
Abstract
Background
Regional citrate anticoagulation (RCA) is being used increasingly in continuous renal replacement therapy (CRRT) as a safer alternative to heparin. However, complex metabolic control to avoid side effects have generated discrepancies about its introduction into everyday practice. We aimed to compare both anticoagulation techniques in terms of efficacy, safety and feasibility.
Methods
Observational retrospective study performed in 3 specialized ICUs in patients receiving CVVHDF with RCA between January 2013 and May 2016. Heparin-treated patients matched by age, sex and disease severity treated in the preceding year were selected as historic controls. Filter lifetime, number of filters used, haemorrhagic complications and metabolic complications were recorded.
Results
54 patients (27 treated with RCA and 27 with heparin) were included in the study. Filter lifetimes in the first 72 hours were 55.1 ± 21.8 hours in the RCA group compared to 38.8 ± 24.8 hours in the heparin group, (p = 0.004). In addition, the number of filters used in the first 72 hours was significantly higher in the heparin group (2.4 ± 1.3 vs. 1.5 ± 0.7; p = 0.004). There was a trend toward a lower incidence of bleeding in the RCA group, with a significantly lower red blood cell transfusion rate (p = 0.027) in the citrate group. No clinically significant metabolic disturbances were observed in the RCA group. Regarding outcomes, there were no significant differences between groups.
Conclusions
These results suggest that the implementation of CVVHDF with RCA using concentrated citrate solutions prolongs filter lifetime, achieves a longer effective hemodiafiltration time and is a safe and feasible method.
Introduction
Acute kidney injury (AKI) occurs in 35% to 65% of intensive care unit (ICU) admissions and in 5% to 20% of general hospital admissions (1). Individuals who survive an AKI hospitalisation have a greater likelihood of a recurrent hospital admission and are at an increased risk of developing end-stage kidney disease and mortality.
Continuous renal replacement therapy (CRRT) is the most common modality of support therapy for the management of haemodynamically unstable patients with AKI in the ICU. CRRT modalities include continuous veno-venous hemofiltration (CVVHF), continuous veno-venous haemodialysis (CVVHD) and continuous veno-venous hemodiafiltration (CVVHDF). Although not formally compared in large clinical trials, CVVHDF has become the preferred modality since it combines both diffusion and convection (2, 3). However, intense effort is required to perform CRRT, which includes the need for specialized expertise and specific equipment, a large nursing workload, continuous monitoring of the patency of the extracorporeal circuit because of the high frequency of coagulation, which shortens the filter and catheter lifespans, causes blood loss and decreases solute clearance.
Heparin infusion in the circuit is the most commonly used anticoagulation method due to its low cost, easy administration, simple monitoring and reversibility by protamine. However, infused heparin has systemic effects and increases the risk of bleeding and may cause heparin-induced thrombocytopenia (HIT), which can lead to life-threatening complications (4).
Regional citrate anticoagulation (RCA) avoids the systemic effects of heparin since it acts as an anticoagulant in the extracorporeal circuit. In RCA there is no systemic anticoagulation because there is significant loss of the citrate-calcium complexes as they cross the semipermeable membrane of the filter into the effluent; additionally, any citrate or calcium-citrate complexes that remain in the venous line and delivered to the patient are diluted in the patient's blood and rapidly metabolized in the liver or skeletal muscles, producing bicarbonate (4). In addition, before the blood re-enters systemic circulation, the calcium is replaced post filter, thus restoring serum ionized calcium levels. However, RCA does have potential complications too, including changes in the acid-base status, electrolyte derangements such as hypocalcaemia, hypernatremia and citrate toxicity (9).
Previous studies have evaluated the efficacy and safety of RCA versus heparin anticoagulation and the results have yielded large discrepancies (5–11), with meta-analysis showing advantages for risk of bleeding but major discrepancies regarding prolongation of the filter lifespan (12–15). The latest KDIGO guidelines recommend RCA as the first option in patients who require CRRT (16).
Most of the studies evaluating citrate have employed CVVHF or CVVHD as CCRT modalities. There are fewer studies evaluating RCA in CVVHDF and all have used protocols in which citrate is administered within a balanced predilution replacement solution rather than as a separate concentrated solution (12, 13). The administration of citrate as a separate solution allows for 100% postfilter replacement as compared to around 33% when it is administered within a prefilter diluted replacement solution, thus allowing for a more efficiently delivered dose. Conversely, concern has been raised about concentrated citrate solutions because of a potential association with hypernatremia and other metabolic complications, although studies using CVVHD have demonstrated its safety (17).
