
Abstract
Background
Exercise intolerance and early muscle fatigue are key symptoms in patients with chronic heart failure (CHF). In advanced stages of the disease, profound metabolic abnormalities have been described finally leading to a catabolic state with progressive loss of muscle bulk. The aim of this study was to investigate morphological, functional and electromyographical parameters of the skeletal muscle in CHF.
Methods
We included 17 patients with CHF and 12 age-matched healthy controls (left ventricular ejection fraction 25 ± 2 versus 68 ± 1%, body mass index 26.6 ± 0.8 versus 28.0 ± 1.0 kg/m2; P=NS) in this study. Cross-sectional area (CSA) of the thigh was assessed by computed tomography. Under electromyographical control, maximal and submaximal (30%) isometric strength as well as the relative decrease of muscle strength of the quadriceps muscle over a period of 20 s were determined.
Results
Patients with CHF showed a significant reduction of muscle CSA (134.8 ± 5.3 versus 165.2 ± 7.4 cm2, P=0.002) as compared with healthy controls. The maximal quadriceps muscle strength was found to be significantly reduced in patients with CHF (226.7 ± 22.3 versus 286.9 ± 17.1 N, P<0.05) who also exhibited a higher extent of muscular fatigability (−2.18 ± 0.33 versus − 0.54 ± 0.20 N/s, P<0.01). Electromyographic activity at 30% submaximal contraction showed a lower increase in patients with CHF (66 ± 22 versus 114 ± 36%; P<0.05) indicating impaired muscle fibre recruitment. Furthermore, a significant correlation between muscular fatigability and reduced electromyographic activity was found in CHF (r=0.84; P<0.001).
Conclusions
Our findings demonstrate an impaired electromyographic activity and muscular function in patients with CHF suggesting a new pathomechanism contributing to functional abnormalities of the skeletal muscle in advanced stages of this disease. Eur J Cardiovasc Prevention Rehab 11:155–161 © 2004 The European Society of Cardiology.
Introduction
Patients with chronic heart failure (CHF) show metabolic abnormalities leading to a progressive catabolic syndrome in advanced stages of the disease [1]. In the course of the disease, a variety of organ systems (e.g. lungs, liver and gastrointestinal tract) are affected consequently leading to peripheral abnormalities in addition to an initial cardiac impairment [2]. A key symptom of patients with CHF is a reduced exercise tolerance that is not directly determined by the degree of ventricular dysfunction and only poorly correlates with deteriorated haemodynamic parameters [3]. Exercise intolerance is linked to intrinsic abnormalities of the skeletal muscle [4] and alterations of muscular ultrastructure and function have been extensively investigated in patients with CHF [5–7]. A number of studies revealed a switch from Type I (slow twitch) to Type II (fast twitch) muscle fibres [4], changes in aerobic enzyme distribution from slow towards fast glycolytic isoforms [8], decreased levels of mitochondrial creatine kinase as well as a reduced number of structurally altered mitochondria [4, 9]. Furthermore, distinct changes in muscular gene expression that are not explained by reduced activity [10] and increased muscular levels of oxidative stress [11] have been demonstrated in CHF. Intriguingly, progressive loss of muscle bulk is associated with an increased mortality in patients with CHF [12].
Muscular activity is coordinated through neuromuscular coupling where axonal impulses are transmitted to skeletal myocytes leading to membrane depolarization that results in calcium (Ca2+) influx from the sarcoplasmic reticulum (SR) and myocyte contraction. In turn, Ca2+ is transported from the cytoplasm to the SR through the ATP-dependent action of the SR ATPase (SERCA) [13]. In CHF, muscular contractile function is impaired [14], at least in part through a reduction of muscular levels of SERCA, leading to increased cytoplasmic Ca2+ levels in patients with CHF [15]. However, neuromuscular function and myographic activity as well as their role in progressive muscular abnormalities in CHF have not been conclusively investigated so far. To date, only a small number of studies have systematically analysed neurophysiological parameters in patients with CHF [16–19]. The aim of our study was to investigate neuromuscular parameters in addition to the assessment of functional and morphological abnormalities of the skeletal muscle in patients with advanced CHF.
Methods
Study protocol
Seventeen male patients (age 60 ± 3 years) with chronic heart failure (NYHA – functional class II-IV) because of dilated cardiomyopathy (DCM, n=7, 41%) or ischaemic heart disease (IHD, n=10, 59%) were included in this study. All CHF patients had clinical, radiological and echocardiographic signs of chronic heart failure and a reduced left ventricular ejection fraction (LVEF) of ≤ 40% as assessed by angiography.
