
Abstract
Introduction:
Given that it is difficult to randomize end-stage renal disease (ESRD) patients to either hemodialysis (HD) or peritoneal dialysis (PD), differences between these renal replacement therapy (RRT) modalities are of major interest and remain controversial.
Methods:
All data on maintenance dialysis patients during 2009 to 2013 in the Renji Hospital in Shanghai, China and in the San Bortolo Hospital in Vicenza, Italy were selected. Patients who changed their therapy from HD to PD or PD to HD during this study were excluded.
Results:
919 maintenance dialysis patients were included in the present study, including 509 patients on HD and 410 on PD. During the 5-year follow-up, mean arterial pressure (MAP) was higher in HD patients. The level of serum HCO3- was significantly better in PD patients than in HD patients. Phosphate was significantly higher in HD patients than in PD patients. With respect to lipid metabolism, triglyceride, total cholesterol and LDL were significantly higher in PD patients. Serum protein and albumin were higher in HD patients than in PD patients. Overall, 236 patients died (25.7%); 150 (16.3%) on HD and 86 (9.4%) on PD. The main cause of death in HD and PD patients was cerebral vascular disease and infection, respectively. After adjusting for dialysis vintage, the Kaplan-Meier patient survival was similar between HD and PD patients.
Conclusions:
Based on 5 years of data, we demonstrate that lipid metabolism and nutritional status were better in HD patients. However, blood pressure control, acid-base balance, phosphate (P) control were better in PD patients. The main cause of death in HD and PD was cerebral vascular disease and infection, respectively. Considering the dialysis vintage, the Kaplan-Meier patient survival was similar between HD and PD patients.
Introduction
It is well known that the worldwide trend toward an increasing prevalence of patients with chronic kidney disease (CKD) is leading to a growing threat to public health and healthcare systems (1). Although early detection and intervention to prevent progression of CKD is a public health priority, it is inevitable that the number of people progressing to end-stage renal disease (ESRD) will increase all over the world (2-4).
In high-income countries like Italy, the projected increase in the incidence and prevalence of ESRD is approximately 5% to 8% per annum (3). Where data are available for rapidly developing countries, the projected increase in ESRD patient numbers is as high or higher (5). In China, the growth in the number of dialysis patients has been exceptionally rapid: about 79.1 per million population at the end of 2008 (5).
Although kidney transplantation is the optimal form of treatment for suitable ESRD patients, hemodialysis (HD) and peritoneal dialysis (PD) will remain the mainstay of treatment for patients with ESRD, due to a global shortage in the availability of organs for transplantation (2, 6). Meanwhile, HD and PD are mature and well-established therapeutic methods with the former being carried out by trained staff. To make an evidence-based decision on the dialysis pattern, patients and physicians should be aware of the benefits and risks of the alternative modalities.
Nevertheless, given that it is difficult to randomize ESRD patients to either HD or PD, particularly due to patients’ unwillingness to accept such a procedure, differences between these renal replacement therapy (RRT) modalities are of major interest and remain controversial (7). A randomized controlled trial named The Netherlands Cooperative Study on the Adequacy of Dialysis attempted in 1997-2000 was forced to terminate prematurely because of poor recruitment (7). Up until now, despite obvious limitations, observational studies represent the next best design to evaluate the difference between HD and PD. The key lies in the power of data, such as the size of sample, different races, the duration of follow-up and the number of centers or countries.
The aim of present study was to compare the parameters (for instance demographic characteristics, dialysis vintage, blood pressure, laboratory test, and drug interventions), the main causes of death and 5-year survival outcomes between HD and PD patients in 2 dialysis centers including China and Italy.
Materials and methods
Materials
All surviving maintenance HD and PD patients who started dialysis before January 1, 2009 in Renji Hospital, Shanghai Jiao Tong University School of Medicine, and the International Renal Research Institute of Vicenza at the San Bortolo Hospital were enrolled. These 2 hospitals are affiliated with medical universities in China and Italy. Patients who changed their therapy from HD to PD or from PD to HD or to transplantation during the period between January 1, 2009 to December 31, 2013 were excluded. Since the study was retrospective and patient data were all de-identified, the Ethics Committees of Renji Hospital and San Bortolo Hospital waived the need for written informed consent.
