
Abstract
Coronary heart disease (CHD) is the leading cause of mortality in the industrialized world and that might also soon be the case in other parts of the world. There are several easily measured and potentially modifiable risk factors that account for a substantial proportion of the risk of CHD. The effect of risk factors interventions appears to be consistent in both genders, across different geographic regions, and by all ethnic groups, suggesting that approaches to prevention can be based on similar principles worldwide. Optimal target levels for serum cholesterol and blood pressure are not yet clear. Future risk CHD reduction will mainly be achieved by improved primary prevention.
Introduction
Coronary heart disease (CHD) is the leading cause of mortality in the industrialized world and that might also soon be the case in other parts of the world.
Treatment of myocardial infarction (MI) has changed dramatically during the last 2 decades. Invasive interventions and aggressive pharmacological treatment are standard options for MI treatment nowadays. Hand in hand with the improved treatment, the hospital mortality rates have decreased dramatically. The treatment of an acute MI will probably continue to improve; however, the big challenge for the future will be the primary prevention. There are a lot of data demonstrating that occurrence of CHD relates strongly to modifiable physiological and biochemical factors and risk factor modifications have been shown to reduce CHD mortality and morbidity, particularly in high-risk patients.
Risk Factors
Multiple epidemiological studies have confirmed that the following risk factors account for the majority of CHD cases (Table 1 ).
Coronary Heart Disease Risk Factors
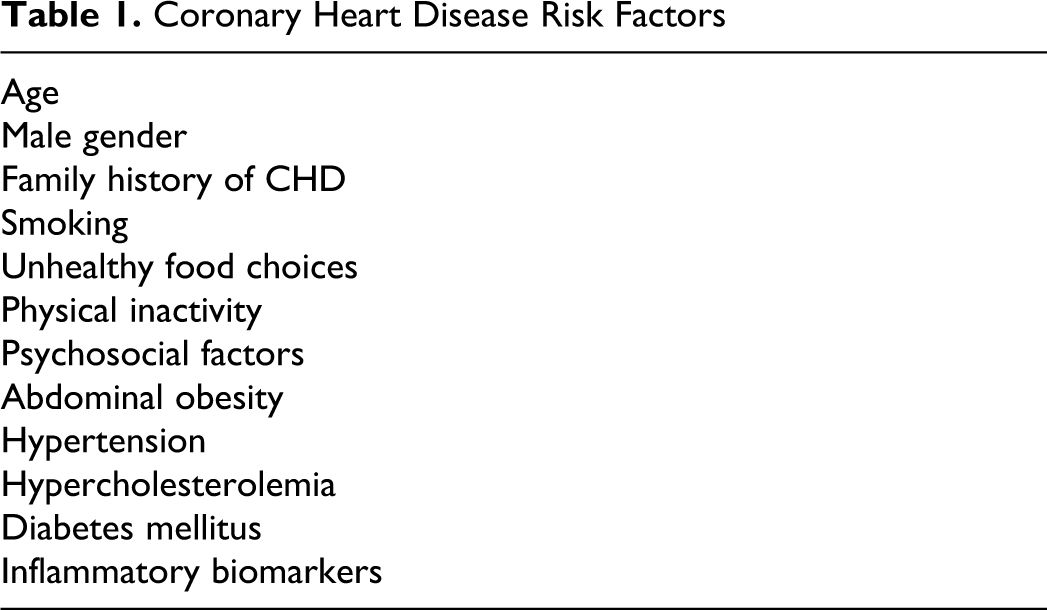
Nonmodifiable Factors
Age, male gender, and family history of CHD cannot be modified. The coronary risk increases with age and men suffer from CHD earlier in life than women. Importantly, 10% to 15% of patients with CHD have no apparent major CHD risk factors.1–2
Modifiable Factors
Smoking
Cigarette smoking represents the most important source of preventable morbidity and premature mortality worldwide. Smoking is responsible for 50% of all avoidable deaths and one half of these are due to cardiovascular disease (CVD).3–4 There is a graded relationship between CHD risk and smoking. Even smoking a few cigarettes daily is associated with an increased risk.2,5 Thus, there is no safe level of smoking and if quitting is not possible, the risk of MI associated with smoking could be significantly reduced by a reduction in the numbers of cigarettes smoked.2,5 Furthermore, the effects of smoking on CHD interact synergistically in the presence of other cardiovascular risk factors, making quitting even more important. Also, passive smoking has been shown to increase the risk of CHD and other smoking-related diseases. 6
The benefits of smoking cessation are well established.5,7 Smoking cessation leads to a quick reduction in the risk of subsequent CHD events in patients with established cardiovascular disease (CVD): the risk falls within 2 to 3 years to the level of those patients with CHD who never smoked. 8 It is potentially the most effective of all preventive measures after an MI.
