
Abstract
Background
Cardiac rehabilitation programmes are a proven treatment for individuals with recent myocardial infarction, resulting in reduced morbidity and mortality compared to usual care. Unfortunately, following completion of a cardiac rehabilitation programme, risk factors and lifestyle behaviours may deteriorate. The GlObal Secondary Prevention strategiEs to Limit event recurrence after myocardial infarction (GOSPEL) study investigates the benefits of a programme of continued educational and behavioural interventions to achieve optimal long-term secondary prevention goals. Design This will be a multicentre, randomized, controlled study carried out in 78 Italian cardiac rehabilitation centres.
Methods
After completion of an initial cardiac rehabilitation programme, patients with recent (<3 months) myocardial infarction were randomized to either a long-lasting (over 3 years) multifactorial continued educational and behavioural programme (intensive approach) or usual care (control) group. Intensive approach patients participated in extensive cardiac rehabilitation sessions, monthly from months 1 to 6, then every 6 months for 3 years. Each session consisted of aerobic exercise, comprehensive lifestyle and risk factor counselling, and clinical assessment Usual care patients returned to their family physicians’ care, and attended the reference centre only for the 6-month and then annual scheduled assessment. The efficacy of the two different strategies will be evaluated in terms of morbidity and mortality as primary endpoint.
Results
From January 2001 through December 2002, 3241 patients were enrolled. Results will be available in mid 2006.
Conclusions
The GOSPEL trial, the rationale and design of which we present here, was designed to test a new strategy of secondary prevention delivery and to raise standards of long-term secondary prevention in Italy. With a cohort of over 3200 patients, GOSPEL is the largest randomized, multifactorial lifestyle and risk factor intervention trial after myocardial infarction conducted so far.
Keywords
Introduction
Although mortality for acute coronary syndrome has been declining in recent years, coronary heart disease (CHD) still remains the major cause of premature disability and death in most western countries [1], resulting in substantial loss of productivity and contributing to the escalating costs of healthcare, particularly in the presence of an aging population.
Given that current optimal life-saving treatments, including revascularization and widespread use of prophylactic drugs, enable the majority of individuals to survive their first symptomatic presentation of an acute myocardial infarction (MI), the potential to reduce the risk of recurrent events and death is considerable [2]. Cardiac rehabilitation programmes (CRPs) are a proven treatment for individuals with recent MI and, in general, with CHD, resulting in reduced morbidity and mortality compared with usual care. The CRP has gradually evolved from an exercise-based programme into a comprehensive professional lifestyle programme addressing issues such as smoking cessation, diet, and increased exercise based on behavioural models of change; stress management, psychosocial and vocational components are also an integral part of this approach [3,4]. Theoretically, through an integrated approach based on lifestyle and risk factor management combined with prophylactic drug therapies, the risk of a further cardiovascular event should be greatly reduced in CHD patients. Current secondary prevention practice is, however, far from optimal. Studies recently showed that secondary prevention measures are not adequately implemented and consequently there is a large potential for improvement as many CHD patients are not achieving the recommended lifestyle and risk factor goals [5,6]. In addition, current CRPs typically rely on short-term exposure to lifestyle behavioural interventions and risk factor modification to gain long-term benefits in terms of quality of life and reduced morbidity and mortality. Unfortunately, it has been clearly documented that after completion of a CRP, exercise adherence decreases, body weight increases and lipid profile deteriorates over time [5–7, indicating that the intervention in the long-term (phase three) is inadequate. Moreover, at discharge after MI a substantial number of patients are not receiving adequate drug therapy, specifically beta-blockers and statins [5, 6,8]. Effective interventions must take global risk into account and modify all risk factors as recommended by national guidelines. So far, few studies have investigated a multifactorial long-term intervention aimed to improve the current undertreatment and prevention of risk factors that occur following MI [8,9]. In a relatively small group of coronary patients, it was shown that a reinforced action on risk factor control can be successful over a 1-year follow-up period [8]. On the other hand, in the Extensive Lifestyle Management Intervention (ELMI) trial, a 1-year multifactorial post-CRP intervention resulted in modest, non-significant benefits to global risk compared with usual care [9].
Thus, to better address this issue and to raise standards of long-term secondary prevention in Italy the GlObal Secondary Prevention strategiEs to Limit event recurrence after myocardial infarction (GOSPEL) trial was conceived and is currently under way.