Data collection
The data of the dialysis patients during January 1, 2009 to December 31, 2013 were reviewed by the Renal Registry Network of Shanghai (http://sh.cnrds.org/) and the Renal Registry Network of San Bortolo Hospital. The following information was recorded: demographic characteristics (age, gender and weight), causes of ESRD, dialysis vintage, blood pressure, laboratory test (blood gas analysis, mineral metabolism, blood routine, C response protein, iron metabolism, lipid metabolism, nutrition, glucose and β2-MG), drug interventions (number of antihypertensive drugs’ type including ARB, ACEI, CCB, alpha blockers, beta blockers, diuretic and centrally acting antihypertensive drug, the dose of binder, vitamin D, erythropoietin, iron and statins), outcome (death or survival) and the causes of death. In addition, predialysis weight and BP were collected in HD patients, while in PD patients the weight was without dialysate. Most of the patients in China were treated with oral vitamin D or oral iron (ferrous succinate). All laboratory tests were measured predialysis in hemodialysis patients. We defined the data near January 1, 2009 as the baseline data.
Follow-up
After the patients were enrolled, we started the follow-up on January 1, 2009 and all patients finished 5 years of follow-up unless they died during this study. According to the quality control requirements of dialysis, all HD and PD patients need to be examined and undergo laboratory tests in each 3-month interval. In this study, over 91.6% of the patients were examined 20 times during these 5 years.
Statistical analysis
Results are expressed as frequencies and percentages for categorical variables, mean ± SD for continuous normally distributed variables, and median and interquartile range for continuous non-normally distributed variables. Student’s t-test or the nonparametric Mann-Whitney U-test was used to compare continuous variables between HD and PD groups. The X2 or Fisher’s exact test was used to compare the categorical variables as appropriate. The incidence and mortality were presented by the adoption rate. The Kaplan-Meier patient survival analysis was performed to compare the difference in survival between HD and PD. Statistical analyses were conducted using the SPSS version 20.0 software package. A p<0.05 was regarded as a statistically significant difference.
Results
Comparative baseline data of demographic characteristics, dialysis vintage, blood pressure and laboratory tests
A total of 919 maintenance dialysis patients were included in the present study; 509 patients were on HD and 410 on PD. The proportion of males in HD and PD were 62.7% (n = 319) and 47.8% (n = 196), respectively (p<0.0001). The proportion of patients from the Han ethnic group was 66.6% (n = 339) and 79.3% (n = 325) in HD and PD, respectively (p<0.0001). At the beginning of this study (January 1, 2009), the mean age (years) was 59.34 ± 14.57 in HD and 56.32 ± 15.45 in PD patients (p = 0.002); patient’s weight and mean arterial pressure (MAP) were similar between HD and PD patients (67.32 ± 13.25 kg vs. 65.69 ± 15.50 kg, p = 0.060; 97.00 ± 14.97 mmHg vs. 98.95 ± 13.43 mmHg, p = 0.080); the dialysis vintage (months) of HD patient was significantly longer than that of PD patients (68.34 ± 61.13 vs. 40.38 ± 33.00, p<0.0001). In comparison with PD patients, HD patients had lower bicarbonate levels and blood platelet cell counts. In subgroup analysis including China and Italy, the trend of the above parameters was consistent with the general trend (Tab. I). In HD patients, the proportion of arteriovenous fistula, including grafts and catheters, was 94.7% (n = 482) and 5.3% (n = 27), respectively. The total number of hepatitis viral infection was 76 (14.9%) patients. The proportion of patients with hepatitis B and C was 42.1% (n = 32), 51.3% (n = 39) and 6.6% (n = 5), respectively. There are no patients with active hepatitis.
