
Abstract
Cryopreservation of ovarian tissue in advance of cytotoxic therapies and later transplantation of the tissue is being performed increasingly often, and the total success rates in terms of pregnancy and delivery have been described in case series. Most pregnancies were achieved after orthotopic transplantation of tissue (in the peritoneum or the remaining ovary); however, treatment of the transplantation site during surgery is controversial. In this observational case-series study, we include four patients who underwent ovarian tissue transplantation between 2012 and 2016 by laparoscopy. Previously ovarian tissue was cryopreserved with slow freezing protocol prior to chemo- and/or radiotherapy. After cancer remission, the cryopreserved ovarian tissues were orthotopically re-transplanted in the ovarian medulla by laparoscopy, using N-hexyl-2-cyanoacrylate as an absorbable adhesion barrier. All patients regained ovarian function between 8 and 24 weeks after transplantation, as shown by follicle development and estrogen production. In patients 1 and 2 the ovarian function ended one year after transplantation. Patient 3 has regular menstrual cycles 2 years after the transplant and patient 4 currently has an ongoing spontaneous pregnancy.
The use of N-hexyl-2 cyanoacrylate can facilitate the placement of ovarian pieces in orthotopic transplantation by laparoscopy without affecting the restoration and duration of ovarian activity.
Introduction
As a result of improvements in oncology treatment, the majority of younger cancer patients are now achieving prolonged survival (1). However, one of the most common long-term adverse effects of chemotherapy and/or radiation therapy is loss of ovarian function and fertility in premenopausal patients. A number of strategies have been developed in recent years to enable these patients to have children using their gametes. When chemotherapy can be postponed, it is possible to use ovarian stimulation to obtain oocytes, which can be frozen in either a fertilized or an unfertilized state (2, 3).
The removal of ovarian tissue prior to starting oncologic treatment and the subsequent transplantation of this tissue after completing therapy have become increasingly important surgical fertility-preserving techniques (4–6). At least 86 live births have been reported worldwide (7). The procedure has been incorporated into numerous national and international networks and programs (Oncofertility Consortium; FertiProtekt; International Society for Fertility Preservation), a technique which is no longer experimental according to the criteria by ESHRE Special Interest Group “Ethics and Law” (8). Nevertheless, some professional societies such as the American Society for Reproductive Medicine still consider ovarian tissue freezing as an experimental technique (9).
Different surgical techniques can be used both for ovarian biopsy and for the transplantation of ovarian tissue. A number of different surgical routes have been used, and the amount of tissue extracted, the instruments used, the treatment of the ovary, the transplantation site, the blood supply to the transplanted ovarian tissue and the procedure used for simultaneous surgical interventions vary (10, 11).
The pelvic cavity (orthotopic site) provides the optimal environment for follicular development compared with heterotopic sites. Two techniques were successfully used to re-implant frozen/thawed ovarian tissue in an orthotopic site: either in a specially created window on the peritoneum or on the remaining ovary. In case of small fragments, they can be placed on the decorticated medulla, but this is particularly difficult when performed laparoscopically. The use of tissue adhesives such as cyanoacrylates, can facilitate the laparoscopy orthotopic transplantation.
The aim of this study was to examine the usefulness of N-hexyl-2-cyanoacrylate in laparoscopic orthotopic ovarian transplantation analyzing the restoration of ovarian activity and reproductive outcome of patients.
Patients and Methods
Patients
In this observational case-series study we include four patients who underwent ovarian tissue transplantation between 2012 and 2016 by laparoscopy. The ethics committee of the hospital approved the study, and all patients provided written informed consent. Table I shows the diagnosis and age of four women undergoing ovarian tissue cryopreservation and transplantation with frozen/thawed ovarian tissue.