In this context, the aim of this study was to evaluate the efficacy and safety of RCA with a protocol that included prefilter infusion of citrate as a separate concentrated solution in CVVHDF with 100% postfilter infusion. The focus of the study was to evaluate efficacy and safety, as well as metabolic controls in everyday clinical practice conditions.
Methods
Study design
This observational, retrospective study was performed in 3 different intensive care units (ICU) at our centre (general surgery ICU, acute coronary care unit, and cardiovascular surgery ICU). The study was approved by the local ethics committee. Patients with AKI according to the RIFLE criteria (1) and with an indication for CRRT who remained on it for a time greater than 72 hours were evaluated, independent of the reason for renal failure. Liver failure (INR >2 with acute, chronic or acute-on chronic liver disease), elective systemic anticoagulation, impaired coagulation (platelet count <50 × 109/L, INR >2, partial thromboplastin time >50 seconds) and high risk of bleeding (bleeding within previous seven days or CNS pathology) were exclusion criteria.
In 2013, RCA in CVVHDF modality was introduced in our centre in the abovementioned ICUs. This study analyses the results of this implementation to test its efficacy and safety compared to the standard method of anticoagulation with heparin in everyday clinical practice conditions between January 2013 and May 2016. The primary outcome was filter patency. Based on published evidence (10), with a mean duration (hours) of 30 (SD25) in the heparin group and mean expected mean of 50 in the citrate group, with an error alpha of 0.05 and a power of 80%, the sample size required was 25 subjects in each group.
Subjects
Forty-two patients were initially identified in the RCA group in the study period. Fifteen patients were excluded because of CRRT for less than 72 hours, transfer to another centre or incomplete data. In total, 27 patients with RCA receiving CVVHDF were included. As a control group, 27 patients matched for age, sex, comorbidity and disease severity and treated with CVVHDF with heparin anticoagulation the preceding year at the same ICUs were included as historic controls. General CRRT protocols and monitoring in the 3 ICU's were nephrologydriven and did not change during the study period for both groups.
Data collection
In order to evaluate the efficacy of both anticoagulant strategies, first-filter lifetime and the number of filters used in the first 72 hours of treatment were registered. The reason of first-circuit interruption was documented as 1) elective in cases of intrahospital transfers or scheduled circuit changes at 72 hours as recommended by the manufacturer and 2) coagulation when visible clots were obstructing flow through the machine or the blood pump was unable to rotate due to clot obstruction.
In order to evaluate the safety of both techniques, bleeding episodes, transfusion requirements and the presence of HIT were documented. For the group receiving RCA, metabolic controls were performed during the therapy by monitoring citrate dose, calcium dose and circuit and patient's ionized calcium. Also the following clinical variables were recorded at CRRT initiation, every 24 hours during the first 3 days and at the end of the therapy: platelet count, pH, metabolic alkalosis (increased base excess >3 mmol/L or pH >7.5), metabolic acidosis (decreased base excess <-3 mmol/L or pH <7.25), hypocalcaemia (ionized calcium value of less than 0.85 mmol/L), citrate accumulation (defined by a ratio of total serum calcium to ionized calcium >2.5) and hypernatremia (serum Na+>150 m Eq/L).
The following variables were recorded for both groups with respect to patient's outcome: time on CRRT, ICU and hospital length of stay, kidney recovery (free of RRT), ICU mortality, 30-day survival and glomerular filtration rate (GFR) at ICU and hospital discharge.
CRRT protocol
CVVHDF was performed with the Multifiltrate® monitor (Fresenius Medical Care), with 2 additional external pumps for citrate and calcium infusion in the group of patients who received regional citrate anticoagulation. CVVHDF with citrate anticoagulation was started at predefined treatment settings following the manufacturer's protocol (Fresenius Medical Care) with a predefined and adjusted blood flow (80, 100, or 120 mL/min), dialysate flow (1,600, 2,000 or 2,400 mL/h) and substitution post dilution solution flow (800, 1,000, 1,200 mL/h) according to the weight of the patient for a prescribed effluent dose of around 30 mL/kg per hour. The dialyzer used was the Ultraflux® AV1000S high-flux polysulfone, surface area 1.8 m2 (Fresenius Medical Care).
