
Abstract
Objective
The value of exercise testing (ET) in asymptomatic subjects remains controversial and is unknown in countries with a low coronary heart disease (CHD) incidence. The aim of this study was to investigate the ability of ET to improve the prediction of a first coronary event in such a population.
Methods
Using a prospective cohort study, 1051 consecutive healthy asymptomatic adults were enrolled in a cardiovascular screening program including ET. The pre-test risk of CHD was evaluated by the 10-year Framingham risk function. Positive ET was defined as a horizontal or downsloping ST-segment depression ≥ 1.0 mm. The primary outcome was total coronary events (CE) occurrence, including cardiac deaths, acute myocardial infarction and stable or unstable angina. The mean follow-up period was 6 years.
Results
Subjects were aged 18-79 years and 36% were women. A total of 89 subjects (8.5%) had a positive ET. Positive exercise testing was associated with CE occurrence in a univariate analysis only in subjects with higher pre-test risk, defined by a 10-year Framingham risk >10.4% [hazards ratio (HR) = 2.61; 95% confidence interval (CI) (1.07-6.40)]. In this risk category, ET was able to provide incremental information over the major risk factors in both men and women [risk factor-adjusted HR for positive ET = 2.86; 95% CI (1.14-7.20)]. This risk excess in subjects with positive ET persisted even when a coronary revascularization was performed. Subjects with intermediate pre-test probability (10-15%) and positive ET had a post-test probability of CE largely equivalent to the probability in subjects with known CHD.
Conclusion
Additional informátion provided by ET in subjects with a pre-test risk at 10-years >10% should lead to a more efficient use of risk-reducing therapies than it would be the case in this risk category with the analysis of traditional risk factors only.
Introduction
Exercise testing (ET) is widely used by clinicians as a diagnostic test in the evaluation of patients with symptoms or history of coronary heart disease (CHD). However, its utility as a screening or prognostic test in asymptomatic subjects remains controversial. Screening with ET in such a population may reduce CHD incidence and mortality in two different ways. The first one, diagnostic-based, aims at detecting subjects with severe and asymptomatic coronary artery lesions, whose prognosis could be improved by revascularization. However, no strong evidence supports the potential benefits of revascularization procedures in asymptomatic subjects and the real accuracy of ET in this setting. The second one is prognosis-based and suggests that ET could help to detect people at high risk of CHD, who could benefit from intensive and aggressive risk factor management. Nowadays, there is no randomized intervention trial data to assess this allegation. Available prognostic information is provided by observational studies, conducted since the 1970s, investigating the relationships between several exercise variables, such as silent ischaemia, exercise capacity or ventricular arrhythmia on the one hand, and occurrence of CHD events or deaths [1–5] on the other hand. International guidelines used these data to not recommend ET in asymptomatic subjects with low risk of CHD [6–8] because of an unacceptably large number of false-positive results and the poor accuracy of ET in asymptomatic subjects without previous risk stratification. Thus, more recent studies [9–12] have investigated the additional information provided by supplementing with ET the recommended risk-factor-based screening [13]. This additional information seems to depend on the pre-test risk [12] and on the primary end-point (total mortality [12] or CHD incidence [11]). However, this has never been assessed in a country with a low incidence of CHD, where a supplementary tool for risk stratification is greatly needed since cardiac events are uncommon and difficult to predict. Our hypothesis is that, in such countries, the assessment of CHD risk factors in clinical practice could be used to select subjects in whom screening should be completed by exercise testing. Thus, this study aimed at determining the ability of exercise testing to improve the prediction of individuals’ risk of developing a first coronary event in a country with a low CHD incidence.
Materials and methods
Subjects
Between September 1995 and September 1999, 1250 consecutive healthy asymptomatic subjects aged 18-79 years, self-referred or referred by primary-care physicians and cardiologists to our preventive cardiology unit for an evaluation of their risk factors and a routine ambulatory cardiovascular screening, were included in a prospective cohort study. Patients who were ineligible for ET and who reported a past history of CHD or suspect cardiovascular symptoms were not included. Subjects were also excluded in case of left ventricular hypertrophy, definite Q-wave or left bundle branch block on standard electro-cardiography at rest, and beta-blocker treatment on the examination day.
