
Abstract
Several relatively uncommon, but important cardiovascular diseases are associated with increased risk for acute cardiac events during exercise (including sudden death), such as hypertrophic cardiomyopathy (HCM), dilated cardiomyopathy (DCM), arrhythmogenic right ventricular cardiomyopathy (ARVC) and myo-pericarditis. Practising cardiologists are frequently asked to advise on exercise programmes and sport participation in young individuals with these cardiovascular diseases. Indeed, many asymptomatic (or mildly symptomatic) patients with cardiomyopathies aspire to a physically active lifestyle to take advantage of the many documented benefits of exercise. While recommendations dictating the participation in competitive sport for athletes with cardiomyopathies and myo-pericarditis have recently been published as a consensus document of the European Society of Cardiology, no European guidelines have addressed the possible participation of patients with cardiomyopathies in recreational and amateur sport activities. The present document is intended to offer a comprehensive overview to practising cardiologists and sport physicians of the recommendations governing safe participation in different types of competitive sport, as well as the participation in a variety of recreational physical activities and amateur sports in individuals with cardiomyopathies and myo-pericarditis. These recommendations, based largely on the experience and insights of the expert panel appointed by the European Society of Cardiology, include the most up-to-date information concerning regular exercise and sports activity in patients with cardiomyopathies and myo-pericarditis.
Keywords
Introduction
Participation in regular exercise and sport by individuals with known cardiovascular (CV) disease conveys a number of clinical and ethical questions, including the most appropriate exercise programme and sport activities in which patients may safely be engaged. In fact, identification of a cardiovascular disease, or incidence of a cardiac event, is usually associated with prudent advice for patients to reduce (or leave) intensive training and competitive sport, justified by clinical concern for the increased cardiac risk associated with exercise and sport [1, 2]. Therefore, physicians often face the paradox to advise patients against regular exercise and sport, which are unanimously regarded as therapeutic procedures for several CV diseases and advocated as a determinant for reducing the impact of CV risk factors.
To resolve this controversial issue, which has relevant practical implications in a large proportion of cardiac patients, the Sports Cardiology Section of the European Association of Cardiovascular Prevention and Rehabilitation prompted publication of the present recommendations, with the aim of providing careful guidelines to physicians and consultant cardiologists concerning the evaluation and appropriate recommendations for safe exercise training and sports participation in patients with CV disease. The present document focuses on a group of uncommon but important diseases associated with increased risk for acute cardiac events, such as hypertrophic cardiomyopathy (HCM), dilated cardiomyopathy (DCM), arrhythmogenic right ventricular dysplasia/cardiomyopathy (ARVD/C) and myo-pericarditis, and follows those previously published for patients with systemic hypertension and ischaemic heart disease. The present recommendations are based on published scientific evidence, when available, and on personal experience and consensus of experts. However, in consideration of the scarcity of scientific investigations concerning the effect of regular exercise training and sports activities on the pathophysiology and clinical course of cardiomyopathies, the panel acknowledges the difficulties inherent in formulating arbitrary recommendations, and caution in applying the present document is needed and efforts should be made to tailor precise advice to each individual.
Hypertrophic cardiomyopathy
Hypertrophic cardiomyopathy (HCM) is a genetically transmitted cardiac disease, caused by a variety of mutant genes encoding protein components of the cardiac sarcomere [3, 4]. At present, 12 mutant genes and over 400 specific mutations in these genes have been implicated in the pathogenesis of clinically diagnosed HCM. Prevalence of the disease is 0.2% in the general population, as assessed by echocardiographic recognition of hypertrophied and non-dilated left ventricle (LV).
Sports participation increases the risk for arrhythmic sudden death in HCM individuals [2–4], and this disease represents the most frequent cause of all the athletic field deaths in the USA [2].
Evaluation
The clinical evaluation of individuals with suspected HCM includes personal and family history, physical examination, 12-lead electrocardiogram (ECG) and echocardiography.
12-Lead ECG
The majority (75–95%) of HCM patients show abnormal ECGs, including markedly increased R or S wave voltages, deep and prolonged Q waves, deeply inverted T waves, loss of the septal Q waves or left axis deviation [5]. ECG abnormalities usually precede the development of LV hypertrophy and, therefore, abnormal ECGs should raise suspicion in family members of HCM patients.