The dialysate used was Ci-Ca® Dialysate K2, with the following composition: potassium 2 mmol/L, sodium 133 mmol/L, chloride 116.5 mmol/L, magnesium 0.75 mmol/L, bicarbonate 20 mmol/L, zero calcium and glucose 1 g/L. The replacement solution was multiBic® K3, with the following composition: potassium 3 mmol/L, sodium 140 mmol/L, chloride 112 mmol/L, bicarbonate 35 mmol/L, glucose 1 g/L. A 4% trisodium citrate solution (136 mmol/L citrate, Fresenius Kabi) was set at an initial concentration of 5 mmol/L, with flow automatically adjusted by the monitor in proportion to blood flow.
The citrate dose was adjusted to have postfilter ionized calcium in the range 0.25–0.35 mmol/L, with an initial control 15 minutes after setting and every 6 hours thereafter. The infusion of pharmacy-prepared calcium chloride solution (91 mmol/L) was initially set at a dose of 1.7 mmol/L and adjusted after control of systemic ionized calcium to have it in the range of 1.12–1.20 mmol/L. Control of the acid-base status was done by changing (20%) the dialysis fluid flow or the blood flow. Controls were done every 6 hours for blood gas analyses (acid-base status and systemic ionized calcium, sodium, potassium, and postfilter ionized calcium). Total calcium, total magnesium, and phosphate concentrations were determined as clinically required and blood cell counts and coagulation parameters were determined on a daily basis.
CVVHDF with heparin anticoagulation was performed using the dialyzer Ultraflux® AV600S high-flux polysulfone, surface area 1.4 m2 (Fresenius Medical Care). The prescribed dose was 30 mL/kg per hour, using multiBic® K3 for both dialysate and substitution fluids (50% convection and 50% diffusion). For anticoagulation, patients received an initial bolus of 1000 U heparin followed by a continuous infusion of 500 U/h, with subsequent adjustments aimed to maintain an activated partial thromboplastin time (aPTT) of less than 45 seconds.
Statistical methods
Statistical analysis was performed using SPSS version 20 software package. Categorical variables are presented as number and percentage and continuous variables as mean ± standard deviation. Continuous outcomes that were normally distributed were compared using a t-test; otherwise, a Mann-Whitney U-test was used. Proportions were compared using a chi-square test. A plot of the Kaplan-Meier estimate for the survival function of each subject's first circuit was performed, and the circuit lifespan in the 2 groups was compared using a log-rank test. A 2-sided p value <0.05 was considered significant.
Results
Study population
The baseline and demographic characteristics of the 54 patients included in the study are summarized in Table I. Both groups were similar with respect to age and gender and there were no statistically significant differences in laboratory values (serum creatinine, haemoglobin, platelet count and serum K+ and Na+) at CRRT initiation. Baseline characteristics and the mean Charlson index, as well as SOFA and APACHE II scores at initiation of CRRT were similar in both groups. The percentage of mechanical ventilation, antibiotic use and vasopressor use was similar in both groups, and no statistically significant differences were observed regarding the vascular access employed (femoral versus jugular). In the citrate group, 25% of the patients presented AKI on chronic kidney disease (CKD), a rate similar to that observed in the heparin group (37%).
Baseline and demographic data of the patients included in the study
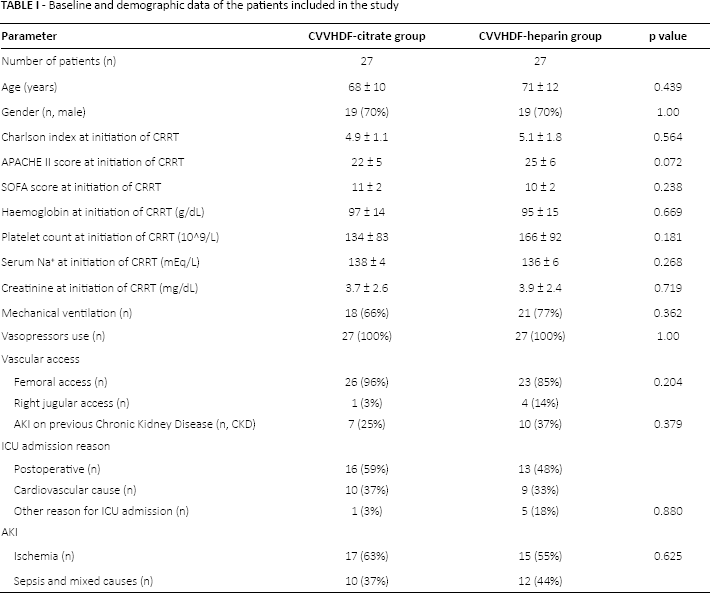
In most cases, the reason for ICU admission in both heparin and citrate anticoagulation groups was previous surgery (emergent or elective). Acute cardiovascular disease, such as myocardial infarction or aortic dissection, was second in frequency in both groups. No cases with severe liver failure were treated with RCA. Most cases of AKI were attributed to ischemic acute tubular necrosis in both groups.
