
Abstract
Background
In the advanced stages of chronic heart failure (CHF) the expression of inducible nitric oxide synthase (iNOS) in skeletal muscle (SM) may contribute to exercise intolerance and early fatigue. Cell culture studies and promoter analysis demonstrated that the transcription factor nuclear factor kappa B (NF-κB) is essential for iNOS-expression. The aim of this study was to assess whether NF-κB is activated in skeletal muscle of patients with CHF and linked to the expression of iNOS.
Methods
Skeletal muscle biopsies were obtained from seven CHF patients and seven healthy controls (HC). Nuclear proteins were isolated and the content of activated NF-κB was analysed by electrophoretic mobility shift assay (EMSA). Inducible nitric oxide synthase expression in SM was determined by real time polymerase chain reaction (PCR).
Results
The expression of iNOS (1.4±0.2 versus 0.5±0.08 arbitrary units, P=0.001) and the activation of NF-κB in the SM (0.5±0.1 versus 0.1±0.04 arbitrary units, P=0.009) was significantly increased in CHF patients as compared to healthy controls. Furthermore, a linear correlation was observed between NF-κB activation and iNOS expression (r=0.78, P < 0.001).
Conclusions
The results of this study indicate for the first time that in the skeletal muscle of patients with chronic heart failure the activation of the transcription factor NF-κB is increased and may represent one important regulatory factor for the expression of iNOS in patients. Nevertheless, due to the small sample size this observation has to be confirmed in subsequent studies with more patients. Eur J Cardiovasc Prevention Rehab 10:273–277 © 2003 Lippincott Williams & Wilkins.
Introduction
Chronic heart failure (CHF) is not only associated with increased mortality and morbidity, but also with exercise intolerance and early fatigue. It has been frequently pointed out, however, that exercise capacity could not be predicted by classical parameters of left ventricular function [1, 2]. Therefore, considerable attention has focused on alterations in the peripheral skeletal muscle. Several metabolic as well as ultrastructural abnormalities have been described [3, 4]. Recently, we and others have demonstrated an increased expression of inducible nitric oxide synthase (iNOS) in skeletal muscle biopsies of CHF patients, which was inversely correlated with exercise capacity [5–7]. These results implied that iNOS expression might contribute to the reduced contractile performance of peripheral skeletal muscle in CHF.
Genomic analysis of the iNOS promoter [8], as well as cell culture experiments in different cell types including skeletal muscle myoblasts [9–13], suggested that inflammatory cytokines are an important trigger for the induction of iNOS-expression. Indeed, circulating levels of inflammatory cytokines, such as tumour necrosis factor-alpha (TNF-α), interleukin-1β (IL-1β) and interleukin-6 (IL-6), have been reported to be increased in patients with chronic heart failure and exhibit a relation to the severity of the disease [14–17]. Recently we could demonstrate in a rat skeletal muscle myoblast cell culture model that the cytokine mediated iNOS induction was significantly reduced by blocking ERK1/ERK2 activation and completely abolished by the inhibition of nuclear factor kappa B (NF-κB) [9]. These results suggest that the activation of NF-κB is absolutely necessary to induce cytokine-mediated iNOS expression [9]. In addition to cell culture experiments, an increased activation of NF-κB was detected in myocardial tissue samples of patients with end stage heart failure [18].
So far the extent of NF-κB activation in skeletal muscle of CHF patients and its in-vivo relationship to iNOS expression remains largely unknown. Therefore, the aim of this study was to determine the amount of activated NFκB in skeletal muscle biopsies of patients with CHF in comparison to healthy controls and its relation to local iNOS expression.