In clinical practice, the assessment of smoking status should be done at every opportunity. Stopping smoking should be encouraged in all smokers. There is no age limit to the benefits of smoking cessation. The physician’s explicit advice that a person should stop smoking completely is the most important factor in getting the smoking cessation process started. Both individual and group behavioral interventions are effective in helping smokers to quit. 9 The momentum for smoking cessation is particularly strong at the time of diagnosing atherothrombotic CVD, but obviously the best way is to quit before the patient suffers from a cardiovascular event.
Quit rates in clinical studies are very low, averaging only around 2% among those attempting cessation without pharmacotherapy or counseling. Therefore, pharmacologic smoking cessation aids are recommended for all smokers who are trying to quit, unless contraindicated. Evidence-based guidelines recommend nicotine replacement therapy, bupropion, and varenicline as effective alternatives for smoking cessation therapy, especially when combined with behavioral interventions.5,10 Combination pharmacotherapy is indicated for highly nicotine-dependent smokers, patients who have failed with monotherapy.5,10 The rate of successful smoking cessation at 1 year is 7% to 16% if the smoker undergoes behavioral intervention, and up to 24% when receiving pharmacological treatment and behavioral support. 11
As cigarette smoking is a major general health problem and society has a responsibility to discourage smoking by taxes and laws. Already after a few years, we know that smoking bans in public places and workplaces are significantly associated with a reduction in MI incidence, particularly if enforced over several years. 12
Unhealthy Food Choices
Diet plays an important part in the maintenance of optimal cardiovascular health. In the INTERHEART study, 2 regular consumption of fruits and vegetables was associated with a 30% relative risk reduction. However, there are a lot of confounding factors. Fruit and vegetable intake is associated with particular lifestyle characteristics that might also confer protection against CHD. As these confounders are not adequately controlled in observational studies, the conclusion that a causal relationship exists between fruit and vegetable intake and CHD prevention is not obvious. 2
Similar observations have been reported in US Nurses Health Study 13 and Lyon Heart Study. 14 In the latter study, participants in the Mediterranean diet group supplemented with α-linoleic benefited from a substantial reduced relative risk for fatal and nonfatal MI, compared with the control group who followed a standard low-fat diet. These findings were independent of lipid levels and blood pressure (BP). The mechanism for this risk reduction is unclear and it is neither clear what contents in the diet are responsible for the positive effect.
Omega-3 polyunsaturated fatty acid therapy has shown positive outcome in primary and particularly in secondary prevention of cardiovascular CVD. Based on results from the Gruppo Italiano per lo Studio della Sopravvivenza nell’Infarto (GISSI)-Prevenzione study, 15 American Heart Association (AHA) dietary guidelines recommend combined eicosapentaenoic acid (EPA), and docosahexaenoic acid (DHA) in a dose of approximately 1000 mg/day in patients with CHD. 16 For those individuals without CHD, the AHA recommends 2 oily fish meals per week. However, recently an additional daily intake, added in margarine, of 400 mg of EPA + DHA and 2 g of α-linolenic acid (ALA) on CVD in participants with a history of MI had no effect on the outcome. 17
The 2005 US Dietary Guidelines for Americans recommend that consumption of red and processed meat should be moderated. 18 Such recommendations are in large part derived from the expected effects of saturated fat in meat on low-density lipoprotein and total cholesterol levels. However, data are not consistent. Red versus processed meats may have some important nutritional differences, such as in the contents of calories and specific fats. In a recent large meta-analysis, 19 consumption of processed meats, but not red meats, was associated with higher incidence of CHD.