Efficacy
The efficacy of both anticoagulation strategies in maintaining the circuit permeability is summarized in Table II. The mean first filter lifetime was 55.1 ± 21.8 hours in the citrate group, compared to 38.8 ± 24.8 hours in the heparin group (p = 0.004). In total, 43 filters were used in the citrate group, compared to 67 filters in the heparin group. The mean number of filters in the first 72 hours was 1.5 ± 0.7 in the citrate group and 2.4 ± 1.3 in the heparin group (p = 0.004). The cause of circuit interruption was documented and the heparin group presented a higher rate of circuit coagulation (66% of the first filters) with only 22% of the first filters interrupted for an elective cause (p = 0.013). In contrast, the citrate group presented a lower rate of circuit coagulation (33%) and the circuit interruption was due to an elective cause in more than half the cases. First filter lifetime for both groups is represented in Figure 1.
Efficacy and safety of RCA compared to heparin
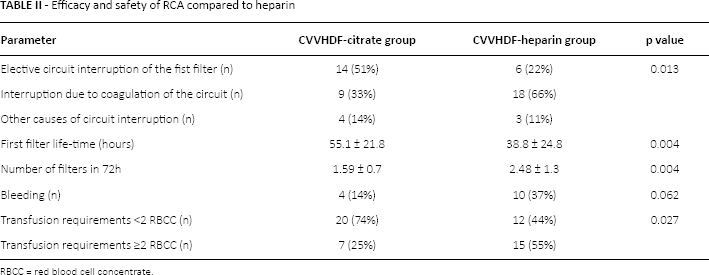
RBCC = red blood cell concentrate.
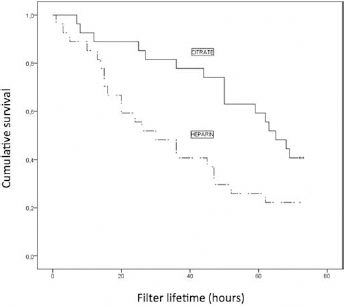
Kaplan-Meier curves for first-filter lifespan in the citrate and heparin groups (p = 0.022).
Safety
In order to evaluate the safety of both techniques, the incidence of bleeding and transfusion requirements was documented (Tab. II). Regarding the incidence of bleeding, there were a higher number of bleeding episodes in the heparin group (37%) than in the RCA group (14%), although the difference did not reach statistical significance. However, there were statistically significant differences in the rate of transfusion requirements (p = 0.027): while in the heparin group 55% of the patients required 2 or more transfusions of red blood cell concentrates (RBCC), this was the case in only 25% of patients in the citrate group. Moreover, in the citrate group, almost 75% of the patients received 0 or 1 RBCC transfusion and, in most cases, transfusion requirements were related to a previous surgery. No cases of HIT were documented in the heparin group.
In terms of metabolic stability, a continuous monitoring was performed in the citrate group, with special attention to citrate and calcium doses, ionized calcium value, platelet count, base excess, pH, incidence of hypocalcaemia and hypernatremia (Tab. III). The mean citrate dose was 4.6 ± 0.58 mmol/L at the beginning of CRRT and 4.47 ± 0.42 mmol/L at the end of the technique. The mean calcium dose values were 1.93 ± 0.2 mmol/L and 2.29 ± 0.5 mmol/L at the beginning of CRRT and at the end of CRRT, respectively. Values of ionized calcium during citrate CRRT course were mostly within the normal range. Hypocalcaemia, defined by an ionized calcium value of less than 0.85, only occurred in 2 patients of 27 (7%) at different times during the technique, with no clinical significance.
