
Abstract
Purpose
To evaluate the impact of bowel endometriosis surgery on obstructive defecation syndrome symptoms, bladder dysfunction, pain symptoms and quality of life (QOL).
Methods
This was a retrospective cohort study of patients who underwent surgery for endometriosis where bowel was involved between 2005 and 2013. Patients were grouped according to extent of bowel endometriosis treatment: Group 1 - no treatment of bowel endometriosis, Group 2 - “shaving” of endometriosis, Group 3 - wedge resection, or Group 4 - segmental bowel resection. Data were collected via chart review and a mail-out survey consisting of six validated questionnaires designed to evaluate the study aims.
Results
Of 337 eligible patients, completed survey responses were returned by 99.
There were 22 patients in Group 1, 61 in Group 2, 5 in Group 3 and 11 in Group 4. Patient demographic data were similar across the groups. There was no difference in disease severity between Groups 1-4, nor between respondents and non-respondents. Patients in Group 4 were more likely to have open surgery (p<0.001) and to have a stoma placed (p = 0.001). Patients in Group 3 were more likely to have dysmenorrhoea post-operatively (p = 0.02). Otherwise, bowel and bladder symptoms, pain, and health status were comparable between the groups, with a low incidence of bladder symptoms, generally low pain scores, and high QOL for all patients.
Conclusions
Deciding the extent of surgical aggressiveness based on symptom severity has resulted in similar long-term post-operative bowel and bladder symptoms, pain scores, quality of life and overall health across the groups.
Introduction
The prevalence of endometriosis is estimated to be 10%-15% in women of reproductive age (1). Endometriosis involving bowel is seen in a subset of 5%-12% of the endometriosis population (2-3-4-5-6); the rectum and sigmoid colon are the most frequently involved portions. Symptoms of endometriosis vary but include dysmenorrhoea, menorrhagia, pelvic pain, dyspareunia, cyclical pain on defecation, pain with a full bowel, stabbing rectal pains, urinary frequency, dysuria, or pain with a full bladder (7, 8). There are a proportion of women who are asymptomatic. If symptoms are impacting on quality of life (QOL) then management options include analgesia, hormonal manipulation or surgery.
Surgery for rectal endometriosis may involve ‘shaving’ of disease off bowel, excision of a small area (wedge) of anterior bowel wall or segmental resection. Complete excision of endometriosis has been found to provide long-term symptomatic relief (9-10-11-12); however, it is not without its complications. Surgical procedures extending to the pelvic side-wall may damage the autonomic nerve supply to the bladder, with dysfunction seen after both local excision of endometriosis and radical rectal resection (13). One systematic follow-up study including both techniques found transient voiding problems in almost all patients (14). Studies have demonstrated acute urinary retention in 6%-25% of patients after segmental rectal resection (3, 8, 10, 15-16-17); a recent review reported that the incidence of temporary bladder dysfunction after segmental resection was 8.1% (18).
Whilst studies of urinary symptoms tend to focus on the immediate post-operative period, unwanted complications may persist for significant periods of time. One study (3) reported that 25% of the patients experienced bladder atony and some were still self-catheterising after 12 months. Another study reported a mean self-catheterisation time of 120 days (19). Classically, it has been thought that post-operative bladder dysfunction is due to damage to the splanchnic (parasympathetic) pelvic nerves. However, one group postulates that in fact the most frequent aetiology of bladder retention may be chronic myogenic destruction due to chronic bladder over-distention in the setting of damage to sympathetic pelvic nerves (20). A potential confounding issue is the uncertainty about what effect, if any, the severe endometriosis disease itself, has on bladder function.
The effect of the presence of rectal endometriosis on function has been explored with anal manometry (21), and has been associated with raised internal anal sphincter tone and the symptom of incomplete defecation. Immediate complications recorded after a wedge or segmental resection for endometriosis have included anastomotic stricture, anastomotic leak, anastomotic bleeding, adhesive small bowel obstruction, and pelvic collection (7). Long-term bowel functional changes have included faecal frequency (7), constipation and alternating constipation and diarrhoea (22), with possible aetiologies including changed transit time, anastomotic stenosis, colonic intussusception and neurological damage.
The aim of this survey was to identify whether or not the extent of surgical resection of deep infiltrating bowel endometriosis results in long-term differences in bowel and bladder function, pain symptoms, and subsequent QOL.
Methods
This was a retrospective cohort study (Canadian Task Force Classification II-2) of patients who underwent surgery for endometriosis between 2005 and 2013, where bowel was involved. Ethics approval was obtained through the Royal Women's Hospital Human Research Ethics Committee (Project no. 13/33).