Echocardiography
Classically, HCM is diagnosed when LV wall thickness is ≥ 13 mm, but a substantial LV wall thickening (> 30 mm) may be found. All patterns of LV hypertrophy are possible, but the anterior ventricular septum is usually the most thickened region, with a sharp transition to contiguous segments [3, 4]. LV hypertrophy becomes evident during adolescence, in association with body growth [3, 6], but in a few individuals may not be evident until midlife or beyond [7]. The LV cavity is of normal or even reduced dimension, with an abnormal and sometimes bizarre shape. Abnormalities of diastolic LV filling (by Doppler-echocardiography) and tissue Doppler imaging (TDI) are present in the majority of HCM patients and may precede the recognition of LV hypertrophy [8]. Other alterations include malformation of the mitral valve, with elongation of the leaflets, or anomalous insertion of papillary muscles [3, 4].
In athletes with physiological cardiac remodelling and LV hypertrophy, the distribution of LV wall thickening is substantially symmetrical and maximum thickness does not exceed 15–16 mm [9]. The LV cavity is enlarged (i.e. end-diastolic diameter ≥ 55 mm) with a normal shape, the mitral valve is normally positioned and there is no evidence of outflow obstruction [9]. Indeed, LV filling (as assessed by Doppler) and relaxation (by TDI) are normal [8]. Most important, serial echocardiographic studies demonstrate a reduction in wall thickness after complete deconditioning [10]. The clinical criteria currently used to distinguish HCM from physiological LV hypertrophy are shown in Table 1.
Criteria for the differential diagnosis of left ventricular (LV) hypertrophy in hypertrophic cardiomyopathy (HCM) and ‘athlete's heart’
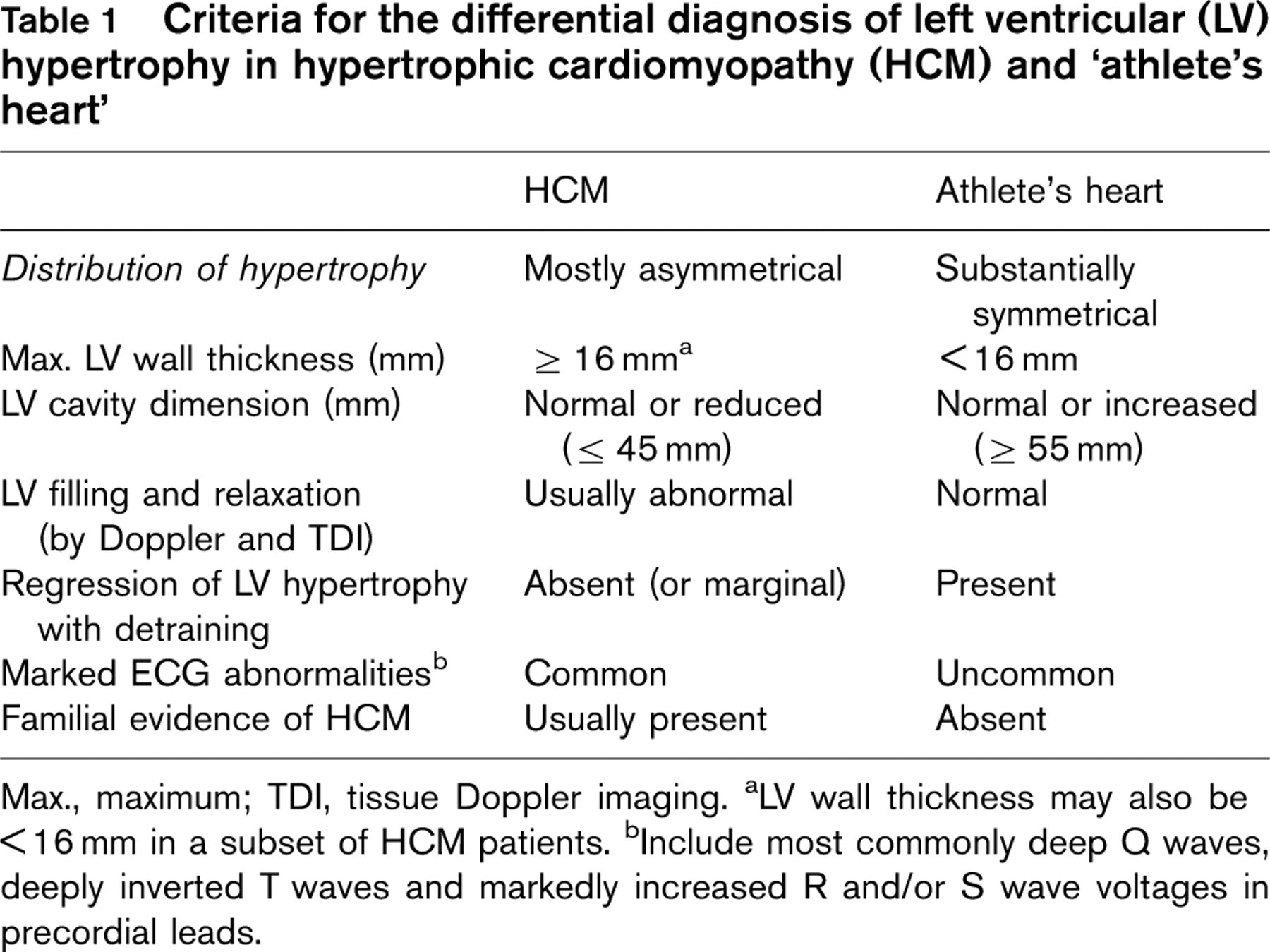
Max., maximum; TDI, tissue Doppler imaging.