Materials and methods
Patients
Seven male patients ≤ 70 years with chronic heart failure (New York Heart Association functional class II to III) as a result of dilated cardiomyopathy or ischaemic heart disease and seven sedentary normal individuals were studied. Healthy subjects had a normal physical examination, electrocardiogram, chest X-ray, M-mode and two-dimensional echocardiographic evaluation. All patients had clinical, radiological and echocardiographical signs of chronic heart failure and a reduced left ventricular ejection fraction (LVEF ≤ 40%), as assessed by angiography. Exclusion criteria were diabetes mellitus, chronic alcohol abuse, immunosuppressive therapy, renal failure, chronic lung disease, primary valvular disease, hereditary or acquired neuromuscular disorders, or recent myocardial infarction (less than 3 months).
The protocol of this study was approved by the Ethics Committee of the University of Leipzig, and written informed consent was obtained from all subjects prior to the beginning of the study.
Exercise testing and respiratory gas exchange measurements
All individuals underwent a baseline exercise test to exclude myocardial ischaemia, significant ventricular tachyarrhythmias and to familiarize the subjects with ergospirometry. Exercise testing was performed on a calibrated, electronically braked bicycle in an upright position. Workload was increased progressively every 3 min in steps of 25 W beginning at 25 W. Exercise was terminated when patients were physically exhausted or developed severe dyspnea or dizziness. Respiratory gas exchange data were determined continuously throughout the exercise test as recently described [19, 20].
Skeletal muscle biopsy
Percutaneous needle biopsies were obtained from the middle part of the m. vastus lateralis under local anaesthesia as described in detail by Bergström [21]. The biopsies were immediately frozen in liquid nitrogen and stored at −80°C for subsequent analysis.
Isolation of nuclear proteins
Briefly, skeletal muscle biopsies were homogenized in 800 μl ice-cold buffer (HEPES 10 mmol/l; KCl 10 mmol/l; EDTA 0.1 mmol/l; EGTA 0.1 mmol/l; DTT 1.0 mmol/l; PMSF 1.0 mmol/l; aprotinin 10 μg/ml, pepstatin 10 μg/ml, leupeptin 10 μg/ml). The samples were incubated on ice for 30 min, vortexed for 30 s after addition of 50 μl of 10% Nonidet-P40, and then centrifuged for 10 min at 4°Cin an Eppendorf centrifuge. The pellets were suspended in an ice-cold buffer (HEPES 20 mmol/l; NaCl 400 mmol/l; EDTA 1.0 mmol/l; EGTA 1.0 mmol/l; DTT 1.0 mmol/l; PMSF 1.0 mmol/l; aprotinin 10 μg/ml, pepstatin 10 μg/ml; leupeptin 10 μg/ml), incubated on ice for 2 h, mixed frequently, and centrifuged for 10 min at 4°C. The supernatants were collected as nuclear extract and stored at −70°C. The total protein concentration of the samples was determined by the Pierce protein assay reagent (Pierce, Rockford, Illinois, USA).
Electrophoretic mobility shift assay
NF-κB binding study was performed using a double stranded oligonucleotides containing an NF-κB consensus binding site (5‘-AGTTGAGGGGACTTTCCCAGGC-3’). The oligonucleotide was radiolabelled with 32[P]-ATP using T4 polynucleotide kinase (Promega, Madison, Wisconsin, USA) and incubated with the nuclear extract for 20 min at room temperature. The samples were loaded on a 4% non-denaturating poly-acrylamid gel. After electrophoresis, the gel was dried and exposed for 24–48 h to an X-ray film. The bands were quantified by densitometry using a software package (1DScan, Scanalytics, Billerica, Massachusetts, USA).
For competition experiments nuclear extract were incubated with unlabelled double-stranded NF-κB or AP-1 (cJun) (CGCTTGATGAGTCAGCCGGAA) oligonucleotides for 20 min prior to the addition of labelled oligonucleotides, whereas for supershift assays nuclear extracts were incubated with the appropriate antibody (SantaCruz Biotechnology, Santa Cruz, California, USA) overnight at 4°C prior to the addition of the labelled oligonucleotides.
