
Abstract
Corrosion of metallic implants in contact with body fluids is unavoidable, especially at interfaces where movement occurs or in gaps. Corrosion became clinically relevant with the introduction of large modular metal-on-metal total hip joint articulations (MoM THA) early in the 21st century. This review attempts to summarise the scientific knowledge about taper problems available at the time of introduction of these bearings, why this “disaster” could happen. It is speculated that changes to the taper connection made in the 1990s to increase the range of motion with small heads (28 and 32 mm) reduced the mechanical strength of this connection, which did not matter for small heads. With the use of large and very large metal heads in MoM articulations, which have a larger lever arm and can generate high friction in unfavourable situations, suddenly the taper interface exhibited corrosion problems on a previously unknown scale. It is speculated that due to the higher mechanical loading with larger heads, the taper connection became less forgiving with respect to assembly conditions, contamination, manufacturing tolerances and other factors, which are yet not known. Since no major clinical problems had been reported before the introduction of these bearings and the pre-clinical testing was very successful, the disaster took its course. The patient-implant-surgeon system is a very complex intrinsically hazardous system. Pre-clinical testing addresses few and defined factors and such, good results cannot be directly transferred to the clinical reality. A controlled stepwise introduction of innovations is required.
Introduction
The attention paid to the taper junction of modular metal components in orthopedics has risen dramatically in the past 5 years. This interest was evoked primarily by the problems associated with the use of large heads (diameter greater than 36 mm) in combination with metal-metal (MoM) bearing articulations in total hip replacement (THR). This combination was introduced early in the 20th century along the revival of hip resurfacing as a revision option for resurfacing prostheses, which have failed by femoral neck fracture. This option also allowed physicians, who wanted to achieve the same stability as with resurfacing but were either not able to use resurfacing due to availability or didn't believe in the resurfacing concept, the opportunity to combine large diameter bearings with their usual modular hip stems. This opportunity was quickly recognised and used by many surgeons. Since hip joint replacement represents one of the most frequently performed operations and the trend to use large heads was promoted by nearly all the big companies (since there was a demand by many physicians for this product), the absolute number of patients who received them, was accordingly great.
The initial publication that caused particular concern and triggered a number of additional publications dates from 2009 (1). Prior to this publication, the focus was more on friction and wear problems in hip resurfacing than large head metal-on-metal (MoM) prostheses, without making a major distinction between these 2 types of implants (2–4). In the 2009 annual report of the National Joint Registries of England and Wales (NJR), there was no differentiation between resurfacing and large-head MoM (5) (Fig. 1). Furthermore, the MoM results overall were not recognised as worse compared to ceramic-on-ceramic bearings (Fig. 2). In the 2010 NJR report, the problems with large-head MoM prostheses became obvious (6) (Fig. 3) and the focus was increasingly directed to the taper junction since this was the obvious difference between the 2 prostheses types, causing the clinical difference in results between resurfacing prostheses and large-head MoM prostheses. At the beginning one specific implant was made mainly responsible for the bad performance of large MoM prostheses (ASR by DePuy) (7, 8). The device was recalled in 2010; the question about this “category” of implants, large-head MoM on a stem with a taper, arose only slowly. Until today, no other company has recalled their product despite a rising number of concerns. The worst observed clinical endpoint is taper fracture, which has been observed in certain designs with a titanium stem taper and a titanium sleeve connector to the ball head (Fig. 4). This design has only been utilised by one company for their modular MoM prostheses.
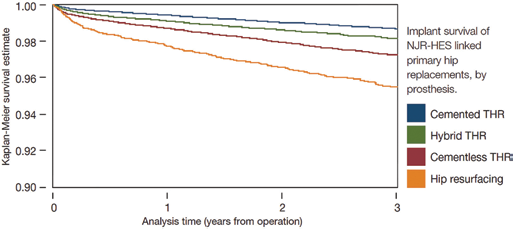
Reproduced with permission from the National Joint Registry of England, Wales and Northern Ireland, 6th Annual Report 2009 (5): Implant survival rate for different prosthesis groups. www.njrreports.org.uk; www.njrcentre.org.uk.
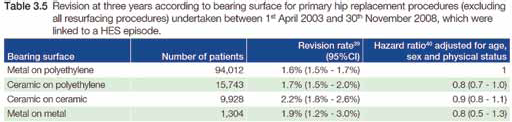
Reproduced with permission from the National Joint Registry of England, Wales and Northern Ireland, 6th Annual Report 2009 (5): Implant survival rate for different bearing articulation materials. www.njrreports.org.uk; www.njrcentre.org.uk.
