
Abstract
Purpose
The purpose of this study is to explore how vascular access care was reimbursed, promoted, and organised at the national level in European and neighbouring countries.
Methods
An electronic survey among national experts to collect country-level data.
Results
Forty-seven experts (response rate, 76%) from 37 countries participated. Experts from 23 countries reported that 50% or less of patients received routine pre-operative imaging of vessels. Nephrologists placed catheters and created fistulas in 26 and 8 countries, respectively. Twenty-one countries had a fee per created access; the reported fee for catheter placement was never higher than for fistula creation. As the number of haemodialysis patients in a centre increased, more countries had a dedicated coordinator or multidisciplinary team responsible for vascular access maintenance at the centre-level; in 11 countries, responsibility was always with individual nephrologists, independent of a centre's size. In 23 countries, dialysis centres shared vascular access care resources, with facilitation from a service provider in 4. In most countries, national campaigns (n = 35) or educational programmes (n = 29) had addressed vascular access-related topics; 19 countries had some form of training for creating fistulas. Forty experts considered the current evidence base robust enough to justify a fistula-first policy, but only 13 believed that more than 80% of nephrologists in their country would attempt a fistula in a 75-year-old woman with comorbidities.
Conclusions
Suboptimal access to surgical resources, lack of dedicated training of clinicians, limited routine use of pre-operative diagnostic imaging and patient characteristics primarily emerged as potential barriers to adopting a fistula-first policy in Europe.
Keywords
Introduction
Clinical practice guidelines worldwide consistently recommend an arteriovenous (AV) fistula as the preferred type of bloodstream access for haemodialysis patients because of its favourable influence on risk of infection, thrombosis and death compared with catheters (1–4). Yet, a substantial number of patients with end-stage renal disease still receive haemodialysis via a catheter, and in many countries, this number has been increasing over the last decade (5, 6).
Among the multitude of factors that can affect uptake of renal guidelines (7) are those related to the organisation and reimbursement of healthcare delivery (8, 9). Previous studies have suggested several healthcare system factors that may influence implementation of a fistula-first policy in daily care, such as access to (surgical) resources (10, 11), availability of formal policies for AV fistula referral (12, 13) and intensity of surgical training (14). However, these studies included no or only some European countries, implying that knowledge on these factors in a broader European context is lacking (6).
European Renal Best Practice (ERBP) is the international organisation that produces clinical practice guidance targeted at health professionals who deliver care to kidney patients in Europe and neighbouring regions (www.european-renal-best-practice.org). In preparation of the development of a new guideline on permanent vascular access in haemodialysis patients, ERBP initiated an international survey among experts to get a broad overall picture of how vascular access care is organised, reimbursed and promoted in countries across ERBP's geographical target area. The study results may serve as a starting point for further research by revealing healthcare system level aspects of vascular access care that show room for improvement, and therefore merit a more detailed investigation. In the meanwhile, the results can inform future guidelines on which factors might affect their uptake.
Methods
Questionnaire development
First, we identified factors with a potential impact on the quality of vascular access care; existing vascular access guidelines (2–4), and a systematic review that included initiatives aimed at improving the quality of vascular access care (15) served as a starting point. Next, we selected those factors that are commonly coordinated or promoted at the national or regional level, for example within a reimbursement scheme or quality improvement programme. We then translated all selected factors into survey items, prepared an electronic questionnaire in Survey Monkey® and piloted it among a panel of seven clinical and methodological experts for clarity and completeness. The final questionnaire consisted of 33 items in four categories: reimbursement; educational and promotional activities; organisation; and expert beliefs (see supplementary file available online at www.vascular-access.info). Throughout the questionnaire, we encouraged respondents to provide additional information on their answers in free text fields.
Participants
We contacted 55 national and regional renal societies from 49 countries within the target area of the European Renal Association - European Dialysis and Transplant (ERA-EDTA), and asked them to appoint a national vascular access expert to represent their society in our study. Forty-one societies responded, of which two indicated that they did not have a representative available. Finally, we invited 62 experts from 39 countries.
Data collection and analysis
We collected data from September 2012 to April 2013. Experts received a survey invitation and up to three reminders by e-mail, with a request to provide country-level data regarding vascular access care as delivered to haemodialysis patients in public renal centres. We asked them to base their answers on national or regional data as much as possible. In case such data were not available, we suggested extrapolating local data from their own centre and/or consulting colleagues from a sample of other centres. After submitting their response, experts were contacted for additional information, for example on seemingly conflicting answers. In case two experts represented a country, we facilitated a consensus procedure to come to one agreed set of answers for that country.