There are data from epidemiological studies, including the INTERHEART study, 2 informing us that a moderate alcohol consumption is associated with a protective effect against CHD. However, the “therapeutic” window is narrow since a larger consumption enhances the risk of other diseases such as strokes, liver cirrhosis, and injuries.20,21For lipid, glucose, and obesity management, see below.
Physical Inactivity and Abdominal Obesity
Regular exercise results in an increase in exercise capacity and lower myocardial oxygen demand, leading to cardiovascular benefits such as lower mortality rates and fewer symptoms of CHD. There was a significant reduction in cardiovascular morbidity and mortality in participants with exercise energy expenditures of more than 2000 kcal per week in male Harvard University alumni without a history of CVD who were followed for 16 years. 22 In a meta-analysis of 10 randomized clinical trials that examined the effects of cardiac rehabilitation after MI, a reduction in cardiovascular mortality among exercise rehabilitation patients compared with controls was found. 23 Also, in the INTERHEART study, 2 physical inactivity was associated with CHD. In the European Society of Cardiology guidelines, it is stated that the ultimate goal is at least 30 minutes of physical activity on most days of the week as almost any increase in activity is associated with measurable health benefits. The intensity may be defined in terms of target heart rate or perceived exertion. A heart rate during peak exercise of 60% to 75% of the average maximum heart rate is suggested. 24
The prevalence of obesity is increasing in both children and adults worldwide. Since obesity with body mass index (BMI) >30 kg/m2 is associated with increased mortality, this is a major health problem. The relationship between BMI and mortality, including cardiovascular mortality, has been suggested to be J-shaped and an excess risk is noted in the lower end as well as in the upper end of the distribution of BMI. 25
Adiposity can be crudely quantified by calculating BMI, which is calculated as weight in kilograms divided by height in meters squared. 26 However, BMI does not give an indication as to how this fat is distributed in the body.26,27 Body fat is stored in various depots, with over 85% of fat stored subcutaneously and around 10% stored in the viscera. 26 Regional distribution of adipose tissue may be more important in determining cardiovascular risk than total body weight.26,27 Excess abdominal fat in particular has been shown to be strongly associated with metabolic and cardiovascular risk.26–28 Because measures such as waist circumference (WC) and waist-hip ratio are known correlates of visceral fat mass, these simple measures may be used for the assessment of CHD risk.26,28 There is no solid evidence for superiority of either variable in the prediction of coronary risk. Waist circumference has the advantage of simplicity, may be a slightly better estimator of risk than BMI, but is probably more prone to measurement error. Physical activity has been shown to have impact on abdominal fat metabolism before weight loss occurs, which emphasize the relevance of physical activity in this matter. 29
Measurement of WC in addition to BMI gives additional information for CVD risk estimation. Reports from WHO and the American National Heart, Lung, and Blood Institute (NHLBI) expert panel on Obesity recommend the use of WC as an additional indicator of metabolic risk factors, within each category of BMI.26,28 Thus, abdominal obesity may be considered as an independent risk factor that can potentially be used to improve CHD risk assessment in the clinical setting. The American Heart association and European Heart Association state that Caucasian men with WC above 102 cm and women above 88 cm are advised to lose weight.24,26 However, it is obvious that different cutoff points for anthropometric measurements are required in different races and ethnicities. 30
Psychosocial Factors
There are data suggesting that psychosocial factors contribute independently to the risk of CHD even after statistical adjustments for the effects of standard risk factors. The following psychosocial risk factors have been shown to influence the risk of CHD: low socio-economic status, social isolation and lack of social support, stress at work and in family life, and negative emotions including depression and hostility.