GOSPEL
GOSPEL is a multicenter, randomized, controlled study carried out in 78 cardiac rehabilitation centres throughout Italy that agreed to take part in the trial and to adopt the study protocol. The study was approved by the local scientific and ethics committees of the participating centres. Each patient was duly informed of the trial objectives, study design, and risks and benefits of study participation. A signed consent form was collected from all patients.
Objectives
The objectives of the GOSPEL study are as follows: to evaluate the effects of two different strategies of secondary prevention implemented in a rehabilitation setting (long-term, multifactorial continued educational and behavioural intervention versus usual care) on a combined endpoint of several major adverse events: cardiovascular mortality, non fatal re-MI, angina requiring hospitalization, urgent revascularization procedures, hospitalization for heart failure, and non-fatal stroke (primary end-point); to evaluate the applicability (in terms of adherence/compliance) of the two strategies, and the effects on long-term lifestyle changes (exercise capacity, diet composition, smoking status, body mass index, hypertension and metabolic profile); to estimate the ‘cost-effectiveness’ of the two strategies.
Trial organization and procedures
Study population
GOSPEL enrolled patients with recent (< 3 months) MI referred to a cardiac rehabilitation programme, either residential or ambulatory, irrespective of any revascularization procedure (coronary artery bypass graft or percutaneous coronary intervention) received after the index event. Exclusion criteria were age over 75 years, severe concomitant non-cardiac disease such as cancer, renal dysfunction (serum creatinine level over 3 mg/dl), liver dysfunction (alanine aminotransferase/aspartate aminotransferase level > 1.5 times the upper normal limit), dementia, any systemic disease limiting exercise, and inability to participate in a prospective study for any logistic reason.
Study design
All eligible patients completed a CRP before randomization. The standard CRP lasted 3–6 weeks and consisted of supervised exercise sessions, comprehensive lifestyle and risk factor management along with medical therapy optimization. After completion of the initial CRP, patients were randomized in a 1:1 fashion to either a long-lasting (over 3 years) multifactorial continued educational and behavioural programme (intensive approach) or usual care (control) group. Allocation of patients to groups was accomplished via fax, and centrally approved at the study co-ordinating centre using computer-generated randomization. Due to the nature of the study, neither participants nor research personnel could be blinded to their group assignment. Randomization data are kept at the co-ordinating centre.
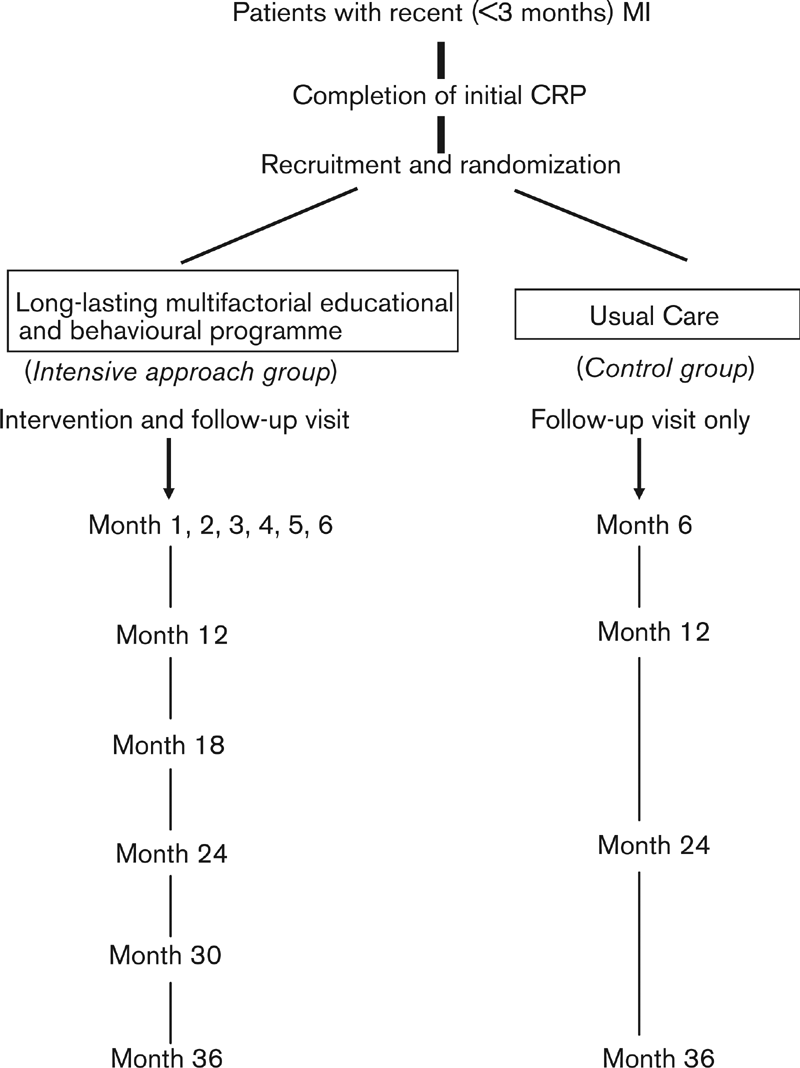
Study timeline. CRP, cardiac rehabilitation programme; MI, myocardial infarction.