Countries were the unit of analysis for data on reimbursement, educational and promotional activities, and organisation, while we analysed expert beliefs on the level of experts. In all cases, we used descriptive statistics for proportions or quantitative data as appropriate.
Results
Participants
In total, 47 of the 62 invited national vascular access experts participated (response rate, 76%). Table I summarises their characteristics. They represented the following 37 of 39 (95%) invited countries (countries marked with * were represented by two experts): Albania*, Algeria, Austria, Belgium-Dutch speaking*, Belgium-French speaking, Bosnia and Herzegovina*, Croatia, Czech Republic, Estonia*, France, Georgia*, Germany*, Greece, Hungary, Israel, Italy, Kosovo, Lebanon, Lithuania, Macedonia F.Y.R., Montenegro, Morocco, Poland, Portugal, Romania*, Russia, Scotland, Serbia*, Slovak Republic, Slovenia*, Spain, Sweden, The Netherlands*, Tunisia, Turkey, Ukraine and the United Kingdom. The Hungarian and Slovak representatives were practising within a dialysis network and submitted data on vascular access care as provided within their network.
Expert characteristics (n = 47)
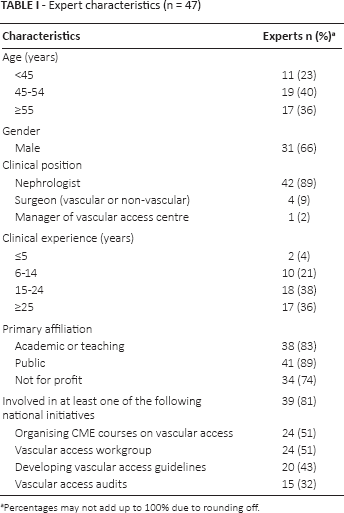
Percentages may not add up to 100% due to rounding off.
Reimbursement for vascular access care
In 21 (57%) countries, reimbursement for establishing vascular access was activity-based (i.e. fee per created access), but payments were seldom made directly to clinicians (n = 6). In seven (19%) countries, reimbursement was included in the rate for providing haemodialysis, while in the remaining countries, healthcare facilities’ budgets were not directly related to the number of provided treatments. Apart from a limited financial contribution to healthcare expenses in general (e.g. the excess of a health insurance policy), patients did not have to pay for vascular access care in the majority of countries (n = 21). In 16 countries, there was a patient fee for several aspects of vascular access care (including access creation, use of imaging techniques to monitor the vessels and so on); in seven, it concerned only medication costs.
Some countries had financial incentive schemes in place. In four cases, dialysis via a fistula was reimbursed at a different rate than haemodialysis via a catheter; three countries financially rewarded centres according to the percentage of patients receiving dialysis via a specific access type. However, in most countries (n = 30), reimbursement for haemodialysis did not depend on the type of vascular access. For 17 of the 21 countries with activity-based reimbursement, experts provided information on the amounts being reimbursed. The fees to create simple (e.g. day case radiocephalic) AV fistulas were either higher (n = 14) or the same (n = 3) than placing permanent catheters.
Educational and promotional activities
Table II summarises the type of educational and promotional activities undertaken in the 37 represented countries. The majority of countries had organised a national campaign (n = 35, 95%) or continuous medical education (n = 29, 78%) addressing vascular access related topics; seventeen (46%) monitored the type and quality of vascular access. For 19 countries (51%), experts indicated that clinicians performing the surgical procedure for a haemodialysis access received specific training, which was often part of the vascular surgery or nephrology curriculum (n = 17) as opposed to an independent and dedicated training programme (n = 2).