aLV wall thickness may also be < 16 mm in a subset of HCM patients.
bInclude most commonly deep Q waves, deeply inverted T waves and markedly increased R and/or S wave voltages in precordial leads.
Additional criteria
Additional criteria include peak oxygen consumption (by cardiopulmonary test), with a peak oxygen consumption (i.e. Vo2max) > 50 ml/kg per min more consistent with athlete's heart [11] (together with detailed knowledge of the training regimen, and exclusion of use of anabolic steroids [12]). Gender is also important, because in women athletes, LV wall thickness does not usually exceed normal values (i.e. 12 mm) [13]. Family screening is mandatory in borderline cases, and identification of the disease in a family member is diagnostic for HCM.
Cardiac magnetic resonance
This is becoming the best imaging technique in assessing the extent and distribution of hypertrophy and is capable of identifying an atypical pattern (such as hypertrophy of the lateral free wall or apex), but requires specific expertise and involves high costs.
Molecular genetics
A variety of mutations of genes encoding structural and regulatory proteins of the cardiac sarcomere cause familial HCM [14–16]. Commercial DNA-based laboratory testing is now available for HCM (website: http://www.hpcgg.org/LMM/tests.html), with the most common genes causing disease (i.e. MYH7, MYBPC3, TNNT2, TNNI3, TMPI) routinely tested. Genetic analysis has the potential to provide a definitive diagnosis should any one of the most common mutant genes be identified; however, important limitations remain, i.e. the substantial genetic heterogeneity of the disease with the potential of false-negative results, and the complex, time-consuming and expensive techniques needed which, so far, limit routine implementation of genetic testing in clinical practice.
Once diagnosis of HCM is established in the single individual, screening of close relatives is required and, if the disease-causing mutation has been identified in an affected family member, molecular genetic testing of asymptomatic at-risk family members may be advisable.
Genetic carriers of HCM
As family genetic screening for HCM will largely be implemented in clinical practice, physicians will face the dilemma of making recommendations regarding sports participation for subjects who have only preclinical evidence of HCM (i.e. genotype positive–phenotype negative).
The clinical significance and natural history of genotype positive–phenotype negative individuals is at present undefined, and no data are available to assess the risk in the single individual. Nonetheless, it is likely that a substantial proportion of such individuals may ultimately develop LV hypertrophy. Moreover, the LV hypertrophy may be evident over the course of several years [3, 6, 7] after initial evaluation, when sports participation could still be an ongoing and important lifestyle issue. Therefore, should the phenotype in HCM convert morphologically from normal to hypertrophied LV, it is possible for the risk level to increase substantially in some patients [3]. Based on these considerations, the evaluation of athletes with preclinical HCM (genotype positive–phenotype negative) includes 12-lead ECG, in addition to serial two-dimensional echocardiography. Cardiac magnetic resonance (CMR) imaging is indicated to reliably assess the presence of LV hypertrophy, which is often not adequately visualized by echocardiography.