Baseline clinical information
On the day of screening, all subjects provided information about their cardiovascular risk factors and lifestyle through a standardized questionnaire, derived from the MONICA population survey [14] carried out in the same region and administered by a single physician. Recorded data included a complete medical history concerning CHD risk factors, past history of cardiovascular disease, possible cardiovascular symptoms, medication, alcohol consumption and socio-professional data. All the subjects underwent physical examination, electrocardiography, a collection of a blood sample and exercise testing. Each subject gave an informed consent and authorization from the appropriate ethics committee was obtained. The mean of two blood pressure measurements taken at rest prior to exercise testing was used for analysis. The risk factors taken into account were: age (≥ 45 years old for men, ≥ 55 years old for women), current cigarette smoking, hypertension (systolic blood pressure ≥140 mmHg or diastolic blood pressure ≥ 90 mmHg or documented use of antihypertensive drugs), diabetes mellitus (fasting glucose level ≥126 mg/dl or documented use of anti-diabetic drugs), hypercholesterolaemia [low-density lipoprotein (LDL)-cholesterol ≥4.14 mmol/l or documented use of lipid-lowering drugs], low high-density lipoprotein (HDL) cholesterol level (< 1.03 mmol/l for men, < 1.29 for women), family history of premature CHD (CHD before 55 years in father or brother/65 years in mother or sister) and overweight (body mass index ≥ 25 kg/m2). Four levels of leisure time physical activity were defined: no regular physical activity, light physical activity (i.e., less than once a week), moderate physical activity (i.e., 20 min at least, once or twice a week) and high physical activity (i.e., 20 min at least, three times a week or more). Although our sample was drawn from a country with a low incidence of CHD, baseline absolute cardiovascular risk was assessed using a 10-year Framingham risk function [15] and was used to define subjects with ‘pre-test’ risk of CHD. We did not use the SCORE project's formula [16] since it was designed to predict fatal cardiovascular events, whose numbers were too small in our study. Concerning the PROCAM European function [17], its applicability to men only in a selected age range (40-65 years) has limited its use.
Since a past history of CHD was an exclusion criterion, each subject's self-reported history was completed by a systematic confirmation including the review of all the medical records available in our hospital database, the interview of the patient's regular physician and consultation of the local CHD registry (belonging to MONICA-WHO project). Due to this thorough investigation, 21 initially eligible subjects were excluded because of no self-reported history of coronary artery disease. Moreover, 16 subjects were excluded because of left ventricular hypertrophy on ECG, five because of definite Q-wave, two because of left bundle branch block and 17 because of beta-blocker treatment on the examination day. Overall, 61 subjects out of the 1250 initially enrolled were excluded.
Exercise testing
All participants underwent a symptom-limited exercise testing. The ECG was continuously monitored during the exercise and continued for 6 min during the recovery period, using orthogonal and V1 to V6 leads. Heart rate and blood pressure were recorded every 3 min during the exercise and the recovery period and at peak exercise. The exercise test was stopped when the participant was unable or refused to continue or/and in case of: ventricular conduction or rhythm disorders, decrease in systolic blood pressure ≥ 30 mmHg, systolic blood pressure ≥240 mmHg or diastolic ≥120 mmHg, electrocardiographic ischaemia or angina. Positive ET was defined as a horizontal or downsloping ST-segment depression ≥ 1.0mm at 80 ms after the J-point, in at least two contiguous leads, occurring at any time of exercise or recovery period. Exercise electrocardiograms were read by two independent trained coders. A maximal exercise testing was defined as a peak heart rate ≥ 85% of the maximal predicted heart rate for a given age.
Follow-up and end-points
Morbidity and mortality data were obtained by mailed questionnaires or by telephone calls to patients and to their regular physicians. The survey was conducted in 2003. Incident cases of cardiovascular death, acute myocardial infarction (AMI) and stable or unstable angina during the survey period were collected, as well as hospitalizations for chest pain, coronary angiography and revascularization procedures. Each reported case and causes of deaths were coded by a medical committee after the review of the medical records (medical history, ECG, cardiac enzymes + / - myocardial scintigraphy or/and coronary angiography reports) and the physicians’ interviews, according to the PRIME study definitions [18]. Acute myocardial infarction was defined as one of the two sets of conditions: (1) new Q-wave or other new typical aspects of electrical necrosis; (2) symptoms (typical or atypical) and new (or increased) ischaemia at ECG and enzymes >twice the upper limit of normal. Angina was defined as the presence of anginal pain and: positive angiography (> 50%) or positive scintiscan (if no angiography) or rest ECG changes (if no angiography or scintiscan). Unstable angina was coded when crescendo pain (change in frequency or severity of chest pain on exertion) or rest pain with resting ECG changes. Stable angina was coded when pain on exertion only was present (not at rest and not crescendo). Coronary death was defined by death with documented CHD event. Sudden death was defined as death occurring within 1 h following the onset of symptoms without explanation [18]. Only the first event was taken into account for survival analyses.
The primary end-point of this study was the incidence of ‘total coronary events’ (CE) during a mean of 6 years of follow-up (1–101 months). The CE included cardiac deaths, sudden deaths, AMI and stable or unstable angina. During the survey period, 138 subjects (11% of eligible subjects) were lost to follow-up. Thus, survival analysis included 1051 subjects.