Citrate and metabolic controls during the therapy
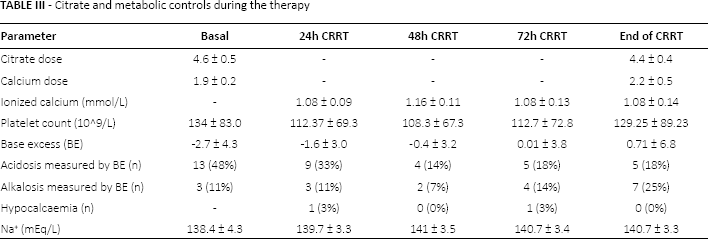
In the citrate group, the mean total calcium 24 hours after the beginning of CRRT was 9.4 ± 0.94 mg/dL, and 9.18 ± 1.07 mg/dL at the end of CRRT. Citrate accumulation was monitored with the ratio of total serum to ionized calcium 2.5. The mean ratio was 2.12 ± 0.34 at the end of the CRRT. Citrate accumulation was detected (ratio >2.5) in 3 patients but none of them required interruption of the technique. Potential derangements of citrate accumulation could be managed by a reduction of blood flow or increase in dialysis flow and ratios were <2.5 in subsequent controls in all of them, allowing continuation of RCA CRRT in all patients.
Acidosis and alkalosis, defined as a base excess (BE) value out of the range between −3 and 3 mmol/L, were documented in the citrate group patients. Before therapy initiation, more than half of the patients presented an altered base excess value. RCA CRRT was associated with an expected rise in BE (Tab. III), with no clinically significant changes in pH (initial mean pH 7.37 ± 0.07; final mean pH 7.43 ± 0.06. Although 4 patients presented metabolic alkalosis (pH>7.5), there were no clinical consequences and they were easily managed by reducing blood flow or increasing dialysis flow as per the manufacturer's protocol. Moreover, as observed in Figure 2, no important differences were observed if these values are compared to the heparin group, with a mean pH value of 7.34 ± 0.1 and 1 case of alkalosis at the beginning of CRRT, and 7.4 ± 0.06 with 3 cases of alkalosis at the end of CRRT.
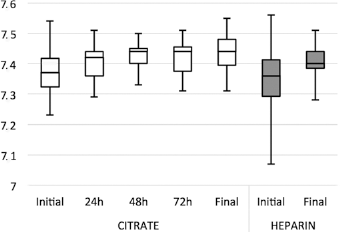
Monitoring results of systemic pH during CRRT in the citrate and heparin groups.
Serum sodium was also monitored during the CRRT, with a mean value of 138.4 ± 4.3 before CRRT initiation. No clinically relevant changes in serum sodium value were documented during the therapy, and there were no cases of hypernatremia (serum sodium >150 mEq/L).
The total CRRT time was 6.0 ± 3.9 days in the citrate group, as compared to 6.1 ± 4.5 days in the heparin group. Unexpectedly, the RCA group presented a longer ICU length of stay (32.5 ± 25.1 days), as compared to 19.6 ± 15.2 days in the heparin group (p = 0.026), a difference explained by the fact that 2 patients in the citrate group had an unusual ICU length of stay of >90 days. On the contrary, there were no differences in hospital length of stay between the groups (57.3 ± 40.5 vs. 43.5 ± 44.1) (p = 0.238). Renal function recovery was similar between groups (66%). Similarly, there were no differences in GFR at ICU discharge (23.5 ± 23.6 mL/min in the citrate group vs. 12.8 ± 16.3 mL/min in the heparin group) and at hospital discharge (24.2 ± 28.0 mL/min in the citrate group vs. 16.3 ± 20.1 mL/min in the heparin group). ICU mortality was the same in both groups (33%) whereas 30-day survival was slightly higher in the citrate group (77% vs. 70%), although the difference was not significant.
Discussion
In this study the implications of RCA implementation in CVVHDF in 3 speciality ICUs from a university hospital were retrospectively evaluated in conditions of everyday clinical practice. As compared to systemic heparin, RCA by infusion of citrate as a separate and concentrated solution prolonged circuit survival and reduced transfusional requirements. In addition, metabolic complications were uncommon and easily manageable. No differences in outcome were observed. These findings confirm that regional citrate is a feasible anticoagulation method for CVVHDF in critically ill patients in clinical practice.