Quantitative reverse transcribed-polymerase chain reaction
For the quantification of iNOS mRNA real time reverse transcriptase (RT)-polymerase chain reaction (PCR) using the Lightcycler system (Roche Diagnostic Inc., Mannheim, Germany) was used. Briefly, aliquots of isolated RNA were reverse transcribed into cDNA using random hexamer primer and reverse transcriptase (Superscript II; Invitrogen, Karlsruhe, Germany). One μl of this cDNA was added to a PCR reaction containing the following specific primer: iNOS-lightU: 5‘-CCGGAAAACCCAAGGTCTACG-3’, iNOS-lightL: 5‘-GTCTTGTGCCTTTGGGCTCCT-3’. The results for iNOS expression were expressed as a ratio over 18S rRNA, which was amplified as the house keeping gene (18s-rRNA-1: 5‘-AAACGGCTACCACATCCAAG-3’, 18s-rRNA-2: 5‘-CGCTCCCAAGATCCAACTAC-3’).
Statistical analysis
Values are given as mean ± SEM for all variables. Single comparisons were performed by non-parametric tests (Mann-Whitney U-test) and a P-value of less than 0.05 was considered statistically significant. Linear regression analysis was performed to assess the relationship between NF-κB activation and iNOS transcription.
Results
Study group
