
Abstract
Impingement of the lesser trochanter on the ischium or the posterior acetabular rim is not a frequent pathology, but has recently received increased recognition. We have seen 14 cases over a period of 14 years, but concentrate on eight hips showing complex deformities revealing similar characteristics. All eight hips had a residual Perthes or a Perthes-like disease with an elliptically deformed femoral head, but a congurent joint a short or absent femoral neck, a high riding greater trochanter, and a reduced vertical distance between the head and the lesser trochanter. Impingement took place between the lesser trochanter and the ischium or the posteroinferior acetabular border, but was hardly recognisable due to the predominant intraarticular impingement of the nonspherical femoral head and the extraarticular impingement of the greater trochanter. In three cases the impingement showed reproducible subluxation of the hip.
While in our hips, excision was the preferred treatment for impingement due to an oversized lesser trochanter, distal advancement was used in the hips with the Perthes morphology; the surgical time was not longer. The overall clinical results in this group however were dominated by a substantial increase in the range of motion (ROM), dependent mainly on the achieved contour of the femoral head and the relative lengthening of the neck.
Strength of active hip flexion was normal. Recurrent subluxation disappeared and no complications were recorded.
Introduction
During the past 15 years intraarticular femoroacetabular impingement (FAI) (1, 2) has been increasingly recognised as an important mechanism for the development of osteoarthritis of the hip (3-7). Extraarticular impingement has been known for much longer; however this occurs less frequently. It can be initiated by a number of factors around the hip. More commonly, extraarticular impingement is caused by ectopic bone formation after trauma. The most frequent pathology that can lead to extraarticular impingement is a high riding greater trochanter, giving rise to the phenomenon of hinged abduction due to its contact with either the superior or the posterior wall of the acetabulum, or the ischium; the shorter the femoral neck, the easier it is for the impingement to take place (8). What is relatively unknown is the extraarticular impingement that can also occur between the lesser trochanter and the ischium (9, 10), more recently this has been subsumed under ischiofemoral impingement (IFI) (11-15).
We have observed impingement of the lesser trochanter in 14 hips and describe here the pathophysiology and the surgical treatment options with special reference to eight hips with rather uniform morphological characteristics of Perthes or a Perthes-like deformity.
Material
The age of our 14 patients ranged between 11 and 63 years. In the Perthes group the average age was 12 years ranging between nine and 19 years; 10 patients in the overall group and seven in the Perthes group were female. All cases were collected between 1997 and 2010.
Besides the Perthes group, in three hips the cause of impingement was a cartilaginous exostosis of the lesser trochanter, two hips had an iatrogenic background (a subtrochanteric valgus osteotomy for developmental dysplasia of the hip, and a total hip arthroplasty (THA) with the combination of a femoral prosthesis with a short neck and a medial cup position). In one hip a pertrochanteric fracture had healed with a medially displaced lesser trochanter and callus formation.
Informed consent was obtained from all patients, and approval was obtained from our ethical review committee.
Pathomorphology
With normal hip morphology the lesser trochanter is located sufficiently lateral to the ischium to not risk a mechanical conflict. In coxa valga this apophysis comes closer and may even overlap on pelvic radiographs. Although the femoral neck and shaft are normally anterior to the ischium, external rotation may further narrow this space as does increased femoral anteversion. If in such a hip one additional parameter is only borderline normal or even pathologic, e.g. medial migration of the femoral head in protrusio, impingement between the lesser trochanter and the ischium may take place. A similar pathomorphological scenario may arise if a femoral prosthesis with a short neck is combined with a medial cup position as in one of our hips. In this case successful treatment consisted of exchanging the modular head with one that lateralised the prosthesis. In the cases of Johnson (9), with a slightly different morphology, the lesser trochanter was resected. Isolated deformities of the lesser trochanter can produce a straightforward decrease in the space between it and the ischium. Deformities with a subsequent increase in volume can happen with a fracture of the lesser trochanter that heals with displacement, but more frequently it is a cartilaginous exostosis as in three of our cases and in the bilateral case of Viala et al (15); resection was executed in all four cases. In the past, subtrochanteric valgus osteotomy was performed frequently for bilateral hip dislocation with the aim of supporting the pelvis by placing the lesser trochanter within the acetabulum. When performed for high subluxations, the lesser trochanter could remain caudal to the acetabulum and eventually produced impingement with the ischium. This problem is not discussed in the literature on subtrochanteric valgus osteotomy, but is described in one of Johnson's cases (9), and was observed in one of our 14 hips.