Exclusion criteria were primary valvular heart disease, uncontrolled hypertension (Psyst > 150 mmHg, Pdiast > 95 mmHg), peripheral vascular disease, chronic obstructive pulmonary disease, diabetes mellitus (increased values of HbA1c and/or increased fasting glucose levels), immunosuppressive therapy, renal failure (increased values of creatinine), and/or musculoskeletal conditions limiting exercise capacity (i.e. rheumatoid arthritis).
Twelve age-matched male patients (age 59 ± 1 years) without evidence of coronary artery disease served as controls. They were normal by physical examination, electrocardiogram (ECG), chest X-ray, two-dimensional echocardiography, coronary angiography and left ventriculogram (LVEF 68 ± 1%). Control subjects had no evidence of hypertension and had normal findings on routine haematologic and biochemical blood analyses. No previous major medical illness was reported (including diabetes or cardiovascular disease) and they were on no medication during the study.
The protocol of this study was approved by the Ethics Committee of the University of Leipzig, and written informed consent was obtained from all individuals prior to enrolment.
Exercise testing and respiratory variables
Exercise testing was performed on a calibrated, electronically braked bicycle in upright position with workload increasing progressively every 3 min in steps of 25 W beginning at 25 W. Respiratory gas exchange data were determined continuously throughout the exercise test as previously described [9].
Determination of lower limb muscle cross-sectional area
Skeletal muscle cross-sectional area of the thigh was measured by high-resolution computed tomography at the mid-thigh level as described previously [20]. Using a Somatom Plus 4 CT-scanner (Siemens, Erlangen, Germany), sections were made halfway between the major trochanter and the medial condylus of the femur (slice thickness 5 mm, 130 mA). Cross-sectional area was determined by manual tracing using the built-in CT software (VB 40 C).
Determination of quadriceps muscle function
Maximal isometric tension development and muscle fatigability were measured in the quadriceps muscle of all individuals. Patients were seated on a chair under ECG, haemodynamic, and electromyographic monitoring. Using a calibrated isometric force transducer (Mechanotronik, Hagen, Germany) with a minimal resolution of < 1 N, peak force at maximal voluntary quadriceps contraction for 20 s was quantified five times with 1-min resting intervals. Peak force and decrease of force over 20 s were averaged for the five repetitions.
Electromyographic assessment
Electromyographic activity of the quadriceps muscle was assessed using skin-attached removable surface electrodes connected to a transportable computer unit for data storage (Muscle Tester EMG, ME 3000 P; MEGA Inc., Kyopio, Finland). After calibration, electromyographic activity was measured over 20 s of maximal isometric muscle strength in five repetitions under the observation of a trained investigator. Number of bursts per ms, maximal amplitude of muscular bursts and the decrease in burst amplitude were assessed over the testing period [21].
Measurement of serum parameters
Blood samples were collected in the morning after a fasting period of 12 h. An antecubital polyethylene catheter was inserted and after supine rest of at least 20 min, 25 ml of venous blood were drawn. After immediate centrifugation at 4°C, aliquots were stored at −80°C. Serum was taken for routine laboratory measurements as well as the assessment of circulating levels of TNFα in all individuals. Serum concentrations of TNFα were measured by a specific high-sensitivity enzyme-linked immunoadsorbent assay kit (Quantakine, R&D Systems, Minneapolis, USA) with a sensitivity of < 0.18 pg/ml. All samples were run in duplicate and the average value of the two measurements was reported.
Statistical analysis
Mean value ± standard error was calculated for all variables. Intergroup comparisons were performed by using Student's t-test if appropriate or otherwise the non-parametric Mann–Whitney U-test, and by one-way ANOVA with corresponding post-hoc tests for more than two groups, respectively. A P-value of less than 0.05 was considered statistically significant.
Results
Patient characteristics
Seventeen patients with CHF (60 ± 3 years, LVEF 25 ± 2%) and 12 healthy age-matched controls (59 ± 1 years, LVEF 68 ± 1%) were enrolled in the study. The height of the patients was 173.5 ± 8.1 versus 177.1 ± 6.2 cm in controls (P=NS). The total body mass of patients was 80.4 ± 13.2 versus 87.8 ± 9.5 kg in controls (P=NS). Ten patients were diagnosed with post-ischaemic CHF (59%) and seven patients with dilated cardiomyopathy (41%). LVEF was not significantly different between dilated or ischaemic cardiomyopathy (27 ± 2 versus 23 ± 2%, P=NS). Maximal oxygen uptake (VO2 max) as determined by bicycle ergospirometry was significantly reduced in patients with CHF (15.4 ± 0.7 versus 25.9 ± 1.6 ml/kg·min in controls, P < 0.001). No significant difference in exercise capacity was noted in patients with ischaemic heart disease as compared with patients with dilated cardiomyopathy (16.6 ± 1.0 versus 14.2 ± 1.0 ml/kg·min, P=NS) (Table 1).