The study group consisted of seven patients with chronic heart failure and seven age-matched healthy controls. As expected the left ventricular ejection fraction (19.7 ± 1.7 versus 70.8 ± 19.0%, P =0.001) and maximal oxygen uptake (13.9 ± 0.9 versus 27.9 ± 2.3 ml/kg per min, P = 0.001) were significantly reduced in the CHF group as compared to the healthy control group (Table 1). All the other parameters like age, body mass index, and weight were comparable in both groups.
Patient characteristics
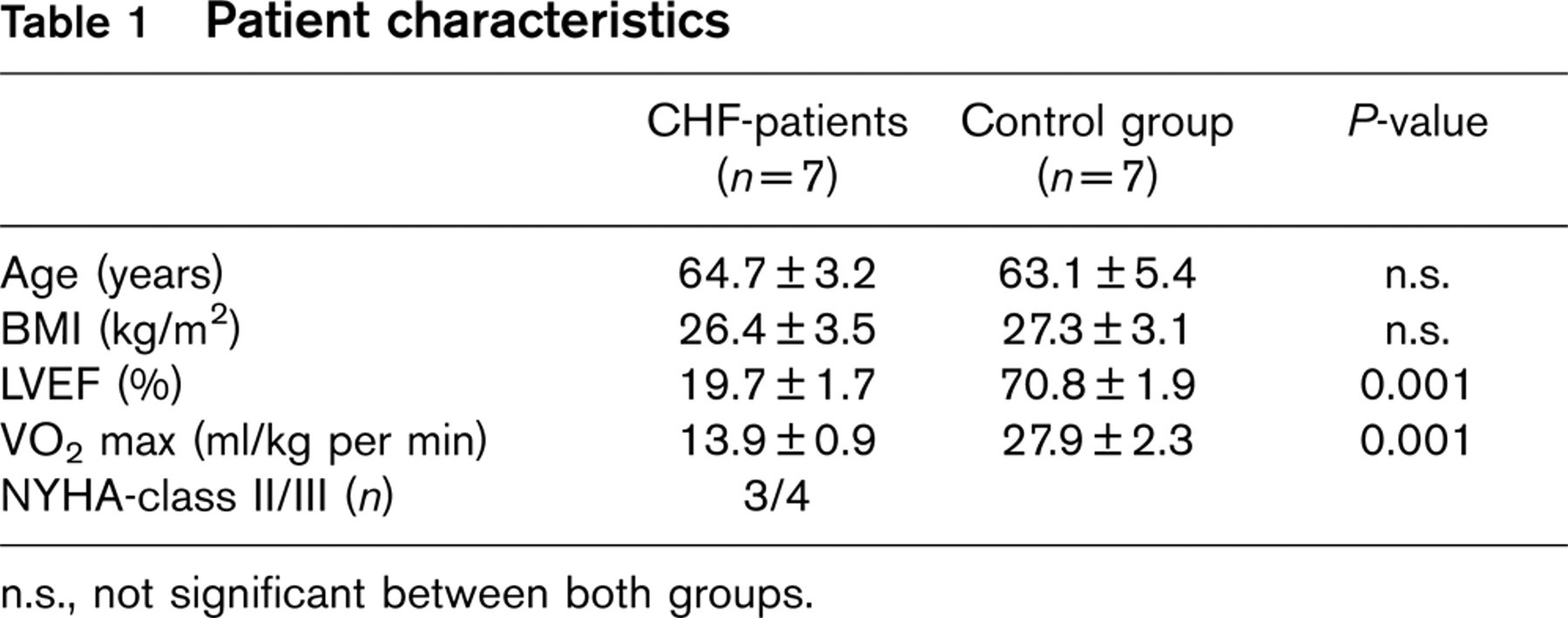
n.s., not significant between both groups.
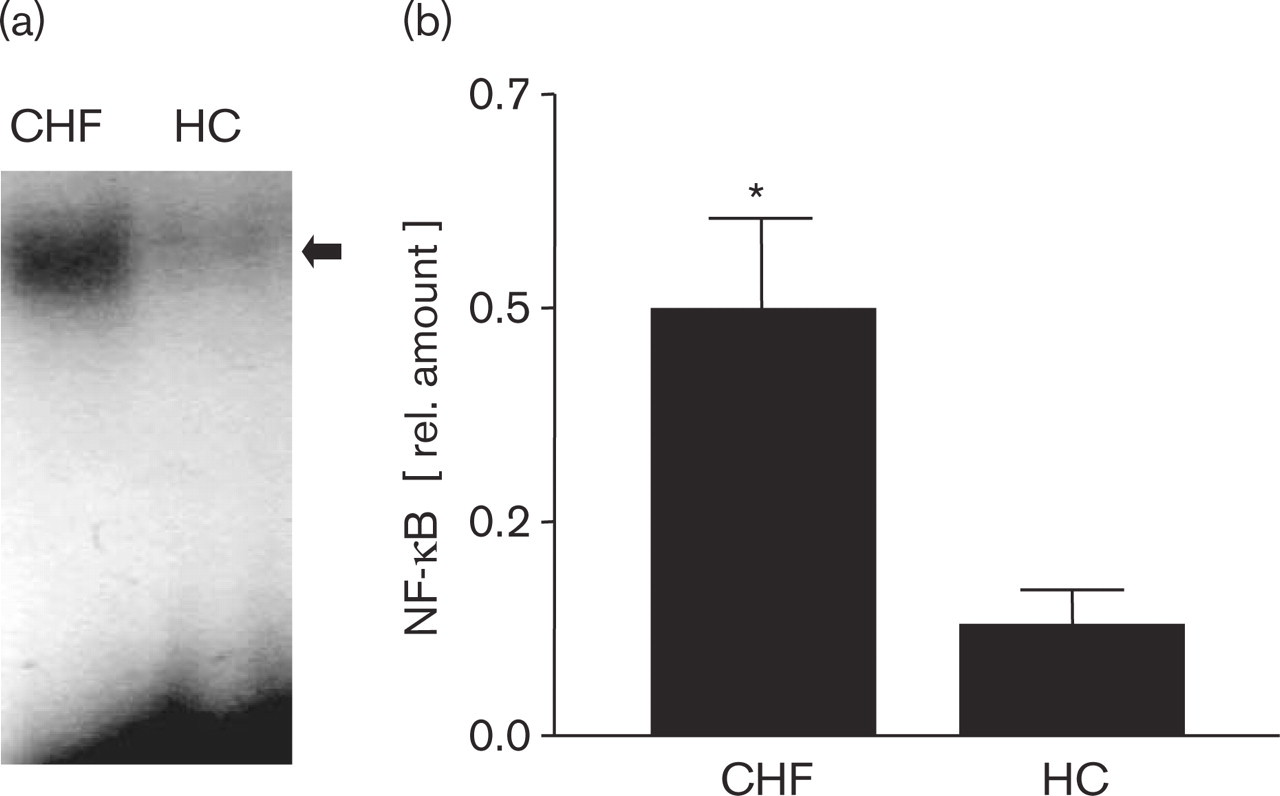
Electrophoretic mobility shift assay (EMSA) of NF-κB in skeletal muscle. (a) The activation of NF-κB was analysed by EMSA in skeletal muscle biopsies of patients with chronic heart failure (CHF) and healthy controls (HC). The incubation of an NF-κB specific probe with nuclear proteins resulted in a shifted NF-κB/oligonucleotide complex (marked with an arrow). (b) The quantitative analysis revealed a significant increase of NF-κB activation in patients with CHF. Results are expressed as mean ± SEM. ∗P≤0.01 versus HC.
All patients were treated with angiotensin-converting enzyme inhibitors, diuretics and beta-blocker, and five patients (71%) also received statins.
Activation of NF-κB in skeletal muscle