Baseline data of demographic characteristics, dialysis vintage, blood pressure and laboratory test between HD and PD patients
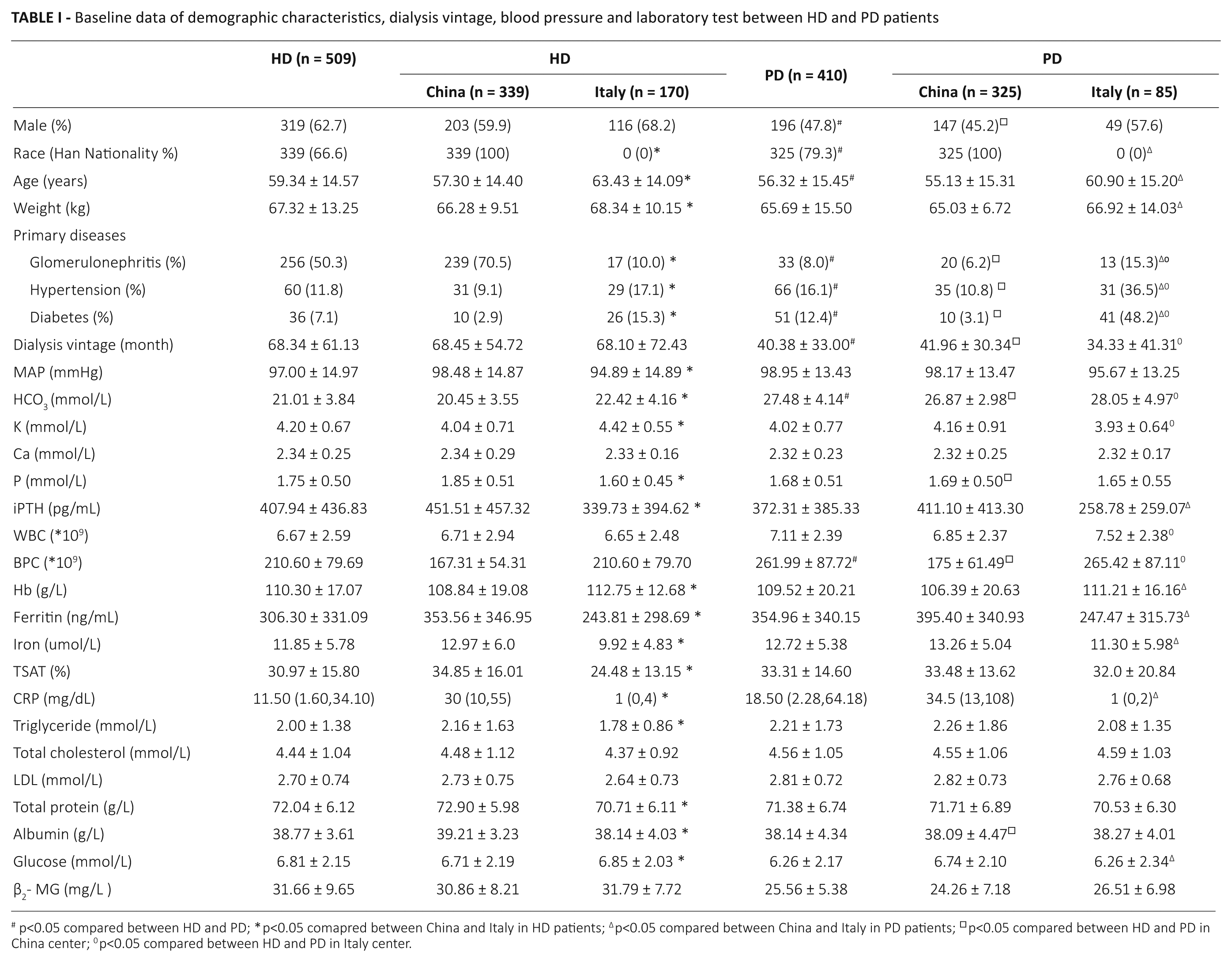
p<0.05 compared between HD and PD; *p<0.05 comapred between China and Italy in HD patients; ∆p<0.05 compared between China and Italy in PD patients; □p<0.05 compared between HD and PD in China center; 0p<0.05 compared between HD and PD in Italy center.