Characteristics of patients with CHF and controls
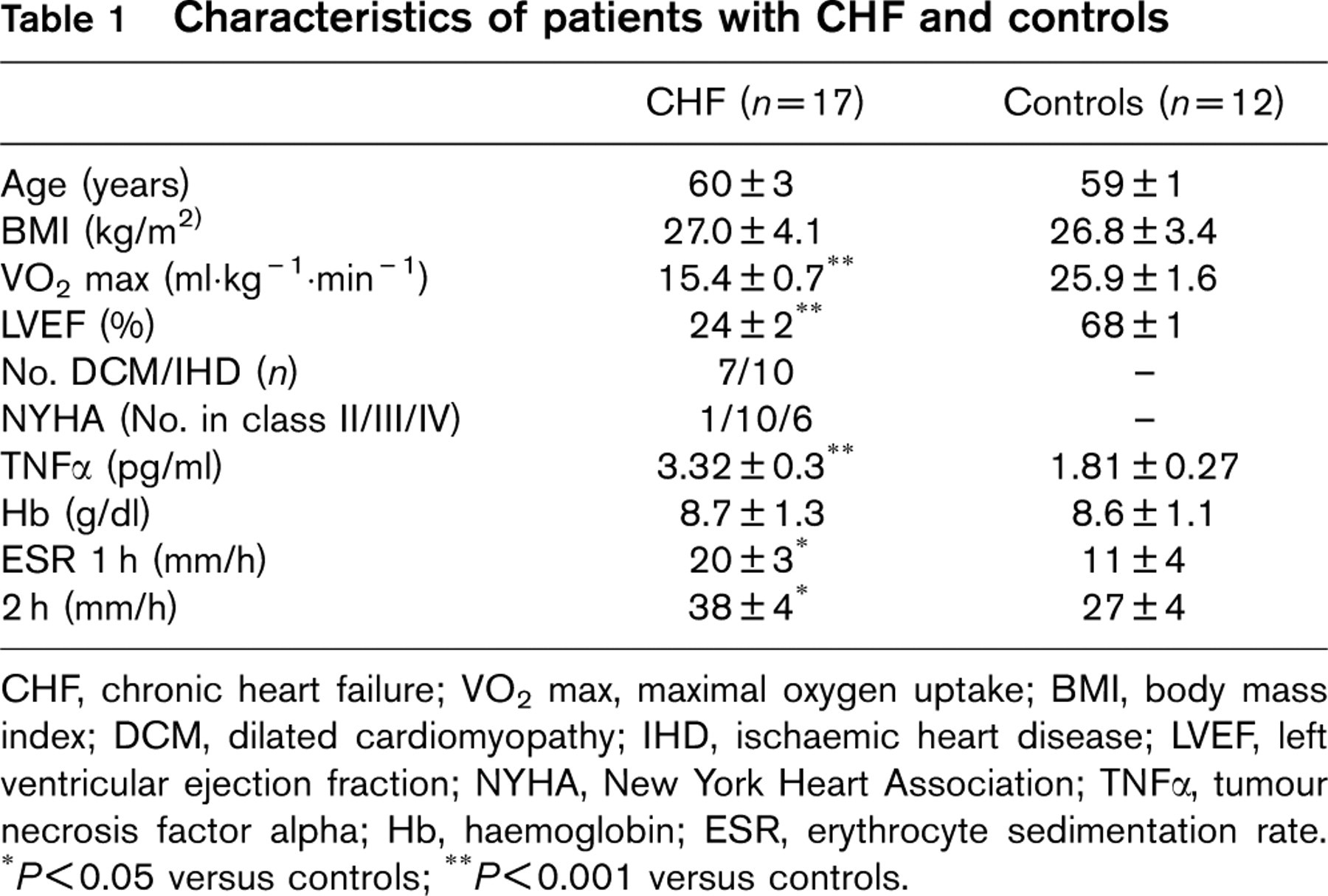
CHF, chronic heart failure; VO2 max, maximal oxygen uptake; BMI, body mass index; DCM, dilated cardiomyopathy; IHD, ischaemic heart disease; LVEF, left ventricular ejection fraction; NYHA, New York Heart Association; TNFα, tumour necrosis factor alpha; Hb, haemoglobin; ESR, erythrocyte sedimentation rate. ∗P<0.05 versus controls; ∗∗P<0.001 versus controls.
Fifteen CHF patients (88%) received angiotensin-converting enzyme inhibitors, 13 (77%) were on diuretic medication, 11 (65%) on digitalis and nine (53%) on beta-receptor blockers. Medication was not found to be significantly different between patients with post-ischaemic versus dilated cardiomyopathy.