After randomization, all patients are required to return to their reference centre for follow-up visits at 6 months, 1 year, 2 years, and 3 years. For patients in the intervention group only, a further detailed schedule for the long-term multifactorial educational programme is provided (see below). Data on vital status and major adverse events will then continue for all patients, and will be stopped in December 2005. The study timeline is reported in Fig. 1.
Long-lasting multifactorial educational and behavioural intervention (intensive approach group)
The multifactorial educational programme is co-ordinated by a specialist cardiac nurse. In each cardiac rehabilitation centre, the core interventional team is made up of a cardiac specialist nurse and a physiotherapist supported by a lead cardiologist. Other specialists may be involved, however, such as a clinical psychologist, dietician or occupational therapist. The lead cardiologist works closely with the team to ensure patients in the intervention group achieve the lifestyle, blood pressure, cholesterol and diabetes target. Moreover, the cardiologist prescribes and uptitrates cardioprotective medications. The team has had several years’ previous experience. In addition, all staff had previously undergone formal training in counselling techniques and the stages of change.
Extensive cardiac rehabilitation sessions are held monthly from month 1 to month 6, then every 6 months for 3 years. Each session consists of 30 min supervised aerobic exercise, comprehensive lifestyle and risk factor counselling, and clinical assessment along with reinforcement on the preventive measures by the lead cardiologist. At the start of the study, each intensive approach group patient received a booklet for exercise, diet, smoking cessation and stress management to aid in lifestyle adherence and to help patients assume a greater role in their healthcare. This booklet summarizes ideal lifestyle and risk factor targets, and is aimed to empower patients to manage each risk factor and lifestyle behaviour. The programme provides both group and one-to-one support.
In all patients, the approach is aimed at individualizing risk factor and lifestyle management based on current treatment guidelines. Strategic steps used to enhance the effectiveness of behavioural counselling (as recommended by the Report of the US Preventive Services Task Force) include ensuring that patients understand the relationship between behaviour, health and disease; gaining commitments from patients to behavioural changes; involving patients in identifying and selecting the risk factors to change; designing a lifestyle modification plan; and monitoring progress through follow-up contact.
Patients and their families require integrated, multi-disciplinary support to achieve appropriate lifestyle changes. Thus, families are encouraged to work together to support each other to sustain the patients over a lifetime. Involving the patient's partner, and other family members sharing the same household, in making and maintaining behavioural change is more likely to be successful than treating the patient in isolation [10].
All treatments proven effective in secondary prevention are positively recommended (specifically aspirin, angiotensin-converting enzyme inhibitors, beta-blockers, statins and n-3 polyunsaturated fatty acids).
The goals agreed for appropriate risk factor and lifestyle behaviour are as follows: giving up smoking; eating a healthy Mediterranean diet (as recommended in the GISSI-Prevenzione trial [11]); physical activity of at least 3 h/week; body mass index below 25 kg/m2; blood pressure below 140/85 mmHg (for those with diabetes below 130/80 mmHg); total cholesterol below 200 mg/dl (5.2 mmol/l); low-density lipoprotein (LDL)-cholesterol below 100 mg/dl (2.6 mmol/l); blood glucose below 110 mg/dl (6.1 mmol/l) and good glycaemic control in all persons with diabetes; and finally ensuring that each of the following classes of cardioprotective medications are prescribed according to guidelines, at the doses used in the clinical trials: antiplatelet therapy; beta-blockers; angiotensin-converting enzyme inhibitors or A-II receptor blockers; statins; n-3 polyunsaturated fatty acids.
Usual care (control group)
For patients in the control group, a letter is sent to the primary care physician recommending secondary prevention goals. There is no attempt by the research cardiologist to aid in lifestyle adherence or in up-titration of cardioprotective medications. Usual care patients come to their reference centre only to undergo the 6-month and then annual scheduled assessment. After each assessment, a copy of the laboratory and exercise testing results is forwarded to their family physicians, responsible for any further decision.