Type of educational and promotional activities, and the number (%) of countries (n = 37) in which they were undertaken
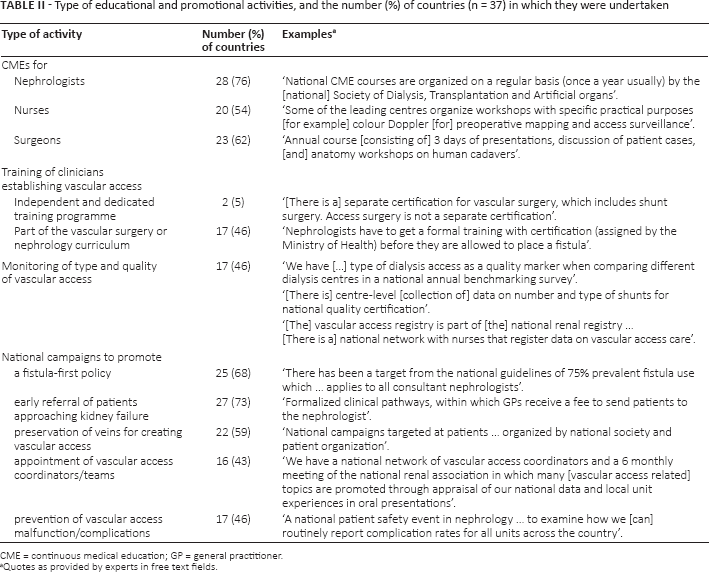
CME = continuous medical education; GP = general practitioner.
Quotes as provided by experts in free text fields.
Organisation of vascular access care
Twenty-three countries (62%) had some form of centralised vascular access care facilities, for example regional outpatient vascular access clinics, or multiple centres sharing the services of one vascular access surgeon. In four of them (11%), a service provider formally facilitated this centralisation.
Preparation for access creation
In the large majority of countries (n = 32, 86%), respondents reported the estimated percentage of late dialysis starts (i.e. within 4 months after first nephrology consult) to be less than 50%. Yet, in 23 (62%) countries, less than half of the patients were estimated to receive routine diagnostic imaging of the vessels prior to access creation. As potential reasons, respondents suggested scepticism among (vascular) surgeons regarding the benefits of imaging, limited access to equipment and expertise, lack of reimbursement and lack of a widespread policy recommending the use of imaging.
Access creation
In most countries (n = 34; 92%), vascular surgeons were among those creating fistulas. Nephrologists created fistulas in eight countries (22%), while this was more common (n = 28, 76%) for placing catheters (Fig. 1, panel A). In 26 countries (70%), more than half of the clinicians placing fistulas performed at least 30 of such procedures annually.
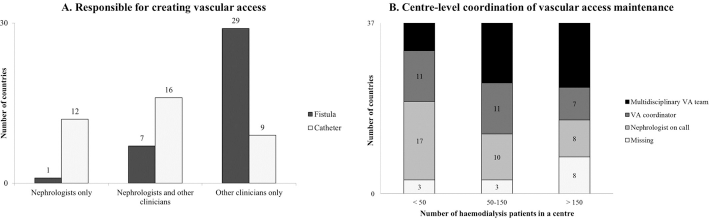
Who is commonly responsible for:
The time between the request for access creation and the actual procedure was usually longer for creating an AV fistula than for catheter placement in 23 (62%) and similar in 13 (35%) countries.
Access maintenance
Figure 1 (panel B) shows that more countries had a dedicated coordinator or multidisciplinary team responsible for arranging routine care around vascular access maintenance at the centre-level, as the number of haemodialysis patients in a centre increased. In 16% of countries, responsibility was with a multidisciplinary team (n = 6), independent of centre size, and in 30% always with individual nephrologists (n = 11).
Vascular surgeons (n = 27; 73%) and/or radiologists (n = 19; 51%) were most commonly among those responsible for performing interventional procedures in case of fistula complications, whereas catheter complications were mainly handled by nephrologists (n = 27; 73%).
The average waiting time for an interventional procedure to salvage a thrombosed access was similar for both access types in most countries (n = 22, 59%), and longer for fistulas in 10 (27%).
Expert beliefs
Most of the 47 experts (n = 40; 85%) thought that the current evidence base was robust enough to justify a ‘fistula first–graft second–catheter last policy’. Fifteen (32%) of them considered fistulas a reliable and durable access in more than 80% of patients, while 25 (53%) indicated that this was true for 51-80% of the patients. When presented with the case of an incident 75-year-old female patient with diabetes and hypertension, 13 (28%) believed that more than 80% of clinicians would attempt to create a fistula (Fig. 2).