These factors tend to cluster in the same individuals and in addition the traditional cardiovascular risk factors, such as smoking, overweight, physical inactivity, and hypertension, tend to cluster in these groups of patients. 2 Furthermore, depressed individuals are less compliant with their medical regimen and lifestyle risk factor modifications. 31
The AHA has recommended routine screening for depression in patients with CHD in clinical practice. However, no clinical trials have assessed whether screening for depression improves depressive symptoms or cardiac outcomes in patients with CVD. The large Enhancing Recovery in Coronary Heart Disease Patients (ENRICHD) trial intervened on depression and low perceived social support soon after MI. 32 The intervention, with cognitive behavior therapy, supplemented with a selective serotonin reuptake inhibitor (SSRI) antidepressant when indicated, did not increase event-free survival, but it did improve depression and social isolation. Furthermore, in a recent meta-analysis, depression treatment with medication or cognitive behavioral therapy in patients with CVD was associated with modest improvement in depressive symptoms but no improvement in cardiac outcomes. 33 Thus, the role of depression as an etiologic or prognostic factor in CHD continues to remain controversial. It is well documented that the correlation between these 2 entities does not entitle it to be causative in nature.
In the Heart and Soul Study, 34 the association between depressive symptoms and cardiovascular events was largely explained by health behaviors, especially physical inactivity. These results suggest that this relationship might be modifiable with behavioral interventions.
Psychosocial factors not directly related to depression appear to increase CHD risk. In a meta-analysis, the association between anger and hostility and CHD in prospective cohort studies was examined. They found that anger and hostility were associated with increased CHD events in the healthy population studies. 35 There are also data supporting that therapeutic and preventive intervention methods that counteract psychosocial risk factors and promote healthy behaviors and lifestyle reduce cardiovascular mortality and morbidity.36,37
Hypertension
Elevated BP is a risk factor for CHD and stroke. The task force for the management of arterial hypertension of the European Society of Hypertension (ESH) and of the European Society of Cardiology (ESC) suggest 120/80 mm Hg as the optimal BP, whereas 140/90 mm Hg is the cutoff level for the definition of hypertension. 38 These levels have, however, been questioned recently since large clinical outcomes trials have shown that the aggressive treatment of systolic and diastolic BP is associated with increases in CVD complications. In a Japanese study of elderly hypertensive patients, there was no difference regarding the incidence of the primary end point of CVD and renal failure between those randomized to systolic BP reduction <140 mm Hg and those randomized to ≥140 mm Hg. 39 Similar observations were also reported in the ACCORD trial, 40 in which patients with type 2 diabetes mellitus were randomized to systolic BP of <120 or <140 mm Hg and followed for 4.7 years. At the end of the study, there was no difference in cardiovascular events between the 2 groups, and the aggressively treated group had significantly more side effects than the more conservatively treated group.
Whereas there seems to be a linear relationship between diastolic BP and risk of stroke, the relationship between diastolic BP and risk of CHD appears to be J-shaped. The J-curve phenomenon describes a situation whereby cardiovascular complications increase when diastolic BP is lowered below a certain point. In most studies, the J-curve effect has been observed with diastolic BP. However, 2 recent large clinical outcomes trials observed J-curve relationships with systolic BP besides diastolic BP and cardiovascular complications.41,42 In these studies, J-curve effects were observed with systolic BP ≤130 mm Hg and diastolic BP ≤80 mm Hg for cardiovascular complications, but not stroke complications. In an analysis comprising 48 000 patients with hypertension, a definite J-curve effect with a threshold diastolic BP of 85 mm Hg and increased cardiovascular mortality, but not stroke, was observed. 43 Coronary artery perfusion happens mainly during the diastolic phase of the cardiac cycle and therefore there is an association between diastolic BP and coronary perfusion. Coronary artery perfusion depends on the pressure gradient between the coronary arteries and the left ventricle in diastole, and thus lowering diastolic BP may cause decreased coronary flow.
A huge number of placebo-controlled trials have conclusively demonstrated that BP reduction lowers CHD morbidity and mortality in hypertensive populations. 38 The primary goal of treatment of a hypertensive patient is to achieve the maximum reduction in the long-term cardiovascular risk and therefore treatment of all reversible risk factors should be executed. 44 The decision to start antihypertensive drug treatment depends on total CVD risk, which may be calculated with risk scores. 25 The main benefits of antihypertensive treatment are owing to lowering of BP per se, rather than choice of drug type.