Patient characteristics and time of orthotopic transplantation

Patient 1
In 2010, a 39-year-old woman was diagnosed with nasopharyngeal carcinoma. Ovarian tissue cryopreservation was carried out before radio- and chemotherapy She became amenorrheic shortly after initiation of chemotherapy. Levels of follicle-stimulating hormone (FSH), luteinizing hormone (LH), and estradiol were, 92.3 mlU/mL, 82.5 mlU/ml, and 15 pg/mL, respectively, following chemo- and radiotherapy, confirming castration. This ovarian failure profile was confirmed 3 months later.
In 2012, the patient expressed a desire to conceive. Her present amenorrhea and FSH levels were >100 mlU/mL Orthotopic ovarian tissue transplantation was performed by laparoscopy placing eight pieces of thawed ovarian tissue in the medulla of contralateral ovary to the biopsy. Six months later, a first estradiol peak was detected, with a concomitant decline in FSH. Ultrasonography revealed the development of a follicle with each cycle. Restoration of consecutive menstrual bleeding was observed, and the patient was encouraged to have regular sexual intercourse. In one cycle when follicle reached 18 mm, human chorionic gonadotropin (hCG) was added, and follicle aspiration was performed 36 hours later. A single mature egg was retrieved and fertilized with her husband's sperm in vitro. On day two, post-fertilization, a four-cell embryo was transferred to the uterus. Pregnancy was not achieved. This obviously prevents exact knowledge of whether or not the oocyte originated in the transplanted tissue, and this is a limitation that we want to acknowledge.
Twelve months after transplantation FSH levels increased and the patient presented with menstrual irregularity, and absence of follicular development was observed by ultrasound.
Patient 2
In 2002, a 35-year-old woman was diagnosed with breast cancer. Ovarian tissue was removed by laparoscopy for cryopreservation before the chemotherapy. She became amenorrheic 3 months after initiation of chemotherapy. Levels of FSH, LH, and estradiol were 75.3 mlU/mL, 45.5 mlU/mL, and 18 pg/mL, respectively, confirming ovarian failure.
In 2012, the patient wished to conceive. Her FSH levels were >100 mlU/mL and she became amenorrheic. Orthotopic ovarian tissue transplantation was performed by laparoscopy placing nine pieces of thawed ovarian tissue in the medulla of contralateral ovary. Four months after re-implantation restoration of menstrual bleeding was observed and spontaneous follicle development was proved by vaginal ultrasound. Ovarian activity remained regular until one year after the transplantation. Finally, FSH levels increased and the patient became amenorrheic.
Patient 3
The patient was diagnosed with breast cancer in 2011 at 35 years of age. Ovarian tissue was removed simultaneously during breast cancer surgery. She was amenorrheic from her third chemotherapy cycle and her serum FSH and anti-mullerian hormone (AMH) levels were 45.3 mlU/mL and 0.1 ng/mL, respectively.
Ovarian tissue transplantation was performed in 2014. Eight pieces of frozen/thawed tissue were placed into the ovarian medulla by laparoscopy. Two months after re-implantation, spontaneous follicle development was observed by ultrasonography, and basal FSH was 7.9 mlU/L. After regular intercourse without pregnancy, IVF-modified natural cycle was performed in three cycles. In our institution, this protocol attempts to allow spontaneous growth of the dominant follicle without administration of any additional drug that may distort folliculogenesis or modify endometrial receptivity. However, in case of spontaneous LH surge (defined as an LH value that exceeds 180% of the mean baseline value), on the day of hCG, supplementary administration of 0.25 mg subcutaneous injection of a GnRH antagonist was given to prevent premature ovulation before oocyte retrieval. In case an LH surge was identified before a dominant follicle reached 15 mm, gonadotropin-releasing hormone (GnRH) antagonist and 75 IU of SC gonadotropin/menotropin were used daily until triggering criteria were present. When follicle reached 18 mm, hCG was added, and follicle aspiration was carried out 36 hours later (12). In each of the cycles one embryo was transferred without success. Two years after transplantation the patient maintains regular menstrual cycles.
Patient 4
In 2011, a 32-year-old women was diagnosed with breast cancer. Breast surgery and laparoscopic ovarian preservation procedure were carried out in the same setting. The patient was amenorrheic from her third chemotherapy cycle and blood tests showed menopausal hormone values (FSH 82 mUI/mL).