Mean arterial blood pressure, weight and laboratory test values in HD versus PD patients during the 5-year follow-up period
In comparison with PD, and weight were higher in HD patients (100.16 ± 14.54 mmHg vs. 95.11 ± 15.27 mmHg, p<0.0001; 70.96 ± 16.30 kg vs. 61.89 ± 12.13 kg, p<0.0001). The level of HCO3- was significantly higher in PD patients than in HD patients (25.48 ± 4.44 vs. 21.68 ± 4.03, p<0.0001) while the concentrate of serum potassium (K) values were similar (p = 0.236). As for the mineral metabolism markers, phosphate (P) was significantly higher in HD patients than in PD patients (1.66 ± 0.56 vs. 1.55 ± 0.61, p<0.0001) while calcium (Ca) and iPTH were similar (p>0.05 for both). The infection markers, such as WBC and C-reactive protein (CRP), were significantly higher in PD patients than in HD patients (7.47 ± 2.78*109 vs. 6.37 ± 2.71*109, p<0.0001; 3.93 [0.84, 22.23] mg/dL vs. 3.0 [0.91, 12.56] mg/dL, p<0.0001). Hemoglobin (Hb) was significantly higher in PD patients than in HD patients (112.52 ± 17.86 g/L vs. 111.21 ± 15.81g/L, p<0.0001). Conversely, ferritin was significantly lower in HD patients than in PD patients (345.32 ± 377.06 ng/mL vs. 415.03 ± 356.14 ng/mL, p<0.0001). With respect to lipid metabolism, all markers such as triglycerides, total cholesterol and LDL were significantly higher in PD patients than in HD patients (p<0.0001 for all). As for nutrition biomarkers, total protein and albumin were higher in HD patients than in PD patients (69.54 ± 7.91g/L vs. 68.06 ± 7.99g/L, p<0.0001; 39.27 ± 11.24g/L vs. 37.56 ± 5.16g/L, p<0.0001). In spite of using peritoneal dialysate containing glucose, fasting blood glucose (Glu) was lower in PD patients than in HD patients (5.70 ± 2.62 mmol/L vs. 6.15 ± 2.45 mmol/L, p<0.0001). The concentrate of serum β2-MG was similar in HD and PD patients (p = 0.287) during the 5-year follow-up (Tab. II). In subgroup analysis including China and Italy, the tendency of the above parameters was consistent with the overall trend (Tab. II).
The mean value of blood pressure, weight, laboratory test and drug interventions comparing HD and PD patients during the follow-up period of five years
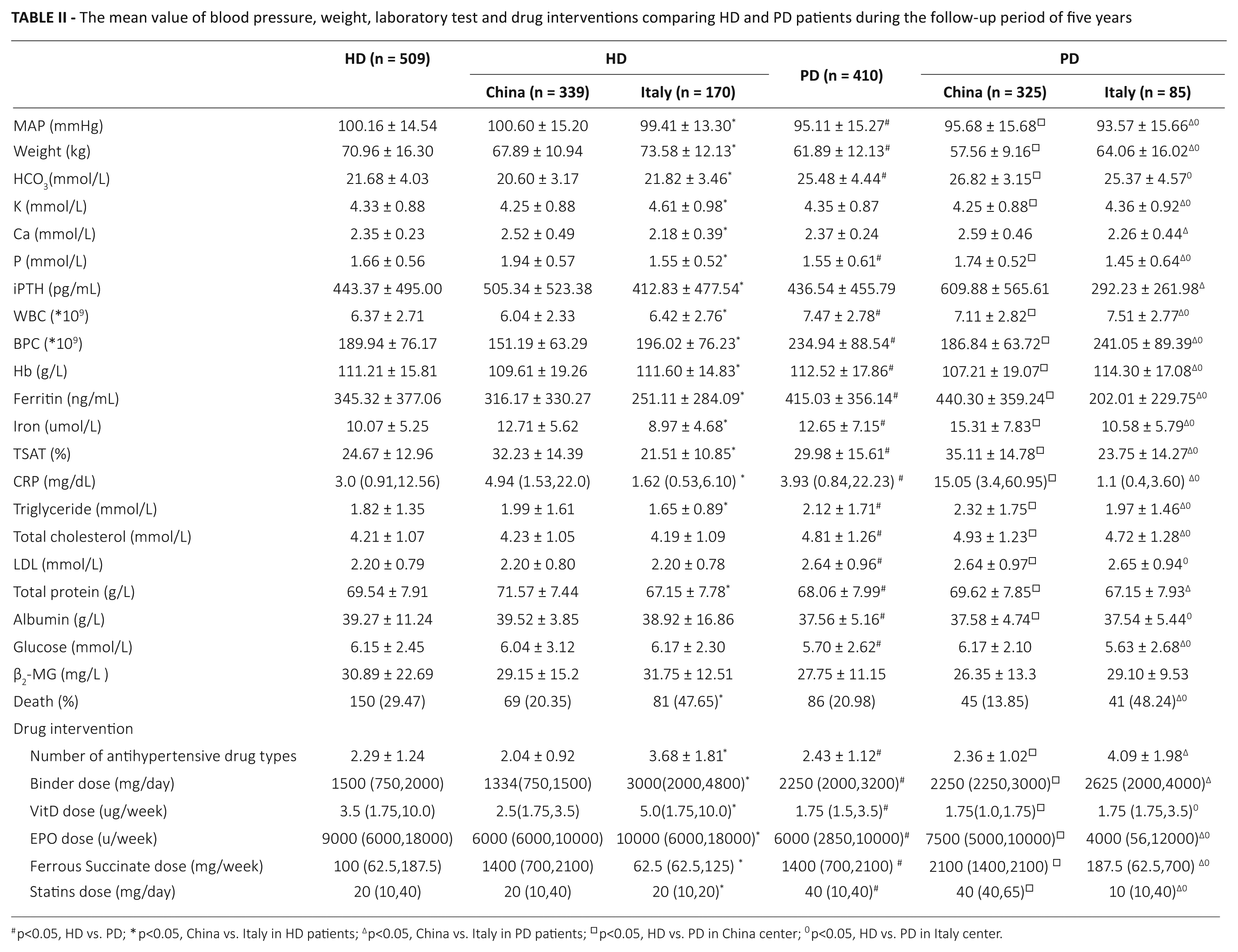
p<0.05, HD vs. PD; *p<0.05, China vs. Italy in HD patients; ∆p<0.05, China vs. Italy in PD patients; □p<0.05, HD vs. PD in China center; 0p<0.05, HD vs. PD in Italy center.