Statistical analysis
Analysis of variance and X 2 tests were used for comparisons between groups. A two-sided P value of less than 5% was considered statistically significant. Univariate association between positive ET and the risk of CE was analysed using Kaplan-Meier survival curves and the log-rank test. Multivariate analysis was performed using risk factor-adjusted, forced Cox proportional hazards model. Proportional hazards assumptions were checked by plotting of ln[−ln(S(t))] versus ln(t). Possible interactions among variables introduced in the model were checked. The incremental value of positive ET over the pre-test score was tested by calculating the likelihood ratio statistic between two models: one with risk factors only and the other with risk factors and exercise testing results. Subjects were stratified according to the presence of silent ischaemia and their pre-test risk, defined by 10-year Framingham risk of CE [15]. Cut-off used for stratification in lower or higher pre-test risk category was the median (10.4%) of Framingham risk for our sample. In order to evaluate the clinical effects of positive ET on the risk of CHD occurrence within the next 10 years, we developed a simple equation allowing the calculation, for a given subject, of the post-test probability of developing CHD, according to the results of ET. This probability depends on the pre-test probability of CHD, clinically defined by Framingham risk score on the one hand and on the likelihood ratios for positive or negative ET on the other hand ([post-test probability = post-test odds/(1 + post-test odds)] and [post-test odds = pre-test odds ∗ likelihood ratio], with [pre-test odds = pre-test probability/(1 - pre-test probability)]). The likelihood ratio for positive ET is (sensitivity/[1 - specificity]) and the likelihood ratio for negative ET is ([1 - sensitivity]/specificity). As we used censored data for this calculation, sensitivity and specificity of positive ET were defined as cumulative sensitivity and specificity for 10 years of follow-up and calculated as functions of time [19]. Data were analysed using the STATA 7.0 statistical software (Stata Corporation, College Station, Texas, USA).
Results
Baseline characteristics and exercise testing results
Subjects were aged 18-79 years. More than one-third of the sample was women. Among the 1051 included subjects, 89 (8.5%) had a positive ET. Nine subjects complained of chest pain and/or dyspnoea, of whom five had a positive exercise testing. Table 1 gives baseline characteristics of subjects with positive or negative ET. There was no significant difference in major risk factors (except for age) between subjects with positive or negative ET.
Outcomes
During a mean (SD) follow-up of 6 (1.1) years, there were 18 (2.9/1000 person-years) deaths from all causes.
Baseline characteristics
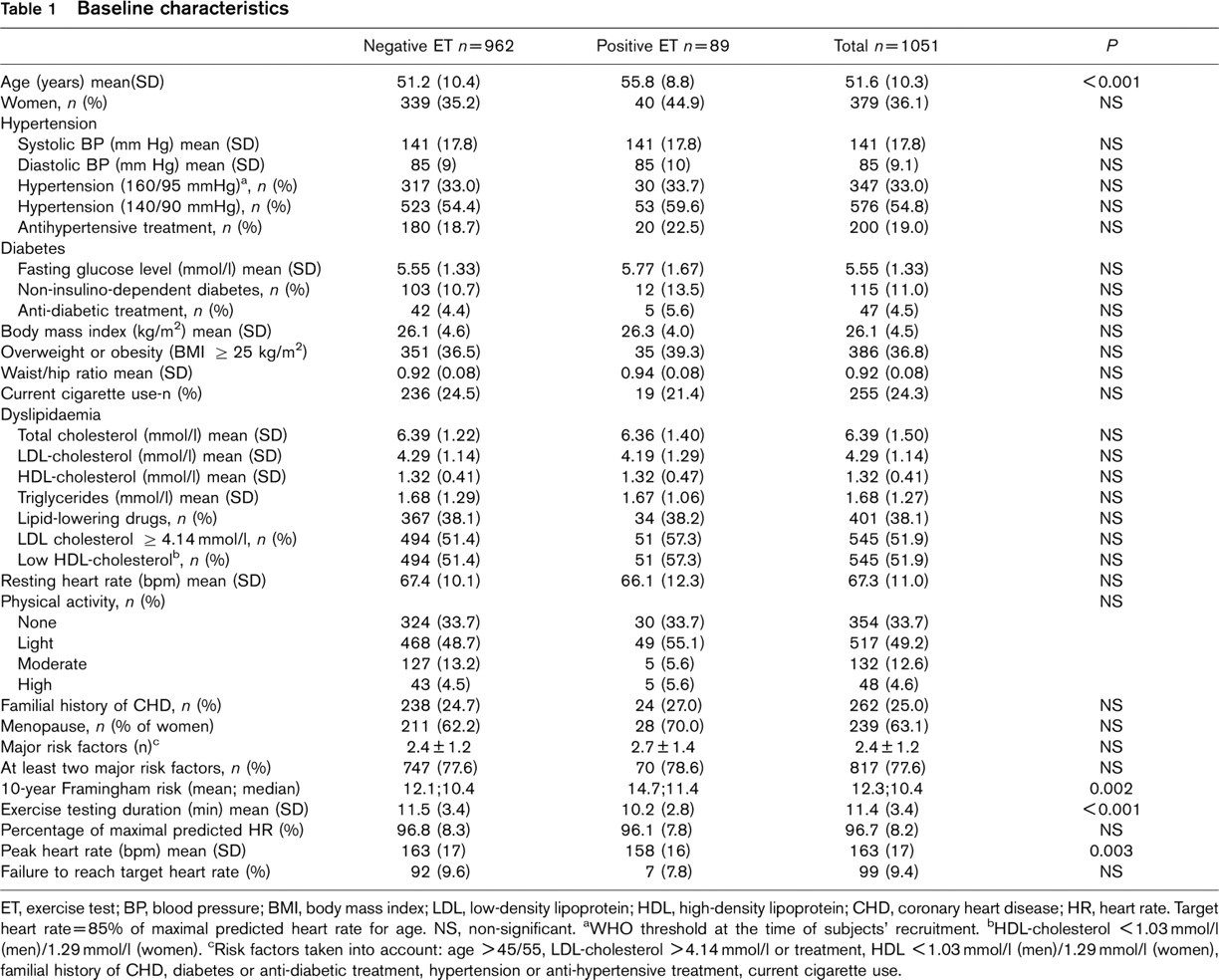