In hips with the sequelae of Perthes or similar morphologies resulting from disturbances to the perfusion of the femoral head, the deformity can be rather complex (16). Besides a large and high riding greater trochanter, the femoral neck can be very short or even absent. As a consequence, the distance between it and the pelvis is reduced. The vertical distance between the lesser trochanter and the femoral head can also be very small. Version of the femoral neck is difficult to define, however, there is a tendency for it to be highly anteverted. The femoral head can be placed anteriorly but also posteriorly on the neck, depending on its deformity. With all of these deformities together, the lesser trochanter critically approaches the proximal part of the ischium or even the posterior acetabular border (Figs. 1 and 2).
Pathophysiology
Symptoms of extraarticular impingement of the lesser trochanter are often nonspecific. Pain may be referred to the inferior buttock area with extension along the inner side of the thigh and intensify during longer walking distances. A feeling of crepitation has been described in the case of Patti et al (10). Iconographic equivalents of the impingement can be seen occasionally with cystic and sclerotic changes to the contact area on the ischium, or on MRI with oedema of the short external rotator muscles in the vicinity of the impingement, especially the quadratus femoris (10, 11, 13, 14). ROM may be limited during rotation and become painful when provoked with adduction. In other cases, especially with increased volume of the lesser trochanter, patients may deny having pain, but the leg is held in abduction and cannot be placed in a normal position relative to the pelvis leading to a functional lengthening of the extremity. Three patients (two with the Perthes morphology, one with an exostosis) reported feelings of hip instability related to rotation, a phenomenon that could be substantiated as reproducible subluxation during impingement of the lesser trochanter. All three cases had borderline acetabular dysplasia (Fig. 1B). On the other hand, in complex deformities, impingement of the lesser trochanter can be hidden behind an intrarticular anterior impingement of a nonspherical head within the acetabulum and an extraaticular posterosuperior impingement produced by a high riding greater trochanter against the pelvis.
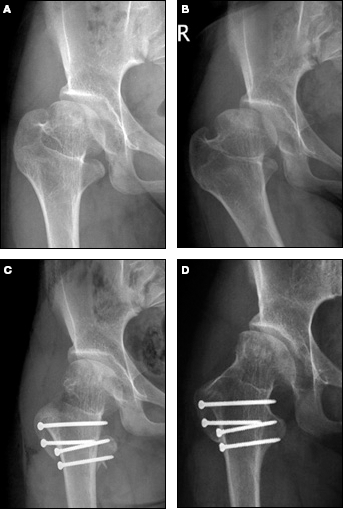
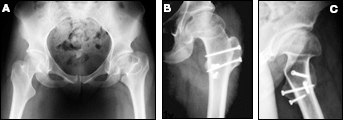
A) 11-year-old female patient with epiphyseal dysplasia and a Perthes-like deformity of the right hip. It is a complex deformity with a nonspherical femoral head, a short neck, and relative overgrowth of the greater and the lesser trochanters. There is slight subluxation and subtle structural changes of the ischial bone in the vicinity of the lesser trochanter. B) Radiograph of the right hip in adduction with increased subluxation, apparently levered by the ischial contact of the lesser trochanter. C) Full relocation of the femoral head into the acetabulum after relative lengthening of the femoral neck and distal advancement of the lesser trochanter. D) Radiographic result four years later with good containment and congruency.
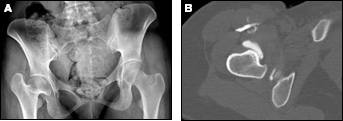
15-year-old female patient with a Perthes-like deformity of the right hip after conservative treatment of developmental dysplasia in early childhood. There is good coverage and congruency of the femoral head, a nearly absent femoral neck, and a high riding greater trochanter. There is a small distance between the head and the lesser trochanter that is level with the posteroinferior acetabular border. B) Arthro-CT section through the lesser trochanter shows the immediate proximity with the posterior acetabular rim.
Generally speaking, the existence of impingement of the lesser trochanter may be suspected from clinical examination and standard radiographies, however for confirmation, MRI or computer tomography is recommended (Fig. 2). Recent technology has used models from 3D reconstruction to simulate the impingement and can concentrate on the lesser trochanter by subtracting other impingement sources (8).
Treatment
Mild symptoms of lesser trochanteric impingement can be treated with pain medication and reduction of irritating activities. Compensation of the leg length discrepancy may have a contrary effect; it can bring the lesser trochanter closer to the ischium and eventually within the critical distance for impingement. For more severe and chronic problems, surgery has to be discussed. In the context of THA, the spectrum ranges from selecting a prosthesis with a sufficient head-shaft offset, eventual resection of the lesser trochanter, to revision surgery.