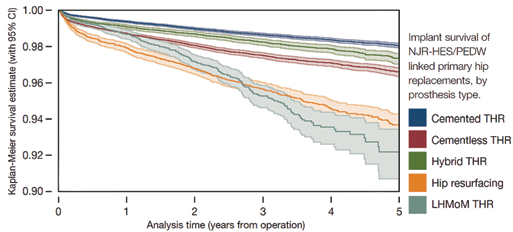
Reproduced with permission from the National Joint Registry of England, Wales and Northern Ireland, 7th Annual Report 2010 (6): Implant survival rate of different prosthesis groups. www.njrreports.org.uk; www.njrcentre.org.uk.

Stem taper fractures in BiMetric (Ti6AI4V; Biomet, Warsaw, IN, USA) hip prostheses with M2A Magnum heads (taper inserts made from same Ti). Fracture in all 3 patients occurred due to fretting and crevice corrosion without warning. Heads were cut for further analysis (courtesy of Ake Hamberg, Harmen Ettema, Caes Verheyen).
The rising problem with taper connections in hip replacement was ultimately addressed politically by the European Union with the establishment of a SCENIHR (Scientific Committee on Emerging and Newly Identified Health Risks) working group investigating “The safety of Metal-on-Metal joint replacements with a particular focus on hip implants about the MoM problems”. The preliminary consensus of this working group was published in September 2014 and addressed this topic explicitly:
“This metal debris can originate either from the bearing articulation directly or from the modular taper junction between prosthesis head and stem. In the past, the taper has only been reported anecdotally as the origin of problems. Recently, the taper has emerged as the focus of attention, since large modular metal heads for MoM arthroplasty were introduced due to their ability to reduce dislocation risk, which is the second major complication in hip arthroplasty. These larger heads, however, put larger loads on the taper junction and are suspected to be responsible for the problems suddenly occurring at this side” (Page 10, Opinion on “The safety of Metal-on-Metal joint replacements with a particular focus on hip implants”, http://ec.europa.eu/health/scientific_committees/emerging/docs/scenihr_o_042.pdf: accessed 27 April 2015).
The reason for the great public interest was the fact that the metal debris produced by wear and corrosion were suddenly directly associated to clinical symptoms that in many cases lead to revision. This started after 2005 (9, 10) and first for resurfacing and not for large metal heads. Since this time, the number of publications addressing the taper issue has exploded (11) from a total number of publications between 1988 to 2009 (21 years) of 57 to 87 between 2010 and 2014 (4 years). The question that arises with the current knowledge is quite obvious:
Were there serious indications of possible taper problems with consequences on the clinical outcome of hip joint replacement at the time, when large-head MoM prostheses were introduced? Or, phrased differently, did we overlook the obvious?
This question will be discussed in this review based on the historical scientific studies available at the time of the market introduction of this prosthesis type. The review is organised into 4 sections according to the type of available studies, which each conclude with a summary, and a conclusion at the end:
Clinical Evidence (tumours, pseudotumours);
Results based on explant analyses;
Findings from laboratory investigations;
Opinions, Reviews.
Tapers of modular revision stems are not included in this analysis.
Literature Analysis
Clinical Evidence
McDougall 1956 (12): Reported on a malignant soft tissue tumour caused by a bone plate and screws. According to the authors, the first report of a soft tissue tumour caused by metal abrasion/corrosion.
Penmann 1984 (13): Osteosarcoma suspected to have been caused by cobalt particles. Overall risk of tumour development as the result of hip joint replacement is considered very low.
Swann 1984 (14): Case study of a patient with a soft tissue tumour after hip joint replacement.
Ryu 1987 (15): Case study of a patient with a soft tissue tumour after hip joint replacement with a ceramic joint articulation. Warning about the correlation on radiographs with fluid accumulations caused by wear. Recommend to check for tumours in hip implant loosening.
Ingram 1988 (16): Case study of a patient with a soft tissue tumour after hip joint replacement with a ceramic joint articulation.
Brien 1990 (17): Case study of a bone tumour after hip joint replacement.
Salvati 1995 (18): Indication of the development of metal wear on modular junctions with osteolysis as a clinical consequence. Demands that taper junctions be designed so that no wear particles occur.