Based on the level of present knowledge, the decision for participation in competitive sport should be individualized. However, prudent recommendation suggests restriction of these individuals from participation in competitive sports, especially those with high cardiac demand (i.e. high dynamic, high static sports, see Table 6), and to recommend prudently amateur and leisure-time sport activities.
A systematic follow-up of these individuals is recommended, and close evaluation is needed if there is a family history of sudden cardiac death [3, 4, 14]. Relevant to these considerations are the prior observations that abnormalities on 12-lead ECG [17] and preload-independent measures of diastolic dysfunction with TDI [18] may precede the appearance of LV hypertrophy, providing clues to impeding development of disease phenotype.
Isolated abnormal ECGs
Special attention should be paid to asymptomatic athletes with isolated ECG abnormalities (such as markedly increased QRS voltage, diffuse T wave inversion, deep Q waves in precordial leads) suggestive of HCM, in the absence of morphological cardiac abnormalities and familial incidence of the disease. Evaluation of these athletes should include complete family and personal history, 12-lead ECG, echocardiography and Holter ECG monitoring. In the absence of clinical evidence of cardiac disease (specifically, HCM), these athletes should not be restricted from participation in competitive sport. However, serial clinical and cardiac imaging controls are required to exclude ensuing evidence of cardiovascular disease. As genetic screening for HCM becomes routine clinical practice, these individuals will become natural candidates for DNA analysis of HCM genes, and recommendations about competitive sport will be adapted consequently.
Recommendation for competitive sport participation in athletes with cardiomyopathies, myocarditis and pericarditis
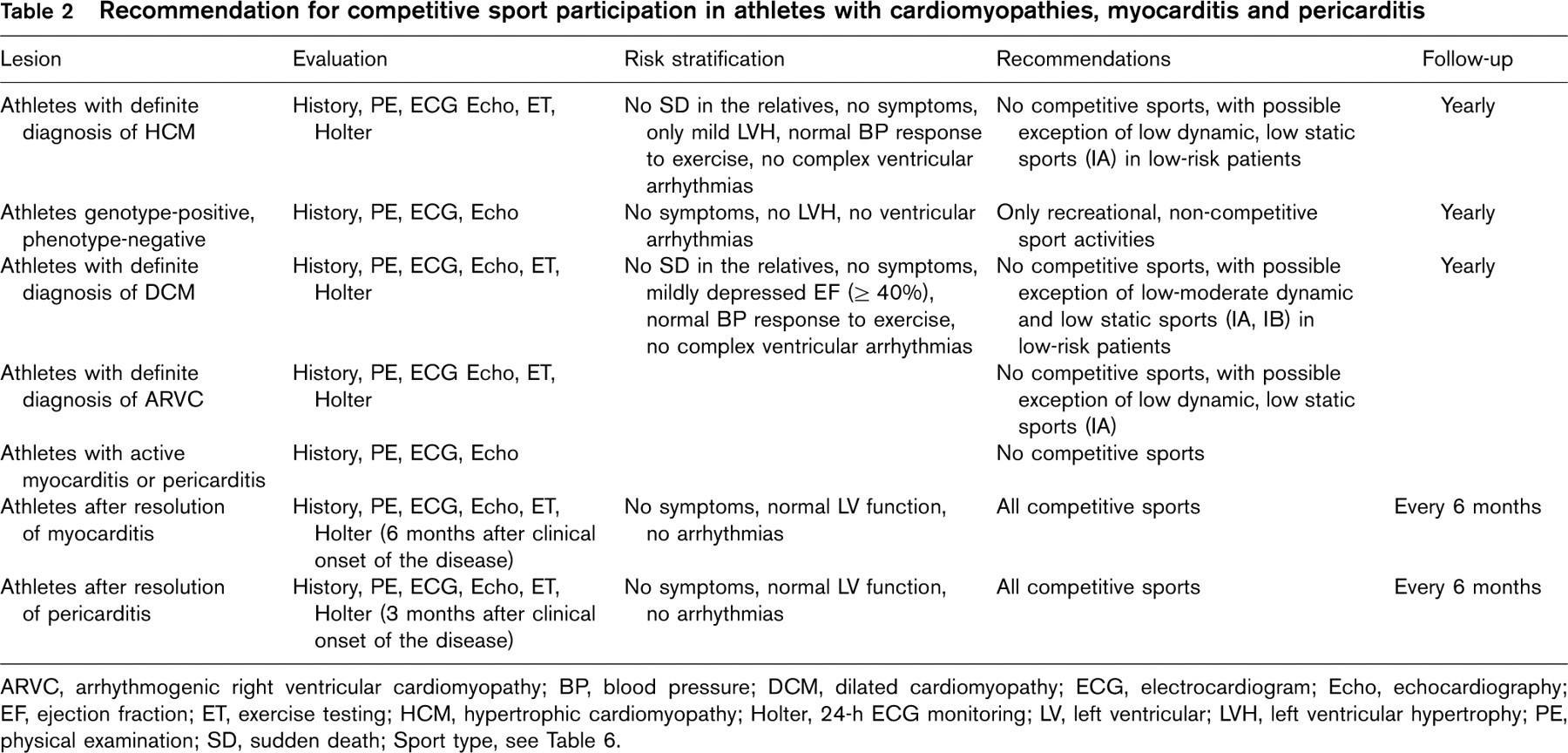
ARVC, arrhythmogenic right ventricular cardiomyopathy; BP, blood pressure; DCM, dilated cardiomyopathy; ECG, electrocardiogram; Echo, echocardiography; EF, ejection fraction; ET, exercise testing; HCM, hypertrophic cardiomyopathy; Holter, 24-h ECG monitoring; LV, left ventricular; LVH, left ventricular hypertrophy; PE, physical examination; SD, sudden death; Sport type, see Table 6.
Recommendations for participation in competitive sports (Table 2)
Athletes with a diagnosis of HCM should be excluded from most competitive sports, with the only possible exception being those of low intensity (class IA, see Table 6) in individual cases as a result of expert cardiovascular evaluation. This recommendation is independent of age, gender and phenotypic appearance, and does not differ for those athletes without symptoms, LV outflow obstruction, or prior treatment with drugs or major interventions with surgery, alcohol septal ablation, pacemaker or implantable defibrillator (ICD).