As shown in Fig. 1a, incubation of an NF-κB binding-site-specific probe with nuclear proteins isolated from skeletal muscle biopsies resulted in a single shifted band that was detected very weakly in healthy control patients (HC) and is markedly induced in CHF patients. A quantitative analysis of the electrophoretic mobility shift assay (EMSA) (Fig. 1b) revealed, that in skeletal muscle biopsies obtained from CHF-patients NF-κB activation was significantly increased as compared to healthy controls (CHF: 0.5 ± 0.1 versus HC: 0.1 ± 0.04 relative units, P= 0.009). To confirm the identity of the shifted band as NF-κB, competition and supershift experiments were performed. Due to the small amount of nuclear extracts available from the skeletal muscle biopsies of CHF patients these experiments were performed on cytokine-stimulated (IL-1β 50ng/ml in combination with 100 U/ml γ-IFN; 24-h stimulation) L6 rat skeletal muscle myoblasts, as recently described by our group [9]. As expected IL-1β in combination with γ-IFN increased the activation of NF-κB (Fig. 2a, lane 3). A supershift was observed when an NF-κB specific antibody against the subunit p65 was applied (Fig. 2b, lane 2). In competition experiments the intensity of the shifted band was dramatically reduced with an access of unlabelled NF-κB oligonucleotide (Fig. 2b, lane 3), whereas an AP1 specific oligonucleotide did not result in an intensity reduction (Fig. 2b, lane 4).