Drug interventions in HD versus PD patients during the 5-year follow-up period
PD patients took more types of antihypertensive drugs than HD patients (2.43 ± 1.12 vs. 2.29 ± 1.24, p = 0.001). The binder dose was significantly higher in PD patients than in HD patients (2250 [2,000, 3,200] mg/day vs. 1,500 [750, 2,000] mg/day, p<0.0001) while the dose of activated vitamin D (Vit D) was significantly lower in PD patients than in HD patients (1.75 [1.5, 3.5] ug/week vs. 3.5 [1.75, 10.0] ug/week, p<0.0001). HD patients received higher doses of erythropoietin (EPO) (9,000 [6,000, 18,000] u/week vs. 6,000 (2,850, 10,000) u/week, p = 0.001]. Conversely, HD patients received lower doses of ferrous succinate [100 (62.5, 187.5) mg/week vs. 1,400 (700, 2,100) mg/week, p<0.0001). PD patients needed to take higher doses of statins than HD patients (40 [10, 40] mg/day vs. 20 [10, 40] mg/day, p = 0.004) (Tab. II). In the subgroup analysis of the two groups including China and Italy, the trend of the drug interventions was similar to the general tendency (Tab. II).
Mortality and the cause of death in HD versus PD patients
During follow-up, 236 patients died (25.7%), including 150 on HD and 86 on PD; the mortalities were 29.47% and 20.98% in HD and PD patients, respectively. The top 3 causes of death in HD patients were cerebral vascular disease, including ischemic or hemorrhagic stroke (34.8%), infection (20.3%) and cardiovascular disease (14.5%). In PD, infection (28.9%) was the main cause of death, followed by cerebral vascular disease (17.8%) and cardiovascular disease (17.8%). The 1-year patient survival rate was 91.4% in HD patients and 93.2% in PD patients (p = 0.326), the 2-year survival rate 85.5% and 86.8% (p = 0.567) and the 5-year survival rate 70.5% and 79.0% (p = 0.004), respectively (Tab. III). The survival trend was consistent with the general trend in the subgroup analysis including China and Italy (Tab. III).
Survival rate between HD and PD patients
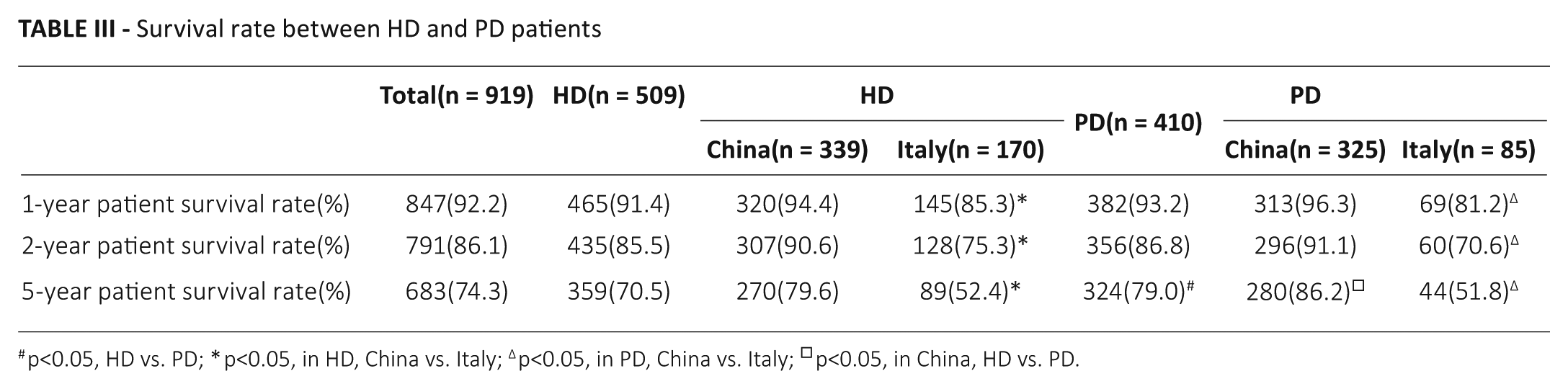
p<0.05, HD vs. PD; *p<0.05, in HD, China vs. Italy; ∆p<0.05, in PD, China vs. Italy; □p<0.05, in China, HD vs. PD.