Picard 1997 (19): Case study of a pseudotumour as a result of metallosis after implantation of an isoelastic hip prosthesis. Considered a rare occurrence which could be detected due to the concomitant osteolysis.
Langkamer 1997 (20): Analysis of the Bristol tumour register from 1980 -1992 with about 240 malignant soft tissue tumours; 4 of them soft tissue tumours after hip joint replacement.
Bal 1997 (21): Osteolysis at the tip of an uncemented Moore prosthesis. Recommendation that all joint implants be investigated for such complications.
Bell 1997 (22): Risk of the development of a sarcoma as the result of metal wear after prosthesis loosening.
Brodner 1997 (23): Determined serum cobalt levels in 55 patients by atomic absorption spectrophotometry before and after implantation of uncemented total hip arthroplasties. In a randomised, prospective trial, 27 MoM articulations were compared with 28 ceramic-on-polyethylene hips. The MoM group produced detectable serum cobalt levels (median 1.1 μg/l after 1 year) which were significantly higher from those of the ceramic-on-polyethylene control group (median below detection limit of 0.3 μg/l after 1 year). Findings indicate that MoM bearings generate some systemic release of cobalt.
Paavolainen 1999 (24): Finnish Register (31,651 PE on metal prostheses). No sarcomas in the vicinity of the prosthesis. Hip joint replacement has no effect on cancers.
Jacobs 1998 (25): Conjecture that the taper junction between head and stem is responsible for the significant increase in titanium- and cobalt concentrations in the patient, even when the prostheses are functioning well. In the long-term this could lead to local and systemic consequences. In symptomatic patients, metal concentrations in the blood should be checked since they could indicate fretting corrosion.
Jacobs 1998 (26): Prospective study with 3 patient groups (and control group) with different hip stems (cemented modular cobalt-alloy stem and head, uncemented porous-coated cobalt-alloy stem and head, uncemented proximally porous-coated titanium-alloy) all with a cobalt-alloy head and an uncemented titanium socket. After 3 years, all patients with implants had increased titanium, cobalt and chromium levels in urine and serum. It was concluded that that fretting corrosion at the head-neck coupling is an important source of metal release that can lead to increased concentrations of chromium in the serum. It was suggested to monitor metal ions in symptomatic patients.
Lucas 2001 (27): Case study of sarcomas in 2 patients with hip joint replacements. Compared to the joint replacement operations performed during the last 40 years, the number is considered extremely low and, for that reason, considered more likely to be incidental.
Leinung 2002 (28): Inflammatory tumour in a 62-year-old patient as a result of significant metal wear.
Savarino 2002 (29): Prospective study in 2 groups of patients with the same prosthesis but different bearings: metal-on-metal versus metal-on-PE. After 1 to 3 years, the MoM bearing group showed a significantly higher systemic release of cobalt and chromium compared to metal-on-PE and reference. It is suggested to improve the bearing materials or, at least, to study the biologic fate of metal ions and consequently their long-term effects. In such a way a risk-to-benefit ratio for the patient could be established.
Savarino 2003 (30): Extension of the previous study looking at serum ion values in the short-term after a mean of 2 years versus medium-term (mean follow-up: 52 months). Co and Cr levels in the medium-term were not decreased in comparison with the short-term values and still significantly higher than pre-surgical and reference values. The authors concluded that despite the apparent advantage of metal-on-metal coupling, especially in younger patient populations, a major concern regarding the exposure to Cr and Co ions remains. The exposure should be carefully monitored, in order to clarify the biologic effects of ion dissemination and, consequently, to identify risks concerning long-term toxicity of metals.
Adams 2003 (31): Case study of an osteosarcoma after hip joint replacement. The porous implant surface was also mentioned as a cause.
Clarke 2003 (32): Prospective study comparing resurfacing arthroplasty to 28 mm MoM total hip arthroplasty (THA). At a median of 16 months, both groups had significantly increased ion levels. Resurfacings resulted in a greater systemic exposure of cobalt and chromium ions than bearings of small diameter. This was deemed to possibly be of relevance for potential long-term side-effects.