When the natural hip is to be preserved, surgery must protect the blood supply of the femoral head. Due to the short distance between the femoral head and the lesser trochanter, the deep branch of the medial femoral circumflex artery (MFCA) runs even closer than normal to the superior border of the trochanter and towards the posterior joint capsule (Fig. 3) (17); this vessel serves in 80% of hips as the main provider of femoral head perfusion (18). With a large and irregularly shaped exostosis of the lesser trochanter, angiography may help you to understand the individual topographical relationship between the vessel and the exostosis, allowing its preservation during the excision of the tumor. In the Perthes deformity with a normally shaped lesser trochanter, one may consider preservation of the trochanter with its psoas attachment and instead perform a distal advancement, a method that has been executed in our eight Perthes cases.
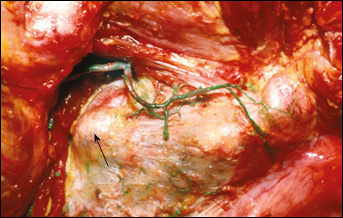
Cadaveric dissection of the posterior aspect of a right hip with vessel injection of green-coloured latex. The depicted vessel is the deep branch of the MFCA running just proximal to the lesser trochanter (arrow) and distal to the obturator externus muscle and tendon, towards the trochanteric crest. The deep branch is the main provider of blood for the femoral head.
Technique of Advancement of the Lesser Trochanter
In a Perthes hip with a complex deformity, a lateral approach to the proximal femur, performing a trochanteric flip osteotomy and then dislocating the joint is routine (19). Subsequent shaping of the femoral head and relative lengthening of the neck increases ROM. The technical aspects of this approach are described elsewhere in detail (20). Briefly, the surgery takes place in a lateral decubitus position with the upper leg draped freely. After a longitudinal incision is made over the greater trochanter, the fascia is opened along the anterior border of the gluteus maximus muscle (21) and the entire muscle belly is retracted posteriorly. The osteotomy is performed using an oscillating saw in such a way that the insertions of the gluteus medius, vastus lateralis, and the long head of the gluteus minimus remain attached to the trochanteric fragment, while the insertions of all of the external rotators remain attached to the stable trochanter. The capsule is approached between the gluteus minimus and the piriformis tendon, a gap that allows the best preservation of both the primary and the anastomosing blood vessels that supply the femoral head (18). After anterior, superior, and posterosuperior exposure of the capsule, a Z-shaped incision (right side) is performed. It extends along the anterolateral head-neck contour with an anterior branch near the base of the femoral neck and a posterior branch along the acetabular rim allowing subluxation, and after section of the round ligament, full dislocation of the femoral head. In hips with an extremely short femoral neck and a very large greater trochanter, dislocation can be executed more easily after trimming the base of the trochanter, which is also part of the technique of relative lengthening of the neck. The trimming is performed in a piecemeal fashion and the pieces are resected strictly subperiosteally until the level of the superior and the posterior femoral neck is reached (Fig. 4). After shaping the femoral head and completion of the relative lengthening of the neck, impingement of the lesser trochanter is confirmed with rotational manoeuvres in extension and extension-adduction.
To expose the lesser trochanter the femur is further internally rotated. The base of the lesser trochanter is identified using periosteal elevators. A strictly subperiosteal exposure of its superior contour is more effective at protecting the deep branch of the MFCA. The psoas tendon is preserved in its entity but does not need to be visualised. The osteotomy at the base of the lesser trochanter should produce an area of cancellous bone that is big enough to place two screws (Fig. 1); it is best performed using a straight osteotome. After completion of the osteotomy, the fragment is mobilised and pulled distally using a bone hook. It is provisionally fixed using an anteroposterior Kirschner wire. After an on-table assessment is performed to ensure that there is now impingement-free motion, two lag screws each with a diameter of 3.5 mm are inserted either from anterior or from posterior (Figs. 1 and 5).
The postoperative management is determined primarily by the achieved contour of the femoral head and the relative lengthening of the neck. To protect the fixation of the lesser trochanter, active leg raise and forceful rotation should be avoided during the first four weeks. After six weeks of partial weight bearing with two crutches, all osteotomies are sufficiently healed for increased loading and function. When a femoral derotation was performed in addition, this time may be increased to 8–10 weeks. Unrestricted function should be allowed between 12 and 14 weeks after surgery.