Assessment of skeletal muscle cross-sectional area
Total skeletal muscle cross-sectional area of the thigh decreased in patients with CHF as compared with controls (132.7 ± 7.5 versus 165.6 ± 4.8 cm2, P=0.003). No significant difference in total fat area were found between the two groups (59.4 ± 4.5 versus 57.5 ± 3.7 cm2, P=NS) (Fig. 1a).
Activation of inflammatory parameters
Cytokine levels were systemically elevated in CHF (TNFα: 3.32 ± 0.30 pg/ml in CHF versus 1.81 ± 0.27 pg/ml in controls; P=0.001). Patients with ischaemic cardiomyopathy showed a trend towards higher serum levels of TNFα as compared with patients with dilated cardiomyopathy (TNFα: 3.68 ± 0.42 pg/ml in ICM versus 2.80 ± 0.34 pg/ml in DCM; P=0.1). Erythrocyte sedimentation rate (ESR) exhibited a significant elevation after 1 and 2 h in patients with CHF as compared with controls (20 ± 3 and 38 ± 4 mm in CHF versus 11 ± 1 and 27 ± 4 mm in HC; both P<0.05 respectively) (Table 1 and Fig. 1b).
Correlation between skeletal muscle cross-sectional area and serum levels of TNFα
Patients with CHF exhibited a significant correlation between serum levels of the pro-inflammatory cytokine TNFα and skeletal muscle cross-sectional area of the thigh (r= −0.592; P=0.01) (Fig. 1c).
Measurement of skeletal muscle isometric contractility
Patients with CHF showed a significant decrease in maximal isometric muscle strength as compared with healthy controls (309.8 ± 20.6 versus 249.8 ± 18.2 N, P<0.05). Furthermore, patients with CHF exhibited a significant decrease in maximal isometric muscle strength per second as a parameter of skeletal muscle fatigability as compared with healthy controls (−2.27 ± 0.34 versus −0.55 ± 0.19 N/s, P < 0.0001) (Fig. 2a and b).
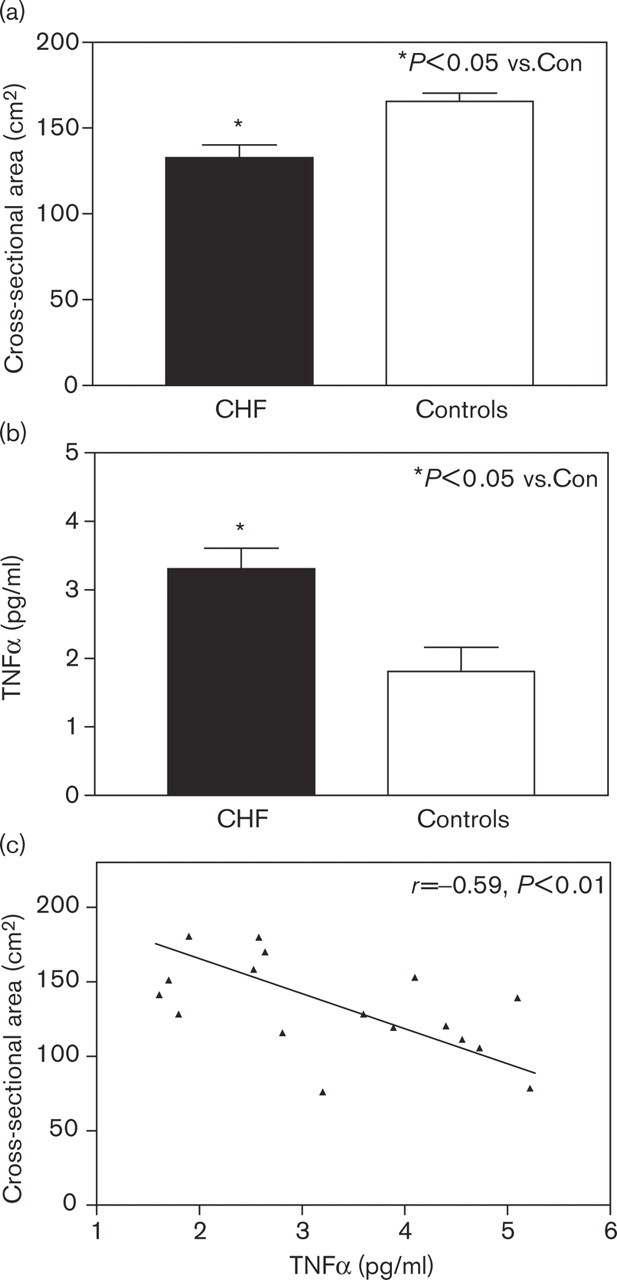
Serum level of TNFα and skeletal muscle bulk. (a) Serum concentration of TNFα demonstrates a significant proinflammatory activation in patients with chronic heart failure as compared with controls (∗P<0.05 versus controls). (b) Skeletal muscle cross-sectional area of the thigh shows a reduction in advanced chronic heart failure (∗P<0.05 versus controls). (c) In the subgroup of patients with chronic heart failure, a linear correlation was found between increased serum levels of TNFα and reduction in muscle cross-sectional area (r= −0.59; P<0.01).