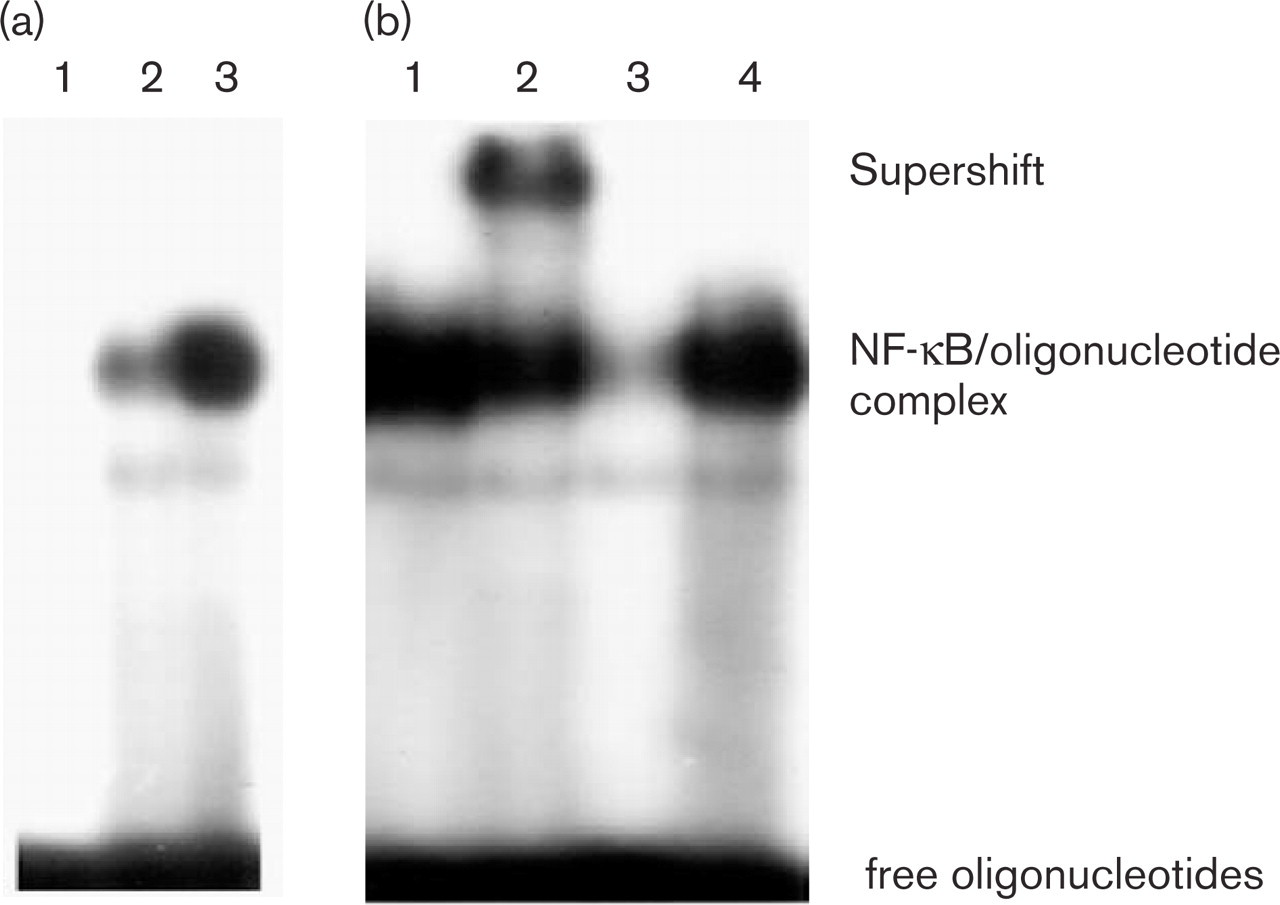
EMSA of L6 rat skeletal muscle myoblasts incubated with cytokines. L6 cells were incubated for 24 h with or without interleukin-1β (50 ng/ml)/γ-interferon (100 U/ml). Nuclear proteins were isolated and incubated with a radiolabelled NF-κB oligonucleotide and separated on a non-denaturating gel. (a) Lane 1: negative control; lane 2: untreated L6 cells; lane 3: L6 cells treated with IL-1 β/γ-IFN for 24h. (b) Lane 1: L6 cells treated with IL-1 β/γ-IFN for 24 h; lane 2: incubation with a specific antibody against the p65 subunit of NF-κB; lane 4: competition with excess of unlabelled NF-κB specific oligonucleotide; lane 4: competition with excess of unlabeled AP-1 specific oligonucleotide.