Hypercholesterolemia
Cholesterol is linearly related to CHD mortality. 45 Evidence from the research literature indicates that an increasing level of serum cholesterol is an important cause of CHD, and lowering serum cholesterol reduces that risk. 46 The higher the risk, the greater the benefit. A 10% reduction in plasma total cholesterol is followed by a 25% reduction in incidence of CHD after 5 years, and a reduction of low-density lipoprotein (LDL) cholesterol of 1 mmol/L is accompanied by a 20% reduction in CHD events. 47 The relationship between LDL cholesterol and CVD risk is continuous and graded over a broad range of LDL levels from low to high.
Despite there being no data informing us where the optimal levels of plasma cholesterol are, guidelines suggest that total plasma cholesterol should be below 5 mmol/L and LDL cholesterol should be below 3 mmol/L. 24 In high-risk participants, especially those with clinically established atherosclerotic CVD and patients with diabetes, the treatment goals should be lower: total cholesterol, 4.5 mmol/L and LDL cholesterol, 2.5 mmol/L. No specific treatment goals are defined for high-density lipoprotein (HDL) cholesterol and triglycerides, but the concentrations of HDL cholesterol <1.0 mmol/L in men and <1.2 mmol/L in women, and fasting triglycerides >1.7 mmol/L serve as markers of increased CHD risk. 24 In the guidelines, screening of the plasma lipid profile is recommended in adult men who are at least 40 years of age, and in women who are at least 50 years of age or postmenopausal. 24 In screening programs, total cholesterol may be used to estimate risk. In the individual case, however, total plasma cholesterol may be misleading. This is especially the case in women who often have high HDL levels and in participants with diabetes or the metabolic syndrome who often have low HDL levels. 48
There are substantial data supporting the concept that dietary saturated fat is the dietary factor with the strongest impact on LDL cholesterol levels in the general population as well as in hypercholesterolemic individuals. 49 Thus, a diet aiming at decreasing consumption of saturated fat would be beneficial for LDL cholesterol levels.
A number of large-scale clinical trials have demonstrated that the statins substantially reduce cardiovascular-related morbidity and mortality in both primary and secondary prevention studies. Statins have also been shown to slow the progression or even promote regression of coronary atherosclerosis. In a primary prevention study (WOSCOPS), 6595 men with a total cholesterol level >6.5 mmol/L and without previous MI were randomized to receive 40 mg pravastatin or placebo. 50 The average followup period was 4.9 years. Pravastatin lowered plasma cholesterol levels by 20% and LDL cholesterol levels by 26%. Major coronary events were significantly reduced by 31%. AFCAPS/TexCAPS was a randomized, primary prevention trial, which included 6605 men and women with no prior history of cardiovascular disease. 51 Total cholesterol was from 4.65 to 6.82 mmol/L and the participants were randomized to 20 to 40 mg lovastatin or placebo. After an average followup of 5.2 years, lovastatin significantly reduced the incidence of first acute major coronary events by 37%. Lovastatin reduced LDL cholesterol by 25% in this study. Thus, there are data demonstrating a decreased number of CHD events during statin treatment in primary prevention studies.
Diabetes Mellitus
Diabetes mellitus is associated with and increased CHD risk. 52 In participants with impaired glucose tolerance, it has been demonstrated that progression to diabetes can be prevented or delayed by lifestyle intervention. 53
In patients with type 1 diabetes as well as with type 2 diabetes, randomized trials have demonstrated that good metabolic control prevents microvascular complications.54,55 The effect of good metabolic control on macrovascular disease is less clear. However, evidence from epidemiological studies and intervention trials indicates an effect of glucose control on risk of CHD. Thus, a good metabolic control is an aim in both types of diabetes. A multifactorial risk factor intervention is especially important in patients with diabetes mellitus and targets for BP and lipids are more ambitious in patients with diabetes than in nondiabetic participants.