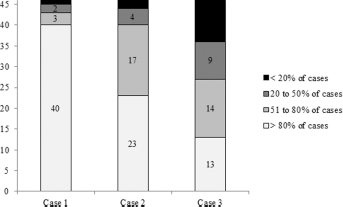
Beliefs reported by 46 experts on the percentage of nephrologists in their country who would attempt to create a fistula in a new haemodialysis patient (
Forty-five experts selected a top three of factors that – in their personal opinion – had the maximum impact on the type and quality of vascular access care in their country. The four factors most frequently perceived as having a positive influence were attitude of nephrologists (n = 24; 53%); early referral and access to nephrology care (n = 22; 49%); promotion of a fistula-first policy (n = 15; 33%); and monitoring of type and quality of vascular access (n = 11; 24%). Factors commonly believed to negatively affect the quality of vascular access care were (lack of) surgical capacity (n = 18; 40%); reimbursement system for establishing or maintaining vascular access (n = 13; 29%); (lack of) training and education of health professionals (n = 12; 27%); and (lack of) requirements for minimum numbers of procedures for those creating vascular access (n = 12; 27%).
Discussion
Summary of main findings
This study provides a broad overview of how vascular access care is currently reimbursed, promoted and organised across 37 countries in Europe and neighbouring regions. Aspects that primarily emerged from our results as potential barriers to adoption of a fistula-first policy were limited access to and centralisation of surgical resources for creating fistulas; lack of dedicated training for clinicians who create fistulas; limited routine use of pre-operative diagnostic imaging of vessels; and patient characteristics. Factors that appeared less prominent barriers were overall attitudes towards fistulas as the preferred access; late patient referral; promotion and education around vascular access; and reimbursement policies.
Overall attitudes towards a fistula-first policy
From our survey, the overall attitudes towards the fistula as the preferred access appeared positive: besides many countries having nationally promoted a fistula-first policy, most experts considered fistulas a reliable and durable access in the majority of patients. This may partly be explained by our finding that they considered the evidence base for preferring fistulas to grafts and catheters sufficiently strong. This perceived evidence strength does not correspond with vascular access guidelines consistently grading their evidence base as being moderately strong at most (1, 3, 4). Furthermore, the recent systematic review by Ravani et al (16) identified a high risk of selection bias in studies exploring the association between access type and dialysis outcomes. On the basis of our study results, it would be of interest to further investigate the gap between perceived and actual evidence strength among a larger sample of individual clinicians, for example by asking how familiar they are with the vascular access literature, how this influences their practice and whether they see a need for further strengthening of the evidence base.
Influence of Patient Characteristics on Clinicians’ Fistula Preference
In line with other studies (6, 12, 13, 17), we found that clinicians seem less likely to attempt a fistula in older patients with comorbidities. Previous research also identified a history of fistula failure and a high body mass index as factors negatively influencing fistula preference (12, 13). Despite these congruous indications that clinicians incorporate patient characteristics into the decision-making process around access type, current clinical practice guidelines do not provide recommendations on how to do this. Future guidelines should therefore make an effort to further specify which patients may benefit from the creation of a fistula.
Routine pre-operative monitoring prior to fistula creation
Although the evidence base for the positive effect of pre-operative monitoring on fistula success rates may need further strengthening (18), existing guidelines consistently recommend routine use of imaging techniques before creating a fistula (3, 4, 19). Nevertheless, our study suggested suboptimal uptake of this practice in Europe, which might consequently hamper implementation of a fistula-first policy (12, 13). The majority of 21 European surgeons participating in a small international study reported to offer ultrasound mapping to all their patients, but at the same time stated that the mapping results hardly ever altered their choice of vascular access (13). These and our findings merit more detailed investigations of (reasons for low) uptake of pre-operative imaging, which may guide future efforts to further optimise its implementation in daily practice.
Accessibility of surgical resources for creating fistulas
In keeping with prior research (12, 13), experts in our study believed lack of surgical capacity to be an important factor negatively influencing the quality of vascular access care in their country. This perceived suboptimal accessibility might partly be explained by our finding that in the majority of countries, centres had to share vascular access resources without this being formally arranged by a service provider. Mishler et al (20) found that establishing an outpatient vascular access centre serving 21 dialysis facilities improved accessibility of resources, as well as vascular access outcomes. Further, timely access to a surgeon has been shown to be associated with more patients starting dialysis with a fistula (17). Future guidelines may include a separate section on how to organise vascular access care. However, due to the limited evidence base for the effectiveness of interventions to improve vascular access care (15), we expect this section to mainly contain suggestions instead of strong recommendations.