ET, exercise test; BP, blood pressure; BMI, body mass index; LDL, low-density lipoprotein; HDL, high-density lipoprotein; CHD, coronary heart disease; HR, heart rate. Target heart rate = 85% of maximal predicted heart rate for age. NS, non-significant. aWHO threshold at the time of subjects’ recruitment. bHDL-cholesterol < 1.03 mmol/l (men)/1.29 mmol/l (women). cRisk factors taken into account: age >45/55, LDL-cholesterol >4.14 mmol/l or treatment, HDL ≤1.03 mmol/l (men)/1.29 mmol/l (women), familial history of CHD, diabetes or anti-diabetic treatment, hypertension or anti-hypertensive treatment, current cigarette use.
A cardiac cause of death was identified in six subjects. Thirteen subjects (2.1/1000 person-years) had stable or unstable angina during the follow-up. Non-fatal myocardial infarction occurred in 15 patients (2.4/1000 person-years). Overall, CE incidence was 5.5/1000 person-years.
Exercise testing and risk of total CE without prior risk stratification
In a univariate analysis including all the subjects without previous stratification on pre-test risk, the relative risk of CE in men and women with positive ET was 2.34 [95% confidence interval (CI), 0.97–5.64] (Table 2). Relative risks were significant for the occurrence of stable or unstable angina [hazards ratio (HR) = 4.73 (95% CI, 1.26–15.80)] but not for cardiac deaths or non-fatal AMI [HR = 1.62 (95% CI, 0.44–6.18)]. Milder silent ischaemia (ST-depression between 0.5 and 1 mm) was not associated with an increased risk of total CE. After adjustment for age, sex, diabetes, current smoking, systolic blood pressure and LDL-cholesterol, the multi-variate relative risk for CE was 2.27 (95% CI, 0.87–5.59) for patients with positive ET.
Exercise testing and risk of total CE with previous risk stratification
The survival curves after a first stratification according to the Framingham pre-test risk and a second one, on the results of ET, and corresponding hazard ratios are given in Figure 1 and Table 3. Of the 34 CE, only four occurred in the lower pre-test risk group, defined by a Framingham 10-year risk < 10.4%. Furthermore, none of these four events occurred among subjects with positive ET. Hence, a positive ET had no significant influence on the risk of CE in subjects with lower pre-test risk and all subjects with a low pre-test risk were gathered in Figure 1. Conversely, a positive ET was associated with a consistently increased risk in subjects with higher pre-test risk. As shown in Table 2, an incremental value of positive ET over the pre-test risk was found in a multivariate analysis only in subjects with higher pre-test risks, since the likelihood ratio test was significant only in this risk category. This is confirmed by Figure 2, which shows a consistent increase between pre-test and post-test probability when subjects with higher risk had a positive ET, while there was only a slight decrease in case of a negative test.