Summary
A few isolated cases of soft tissue tumours are documented in the literature, likewise a very small number of cancer cases. The groups around Jacobs, Savarino and Clarke showed elevated metal ions after MoM THR and all cautioned to monitor (especially symptomatic) patients, to improve materials and tapers. None of the authors really did “ring the bell” that there might be a major problem. Furthermore, none of these papers investigated XL MoM heads. The studies investigate patients with small metal heads or resurfacings, which are continued to be used today, since the registry results of small metal heads are similar to other bearings up to 12 years after implantation (Annual report of the National Joint Registry, AOA, 2014). The same can be said for resurfacing arthroplasty in a defined subsample of the patient population, which can still be called “acceptable” (33).
Explant Analyses
Collier 1991 (34): Corrosion between cobalt chromium head and titanium stem in 57% of analysed revision hip joint replacement components (30 components implanted 0.5 to 67 months.) Concern about the development of metal ions and possible junction failure.
Mathiesen 1991 (35): Case study of 9 patients with necrosis as the result of metal particles during revision. Crevice corrosion on the taper between head and stem suspected as the cause.
McKellop 1992 (36): Case study documenting corrosion at the taper junction of a hip prosthesis.
Collier 1992 (37): Analysis of 250 explants. Fretting corrosion seen as a problem that must be prevented through design improvements and low tolerances so that the advantages of modularity outweigh the disadvantages.
Collier 1992 (38): Analysis of the modular head junction of 230 explants. No corrosion with junctions from the same metal compared to 50% with junctions from different metals, increasing with length of implantation. Galvanic corrosion is considered the cause.
Gilbert 1993 (39): Analysis of the modular head junction of 148 explants. Significant corrosion with all material pairings (same and mixed), increasing with length of implantation. Conjecture that corrosion could lead to implant failures or increased wear or metal accumulation in the tissue.
Lieberman 1994 (40): Analysis of the modular head junction of 48 explants. No corrosion between the same metals and mixed metals with high taper junction strength. Improvement of the tolerances is recommended to increase junction strength, which, in turn, would reduce the micro-motion and entry of fluid.
Boggan 1994 (41): Analysis of the modular head junction of 3 explants. No corrosion, slight fretting, no material wear.
Cook 1994 (42): Analysis of the modular head junction of 108 explants. Distinctly greater percentage with corrosion and wear in the group with mixed metals after an average of 2 years. No connection with other parameters (e.g. weight and length of implantation). Stems with corrosion were less likely to have bone ingrowth. 84% of the explants without corrosion. “Better” manufacturing methods should be developed.
Urban 1994 (43): Analysis of the modular head junction of 15 explants. Corrosion products on the prosthesis and in the periprosthetic tissue.
Brown 1995 (44): Analysis of the modular head junction of 79 explants. Short-term results do not indicate any increase in corrosion problems with mixed metals. Design improvements should increase junction strength and thus reduce the fretting corrosion.
Jacobs 1995 (45): Analysis of the modular head junction of 79 explants. Short-term results do not indicate any increase in corrosion problems with mixed metals. Design improvements should increase junction strength and thus reduce the fretting corrosion.
Collier 1995 (46): Analysis of a total of 731 modular head junctions. Survey of the manufacturers, all of which viewed corrosion as the principal modular junction problem. Corrosion was found in 7% to more than 30% of the explants, depending on material combinations and series.
Goldberg 2002 (47): Analysis of a total of 231 modular head junctions. Greater corrosion with mixed metals (and manufacturing methods) and on the head of the prosthesis, increasing with mechanical stress (implantation time, neck stiffness). Larger taper diameters are identified as a possibility for the reduction of fretting corrosion, but should not restrict the range of motion too greatly.
Jones 2001 (48): Analysis of modular fracture nails. Metal wear is shown to create osteolysis and soft tissue reactions.
Windler 2003 (49): Analysis of 155 12/14 taper CoCr heads implanted up to 113 months. 50% of the ball heads showed evidence of corrosion after 4 years. No effect of neck length. Observations only partly similar to results of the laboratory experiments.
Schaaff 2004 (50): Literature review with regard to the significance of fretting corrosion. Despite the evidence available from explant studies, it is concluded that no “quantitative” conclusions can be drawn. Better methods for measuring corrosion and abrasion are required.
Summary
Almost all studies report corrosion at the taper junction with the corresponding effects: implant failure, increased metal wear on the taper as well as release of ions- and particles. The influence of the material pairing was also recognized early (possibly more problems with mixed metals). Almost all of the conclusions lean toward requirements with regard to design improvements, fewer toward warnings of biological consequences. It is interesting that the Windler study indicates that the results of the laboratory investigations do not agree with the explants but this finding did not draw any consequences (49).