The Kaplan-Meier patient survival analysis between HD and PD patients
After adjusting for dialysis vintage, the Kaplan-Meier patient survival was similar between HD and PD patients (p = 0.832) (Fig. 1).
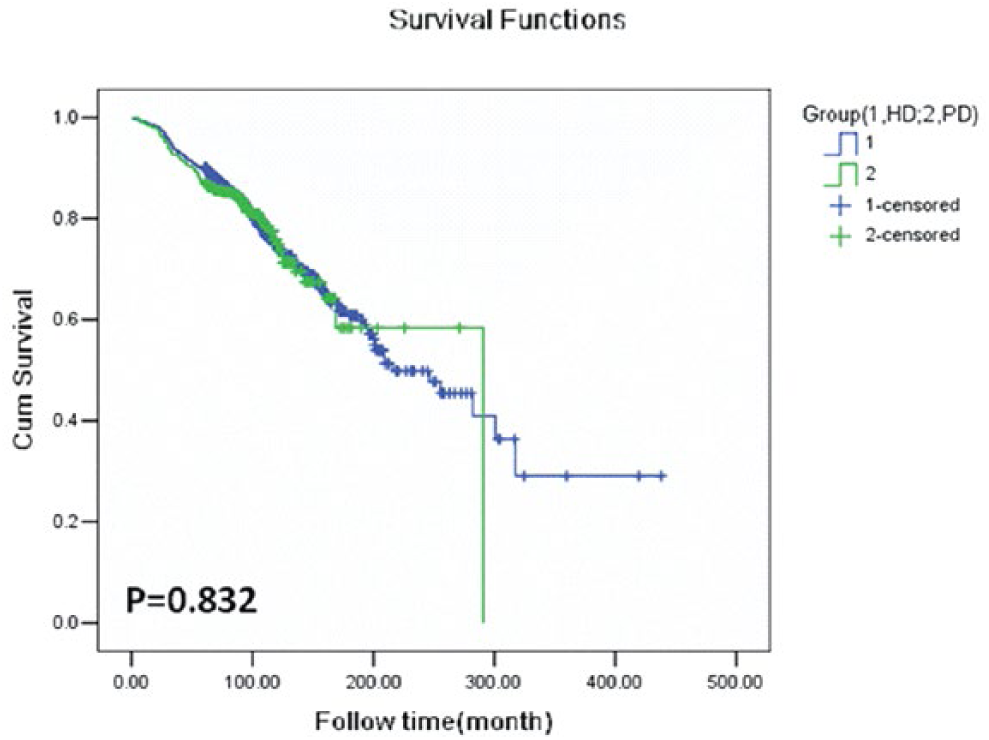
The Kaplan-Meier patient survival analysis after adjusting for dialysis vintage.
Discussion
The present study adopted a real-world design for 2 international incident dialysis populations including China and Italy, followed for 5 years, and compared the differences between HD and PD patients.