Cases were identified by searching through surgical coding allocations for English-speaking patients over the age of 16 years with recto-sigmoid bowel endometriosis who underwent surgery at a tertiary referral hospital in Melbourne or through a private gynaecologist's practice. Valid participants were mailed a survey inviting them to participate in the study; participation in the study was voluntary with an opt-out option. Patients were excluded if they had insufficient English to consent to the study or if they declined participation. To improve response rates, patients who did not return surveys were sent a second survey invitation 6 months after the first. Where patients had missed a question in a returned survey, they were phoned and asked to complete the question. If a respondent with missing data was uncontactable, the missing response was replaced with the median value for that data point.
All patients recruited had previously undergone a laparoscopic or open procedure with a gynaecologist who had advanced laparoscopic training of more than 2 years and was experienced in treating endometriosis involving the bowel. When a bowel resection was performed (wedge or segment) a colorectal surgeon was also present to perform this part of the operation.
Patients were grouped under the following criteria: Group 1: patients in whom bowel endometriosis was seen but not treated (control); Group 2: patients in whom bowel endometriosis was resected, by “shaving” of disease to the level of bowel serosa but who had some residual disease; Group 3: patients in whom endometriosis was fully resected by excision of a rectal wedge; and Group 4: patients in whom endometriosis was fully resected by segmental resection of bowel. Patients were encouraged to choose their intervention based on the severity of their bowel symptoms, with excision of bowel (Groups 3 and 4) limited to those whose symptoms were significantly impairing their QOL.
Medical records of consented participants were reviewed to collect demographic information consisting of age at surgery, BMI, gravidity, parity, pre-operative symptoms, imaging results, surgical details, and post-operative review. Operation reports and histopathology were used to determine the American Fertility Society (rAFS) score and stage (23).
Patient Survey
Surveys were sent to patients between late 2013 and early 2015. The survey consisted of six validated questionnaires designed to evaluate the impact of surgery on bowel function, bladder function, pain symptoms, QOL and overall health. Along with the survey, a covering letter introducing the study and consent plus opt-out forms were sent.
Bowel symptoms were assessed with three validated questionnaires comprising; a modified Cleveland Clinic constipation score (24) which ranged from 0 to 17 (with a higher score equating to worse constipation), the 5-item obstructive defecation syndrome (ODS score) (25) for ODS ranging from 0 to 20 (with a higher score indicating ODS), and the Cleveland Clinic faecal incontinence score (26) ranging from 0 to 20 (with a higher score equating to worse function).
Bladder symptoms were assessed using the Core Lower Urinary Tract Symptom Score (CLSS) (27). The CLSS ranges from 0 to 44 with a higher score indicating worsening bladder function. It assesses several domains of voiding function (urgency, urge incontinence, stress incontinence, slow stream, straining, incomplete emptying, daytime frequency, nocturia) as well as bladder and urethral pain.
Pain was assessed using visual analogue pain scales (VAS) for dysmenorrhoea, non-menstrual pelvic pain, dyspareunia, dyschezia and pain with a full bladder. The scale was a 10 cm line with the ends labelled “no pain” and “worst possible pain”. Patients were asked to score the worst pain they had experienced in the 3 months preceding the questionnaire and scales were measured to the nearest 1 mm.
Finally, QOL was assessed using the EuroQol (EQ-5D)-5L instrument (28). The EQ-5D instrument has two components: EQ-5DIndex quantifies health state in terms of five dimensions (mobility, self-care, usual activity, pain or discomfort, and anxiety or depression), and the EQ-5DVAS generates a self-rating of current health-related QOL on a VAS. Both components are based on the health of the patient on the day they complete the questionnaire.
Statistical Analysis
As most data were not normally distributed, medians with 5th and 95th centiles were used to describe variables. Continuous variables were compared using Mann-Whitney U-test (2 groups) and the Kruskal-Wallis test (>2 groups). The Chi square test (with Yates correction) or Fisher's exact test were used as appropriate to compare proportions. A p value <0.05 was considered statistically significant. Analysis was performed with SPSS 22.0 (SPSS, Inc., Chicago, IL).
Results
We identified 337 patients who were eligible for participation in this study. Of these, 186 patients were from the tertiary referral centre, and 151 were from a private practice. After completing our mail-out, we received 121 survey responses (a response rate of 36%) with 99 of these consenting to participate. The distribution of patients and their responses can be seen in Figure 1. There was no significant difference in the demographics, duration of follow-up, type of operation, or rAFS score between respondents and non-respondents; however, private patients were more likely to be respondents (p = 0.04).