Relative risks of coronary events according to pre-test risk categories and exercise testing data
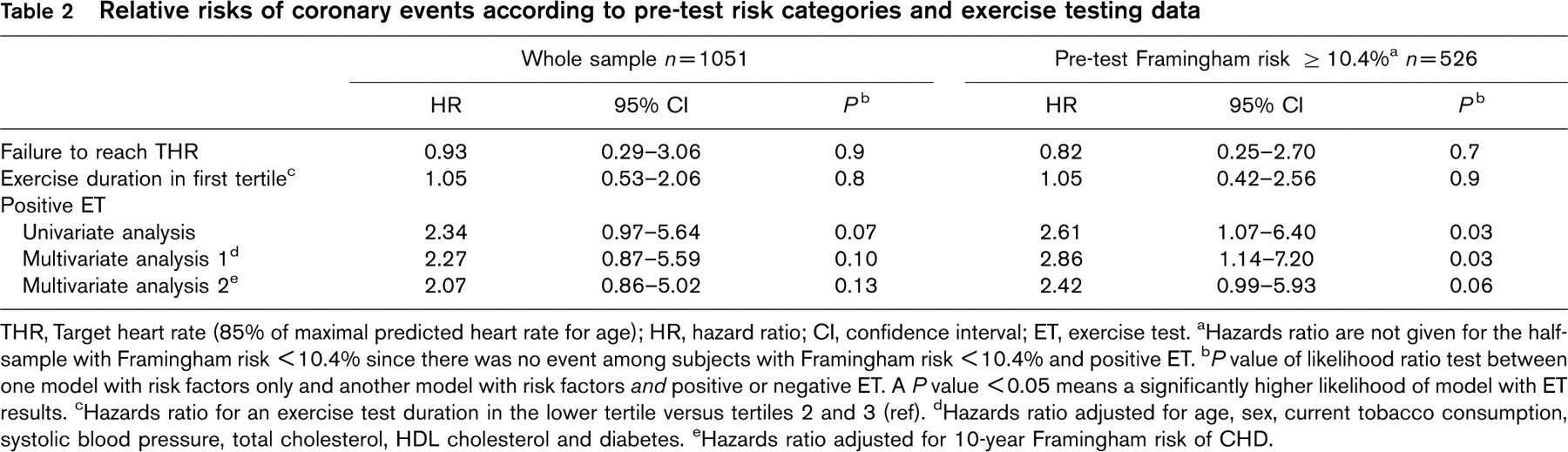
THR, Target heart rate (85% of maximal predicted heart rate for age); HR, hazard ratio; CI, confidence interval; ET, exercise test. aHazards ratio are not given for the half-sample with Framingham risk < 10.4% since there was no event among subjects with Framingham risk < 10.4% and positive ET. b P value of likelihood ratio test between one model with risk factors only and another model with risk factors and positive or negative ET. A P value < 0.05 means a significantly higher likelihood of model with ET results. cHazards ratio for an exercise test duration in the lower tertile versus tertiles 2 and 3 (ref). dHazards ratio adjusted for age, sex, current tobacco consumption, systolic blood pressure, total cholesterol, HDL cholesterol and diabetes. eHazards ratio adjusted for 10-year Framingham risk of CHD.
Hazards ratio (HR) of coronary event in four groups resulting from risk stratification on pre-test risk and results of exercise testing

ET, exercise testing; CI, confidence interval. aNo event in the “positive ET” group. bAll subjects with low risk were gathered in Model 2 (reference group).
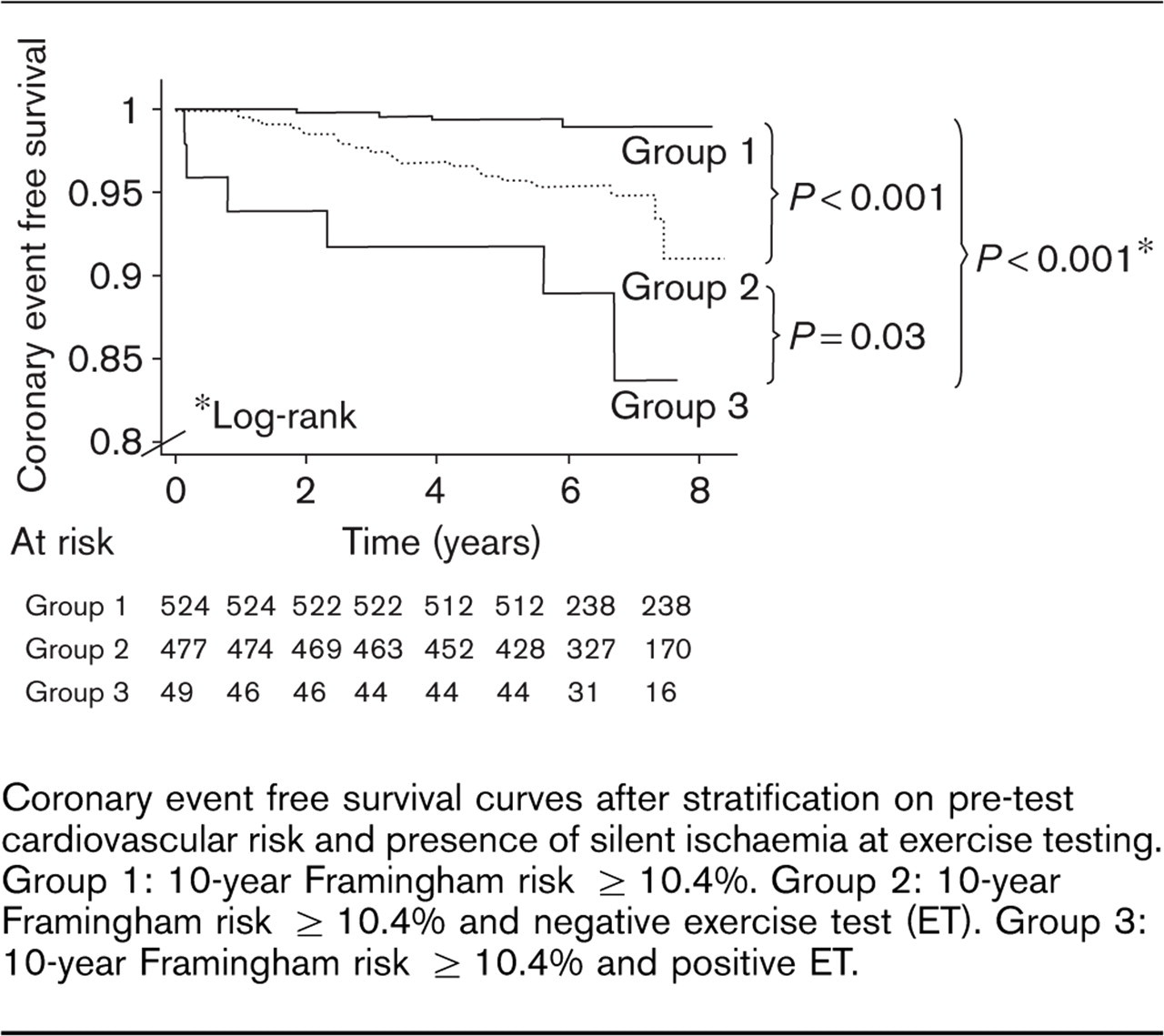
Coronary event free survival curves after stratification on pre-test cardiovascular risk and presence of silent ischaemia at exercise testing. Group 1: 10-year Framingham risk ≥ 10.4%. Group 2: 10-year Framingham risk ≥ 10.4% and negative exercise test (ET). Group 3: 10-year Framingham risk ≥ 10.4% and positive ET.
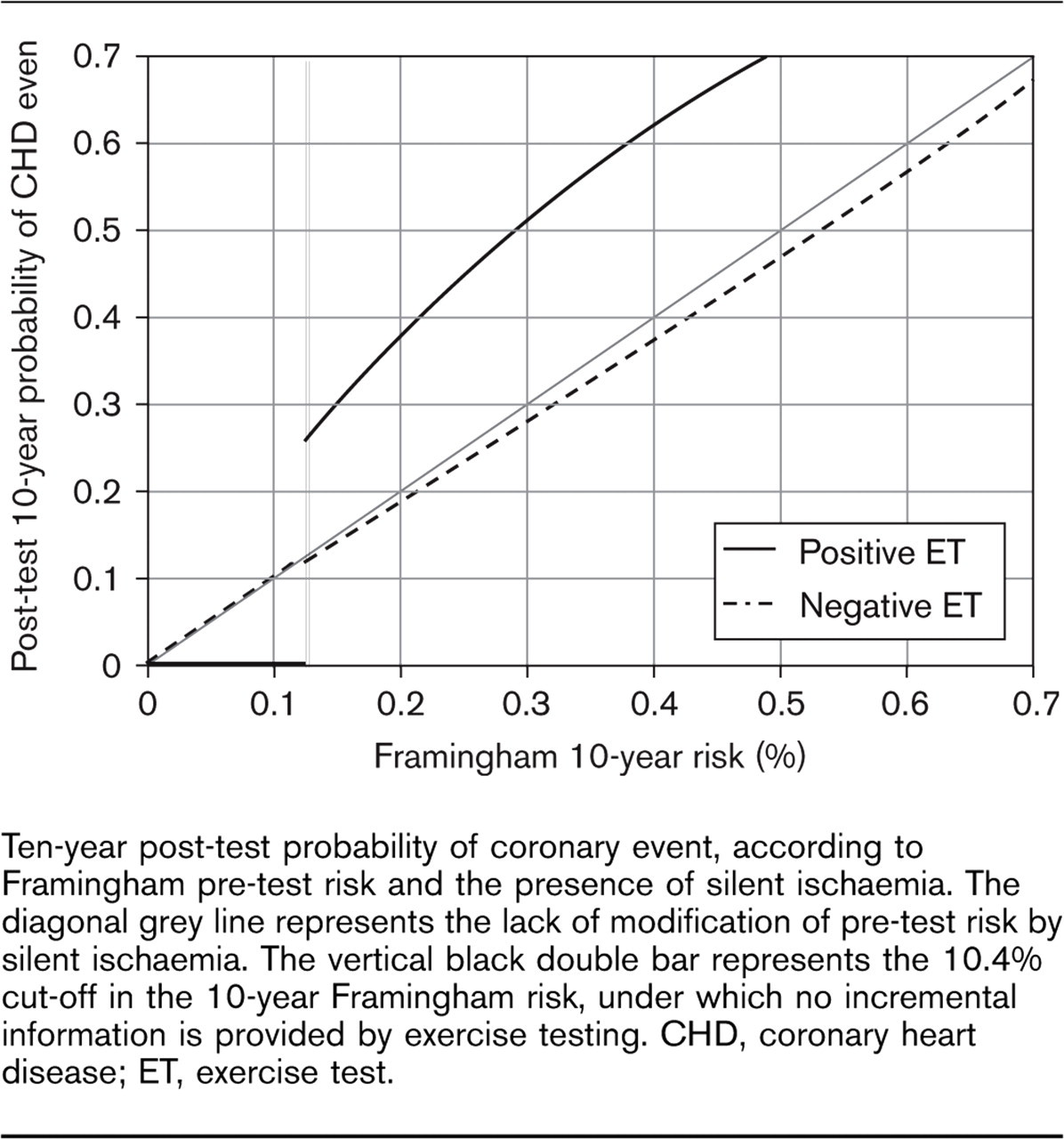
Ten-year post-test probability of coronary event, according to Framingham pre-test risk and the presence of silent ischaemia. The diagonal grey line represents the lack of modification of pre-test risk by silent ischaemia. The vertical black double bar represents the 10.4% cut-off in the 10-year Framingham risk, under which no incremental information is provided by exercise testing. CHD, coronary heart disease; ET, exercise test.