Based on 5 years of data, our results show that the lipid metabolism was better in HD patients. Kanbay et al (8) performed a study to determine the effect of dialysis type on serum lipid levels. They found that the maintenance PD treatment is associated with more pronounced alterations of the lipid metabolism than those observed during HD treatment. In our study, we also observed that even if PD patients take higher doses of statins than HD patients, the lipid metabolism markers such as triglycerides, total cholesterol and LDL were significantly higher in PD patients than in HD patients during the 5 years of follow-up. As we all know, dyslipidemia is one of the main risk factors of vascular atherosclerosis, which can lead to cardiovascular or cerebrovascular events among the general population (9). However, the latest epidemiological data has shown that hypercholesterolemia appears to be a protective feature that is associated with greater survival among ESRD patients, leading to it being referred to as a “reverse epidemiology” (10). Our research found that cerebral vascular disease is the main cause of death in HD and that the 5-year survival rate was a little bit better in PD than in HD (79.0% vs. 70.5%, p = 0.004), perhaps due to the hypercholesterolemia in PD patients.
It is undeniable that hypertension is a common complication in dialysis patients and that it is often inadequately controlled. Agarwal et al reported that control of hypertension in dialysis patients is inadequate, despite the frequent use of antihypertensive drugs (11). In this context, according to the 2005 National Kidney Foundation Kidney Disease Outcomes Quality Initiative (NKF-KDOQI) guidelines (12), we found that the management of blood pressure (BP) in these 2 international dialysis centers reached the target value (<140/90 mmHg) in both HD and PD patients. Furthermore, our study showed that MAP was significant higher in HD patients than in PD patients. Interestingly, PD patients took a greater number of antihypertensive drugs than HD patients. The main reason may be that BP fluctuates during hemodialysis process, especially before dialysis, due to volume overload (13). This indicates that using conventional predialysis BP recordings may be problematic. Therefore, the 2017 European Renal Association-European Dialysis and Transplant Association (ERA-EDTA) and the European Society of Hypertension (ESH) guidelines recommend an average home BP <135/85 mmHg (MAP <101.7 mmHg) in dialysis patients instead of a predialysis BP of <140/90 mmHg (the 2005 NKF-KDOQI guidelines) (14). Importantly, many recent observational studies of BP and mortality in dialysis patients have shown that survival is significantly better among patients with a predialysis SBP of 130 to <160 mmHg (15). Furthermore, an increased risk of death in dialysis patients was associated with low, but not high, BP levels (16, 17). This corroborates accumulating evidence from clinical studies in dialysis that intradialytic hypotension-induced myocardial stunning may contribute to the development of heart failure and increased mortality (18, 19). Therefore, due to the paucity of evidence-based data, recent KDIGO guidelines for BP management did not recommend BP goals for dialysis patients (20, 21). Ongoing controversies in ideal BP management in the context of dialysis are highlighted along with key areas for future research.
Metabolic acidosis is very common in ESRD patients, with deleterious consequences on their nutritional status, inflammation and mortality. Serum bicarbonate administration in dialysis patients is determined by several factors that include dietary protein intake, nutritional status and dialysis prescription, and especially dialysate. Based on 5 years of data, we demonstrate that the level of serum bicarbonate was significant lower in HD patients than in PD patients. A recent study indicates that higher protein intake may lead to lower serum bicarbonate level in patients treated with dialysis. The interpretation may be related to adequate dietary protein intake that may produce more acid generation and lead to a lower serum bicarbonate level (22). This phenomenon was confirmed in our study, since the nutritional status was better in HD patients than in PD patients. Conversely, the serum bicarbonate level was lower in HD patients. In addition, we do not deny the fact that serum bicarbonate fluctuates in HD patients and that the concentration in predialysis is the lowest. Therefore, a high predialysis serum bicarbonate concentration should prompt nephrologists to perform nutritional investigations to detect insufficient dietary protein intake (23). Moreover, the DOPPS study points out that moderate predialysis acidosis (serum bicarbonate concentration 16-24 mEq/L) seems to be associated with better nutritional status and lower relative risk for mortality or hospitalization (24). In other words, both excessively low as well very high levels of serum bicarbonate have been associated with adverse outcomes in this population (25). Until now, there are no prospective studies available that have examined the association of serum bicarbonate with mortality in dialysis patients. Hence, the optimal level of serum bicarbonate in dialysis patients needs further study to be confirmed.
Hyperphosphatemia is a common complication of ESRD patients and likely promotes calcification of the myocardium, valves, and arteries. It has been associated with arterial dysfunction (26) and all-cause mortality (27, 28). In this retrospective observation, we found that serum phosphorus control was better in PD patients, although the calcium and iPTH levels were comparable. The higher doses of phosphate binders taken by PD patients may be the most likely reason. In fact, protein intake and residual renal function are also associated with the serum phosphorus level. The protection of RRF was better in PD patients than in HD patients. Moreover, Wang AY, et al demonstrated the importance of RRF in maintaining serum phosphorus levels in PD patients (29). However, one of the limitations of this study is that the residual renal function or normalized protein catabolic rate was not available and we cannot estimate whether these 2 factors affected the observed outcome.
