 0.004, p = 0.029).
Patient satisfaction questionnaire responses
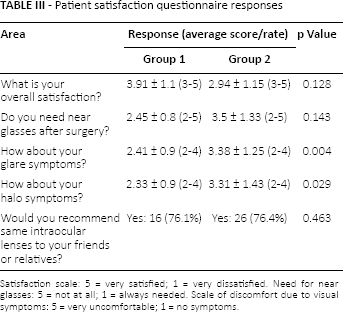
Satisfaction scale: 5 = very satisfied; 1 = very dissatisfied. Need for near glasses: 5 = not at all; 1 = always needed. Scale of discomfort due to visual symptoms: 5 = very uncomfortable; 1 = no symptoms.
Discussion
Multifocal IOLs were developed to provide patients with good visual acuity at more than one distance. The latest developed segmented asymmetric refractive multifocal IOLs (MIOLs) demonstrate better contrast sensitivity outcomes compared to diffractive MIOLs (6). These IOLs with refractive rotational asymmetry were developed to minimize side effects such as glare, halos, and reduced contrast sensitivity (7). However, using an IOL with an addition of +3.0 D might result in an insufficient target distance for patients who frequently use computers and electronic devices, which have working distances of approximately 60-70 cm. Patients now have higher expectations of vision quality following cataract surgery, including intermediate distance (e.g., cooking, driving). Therefore, multifocal IOLs with a special emphasis on intermediate vision are needed. The LS-313 MF15 IOL (+1.5 D-add) was produced to customize these patient needs. In the present study, we evaluated 2 models of the Lentis plus MIOL, which is based on the concept of refractive rotational asymmetry.
As expected, the UNVA at 40 cm was significantly better with the +3.0 D-add IOL than with the lower add IOL 1 month after surgery. At 5 months, the UNVA was also better with the +3.0 D-add IOL, but this difference was not significant. The UIVA at 70 cm was significantly better with the +1.5 D-add IOL both 1 and 5 months after surgery. The defocus curve also demonstrated better intermediate visual acuity with the +1.5 D-add IOL, as it did not show 2 peaks like the + 3.0 D-add MIOLs, but a gradual decrease from distance to near visual acuity.
Another remarkable finding of our study was the significantly lower symptoms of glare and halo with the +1.5 D-add IOL. Despite high levels of general patient satisfaction after multifocal IOL implantation, some patients will be dissatisfied even to the point that the lens must be explanted (8). There is a trade-off between spectacle independence and visual quality (9, 10). A recent study reported less glare and halo symptoms in low-add diffractive MIOLs (11). Interestingly, patients who received the rotational inferior-sector MIOLs reported less dissatisfaction due to glare and halo symptoms. The reason for this lower perception of halos in the +1.5 D-add group might be that, theoretically, the halo size, which is the size of the out-of-focus image on the retina, depends on the add power of the near-focus UDVA (9). Even though the size of the halo is smaller with lower add powers, the intensity of the halo might be higher (12). Therefore, clinicians should fully educate their patients on possible postoperative symptoms and carefully interview them about lifestyle and postoperative expectations.
In conclusion, the +1.5 D-add rotational near-section IOLs provide good intermediate visual acuity, also providing good distance visual acuity. They would not be a good choice for patients who have a lifestyle that focuses on near tasks, but would be more appropriate for patients who have higher expectations of intermediate distance and are not very sensitive to photic phenomena.
Footnotes
Financial support: No financial support was received for this submission.
Conflict of interest: None of the authors has conflict of interest with this submission.