Electromyographic activity of the quadriceps muscle
In patients with CHF, the assessment of electromyographic activity revealed a pronounced reduction in the amplitude of muscular bursts at maximal isometric contraction as compared with controls (0.076 ± 0.01 versus 0.012 ± 0.008 mV/s; P < 0.001). In addition, electromyographic activity at 30% submaximal isometric contraction showed a reduced increase in patients with CHF (89.7 ± 9.7 versus 177.5 ± 25.2% in controls; P < 0.001) indicating an impaired muscle fibre recruitment (Fig. 3a and b). No significant differences of electromyographic activity were found between patients in regard to NYHA class of CHF.
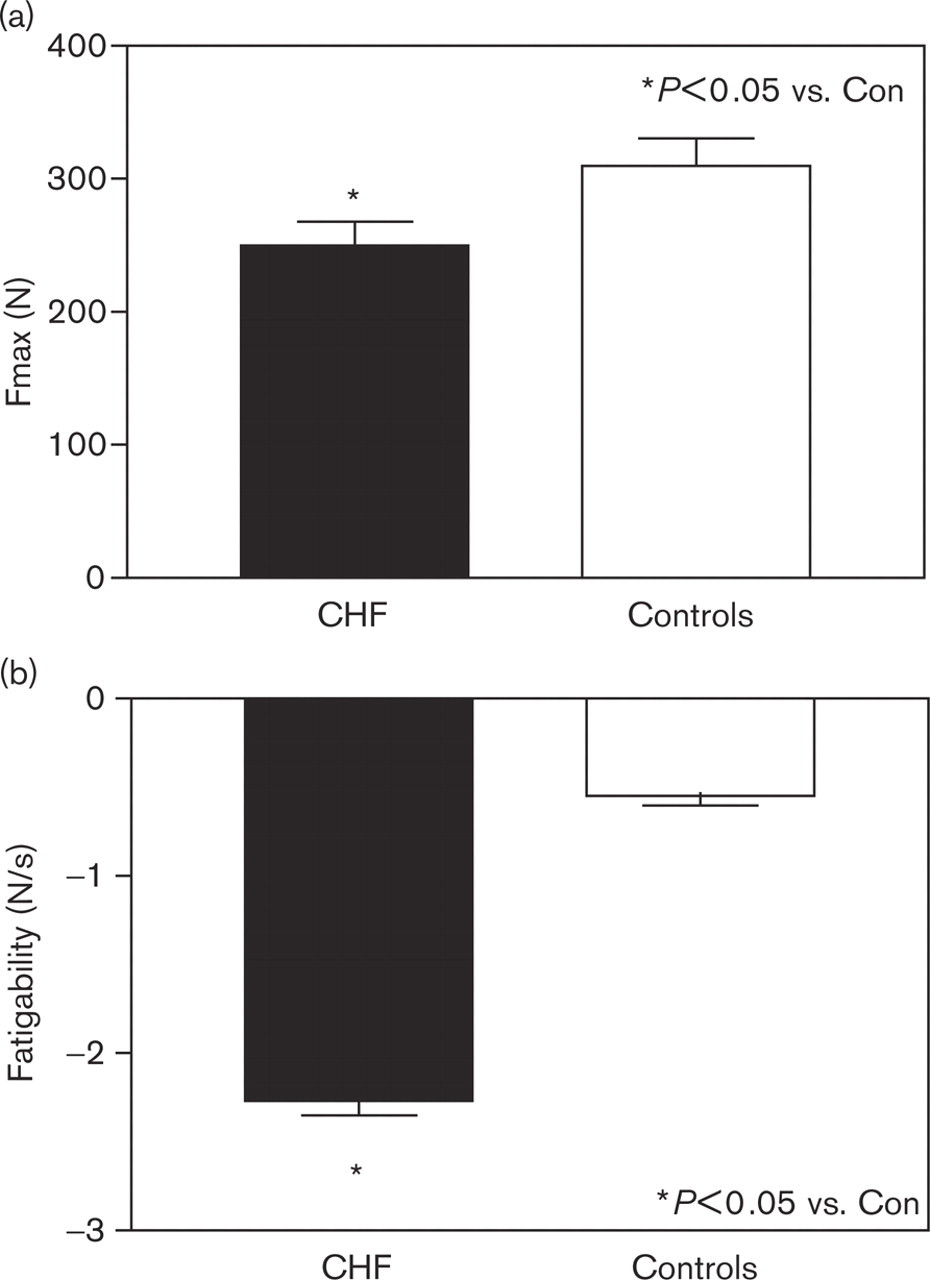
Assessment of skeletal muscle function. (a) Maximal isometric force is reduced in patients with chronic heart failure as compared with controls (∗P<0.05 versus controls). (b) In addition, patients with chronic heart failure exhibit an increased fatigability of maximal isometric contractility over the testing period of 20 s (∗P<0.05 versus controls).