Assessments and procedures
A common core of assessments are performed at baseline and are repeated at each follow-up visit: cardiovascular examination, vital signs, body mass index, 12-lead electrocardiogram (ECG), symptom-limited exercise stress test with continuous 12-lead ECG monitoring, blood chemistry, compliance check, and serious adverse events assessment. An echocardiographic baseline assessment of left ventricular ejection fraction is also performed. Body mass index is calculated from weight in kilograms divided by height in metres squared. A manual sphygmomanometer is used to determine blood pressure (millimetres of mercury), which is recorded as the average of two measures taken 2 min apart after 5 min of supine rest. Laboratory analysis includes fasting total cholesterol, high-density lipoprotein and LDL cholesterol, triglycerides, fasting glucose and HbA1c. Cardiovascular events and healthcare utilization are identified through documentation of medical records.
Questionnaires on smoking habit, leisure-time physical activities, dietary habits, and stress management are also administered at each follow-up visit to all patients by an appropriately trained cardiac specialist nurse who reviews them to ensure that they have been fully completed.
Both at baseline and at 1-year follow-up a psychological evaluation is performed with the Cognitive Behavioural Assessment Hospital (CBAH) form. The CBAH form is a standardized 152-item true/false questionnaire divided into four schedules that explore emotional state, vital exhaustion in the 3 months before evaluation, psychological and behavioural traits potentially related to ischemic heart disease, and behavioural lifestyle [12]. The questionnaire ranges from 0.84 to 0.87 on Cronbach's internal consistency and from 0.42 to 0.63 on retest at 6 months. A checklist of assessments and procedures is depicted in Table 1.
Outcome measures
Major adverse events (primary outcome measure) such as cardiovascular mortality, non-fatal re-MI, angina requiring hospitalization, urgent revascularization procedures, hospitalization for heart failure, and non-fatal stroke are collected at follow-up visits at 6 months, 1 year, 2 years, and 3 years and then yearly until all randomized patients have completed the 3-year study period in December 2005. All events recorded in the study are identified through documentation of medical records on the basis of pre-agreed definitions and procedures. All adverse events are reported to the study co-ordinating centre with the case report form or endpoint documentation. Each report will include narrative summaries with supporting documentation for all events.
Checklist of assessments and procedures

FU, follow-up visit (cardiovascular examination, vital sign, compliance check, lifestyle assessment); AE, serious adverse events and healthcare utilization assessment; EX, exercise stress test; Q, psychosocial questionnaire; B, blood chemistry.
Characteristics of the study population (n = 3421) at randomization
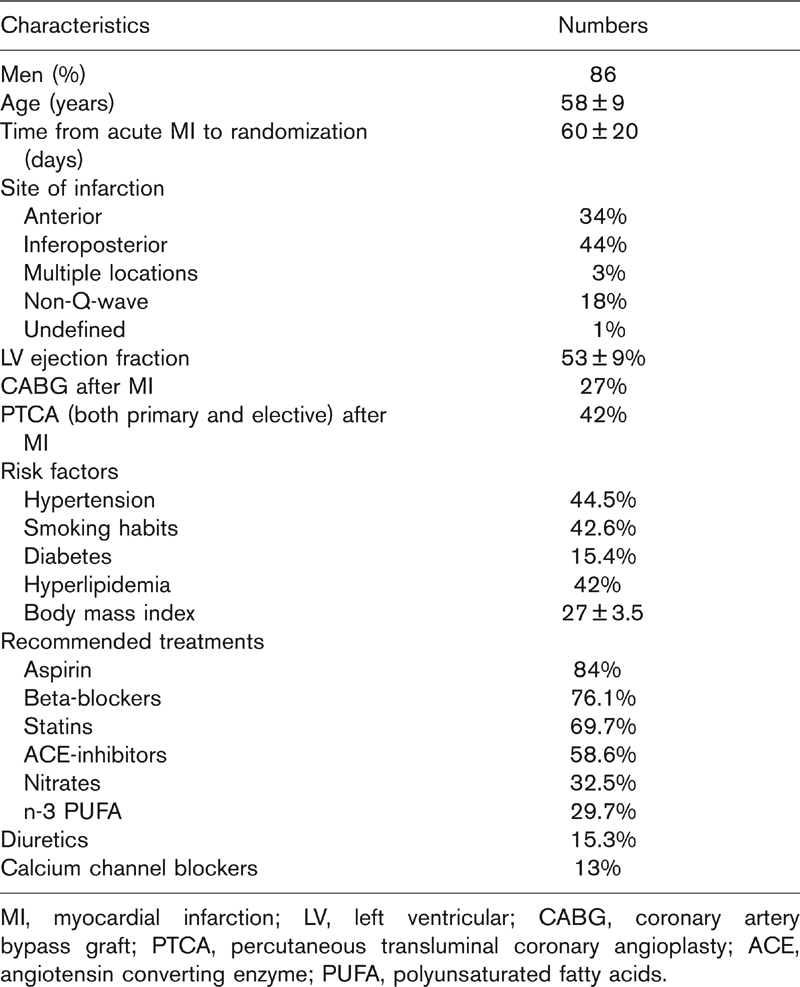
MI, myocardial infarction; LV, left ventricular; CABG, coronary artery bypass graft; PTCA, percutaneous transluminal coronary angioplasty; ACE, angiotensin converting enzyme; PUFA, polyunsaturated fatty acids.