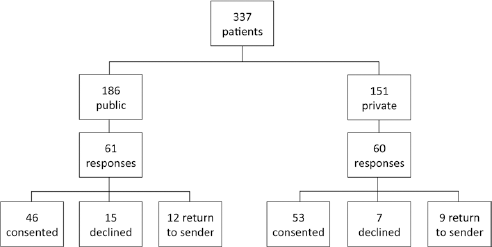
Responses to survey mail-out. Public patients are those treated at the tertiary referral centre, while private patients are those treated by the private gynaecologist.
Twelve patients had incomplete questionnaires and required a follow-up phone call. We were unable to reach three of these and elected to use a median value in place of their data. One patient was missing data for “bowel motions per month” and “urethral pain”. Another was missing data for “bowel motions per week” and “bowel motions per month”. The final patient had missed one page relating to bowel symptoms.
Of the 99 consenting respondents, 22 patients had bowel endometriosis that was not treated (Group 1); 61 patients were treated with shaving (Group 2); 5 patients underwent wedge resection (Group 3) and 11 patients had segmental bowel resection (Group 4). Demographic data, surgical variations, pre-operative symptoms and the rAFS score and stage obtained from the medical record retrospectively are shown for all groups in Table I. The median time to follow-up between surgery and the questionnaire was 3.9 years. There was no significant difference between the rAFS stage of endometriosis between the groups; however, there was a difference in pre-operative symptoms. Of note, the patients in Group 3 had significantly higher rates of menorrhagia. Patients in Groups 3 and 4 had significantly greater rates of dyschezia. Patients in Groups 1 and 2 had higher rates of bladder pain but this was not statistically significant.
Patient demographics, surgical details and pre-operative symptoms
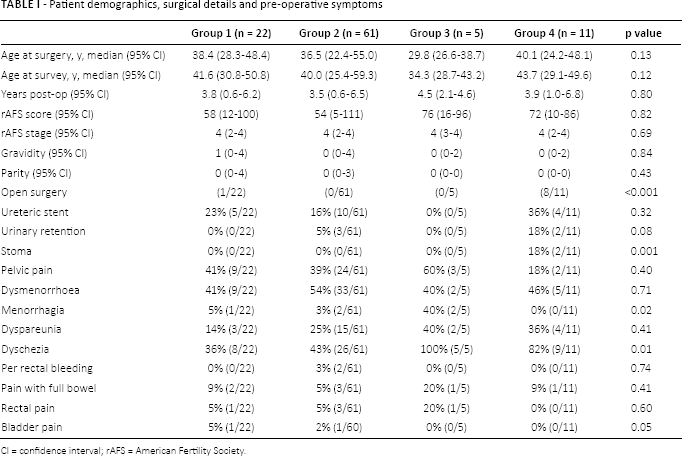
CI = confidence interval; rAFS = American Fertility Society.
Most patients had a laparoscopic approach (n = 90) (91%). Patients undergoing segmental bowel resection were significantly more likely to have an open procedure as a reflection of the preference of the colorectal surgeon (n = 8) (73%), and were also significantly more likely to have a stoma created.
There was one open surgery in Group 1 – a mini-laparotomy to complete a myomectomy.
The rate of urinary retention post-operation was low. Three patients in Group 2 and two patients in Group 4 had difficulty urinating post-operatively. One patient required intermittent self-catheterisation for 3 months. One patient in Group 2 had a bladder injury at the time of surgery and required an indwelling catheter post-operatively until a cystogram confirmed no urine leak.
Table II shows the results of the validated bowel and bladder questionnaires. No significant differences were seen between the groups. In particular there was no difference in ODS scoring or in scoring for bladder dysfunction. Patients with segmental bowel resection appeared to have increased bowel frequency and faecal incontinence, but this result was not statistically significant.
Scores for bowel function questionnaires and bladder symptoms (median score with 95% confidence intervals)
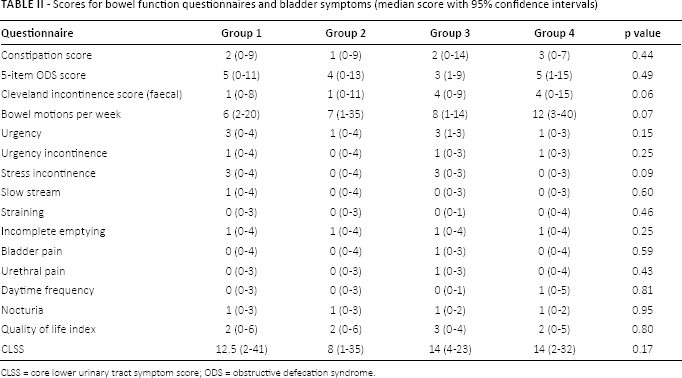
CLSS = core lower urinary tract symptom score; ODS = obstructive defecation syndrome.