Clinical application of RCA dates back to the 1990s, with a number of studies evaluating this anticoagulation (reviewed in 12–15). Moreover, the Kidney Diseases Improving Outcomes Clinical Practice Guidelines (KDIGO) for AKI have recommended RCA as the method of first choice in CRRT if there is no contraindication to its use (16). However, despite this, widespread use of RCA has been limited because of concern of metabolic complications and the perception of added complexity. Our study confirmed the findings in previous studies that, filter lifetime was prolonged in filters that received RCA anticoagulation. When the cause of circuit interruption is analysed, a higher rate of circuit clotting was observed in the heparin group. In addition, the number of filters used in 72 hours was significantly higher in the heparin group. Although there are a number of studies evaluating RCA in CRRT, the comparison is somehow limited by the heterogeneity with respect to the CRRT modality employed. Most randomized studies have employed CVVH either in postdilution or predilution (5, 8, 9, 11). On the contrary, fewer studies have implemented RCA in CVVHDF, all of which used citrate diluted within a balanced solution for predilution infusion (10, 18–20). It is known that filter patency may be longer when using diffusive (CVVHD or CVVHDF) rather that purely convective techniques (CVVH) and with predilution rather than postdilution replacement (4). Implementation of nonanticoagulant measures such as diffusion may reduce the impact of RCA on circuit patency in clinical practice. In the latest meta-analysis by Liu and colleagues (13) in a prespecified subgroup analysis of studies, using CVVHDF and postdilution did not show any significant impact of RCA on circuit patency as compared to studies using CVVH and prediction.
Our study adds new information to the effect that RCA in the setting of CVVHDF with 100% postdilution replacement increases circuit patency. As compared to previous studies using CVVHDF in patients of similar age and severity, circuit patency was longer for both groups in our study than in the trial of Stucker et al (10), with 49 ± 29 hours in the citrate group and 28 ± 23 hours in the heparin group; it was also longer than in the trial of Gattas et al (18), with 39 hours (95% CI 32–48) in the citrate group and 22 hours (95% CI 13–34) in the heparin group.
Regarding safety, patients in the citrate group had a trend to lower haemorrhagic complications and significantly fewer transfusion requirements, results that are in agreement with most previous studies (12, 13, 15) and probably the strongest argument for recommendations of RCA even in patients with increased bleeding risk.
With respect to metabolic complications, our results show that RCA is safe and metabolic complications are rare when a standardized protocol is used to adapt dialysate flow and calcium substitution in order to maintain blood pH and ionized calcium levels within the normal range. The citrate accumulation incidence is concordant to previously published data (6). In studies using diluted citrate within a balanced prediction replacement solution, the incidence of citrate accumulation (a total calcium/ionized calcium ratio >2.5) is 36%, with 9% (21) and 11% (22) of patients requiring interruption of the technique. In our study, citrate accumulation was detected in 3 of the 27 patients (11%) but no patient required interruption of the technique. Moreover, despite the use of a concentrated citrate solution, no cases of hypernatremia were detected. Similarly, no relevant changes in base excess or pH were detected in the citrate group and the incidence of metabolic alkalosis was quite similar compared to the heparin group. Careful monitoring as per the manufacturer's protocol, with optimal adherence of trained staff nurses and physicians allowed easy correction of the expected metabolic deviations.
Regarding patient outcomes, there were no meaningful differences between the 2 groups. Although there are previous studies that suggest a survival benefit for citrate (11), our study does not show a significant reduction in mortality with RCA use, in agreement with recently published studies (5, 13). In any case, our study does not have sufficient power to demonstrate significant changes in mortality rate.
Our study has several limitations: first of all, the retrospective observational design limits the strength of our conclusions. In addition, the sample size is relatively small for obtaining sufficient power for outcome variables. In addition to the confirmatory nature of the main results with previously published reports, the interest and novelty of our study lie in the application of a specific RCA protocol with CVVHDF, which, to our knowledge, is not represented in the literature, and in the setting of everyday clinical practice.
In conclusion, CVVHDF with RCA can be considered a feasible choice for anticoagulation during CRRT in everyday clinical practice in critically ill patients with no very high risk of bleeding or liver failure. The main advantages of RCA demonstrated in this study are prolonged circuit lifespan and fewer adverse events related to the risk of bleeding and transfusion requirements, compared with systemic heparin anticoagulation. The benefits of less circuit downtime, fewer circuit changes and fewer transfusion requirements support the recommendation of RCA use during CRRT as a first-line treatment in suitable patients. Our results suggest that the implementation of regional citrate anticoagulation using concentrated citrate solutions in the setting of routine clinical practice is feasible, safe and effective.
Footnotes
Financial support: No grants or funding have been received for this study.
Conflict of interest: None of the authors has financial interest related to this study to disclose.