At each scheduled visit, data on healthcare utilization are collected to allow a health-economic analysis of the two strategies. The direct costs of both interventions and any other form of healthcare utilization (pharmacological and non-pharmacological) will be estimated from Italian health system Diagnosis Related Groups (DRG) figures. Through the questionnaires on lifestyle variables, lifestyle adherence and risk factor management will be captured.
Data management
All data peripherally collected in paper case report forms are sent to the co-ordinating centre (Centro Studi ANMCO, Firenze) and electronically stored for further analysis.
Sample size and statistical aspects
The cumulative rate of clinical endpoints (cardiovascular mortality, re-MI, angina requiring hospitalization, new revascularisation, hospitalization for heart failure, and stroke) during 3 years of follow-up is expected to be 30% on the basis of the GISSI-Prevenzione results [13]. Accordingly, to detect a 15% risk reduction by intensive approach versus usual care with 90% power and a two-sided significance at α = 0.05, at least 1600 patients in each group are required.
The main analysis will be performed according to an intention-to-treat approach; therefore all patients randomized in the study will be included in the analysis. Every effort will be made to obtain as much data as possible from each participant.
Baseline characteristics of the intervention and control group will be compared using the Pearson χ2 test for categorical factors and the independent samples Student's t-test for continuous factors. We will analyse data by Kaplan–Meier survival curves and the log-rank test. Treatment efficacy will be assessed by baseline values of the risk-stratification variables fitting various Cox's regression models adjusted for the confounding effect of relevant cardiovascular risk factors.
Data will be reported as means ± standard deviations. All statistical analyses will be performed using the SAS programme (SAS Institute Inc., Cary, North Carolina, USA). The significance level for all tests was set at 0.05 and all t-tests are two-tailed.
Discussion
It has been clearly demonstrated that contemporary secondary prevention, which consists of professional lifestyle intervention on risk factors, psychosocial and vocational support, and appropriate use of prophylactic medications, can substantially reduce morbidity and mortality in patients with CHD [3,7,14–16]. With this evidence, international guidelines have strongly recommended reinforcement of actions to improve secondary prevention [3,4].
Unfortunately, risk factor management in patients with CHD in Europe is sub-optimal. Surveys of clinical practice conducted in single countries as well as the multinational European Action on Secondary and Primary Prevention by Intervention to Reduce Events (EURO-ASPIRE) I and II studies have clearly shown that less than a third of coronary patients attend CRPs [5,6], and that secondary prevention measures are not adequately implemented [5–7. Moreover, contemporary CRPs commonly rely on short-term exposure to lifestyle behaviours and risk factor management to gain long-term benefits in terms of reduced morbidity and mortality, even though it has been demonstrated that early after completion of a CRP behavioural recidivism and risk factor deterioration occur [7,17]. Few studies investigated a long-term, multifactorial, individually-tailored risk factor and lifestyle management intervention aimed at preventing the deterioration of risk factors and lifestyle behaviours following a CRP in CHD [9, 14,18].
The GOSPEL trial was designed to test a new strategy of secondary prevention delivery and to raise standards of long-term secondary prevention that can be easily adapted to clinical rehabilitation settings in Italy. From January 2001 through December 2002, 3241 patients were enrolled. Characteristics at randomization of the study population as a whole are reported in Table 2. Given the widespread adherence of rehabilitation centres throughout the country, the study population depicts a cohort representative of the current CRP Italian population. Moreover, this study clearly sets up a tool for implementing secondary prevention strategies through CRPs.
With a cohort of over 3200 patients and a duration of 3 years, the GOSPEL is the largest randomized, multifactorial lifestyle and risk factor intervention trial after MI conducted so far. Results will be available in mid 2006.