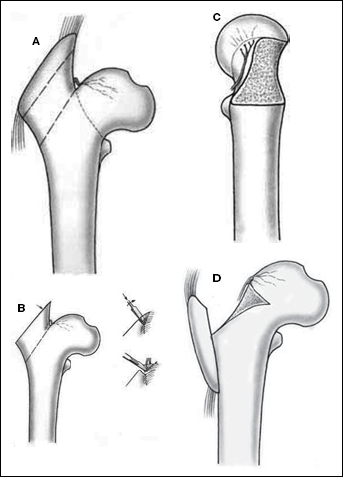
Technique of relative lengthening of the femoral neck. A) After the trochanteric flip osteotomy (upper dotted line), the bone of the remaining stable trochanter has to be resected down to the lower dotted line, while the retinacular vessels have to be preserved. B) The bone is resected in a piecemeal manner. After a fragment is broken and turned with a bone clamp, it is resected in a strictly subperiosteal manner until the posterior border of the greater trochanter is level with the femoral neck. C) Posterolateral appearance of the newly, now longer femoral neck with the retinacular vessels preserved, and D) an anteroposterior view with the supposed final position of the trochanteric fragment. Reproduced with permission from (20) Ganz R, Huff TW, Leunig M. Extended Retinacular Soft-Tissue Flap for Intra-articular Hip Surgery: Surgical Technique, Indications, and Results of Application. In: Azar FM, O'Connor MI (eds): Instructional Course Lectures 58. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2009, pp. 241-255.
Severe Perthes deformity in a 19-year-old female patient. The x-ray shows an extremely high greater trochanter and nearly no gap between the femoral head and the lesser trochanter. Impingement of the lesser trochanter became evident only after shaping the femoral head and increasing the relative length of the neck. B) Anteroposterior radiograph of the 3-year result. C) Lateral view showing the posteroanterior insertion of the screws for fixation of the lesser trochanter.
Results
After follow-up of 3.5 years (2-12), the advanced lesser trochanter had healed uneventfully in all eight hips and there was no visible ectopic bone formation. Clinically, no residual impingement of the lesser trochanter was detectable and the strength of active hip flexion was identical to the opposite side. Subluxation disappeared in all three cases. The overall clinical results in the Perthes group however were dominated by the substantial increase in ROM, dependent mainly on the achieved contour of the femoral head and the relative lengthening of the neck.
Discussion
Impingement of the lesser trochanter against the ischium or the posteroinferior border of the acetabulum is not a frequent pathology; it has been described in a small number of case reports that have included up to three patients (9, 10, 14, 15). More recently, extraarticular impingement of the lesser trochanter has been subsumed under ischiofemoral impingement (11-15), although impingement between the greater trochanter and the ischial part of the posterior wall of the acetabulum also exists and is probably even more frequent (8).
Over a period of 14 years we have collected 14 cases of lesser trochanter impingement presenting in a variety of pathomorphological conditions. With normal hip morphology the distance between the lesser trochanter and the pelvis is approximately 2 cm (10). Less space and oedema of the quadratus femoris have been a consistent finding on MRI in patients with hip pain when compared with individuals without hip pain (11, 13); however no association with any pathomorphological particularities of the hips was discussed. Overlap on anteroposterior radiographs does not necessarily mean impingement because the proximal femur is normally anterior to the ischium. High values of caput-collum-diaphyseal angle (valgus hips) and anteversion (coxa antetorta) of the femoral neck reduce this distance, but there may need to be an additional pathology such as protrusio acetabuli to lead to impingement. This combination is documented, however not mentioned in the case of Patti et al (10). Similar aspects play a role when impingement of the lesser trochanter is correlated with THA (9). While impingement in cases of displaced fragments or tumors of the lesser trochanter is not a difficult diagnostic problem, it may be hidden in complex deformities of the proximal femur when other sites of impingement predominate. This might explain why up to now it has not been described in the relatively frequent Perthes deformity; in our series it is represented in eight cases.
Symptoms are not very specific and in Perthes cases they are typically hidden behind other sources of pain. However, what is striking is the potential for recurrent subluxation caused by the contact of the lesser trochanter against the ischium as seen in our three cases; in all three cases the phenomenon was facilitated by slightly insufficient acetabular coverage.
When surgery was indicated, it consisted of resection of the lesser trochanter if it was oversized. In all cases of Perthes or a Perthes-like deformity, distal advancement of the lesser trochanter was performed. We felt that preservation of the intact insertion of the strong psoas tendon would be preferable in this young age group. Although the overall good results were dominated by the effect of shaping the femoral head and the relative lengthening of the neck as demonstrated in our most recent paper (16), the strength of active hip flexion after advancement of the lesser trochanter was equal to the opposite side.
In summary, extraarticular impingement of the lesser trochanter is a pathology that has recently received interest; it seems to be especially frequent in severe Perthes deformities. There, it may be hidden behind the intraarticular impingement of a nonspherical head and the extraarticular impingement of the greater trochanter. When suspected, it can be demonstrated with MRI and subtractive simulation. It should be verified intraoperatively by palpation after shaping the femoral head and relatively lengthening the neck, and may be treated with distal advancement, which so far has demonstrated uneventful healing and function.
Footnotes
Financial Support: There was no outside source of funding for this study.
Conflict of Interest: There is no conflict of interest for all authors.