Revascularization procedures and risk of total CE
Coronary angiography was performed in 18 patients within 1 month after their exercise test and five of them underwent a subsequent revascularization procedure. Our sample can be subdivided into three groups. In group (a), ET was positive and further exploration by coronary angiography was performed within 1 month after exercise test (1.8% of the whole sample). In group (b), ET was positive but no further exploration by coronary angiography was decided (6.7% of the whole sample). In group (c), ET was negative (91.5% of the whole sample). Incidence of revascularization procedures performed at any time during the follow-up period was 27.8% in group (a), 5.1% in group (b) and 2.1% in group (c). Concerning the main outcome, incidence of CE during the follow-up was 32.3/1000 person-years in group (a), 8.3/1000 person-years in group (b) and 4.9/1000 person-years in group (c), with HR of 6.59 (95% CI, 2.22–23) and 1.69 (95% CI, 0.27–4.84) for comparison of groups (a) and (b) respectively with group (c) (reference).
Discussion
In this prospective cohort of men and women from a country with a low incidence of CHD [20], we found that positive ET had an incremental value in the risk stratification process only in subjects with the highest pre-test risk (Framingham 10-year risk ≥ 10.4%). Most of the previous studies were conducted in countries with a high incidence of CHD, namely, USA, and found a strong relationship between silent ischaemia and CE [1–3,21], death from cardiac causes [10,22] or death from any other cause [9]. We compared the 138 subjects lost to follow-up to the 1051 included in the survival analysis. Subjects lost to follow-up were younger (46.6 years old in lost to