In May 2016, we performed orthotopic ovarian tissue transplantation placing fifteen pieces of frozen/thawed cortex to the left ovarian medulla. Two months after re-implantation the patient presented her first menstruation and she became pregnant naturally, which was confirmed positive by hCG in urine. The vaginal ultrasound revealed a viable intrauterine pregnancy with a crown-rump length (CRL) of 6.8 mm, corresponding to a gestational age of 7 weeks.
Operative technique
We always used a laparoscopic approach to extract ovarian tissue. For the removal of the ovarian cortex we use scissors avoiding the use of coagulation to minimize the surgical trauma to the sensitive ovarian tissue. The bipolar coagulation should only be carried out after the samples of ovarian tissue have been removed and coagulation should be done sparingly to protect the ovarian remnant.
We opted to remove one-third of the ovarian cortex, which was cut into 5 × 5 mm fragments, rinsed with an isotonic saline solution and cryopreserved as the method previously described by Schmidt et al (13). Briefly, the fragments were transferred to the freezing solution (0.1 mol/L sucrose and 1.5 mol/L ethylene glycol in phosphate-buffered saline) and equilibrated for 30 min at 1°C. The fragments were stored in 1.8 mL cryovials (Nunc AS, Roskilde, Denmark) with cryoprotectant and were cryopreserved using a programmable freezer (Planner K10, Planner Ltd., UK). Two fragments were submitted for histological study demonstrating the presence of primordial follicles and to rule out neoplastic cells.
The auto-transplantation was performed by laparoscopy. A longitudinal incision in the ovarian cortex contralateral to the biopsy was performed. The fragments were rapidly thawed in a 37°C water bath and rinsed with thawing solutions with decreasing concentrations of cryoprotectants. The incision was made with scissors avoiding the use of electric coagulation. After exposing the medulla, we placed ovarian tissue and the N-hexyl-2-cyanoacrylate was applied as a surgical adhesive. Finally, once the fragments were fixed, the edges of the ovary were approached using the same material (Figs. 1–4).
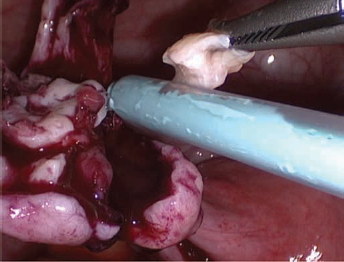
Placement of N-hexyl-cyanoacrylate on the decorticated ovarian medulla.
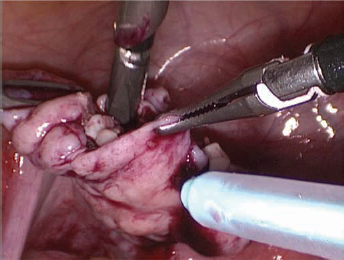
Placement of ovarian fragments.
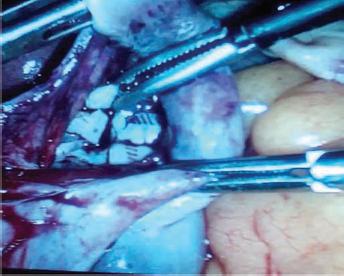
Ovarian fragments are visible on the remaining ovary.
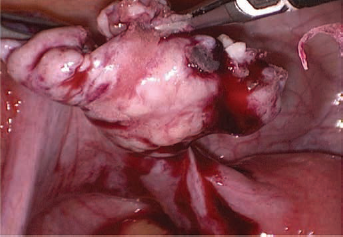
Bonding the edges of the ovary.
Results
All patients were discharged on the same day of the surgery. Restoration of ovarian function was observed in all cases between 8 and 24 weeks after the transplantation by the significant decrease in FSH levels compared to preoperative values (Fig. 5).