The results for the VAS scores and the EQ-5D questionnaire are summarized in Table III. There was no difference between the groups apart from significantly increased dysmenorrhoea scores in patients with bowel wedge resection. Generally, pain scores were low in all categories for all the patients. Overall there was no significant difference in the health status of the survey population. Generally, there was a high QOL among respondents.
Current symptom VAS scores (0 to 100) and EuoQol questionnaire scores (anxiety/depression and pain/discomfort scales 0 to 5; health score [0 to 100])
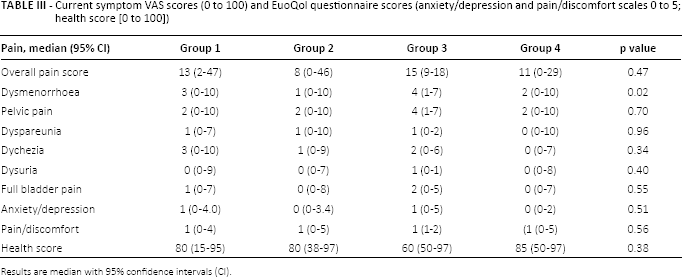
Results are median with 95% confidence intervals (CI).
We then combined the data from Groups 1 and 2, and compared this against the combined data from Groups 3 and 4 (results not shown) in order to see if those patients with minimally treated disease had different symptoms from those with more extensive intervention. The median time of follow-up was still equivalent (4 years for both groups). The increase in bowel motions per week (p = 0.014) and Cleveland Clinic faecal incontinence score (p = 0.007) became significant for the bowel resection group (Groups 3 and 4).
Discussion
There are four major limitations to this study. The first is that the pre-surgery data collection is retrospective and so was not standardised. This recognised limitation of retrospective research limits the ability of our study to make conclusions regarding causation of surgical intervention on the change in QOL and symptom scores pre- and post-surgery. However, we are still able to make a comparison between the absolute QOL and symptom scores between the surgical groups.
The second limitation is that the four treatment groups, although all having bowel endometriosis of a similar stage, differed pre-operatively in symptom severity, a clear selection bias. It is interesting that with the linking of aggressiveness of surgical intervention with symptom severity, the long-term outcome (symptoms and QOL) are so similar across the four groups. This is supportive evidence that not all bowel endometriosis requires complete surgical resection, as previously shown by Fedele et al (29). Allowing symptomatology rather than disease severity to determine the extent of surgery results in similar long-term outcomes without the potential morbidity of more radical surgery, which might require a laparotomy and the creation of a stoma.
The third limitation of our study is that despite repeated mail-outs, we had a relatively low response rate of 36% with small group sizes. In particular, there were low numbers in the wedge and segmental bowel resection groups so it is possible that the responders in these groups are not representative. This is a significant weakness in our study and is a major potential source of bias. These group sizes were too small to allow the use of multivariate analysis, hence potential confounders were listed in Table I.
The final limitation and potential confounder in our study was the exclusion of non-English-speaking women. This decision reflected the lack of resources available for translating questionnaires and patient information and consent forms. The catchment for our hospital is particularly diverse. Despite this, within the recruiting gynaecology clinic less than 10% of patients require or request translation services, indicating a high rate of English utilisation across multiple ethnic backgrounds. The literature provides conflicting data for ethnic and racial differences in endometriosis. A recent review on the topic (30) concluded that significant deficits exist in identifying racial and ethnic differences in the incidence of endometriosis and that further research is needed to better define any differences.
An advantage of the current study is the inclusion of a control group (Group 1) where bowel endometriosis has been left untreated. This provides an opportunity to measure the baseline effect that the presence of bowel disease has on bladder and bowel function and make a comparison with surgical intervention. We have found no evidence that any of the surgical interventions (shaving, wedge resection or segmental resection) resulted in a change in long-term bladder function. In addition, it didn't produce a change in scoring for ODS. The increased bowel motion frequency seen with segmental bowel resection has previously been noted by Brouwer and Woods (7) where 9% of patients described either faecal frequency or urgency.
There are many studies published looking at series of patients following radical surgery for endometriosis. The outcomes focused on to date have been reduction in pain severity, disease recurrence and short-term complications such as anastomosis leak rates (7, 31). There is scope to start looking at other outcomes both with function of the bowel and also nearby organs such as the bladder and vagina.
