
Abstract
We present a case of a stone discovered in a vesicovaginal fistula after a total abdominal hysterectomy.
Case
A 53-year-old woman presented with complaints of severe urinary incontinence, dyspareunia, and post-coital bleeding after hysterectomy. Her partner reported pain with intercourse as well. Physical examination revealed urinary stone wrapped around permanent suture within the vesicovaginal fistula tract. Patient was taken to the operating room for repair of the vesicovaginal fistula, anterior colporrhaphy and cystoscopy.
Introduction
Vesicovaginal fistula is a communication between the vagina and bladder, causing continuous urinary leakage and vaginal discharge. They most commonly occur in developing countries due to obstructed labor (1). Approximately three million women around the world have unrepaired vesicovaginal fistulas, and 30,000-130,000 new cases occur in Africa each year (2). Vesicovaginal fistulas in developed countries are usually the result of malignancy and radiation therapy. It is an uncommon complication of hysterectomy. Vesicovaginal fistulas have been reported to occur in 0.25% of abdominal hysterectomies and 0.05-0.6% in vaginal hysterectomies (3). This is a case of a urinary stone formation inside the canal of the vesicovaginal fistula. Currently, there has not been published case of stone formation within the fistula canal itself.
This patient is a 53-year-old G4P4 who presented with urinary incontinence, lower abdominal cramping, and vaginal spotting for two years following a total abdominal hysterectomy for heavy vaginal bleeding. Her pain was unrelieved with standard non-steroidal anti-inflammatory drugs (NSAIDs) and narcotics. Urinary incontinence started two weeks after her hysterectomy. She describes symptoms consistent with stress incontinence with losing small to large amounts of urine requiring her to wear 3-12 diapers daily. Her incontinence is worse when she has pelvic pain. She reports feeling air come out of her urethra before her urinary streams and vaginal bleeding after penetration with intercourse. She had only had intercourse twice after her hysterectomy, and her partner felt that he “was being cut with a knife.”
She was seen in our Pelvic Health Center. Her post-void residual (PVR) was 50 cc at her initial clinic visit. Urine dip was positive for nitrates. On physical examination in the clinic with placement of the speculum, a calcification wrapped around suture exiting from the right vaginal cuff apex was discovered. There were two stones wrapped around Ethibond suture measuring a total of 5 cm and was continuous with the vesicovaginal fistula tract (Fig. 1). The suture was grasped and cut to remove the suture and stones. Granulation tissue noted at the right angle of the cuff. Cystoscopy was performed immediately with flexible cystoscope. The ureters were visualized with good efflux bilaterally. Vesicovaginal fistula was confirmed on cystoscopy and was present at the bladder base between the urethral orifices. Bladder neck and urethra appeared normal. Patient was given Bactrim DS for urinary tract infection (UTI). Urine culture returned positive for Escherichia coli, sensitive to current treatment plan.
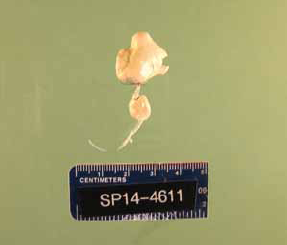
Genitourinary stone around Ethibond suture within vesicovaginal fistula.
The patient was taken to the operating room for repair of vesicovaginal fistula using the method previously described (4). Anterior coloporrhaphy and cystoscopy were also performed. The fistula was identified in the midbase of the bladder 2-3 cm from each ureteral orifice. A 16 French transuretheral catheter was placed at the beginning of the procedure. An 8 size French Foley catheter was inserted into the fistula tract. Inverted U incision was made on the anterior wall of the vagina, circumscribing the fistulas tract with the long end of the incision extended toward the vaginal apex. Dissection was performed along the anterior and posterior flaps. Monocryl was used to close the bladder mucosal layer. The 8 French catheter was removed and sutures were tied to close the fistulous tract. A free peritoneal flap including pre-peritoneal fat was developed and advanced over the posterior bladder peritoneum to cover the fistula repair. Repair was water tight at the end of the procedure. The patient's postoperative course was uneventful. She was discharged on POD #1 with an indwelling Foley for two weeks. On post-operative week 6, the patient presented for follow-up visit. Her incontinence resolved and pelvic pain had improved. Operative cystoscopy and vaginoscopy were performed and revealed normal findings. No defects, stones, or sutures were detected.
Discussion
In our case, the patient had a hysterectomy with permanent Ethibond suture. Operative records were not available but we presume that the permanent Ethibond suture was meant to be used at the angle for support and was sutured through the bladder during closure of the cuff. This highlights the importance of adequate dissection of the bladder. As abdominal surgeries are the major cause of vesicovaginal fistula in the USA, the addition of using permanent suture would increase the risk of fistula formation, especially near the vaginal cuff. Additionally, any pelvic surgery, such as a sacral colpopexy, using permanent suture near the bladder would increase the risk of vaginal suture erosion and possibly fistula formation. An alternative is to use delayed absorbable suture such as monofilament polydioxanone (PDS). Any patient with a history of a previous surgery with permanent suture, incontinence, persistent pain, recurrent urinary tract infections, or copious discharge should warrant further investigation. A cystoscopy in addition to a thorough vaginal examination is recommended to assess for fistula tract formation.
Footnotes
Financial support: No financial support was received for this case.
Conflict of interest: No conflict of interest to disclose.