Experimental Laboratory Studies
Fricker 1990 (51): Short-term investigation of the fretting corrosion behavior on head-stem taper junctions of different metals. Conclusions: it is not expected that any problems will develop with long-term use.
Cook 1993 (52): Warning about the use of bi-modular hip prostheses because of motion and wear production at the stem-shoulder junction.
Bobyn 1994 (53): Investigation of 3 different bimodular prostheses. During long-term stress, significant concentrations of metal particles were found. A missing criterion about permissible metal concentrations is criticised and tougher testing conditions demanded – but without being specific. Higher assembly forces led to lower coloration.
Manley 1994 (54): During bending and torsion tests large quantities of material wear were observed at taper junctions and associated with osteolysis in the patient. Demands that the design, manufacture and tolerances of modular junctions in THA be re-evaluated and that they be used only in areas with low bending and torsion stresses.
Vieconti 1996 (55): Cyclical corrosion test of 2 different hip stems. No corrosion, but fretting was found. Demand for a better design.
Vieconti 1997 (56): Cyclical corrosion test of 1 bi-modular hip prostheses. The amount of realised metal was considered non-critical.
Baleani 1997 (57): Cyclical corrosion test of two bi-modular hip prostheses. Additional metal wear was found, but considered non-critical if the assembly of the junction is done correctly.
Chu 2000 (58): Finite element investigation of the taper joint of a bimodular junction. Separation of the contact in areas of the taper joint during physiological stress that could generate metal wear or corrosion was calculated.
Schramm 2000 (59): Cyclical laboratory testing and explant analysis of modular revision prostheses, even with contaminated joining surfaces. Conclusions: longevity for clinical use is met and the benefit of the modularity is greater than the risk.
Goldberg 2003 (60): Cyclical corrosion test with tapers of a different material pairing. Fretting could be generated with loads below physiological stresses. It was determined that no difference between the different material combinations was observed, but mechanical stress in all leads to corrosion.
Smith 2001 (61): Tribological simulator study which focused on the reduction of the metal wear due to head diameter increase. Abrasion and corrosion were not discussed.
Nassutt 2003 (62): Investigation of the influence of resting phases on the frictional torque in different sliding contact pairings. Large head metal pairings were considered critical, not with regard to overloading of the taper, but rather because of the risk of aseptic implant loosening.
Summary
In all studies, corrosion was reported. Bending as a critical loading mode was identified. Like in the explant analyses, differing views about the effect of the material pairing are presented (same metal alloy vs. different metal alloys). The additional metal debris from the taper connection was not seen as a major problem and there was the belief that improvement in design could reduce this problem. The effect of taper surface contamination during assembly is appreciated, less of the assembly force.
Opinions
Barrack 1994 (63): Modular junctions are considered extremely valuable for all joints. The problems were also taken into account, but the authors assume that the problems could be minimised by design improvements.
Schey 1996 (64): The authors point out that little is known about MoM and basic research is required to understand this combination.
Mc Carthy 1997 (65): For various reasons it was indicated that modular implants should be used with caution and in fact only if monoblock implants cannot be used.
Summary
The problems that can arise at the taper junction were already known in the mid-1990's; however, the extent was not seen since the frequency of problems occurring in patients was rather low or the revision was performed without explicitly referring to the reason for the phenomenons observed in the explants. Besides fretting corrosion, crevice corrosion was made responsible for the damage.
Conclusions
When metal implants are introduced into the body, corrosion due to the contact with body fluids is almost unavoidable, especially at connection sides where relative movement occurs or in gaps and between different metals. For that reason, almost all implants that were in the body for a longer period of time show some traces of corrosion. The assessment of the extent of the corrosion is difficult and usually takes place qualitatively (visual assessment) or through measurement of ion concentrations in fluids. These ion concentrations, however, are comprised of a combination of mechanical material wear and corrosive material wear.
The corrosion problems at taper junctions of modular hip prostheses as well as the biological reactions evoked by metallic debris, were known at the time of the introduction of large MoM bearings – from individual case studies, explant analyses and also laboratory investigations. At this point in time, however, no major clinical problems had been reported and therefore these phenomena were “described” in an anecdotal manner instead of raising major concerns. Compared to the number of the implantation cases, the problems appeared to be minimal; furthermore, there was the conviction that the frequency of these problems could be reduced further by design or tolerance improvements. Interestingly enough, only very few of the studies pointed out the importance of the process of component assembly (assembly force and contaminations). A larger head diameter was also not considered critical in any of the available studies. The importance of the observation that results from explant analyses did not correspond to results of experimental laboratory studies was not recognised (49). It should be pointed out that many studies suggested improvement of taper design and manufacturing methods and tolerances but no publications regarding respective improvements can be found.