The wedge resection employed to excise smaller bowel endometriosis lesions is similar to a stapled trans-anal rectal resection (STARR), which is one mode of treatment for ODS (32). The current study has looked at ODS and found no evidence for a difference in ODS scores following wedge resection, although the sample size was small (n = 5) and the control scores in untreated women are not particularly raised at 5 of a possible 20.
Improvements in pain scores after surgical resection of endometriosis are well documented (3, 8, 12, 16, 33, 34). Our cohort generally had a high pre-operative frequency of pelvic pain, dysmenorrhoea, menorrhagia, dyspareunia and dyschezia. There was no significant difference in frequency of preoperative symptoms between the groups except for menorrhagia (Group 3) and dyschezia (Groups 3 and 4) but this does not tell us about symptom severity, which we were unable to measure. We would have expected that those patients who underwent bowel excision surgery would have had more severe symptoms and the incidence of dyschezia certainly supports this. The similarity in symptom VAS scores and QOL measures between Groups 1-4 at this long follow-up supports the use of less radical approaches in severe disease when the symptoms are milder.
The long interval between the surgery and completion of our study ensured that short-term post-operative symptoms had resolved and any long-term issues had time to present. This is particularly useful in assessing bladder symptoms which may take years to manifest due to the indolent nature of the pathology causing bladder dysfunction with nerve damage leading to subtle changes in bladder filling over time, eventually leading to neurogenic bladder atony. Short-term complications such as urinary retention could be captured from medical record review, though some complications may have been missed if a patient presented to their GP instead of attending the post-operative clinic.
Most of the available literature regarding urinary complications post-treatment of endometriosis focuses on immediate post-operative complications with little long-term data on ongoing urinary symptoms and patient QOL. We had a low incidence of immediate post-operative urinary complications with 3 of 61 patients in Group 2 and 2 of 11 patients in Group 3 having difficulty voiding post-operatively. Our patients also had a low incidence of long-term urinary symptoms post-operatively with no difference in CLSS between the surgical groups. The terms used in the literature for this clinical picture are not standardised, including ‘bladder atony’ (3), ‘retention’ (15, 35), ‘slow bladder emptying’ (16) and ‘neurogenic bladder’ (8). Such inconsistency of terminology makes comparison of studies following radical excision of endometriosis difficult. Some nerve-sparing techniques have been developed to reduce problems related to bladder denervation and possibly result in post-operative voiding being resumed more rapidly (9, 10, 19). Additionally, lower rates of rectal and sexual post-operative dysfunction have been reported with these techniques, leading to an improved QOL (19). Our practice has not yet adopted nerve-sparing techniques, but despite this we have not found a high rate of post-operative bladder dysfunction.
QOL is an important outcome measure of the impact of surgery for endometriosis. QOL after treatment of bowel endometriosis is seldom reported; one systematic review examining the clinical outcome of surgical treatment of deeply infiltrating endometriosis (DIE) with colorectal involvement found that less than 10% of studies reported data on QOL (32). However, when QOL is reported, it is usually found to be improved after surgery (12, 33, 36-39) regardless of open or laparoscopic resection (12). A population-based study in England (40) showed a median EQVAS score of just under 80 in women, which is comparable to the median values in our four groups (range 60 to 85). Our study examined whether QOL outcomes correlate with the extent of surgical excision and we did not find a difference; however, we do not have pre-operative levels so cannot compare the changes in QOL. More and larger studies with a long-term follow-up using the same validated QOL questionnaires are required to allow comparison between different surgical techniques and their impact on the post-operative QOL.
In summary, we found that bowel resections for endometriosis resulted in increased bowel frequency and faecal incontinence. We did not find a difference in urinary and other bowel symptoms or QOL between the four different surgical approaches to endometriosis.
The vast majority of published reports on this topic describe bowel resection surgery with almost no “no resection” papers. Prospective studies are needed to further elucidate the effects of different surgical treatments on bowel and bladder symptoms, with greater focus on less radical procedures, particularly in the setting of milder symptomatology. This is particularly true if a more conservative approach leads to a similar outcome for QOL and pain improvement, with lower rates of complications.
Footnotes
Financial support: No grants or funding have been received for this study.
Conflict of interest: None of the authors has financial interest related to this study to disclose.
Meeting presentation: This work was presented at the Australasian Gynaecological Endoscopy and Surgery Society and International Society for Gynaecologic Endoscopy Congress in March 2015 in Melbourne, Australia.