Correlation between skeletal muscle fatigability and electromyographic activity in patients with CHF
Skeletal muscle fatigability and reduction of electromyographic activity of the quadriceps muscle over the testing period of 20 s at peak isometric contraction showed a significant correlation in patients with CHF (r = 0.832; P < 0.0001) (Fig. 4).
Discussion
Reduced exercise tolerance and early muscular fatigue are major clinical symptoms of patients with CHF and have been attributed to intrinsic abnormalities of skeletal muscle function and morphology [4, 5, 22]. In the current study, we have shown a reduction of muscle isometric contractility accompanied by loss of muscle bulk that correlates to increased serum levels of TNFα in patients with CHF. Furthermore, electromyographical assessment revealed impaired muscle fibre recruitment at submaximal muscular contraction and a pronounced decrease in neuromuscular activity at maximal isometric contraction. These findings support the hypothesis of a muscular impairment in addition to intrinsic skeletal muscle abnormalities in the clinical syndrome of CHF.
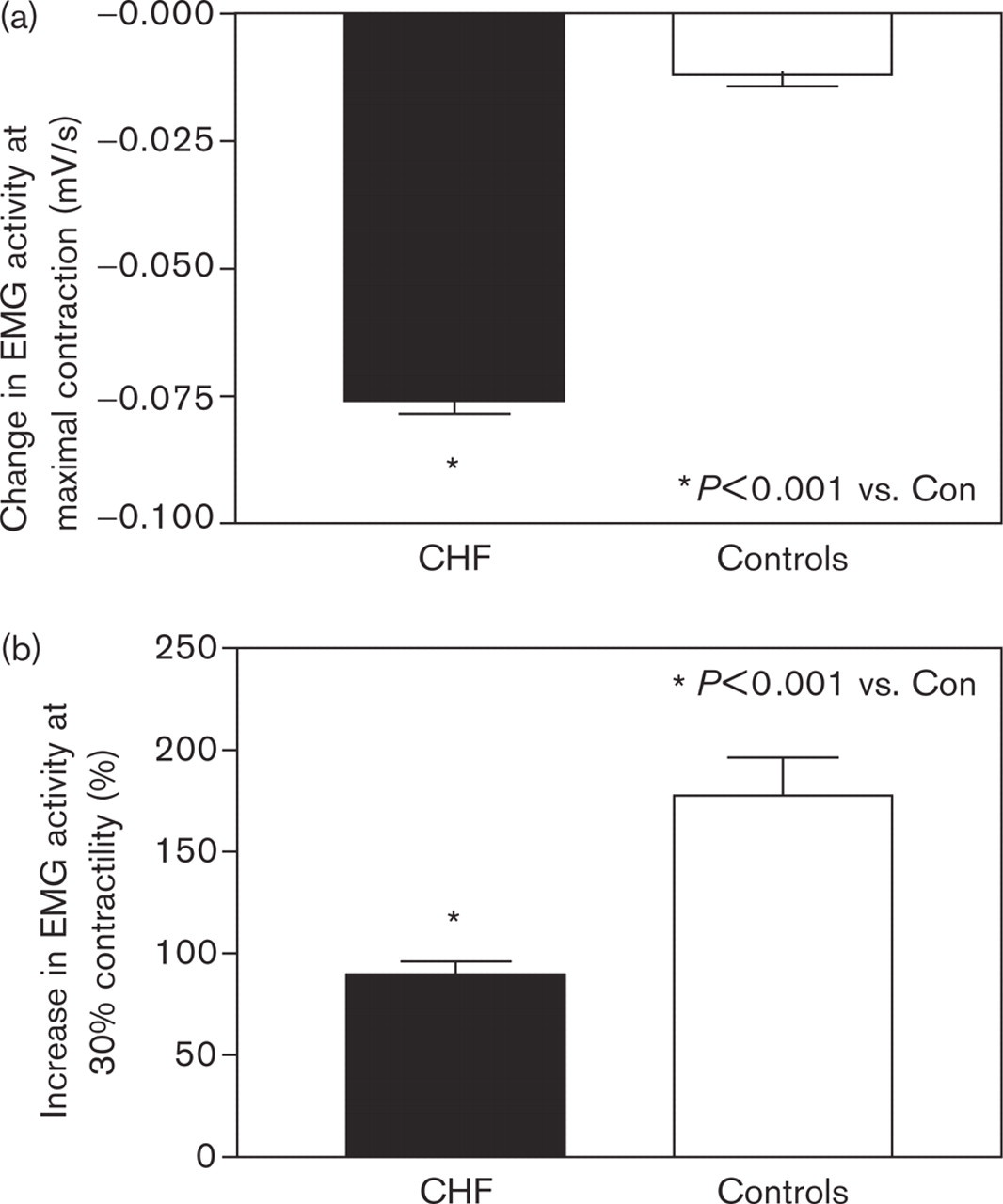
Electromyographic activity of the quadriceps muscle at isometric contraction. (a) In patients with chronic heart failure, the assessment of electromyographic activity at maximal isometric contraction revealed a pronounced decrease over 20 s as compared with controls (∗P<0.001 versus controls). (b) At 30% submaximal isometric contraction, a reduced increase in electromyographic activity revealed an inhibition of muscle fibre recruitment in patients with chronic heart failure as compared with controls (∗P<0.001 versus controls).