It is well recognized that infection is one of the common complications in dialysis patients, such as bloodstream infections related to vascular access in patients undergoing HD and peritonitis in patients undergoing PD (30). Johnson et al found that PD treatment was associated with an increased risk of death from infection compared with HD in Australia and New Zealand. The excess risk of this finding was accounted for by an increased occurrence of fatal peritonitis (31). In our current study, we also found that PD patients might have more chance of infection, and the main cause of death in PD is infection. Further attention to infection control management in PD patients would also appear warranted.
Over the past decade, the survival outcomes between patients receiving HD and PD have been compared in several large-scale epidemiological observational studies (32-36). Although the conclusions from these studies were varied and sometimes confusing to the nephrology community, the majority indicated that there was no evidence for a difference of survival rates between the two modalities (37). In these studies, some differences that existed within the distinct subgroups of the patients, such as suboptimal adjustment for differential modality, switch over time (because PD patients are more likely to switch to HD than HD patients are likely to switch to PD over time) (37). Therefore, in our study, patients who changed their therapy from HD to PD or PD to HD or to transplantation during the study period were excluded. In terms of overall survival, considering to dialysis vintage, the Kaplan-Meier method and log-rank test showed that there were no statistical differences between HD and PD patients during the 5-year follow-up period (Fig. 1). Therefore, our study corroborates the current consensus opinion that HD was associated with a similar risk of mortality compared to PD. The interesting finding is that in comparison with the Italian group, the survival rate is higher in Chinese patients on either HD or PD. The main reason may be that the age is older in the Italian group than in the Chinese group on either HD (63.43 ± 14.09 vs. 57.30 ± 14.40, p<0.05) or PD (60.90 ± 15.20 vs. 55.13 ± 15.31, p<0.05). Furthermore, it may be due to the primary disease of ESRD. The proportion of diabetic patients is much higher in the Italian group than in the Chinese group on either HD (15.3% vs. 2.9%, p<0.05) or PD (48.2% vs. 3.1%, p<0.05). It is universally acknowledged that the mortality of diabetic dialysis patients is high (38). So we cannot conclude that the survival rate is better in the Chinese group than in the Italian group on either HD or PD.
Nevertheless, there are several limitations to our study, as follows. First, baseline conditions were not completely matched in the 2 groups, such as gender, age, dialysis vintage, etc. Second, this study did not record the fluctuation data of serum albumin, hemoglobin, serum phosphorus, etc. Therefore, the risk factor analysis of these parameters could not be carried out. Third, the current observational study calculated the statistic for causes of death; however, multivariate logistic regression analysis was not used for analyzing the risk factors for prognosis in the 2 groups. Fourth, it was not suitable for this study to use WBC and CRP to represent infection in HD and PD patients. Fifth, regarding drug interventions, this study only analyzed the dose of drugs rather than the type of drugs.
Despite its limitations, this real-world study indicated the difference between HD and PD patients in these 2 international dialysis centers. Based on the analysis of these 5 years of data, we demonstrated that lipid metabolism and nutrition were better in HD patients. However, BP control, acid-base balance, P control and the concentration of Hb and iron were better in PD patients. PD patients might have more chance of infection. The main cause of death in HD and PD is cerebral vascular disease and infection, respectively. Considering the dialysis vintage, the Kaplan-Meier patient survival was similar between HD and PD patients. There is also a need for good-quality evidence in this important area, specifically randomized, controlled clinical trials.
Footnotes
Acknowledgements
The authors wish to acknowledge that this study was initiated during the international fellowship of Renhua Lu at the Department of Nephrology, Dialysis and Transplantation, San Bortolo Hospital, Vicenza, Italy, of which Claudio Ronco is the department director.
Disclosures
Financial support: This study received the following grants: Natural Science Fund of the Xinjiang Uygur Autonomous Region (2016D01C094); Shanghai Science and Technology Commission (17695840500); Shanghai Science and Technology Commission (15ZR1425900); Natural Science Fund of the Xinjiang Uygur Autonomous Region (2015211C228).
Conflict of interest: None of the authors has financial interest related to this study to disclose.