The minor dimension of taper problems observed until the beginning of the 21st century can probably be explained by the use of the smaller head diameter until this point in time (up to a maximum of 36 mm). The reduction of the taper diameter (from the original 14/16 to 12/14 or V40) as well as the reduction of taper length (from 2 cm to below 1 cm) to expand the range of motion, was carried out without obvious new problems at the end of the 1990s, since smaller heads “load” the taper junction less than large heads that were introduced around this time (much larger than 36 mm in diameter; to emphasise: originally to allow to keep well-fixed acetabular cups in patients with femoral neck fractures after resurfacing NOT as an option for primary systems). It is hypothesised that the combined perturbation of the originally so successful THA implant system by the changes of 3 parameters (taper diameter, taper length, head diameter) together with the simultaneously occurring spread of MoM joint articulations, which can generate high friction in unfavorable situations (62, 66–68), more or less “suddenly” jeopardised the strength and robustness of the taper junction. The extent to which deviations in the assembly process play a role (contamination and assembly force) has not been conclusively explained yet but is heavily suspected (69–71). It can also be speculated that minimal invasive surgery with small incisions did not help to reduce taper contamination and the application of appropriate assembly forces in taper direction.
Each of the changes alone has been justified and is meaningful from an isolated point of view; in combination, these changes probably caused the dramatic and fast increase of issues associated with the taper junction of the modular components. A minor change (or, as in this case, minor changes of several factors) can lead in complex systems to the occurrence of new faults and failure modes, which is what happened in the case of the large-head metal-on-metal bearings. From the present point of view, this could have been predicted if all of the available information and publications had been properly pieced together and interpreted. However, since there were only a few publications available at this time (11) and none of these publications reported a major clinical problem, this did not happen in a timely manner. Instead the enthusiasm of the community focused on the outstanding wear and dislocation characteristics of these “improved” metal-on-metal bearings, since dislocation and wear were regarded as the dominant factor for the success of hip arthroplasty. It was not realised that possibly the good simulator results would not be reflected in the patient.
Complex systems are intrinsically hazardous (72). Richard Cook has put together some important points which have to be considered in the analysis of failures of complex systems (http://www.ctlab.org/download/allspaw-2010-how-complex-systems-fail-pdf/April 27 2015):
Catastrophe requires multiple failures - single point failures are not enough;
Catastrophe is always just around the corner;
Post-accident attribution to a ‘root cause’ is fundamentally wrong;
Hindsight biases post-accident assessments of human performance;
Change introduces new forms of failure.
Even so manufacturers, patients, surgeons and lawyers are always looking for the ‘root cause’, we probably have to accept that innovation will always be associated with some risk, which can never be fully eliminated, even through the most sophisticated pre-clinical testing. Secondly, the big benefit of modular heads in hip arthroplasty should not be jeopardised in general by questioning the taper connection. Presently corrosion is reported for nearly every joint articulation material and head size down to metal and ceramic heads with diameters as small as 28mm against Polyethylene (73, 74). Some surgeons even ask for the re-introduction of monoblock primary stems. This would be an unnecessary overreaction. If modular heads are used in a sensible way (not too large, not too long, matching and clean tapers, tapers not too small, proper assembly), the advantages of modularity will outweigh its disadvantages without negating that an additional interface will always carry the risk of potential problems.
The “taper disaster” has demonstrated, that the “operation of the century” (75) cannot easily be improved further by changing implant design but rather the opposite can happen: solving a problem by introducing a new, larger problem. In the future, the main focus should be put on a controlled stepwise introduction of innovations, especially in areas – such as hip arthroplasty – where good solutions are already available (76). We have to continue to improve pre-clinical testing methods by including surgical variation, different patient activities, different biological environments and other factors. However, even the most sophisticated pre-clinical testing will never be able to ascertain good clinical performance of new or altered designs – the patient-implant-surgeon system is just too complex for a direct transfer of laboratory results to the clinical situation.
Footnotes
Conflict of interest: None.