follow-up versus 51.6 years old in eligible subjects; P< 0.001) but there was no further difference concerning either conventional risk factors or the 10-year Framingham risk. Hence, subjects lost to follow-up could account for a decrease in the statistical power of the study, but did not bias the relationship between exercise testing and prognosis.
In the present study, 21 subjects were excluded because of a personal history of CHD, prior to inclusion, and discovered by the systematic review of the patient's medical records or the consultation of the CHD registry [23]. Five of these subjects (24%) had a positive ET and 11 (52%) presented a CE during the follow-up. Thus, the inclusion of these patients in our sample would have meant a strong increase in the relative risk for positive ET and a higher statistical significance of the results (i.e., the crude relative risk of CHD in subjects with positive ET would have been 4.56 (95% CI, 2.38–8.75) P≤0.001, instead of 2.34 (95% CI, 0.97–5.64) P = 0.07 in the present analysis). Usually, available studies have not been able to exclude such patients, actually managed in secondary prevention, because subjects’ medical history was self-reported, without systematic confirmation of their status. This could also have led to a less significant association between positive ET and total CE in our study.
The use of stable angina and cardiac deaths as end-points in such studies have been criticized [24] but our study does not seem concerned by this controversy since all cardiac events and causes of deaths were determined using standardized criteria after the review of all the useful medical data, as in several previous studies [21,25,26]. As in the MRFIT study [25], we found a higher predictive value of exercise testing for angina occurrence than for AMI [univariate HR=4.73 (95% CI, 1.66–12.94) for angina and HR=1.62 (95% CI, 0.34–6.18) for non-fatal AMI].