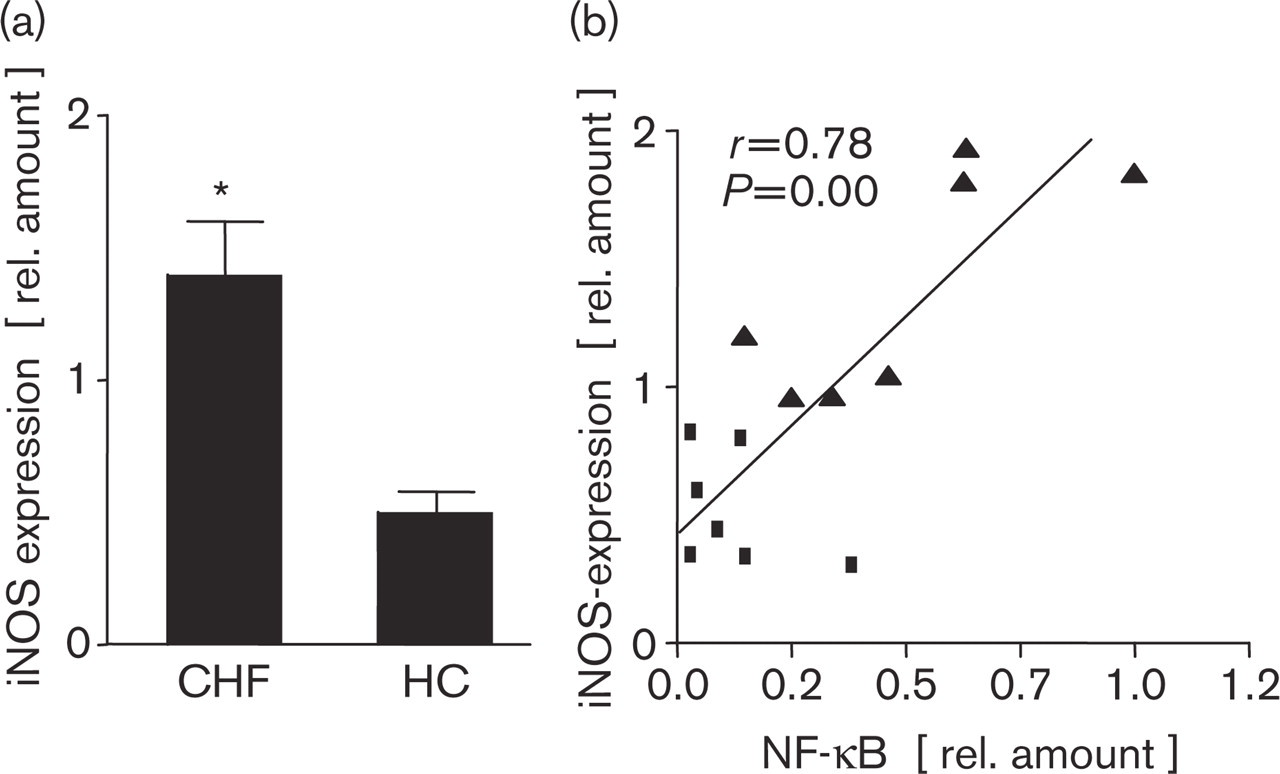
The quantification of iNOS mRNA expression (a) in skeletal muscle of patients with chronic heart failure (CHF) and healthy controls (HC), and a linear correlation between activated NF-κB and iNOS expression (b) is depicted; • = healthy controls, Δ = CHF patients.
Skeletal muscle iNOS expression and its correlation to NF-κB activation
As shown in previous studies [5] the expression of iNOS in the skeletal muscle was significantly increased in biopsies from CHF patients as compared to healthy controls (CHF: 1.4 ± 0.2 versus HC: 0.5 ± 0.08 arbitrary units; P ≤ 0.001) (Fig. 3a).
At least in cell culture experiments it could be demonstrated that the induction of iNOS expression depends on the activation of NF-κB [9]. To investigate this relation in vivo in the skeletal muscle a correlation between NF-κB and the local iNOS expression was analysed. As shown in Fig. 3b a strong linear correlation could be detected between NF-κB activation and the expression of iNOS in skeletal muscle biopsies (r = 0.78, P = 0.008).