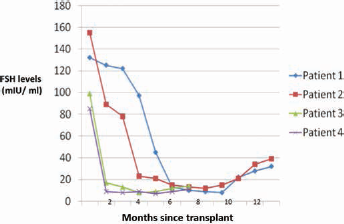
Follicle-stimulating hormone (FSH) values after orthotopic re-implantation of frozen/thawed ovarian tissue.
The time interval between implantation and the restoration of ovarian activity could be explained by a difference in follicular reserve at the time of cryopreservation. Age would explain the observed differences, and also the fact that patients 1 and 2 had a shorter duration of restored ovarian activity. This early restoration of ovarian activity initiated 2 months after transplantation could indicate that the follicular activity would come from the native ovary. It has recently been suggested that after transplantation, the massive recruitment of “trapped” follicles in the residual ovary may be mediated by mechanism via phosphatase and tensin homolog (PTEN) (14–16).
Figure 6 summarizes the follicular activity that was echo-graphically verified and the oocyte recovery in the cycles in which in vitro fertilization was performed in the non-stimulated cycle. Pregnancy was not achieved in any of these cycles. There is no doubt that the percentage of abnormal oocytes (immature or degenerated) is much higher in frozen/thawed transplanted tissue than in the general population undergoing IVF.
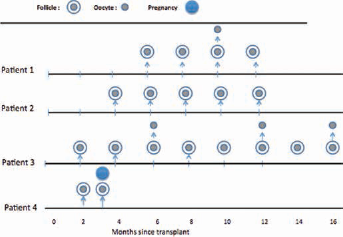
Double circles represent preovulatory follicle, whereas single circles represent retrieved oocytes.
Patient 4 presented spontaneous follicle development 8 weeks after transplantation and she became pregnant naturally three months after ovarian transplantation, which highlights that assisted reproductive techniques are not necessary for most women.
Discussion
This report describes our experience with the use of N-hexyl-2 cyanoacrylate as a fixation surgical treatment in the transplantation site during orthotopic ovarian tissue transplantation. To our knowledge this is the first experience with this synthetic surgical adhesive.
The extraction of ovarian tissue prior to commencing oncologic therapy and the subsequent re-implantation of this tissue after concluding cancer treatment is an innovative method that is becoming increasingly important in fertility surgery. A large number of centers have started to offer this procedure to affected women. The literature shows that the number of pregnancies and births following the transplantation of cryopreserved ovarian tissue has increased continually in recent years, indicating that this has become an established procedure (7, 17, 18). Nevertheless, data on the best surgical technique for this fertility-preserving method are limited.
Patient's age is an important predictor of successful ovarian tissue transplantation; however, there are published case series in which transplants have been performed in women of advanced ages achieving subsequent pregnancies. It can be assumed that individual ovarian reserve and thus follicle density at the time of tissue harvesting have greater influence than merely the patient's age at tissue harvesting (7, 17).
Although most centers opt for the laparoscopic approach for ovarian tissue transplantation, it is true that the laparotomic route has been successfully used by some authors (16). The benefit of the laparoscopic approach is that recovery is fast and the patient can be discharged on the day of surgery, allowing them to start chemotherapy without further delay (17–19).
Opinion is more divided on the question of the amount of ovarian tissue to be extracted. Donnez et al (10) pointed out that biopsies of the ovarian cortex need to be at least 1 mm thick, otherwise they not include primordial follicles under the mesothelium. Other centers prefer ovarian sampling with sample sizes ranging one-third to two-thirds of the ovary (11, 19) or even extraction of an entire ovary. The sampling of a large piece of ovarian tissue offers the opportunity to potentially carry out repeat transplantations of different portions, which could help maintain reproductive and endocrine ovarian function for longer. A possible compromise between the different approaches of the centers could consist of removing a large part of one ovary prior to scheduled aggressive chemotherapy but leaving more tissue in situ when protocols are less toxic (16).