The incidence of CE was surprisingly low in our study, given the high prevalence of major risk factors. This high frequency of risk factors reflects the clinical characteristics of patients seen for cardiovascular screening in everyday practice. In our study, the prevalence of dyslipidaemia, hypertension and diabetes was higher than the prevalence observed in the general population in countries with a very high incidence of CHD, such as Scotland (Glasgow) [27]. However, CE incidence was lower in our sample than in such countries, confirming the relatively low CHD incidence in these asymptomatic subjects despite their high risk and justifying the supplementation of risk-factor-based decision making with an additional tool.
A stratification on Framingham risk was necessary in the higher risk group (≥ 10.4%) since only four events occurred in the group with lower risk (1.25/1000 person-years). This striking issue shows that the prediction of CHD risk, taking into account risk factors only, is clinically relevant for individuals in the lowest pre-test risk category. This result is confirmed by the lack of incremental value of silent ischaemia and the higher rate of false-positive results in this sub-group. On the opposite, the number of misclassification is higher in subjects with the highest risk and the use of exercise testing enabled an improved prognostic determination in this risk category, through a consistent modification in post-test probability of CE, mostly when ET was positive. Indeed, for a subject with an intermediate pre-test probability of 12%, the post-test probability of total CE is 25%, largely equivalent to the probability in a subject with known CHD [7]. The predictivity of positive ET according to the prevalence of conventional risk factors has already been studied in men by Gibbons et al. [28]. Unlike this study, we found that conventional risk factors had a more powerful influence on cardiac risk than positive ET, thus showing that risk assessment should begin with a systematic evaluation of major risk factors, as recommended.
The pre-test risk cut-off chosen for stratification was the median of the sample's 10-year Framingham risk (10.4%). This threshold is also recommended by the Cholesterol Education Program Adult Treatment Panel III [7] to define the intermediate risk category for persons with multiple risk factors. Furthermore, a 10-year projected risk between 6–20% has been used to isolate individuals with intermediate risk, for whom further risk stratification with use of non-invasive procedures could be beneficial [29]. A recently published study [11], conducted in the Framingham cohort where CHD incidence is higher than in France, found the greatest additional prognostic information in subjects with a 10-year Framingham risk of ≥ 20%.
It is an acknowledged fact that Framingham risk functions overestimate cardiovascular risk when applied to European countries [30]. In agreement with these results, the mean ratio between events predicted by the Framingham function and observed events across quintiles of risk was 2.5 in our study. Nonetheless, this does not affect our principal message, since our aim when using a cardiovascular risk function, was not to calculate individuals’ absolute risk but to identify the subgroups of subjects with higher and lower pre-test risk.
Since our study was not a randomized trial, one of its main limitations is the potentially confounding role of non-controlled intervention on the prognosis. Indeed, it could be argued that subjects with silent ischaemia at exercise testing may have a probability of CE occurrence decreased due to an intervention related to their positive test, such as surgical or interventional revascularization procedures. This important potential bias has rarely been investigated in previous studies and could be responsible for an underestimation of the association between silent ischaemia and CE incidence in our study. Asymptomatic subjects who underwent coronary angiography justified by positive ET within 1 month after exercise training had a higher incidence of CE than those with positive ET without coronary angiography or those with negative ET. It only suggests that asymptomatic subjects who underwent a coronary angiography as a consequence of the results of exercise testing had a more severe disease, and then allows ruling out the bias mentioned above. Data on primary prevention drugs prescribed to subjects with positive ET were not available in our study and might also have accounted for an underestimation of the relative risk for positive ET. The most concerned therapeutic classes are beta-blockers and anti-platelet agents but maybe also other primary prevention drugs such as statins, by way of a better observance [31]. However, we think that such treatments have seldom been prescribed without an angiographically documented CHD.
Conclusion
In conclusion, our results showed an association between positive ET and prognosis among men but also women with high pre-test risk in a country with a low CHD incidence and suggest that risk stratification should start by a systematic evaluation of cardiovascular risk factors. In addition, exercise testing might be a useful tool to improve risk stratification and provides significant additional prognostic information in subjects with higher CHD risk, defined by a 10-year Framingham risk ≥ 10%. It provides no further prognostic information in individuals with lower conventional risk, which makes stratification beyond classical risk factors useless. Moreover, revascularization procedures do not seem to be able to unbalance the risk excess represented by positive ET. In subjects with higher risk, a positive ET makes the probability of CHD occurrence as high as in patients with already known CHD. This additional information should have implications in current practice in such asymptomatic patients, and lead to a more efficient use of risk-reducing therapies than would be the case with the analysis of traditional risk factors only. However, the benefit of intensive drug therapy and revascularization procedures in these ‘high risk’ patients remains unknown and needs further investigations, particularly controlled randomized trials.
Footnotes
Acknowledgements
We thank all the physicians who participated in the preventive cardiology unit since 1995 and our patients’ practitioners, who agreed to collaborate to this study. This study was supported by a grant from the Programme Hospitalier de Recherche Clinique (PHRC 2001), CHU de Toulouse, France.