Metabolic abnormalities in CHF affect various endocrine systems leading to an imbalance of catabolic and anabolic function that result in a progressive catabolic state in advanced stages of the disease. Systemic abnormalities in CHF are at least partially associated with decreased physical activity of patients due to the disease, however, other factors such as an increased energy expenditure [23], insulin resistance [24] and increased levels of oxidative stress [25] have been observed in CHF. The neurohumoral activation is accompanied by increased serum levels of proinflammatory cytokines (e.g. TNFα, IL-1β, and IL-6) [26], the activation of the renin–angiotensin–aldosterone-system (RAAS) [27] and catecholamines [28]. Recently, we could demonstrate a correlation of increased serum levels of the adipocyte-derived cytokine leptin and the neurohumoral activation in patients with advanced CHF [29]. In addition, low serum levels of anabolic IGF-I and loss of lean muscle mass consistent with a peripheral GH resistance occur in advanced CHF [30].
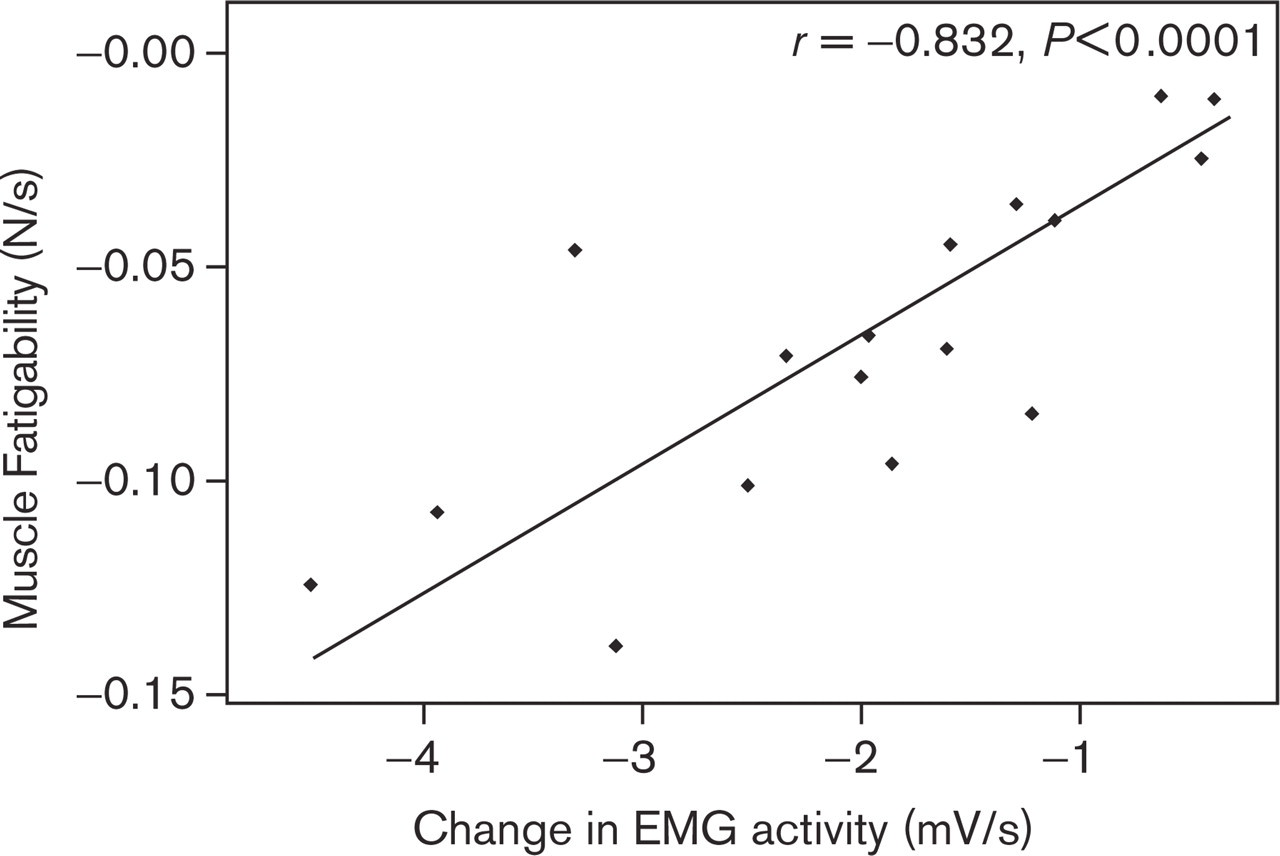
Correlation of reduced electromyographic activity and muscular fatigability. Over the testing period of 20 s, patients with chronic heart failure exhibit a close correlation of decrease in electromyographic activity and muscular fatigability (r=0.832; P<0.0001).