Regarding ovarian cryopreservation techniques, the great majority of pregnancies have occurred following slow freezing of the ovarian cortical pieces; however, recent studies indicate that vitrification may have advantages. In fact, some centers are currently using vitrification exclusively as a method. It will be necessary to wait a few years to have the same experience as with slow freezing (16)
There are three potential sites for transplantation: (i) transplantation to the ipsilateral and/or contralateral ovary, (ii) into an ipsilateral and/or contralateral peritoneal pocket, and (iii) heterologous transplantation. Potential benefits of the ovary as the site of re-transplantation are that the tissue was originally taken from the same site and the transplanted sample can be located easily and removed if necessary. However, the risk of bleeding is higher and there is also a potential risk of trauma to the ovary, which can be avoided by transplantation into a peritoneal pocket. In the reported series, the peritoneal window created close to the ovarian hilus and the ovarian medulla both appear to be equally efficient sites of re-implantation, at least for restoration of ovarian activity (5, 10, 16). Although some authors considered follicular activity in the peritoneal site to be lower than that observed on the medulla (19).
Treatment of the transplantation site during surgery is controversial. The advantage of using sutures or fibrin glue is the secure closure to the peritoneum or the ovary, which ensures that the transplanted tissue will not fall out. However, the sutures or other materials may produce additional trauma to surrounding tissue and the potentially high risk of adhesions and postoperative pain (18, 20, 21).
Auto-transplantation of ovarian tissue in the remaining or in the contralateral ovary presents more difficulty compared to peritoneal pockets, but increases the chance of spontaneous pregnancies and also facilitates the ultrasound monitoring of follicular growth. In our study, all four patients underwent auto-transplantation in the contralateral ovary using the adhesive material N-hexyl-2-cyanoacrylate, which has a capacity greater than fibrin glue fixation and avoids the use of sutures. No postoperative complications and difficulty in ultrasound monitoring of patients were observed. In addition, we performed oocyte retrievals without difficulty.
Currently, tissue adhesives and glues are an alternative technology in clinical applications that are important both to the medical industry and surgical profession. Many of these emerging tissue adhesives could modify difficult surgical procedures by stabilizing tissue surfaces through hemostasis, sealing of wounds, and fixation of tissue in areas inaccessible to staples, clips, and suture placement (22).
There are differences between synthetic (cyanoacrylates) and biological (fibrine glue) tissue adhesives. It should be made clear that biological adhesives are concentrated fibrinogen and factor XIII; in addition, biological adhesives can have contamination (risking transmission of disease). For this reason, they require prior preparation (while synthetic tissue adhesives can be applied immediately after opening) and are much more expensive (23).
Synthetic cyanoacrylate tissue adhesives have been used extensively as an alternative to current conventional treatments in clinical applications and studies, including applications in thoracic, gastrointestinal, neurologic, cardiovascular, ophthalmologic and vascular surgery (24, 25)
The fundamental advantages of N-hexyl-2-cyanoacrylate include the high purity and low polymerization temperatures presented, contributing to the avoidance of toxicity when used as an adhesive. In the absence of impurities in the formulation, its effectiveness as an adhesive is not compromised. This purity of this cyanoacrylate means that stabilizers are not needed, as is often the case in other cyanoacrylates, and it can be applied immediately after opening (26).
Although the study includes a small number of patients, we demonstrated the effectiveness of the application of N-hexyl-2-cyanoacrylate at the transplantation site. In all patients, ovarian function was restored and maintained for at least one year. Obviously, age was an important prognostic factor because in the last 2 patients ovarian tissue was stored at an earlier age and the restoration of ovarian function was achieved earlier. In the last of transplanted patients, spontaneous pregnancy was achieved, showing that ovarian orthotopic transplant can facilitate this possibility.
In conclusion, we relate our experience with the use of N-hexyl-2-cyanoacrylate as adhesive material in the orthotopic transplantation of ovarian tissue. We have proven their potential adhesive facilitating the apposition of the fragments of tissue in the ovarian medulla without affecting the restoration of ovarian activity and its effectiveness in reproductive terms.
Footnotes
Financial support: No grants or funding have been received for this study.
Conflict of interest: None of the authors has financial interest related to this study to disclose.