Discussion
Two important messages emerge from this study: (1) the amount of activated NF-κB is increased in the skeletal muscle of patients with chronic heart failure, (2) the amount of activated NF-κB correlates with the expression of iNOS in the skeletal muscle supporting the in-vitro findings that iNOS transcription in skeletal muscle is regulated by NF-κB activation. These results suggest that the activation of the transcription factor NF-κB is involved in the regulation of the inflammatory response like iNOS transcription in the skeletal muscle of patients with chronic heart failure.
Recent evidence has suggested, that an inflammatory response participates in the development of heart failure, and NF-κB activation may be an important event in the pathogenesis [18, 22, 23]. Indeed myocardial tissue of patients with CHF exhibited an increased activation of NF-κB and an increased expression of NF-κB-regulated genes like cyclooxygenase-2 [18] or inducible nitric oxide synthase [24]. Besides the molecular, structural and functional alterations in the myocardium, changes in the peripheral skeletal muscle contribute to the exercise-limiting symptoms of the chronic heart failure syndrome. These changes include structural and metabolic alterations as well as the induction of inducible nitric oxide synthase. The linear correlation between the expression of iNOS in the skeletal muscle with the maximal oxygen consumption [6], a measurement for the exercise capacity, implies that iNOS expression is somehow pathophysiologically related to the reduced contractility of the muscle. In animal experiments, at least, the impact of increased synthesis of nitric oxide through induction of iNOS on skeletal muscle contractility could be documented [25]. Due to this pathophysiological link with exercise intolerance, it is of great importance to understand the molecular regulation of iNOS activation and expression. In the last decade evidence has demonstrated that iNOS activation is mainly regulated at the transcriptional level, and cannot be regulated by Ca2+-calmodulin—as it is the case for eNOS, another enzyme of the family of nitric oxide synthases [25, 26]. Studies investigating the structure of the human iNOS-gene promoter revealed the presence of three interferon γ response elements and one NF-κB binding site [27]. In-vitro studies mainly in macrophages, but also in skeletal muscle myoblasts, confirmed the relevance of NF-κB for the lipopolysaacharide or cytokine induction of iNOS [9, 28].
Are these in-vitro studies transferable to the in-vivo situation? At least elevated levels of inflammatory cytokines are detectable in the plasma of CHF patients and are correlated with the severity of the disease [14, 15, 17]. They are considered as pathophysiological stimuli for the observed skeletal muscle alterations, in particular with respect to iNOS expression, which is also significantly increased in the skeletal muscle of CHF-patients [5, 7]. Is NF-κB the intracellular mediator for the cytokine-induced iNOS-expression? The significant increase of NF-κB in the skeletal muscle of patients with CHF as compared to healthy controls and the close linear correlation between the NF-κB and iNOS-expression favour a significant role of NF-κB in the regulation of iNOS expression in vivo in the skeletal muscle.
Besides the regulation and induction of iNOS-expression NF-κB seems to be an important factor for the cytokine-mediated muscle protein degradation [29].
In patients with chronic heart failure muscle wasting is an important feature of the disease especially in advanced stages [30]. In addition to the impact of a reduced expression of local insulin-like growth factor-1 for muscle wasting [31], a TNF-α induced NF-κB mediated induction of factors involved in protein breakdown could be documented in immobilized rats [29] supporting the importance of the up-regulation of NF-κB as shown in this report. A limitation of the present study is the small sample size. Therefore to validate the reported results it will be necessary to confirm the observations in a larger cohort of CHF patients.
In summary, NF-κB activation is increased in the skeletal muscle of patients with chronic heart failure as compared to healthy controls. This activation may lead to the activation of iNOS-transcription, a factor possibly involved in the pathogenesis of exercise intolerance, a key symptom of the syndrome heart failure.