Training of clinicians creating fistulas
For many countries in our study, experts reported that learning how to create haemodialysis access was part of the vascular surgery or nephrology curriculum. However, we cannot infer from this that the experience level of clinicians who create fistulas is similar between these countries. Saran et al (14) reported large variation between European countries in the number of fistulas placed during training, as well as the perceived degree of emphasis on vascular access creation. They showed that besides being associated with a higher probability of placing fistulas in practice, an increased number of fistulas placed during training decreased primary and secondary fistula failure rates (14). Concordant with the recommendation by Saran et al, future guidelines may suggest the introduction of minimum requirements for the number of procedures during training, for example as part of a separate training programme for those creating vascular access.
Strengths and limitations of the study
The main strength of our study is the high number of represented countries, which enabled us to provide a broad overview of how vascular access care is organised across Europe. Furthermore, many respondents elaborated on their answers in the free text fields or on our request. These additional qualitative data allowed us to illustrate and explain some of the quantitative results.
Collecting information on the country-level increased the feasibility and coverage of our study. Whereas country-level data were suitable for most survey items, they may have been less appropriate to describe aspects of vascular access care for which between-centre variation within countries was potentially large (e.g. percentage of late referrals, use of pre-operative monitoring, waiting times for access creation). Even though in such cases many experts made an effort to base their answers on data from registries or a sample of centres, we cannot draw firm conclusions based on our study results. Instead, they are only a starting point for future studies further investigating these aspects based on centre-level data.
Lastly, the majority of our experts were nephrologists. Although they are commonly involved in access preparation and maintenance, they were often not the ones establishing fistulas. As in most countries vascular surgeons were responsible for this aspect of care, their knowledge and views would have complemented our study results.
In summary, this survey gives a broad overview of organisational aspects of vascular access care in Europe. Potential topics for further research that emerged from our findings are the gap between perceived and actual strength of the evidence base underlying a fistula-first policy, and the (reasons for low) uptake of pre-operative imaging techniques. In addition, future guidelines may consider including guidance on how to incorporate patient characteristics in the decision-making about access type; adding a section with suggestions on how to organise vascular access care may help guideline users to optimise the adoption of a fistula-first policy in practice.
Footnotes
Acknowledgments
We kindly acknowledge the following experts for participating in our study (in alphabetical order): Prof. Anton Andrusev, Prof. Rabia Bayahia, Prof. Fatma Ben Moussa, Prof. Reinhard Brunkhorst, Prof. Jadranka Buturovic, Dr. Cécile Couchoud, Prof. Petar Dejanov, Prof. Annemie Dhondt, Prof. Nada Dimkovic, Dr. Ymer Elezi, Dr. Eliezer Golan, Dr. Marc Hemmelder, Prof. Markus Hollenbeck, Dr. Dkhissi Houcine, Dr. Jose Ibeas López, Dr. Tamara Jemcov, Dr. Jose Khabouth, Prof. Mykola Kolesnyk, Dr. Reinhard Kramar, Dr. Nihad Kukavica, Dr. Kakha Kuntelia, Dr. Sondra Kybartiene, Dr. Krzysztof Letachowicz, Dr. Aleksander Lõhmus, Dr. Carlo Lomonte, Prof. Jan Malík, Dr. Fahrudin Masnic, Prof. Eugen Mota, Dr. Suela Mumajesi, Prof. Fernando Nolasco, Dr. Stelios Panagoutsos, Prof. Rafael Ponikvar, Prof. Sanjin Racki, Dr. Marina Ratkovic, Prof. Tahar Rayane, Prof. Halima Resic, Dr. Ramón Roca-Tey, Prof. Mai Rosenberg, Prof. Irma Tchokhonelidze, Dr. Damien Thibaudin, Dr. Peter Thomson, Prof. Jan Tordoir, Dr. Marietta Török, Dr. Eliza Trican, Dr. Sv&ecar;tlana Va&ncar;ková, Dr. Gunilla Welander, Prof. Waclaw Weyde, Prof. Müjdat Yenicesu, Dr. Arben Zeneli.
Financial support: None.
Conflict of interest: W. Kleophas received travel fees on different occasions from Amgen, Hexal, Baxter, and serves as a steering committee member of CK-DOPPS study. S.H. Hoischen is Diaverum's country medical director in Germany. W. van Biesen received travel fees on different occasions from Baxter, Fresenius and Gambro, and serves as a steering committee member of a Fresenius sponsored study (IPOD-PD). The other authors have no conflict of interest to declare.