In the current study, we demonstrate a close correlation of circulating levels of TNFα and reduced skeletal muscle CSA in patients with CHF. This is well in line with previous findings that demonstrated a correlation between systemic markers of inflammation and signs of muscular atrophy in other chronic illnesses [1, 31]. Both, proinflammatory cytokines and IGF-1 have been implicated in the development of myopathic alterations in chronic diseases such as cancer [32], renal failure [33] and CHF [1, 30, 31]. Intriguingly, TNFα induces a catabolic metabolism as well as muscular atrophy and reduces skeletal muscle contractility in experimental studies [34].
Functional and morphological skeletal muscle abnormalities have been extensively investigated in patients with CHF [4, 5, 8, 16, 35]. Fibre type distribution, quantities of glycolytic enzymes and contractile structures are specific for different types of muscles and define the efficiency of muscle work [13, 21]. It has been shown that the syndrome of CHF is accompanied by intrinsic skeletal muscle alterations even in early stages of the disease that include a switch from Type I (slow twitch muscle fibres) to Type II (fast twitch muscle fibres) fibres [4, 36]. In addition, changes in aerobic enzyme distribution towards fast glycolytic isoforms from slow glycolytic isoforms [8] and alterations in skeletal muscle energy expenditure due to decreased levels of mitochondrial creatine kinase [22] as well as increased levels of oxidative stress have been demonstrated in the skeletal muscle of CHF [11]. Furthermore, a decreased number and structurally altered mitochondria have been found in skeletal muscle biopsies obtained from patients with CHF [4, 22]. Altogether, these alterations might contribute to a decrease in maximal muscle strength and increased skeletal muscle fatigability in addition to muscular atrophy as demonstrated in the present study.
Pronounced muscular fatigability is a key syndrome in patients with CHF. The physiological muscle activation depends on central nervous stimulation, neuromuscular transmission and intramuscular conductance [13, 21]. Central fatigue with reduced central motor drive has been shown in the chronic fatigue syndrome but not in CHF [16]. Moreover, no significant difference was found in neuromuscular transmission assessed through a single tetanic nerve stimulation in a previous study on patients with CHF [16]. However, no study has investigated electromyographic activity as an indicator of intramuscular post-axonal stimulation. The current study included the continuous measurement of quadriceps electromyographic activity during maximal and 30% submaximal isometric contraction. In the light of rare total activation of muscle force in patients with advanced CHF, functional testing at 30% submaximal isometric contraction seems to represent a more realistic indicator of muscular function. The pronounced decrease of EMG signal intensity at maximal isometric contraction in patients with CHF and its close correlation to muscular fatigability indicates an impairment of intramuscular excitation in CHF. In addition, muscle fibre recruitment at 30% submaximal contraction is abnormal in patients with CHF. However, a limitation of the present study is the absence of an EMG power spectrum analysis and the assessment of EMG signal frequency as previously performed by other groups [37, 38].
In conclusion, the findings of the present study demonstrate functional, morphological and electromyographical abnormalities of the skeletal muscle in patients with chronic heart failure. Systemic catabolic alterations in advanced CHF are accompanied by skeletal muscle atrophy and impaired muscular function. Furthermore, an additional impairment of muscular function is indicated by an altered electromyographic activity in patients with CHF. Our findings suggest a new pathomechanism contributing to functional abnormalities of the skeletal muscle in advanced stages of CHF.