Inflammatory Biomarkers
Patients with inflammatory diseases, including rheumatoid arthritis, psoriasis, and systemic lupus erythematosus (SLE) have an increased CHD risk. 56 There is also strong evidence from numerous studies that circulating markers of activated inflammation such as C reactive protein (CRP) are associated with the risk of CHD. 57 Statin treatment decrease CRP levels and several beneficial effects of statins may be owing to anti-inflammatory activity. In the “JUstification for the use of statins in Prevention: an Intervention Trial Evaluating Rosuvastatin” (JUPITER) study, 17 802 apparently healthy participants with LDL cholesterol below 3.4 mmol/L and high-sensitivity CRP levels of 2.0 mg/L or higher were randomized to 20 mg rosuvastatin or placebo. 58 The median followup was 1.9 years. Rosuvastatin reduced LDL cholesterol levels by 50% and high-sensitivity CRP protein levels by 37%. The combined endpoint (MI, stroke, arterial revascularization, hospitalization for unstable angina, or death from cardiovascular causes) was reduced by 44% in the rosuvastatin group. Thus, an elevated high-sensitivity CRP may indicate an increased CHD risk.
Risk Assessment
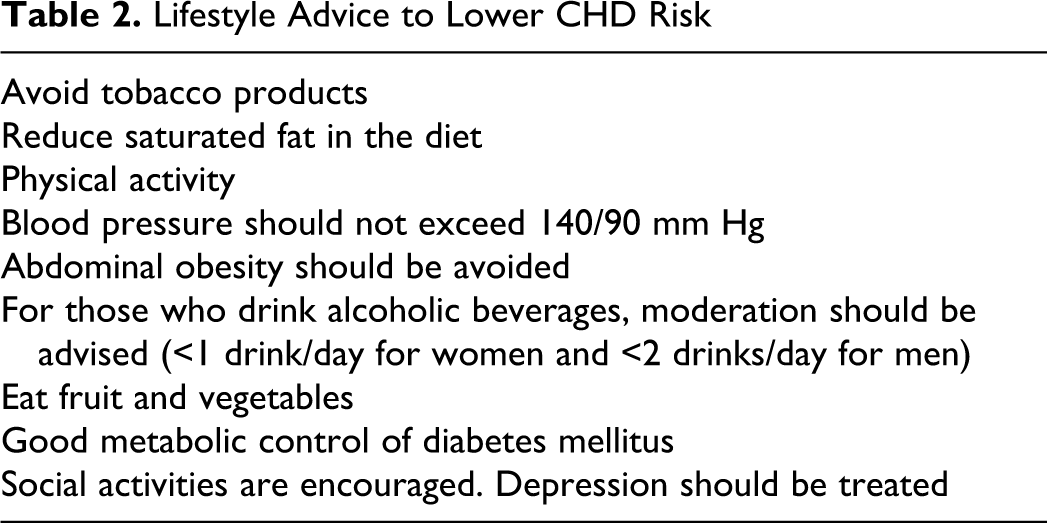
Rather than just treating a cardiovascular risk factor, the total cardiovascular risk should be assessed for the individual participant. The guidelines provide us with risk scores, which may help us to decide the intervention activity. 24 General advice to decrease CHD risk should be provided to the individual (Table 2 ).
Lifestyle Advice to Lower CHD Risk
Conclusions
Effective CHD prevention needs a global strategy based on the knowledge of the importance of risk factors for CVD. Several easily measured and potentially modifiable risk factors account for a substantial proportion of the risk of CHD. Modifiable risk factors are smoking, abnormal lipids, hypertension, diabetes, abdominal obesity, some psychosocial factors, poor diet with low consumption of fruits and vegetables, alcohol consumption, and regular physical activity. The effect of risk factors interventions on these factors appears to be consistent in both genders, across different geographic regions, and by all ethnic groups, suggesting that approaches to prevention can be based on the similar principles worldwide. This may be achieved in several different ways, such as public health education, financial interventions with taxes on unhealthy products, and by law restrictions such a banning smoking in public places. Health-care systems may provide the citizen with guidance toward a healthier lifestyle. The last step is to introduce pharmacological treatment to decrease CHD risk after an individual cardiovascular risk estimation of the subject.
Footnotes
The author(s) declared no conflicts of interest with respect to the authorship and/or publication of this article.
The author(s) received no financial support for the research and/or authorship of this article.