Special considerations
The placement of an ICD in an HCM patient does not change the recommendations for this disease (as previously noted), namely, that restriction from participation in contact and non-contact sports is advisable; such individuals may eventually engage only in low-intensity competitive sports (class IA, see Table 6).
The presence of a free-standing automated external defibrillator (AED) at sporting events should not be considered either absolute protection against sudden death, or treatment strategy for known cardiovascular disease, nor a justification for participation in competitive sports in athletes with previously diagnosed HCM.
Dilated cardiomyopathy
Dilated cardiomyopathy (DCM) is a myocardial disease characterized by LV dilatation and impaired systolic function. DCM includes disorders that are familial or genetic in origin, or secondary to infection or inflammation, exposure to toxic substances, metabolic disorders or idiopathic [19, 20]. Familial dilated cardiomyopathy has been recognized in a growing proportion of patients, and is currently believed to represent 30–50% of cases [19]. DCM most commonly exhibits familial transmission consistent with autosomal dominant inheritance (approximately 90%) and, to a lesser extent, X-linked (5–10%) and autosomal recessive (AR) or mitochondrial inheritance. Mutations in more than 15 genes (all autosomal dominant except one autosomal recessive and two X-linked genes) have been suggested to be causative [19].
Although not frequently, DCM represents a cause of arrhythmic sudden death in young/adult individuals engaged in sport activities.
Evaluation
The clinical evaluation of athletes with suspected DCM includes personal and family history, physical examination, 12-lead ECG, echocardiography and Holter monitoring.
12-Lead ECG and Holter monitoring
In DCM, arrhythmias may be present in the very early stage of the disease, including supraventricular and ventricular tachyarrhythmias, as well as A-V blocks and major conduction delays [i.e. left bundle branch block (LBBB)].
Echocardiography
The LV cavity is often disproportionately enlarged with respect to LV walls, which are normal or mildly thickened. LV shape becomes more spherical; the mitral annulus enlarges with resultant distortion of leaflets and valvular regurgitation [20]. The systolic function is diminished (with ejection fraction < 50%), segmental wall motion abnormalities are present, stroke volume is reduced and end-diastolic chamber pressure increased.
Cardiopulmonary testing may be useful to assess the impairment in physical capacity and occurrence of exercise-induced supraventricular/ventricular arrhythmias [21].
Differentiation from physiological LV enlargement present in a large proportion of trained athletes, mostly engaged in aerobic disciplines (such as cycling, crosscountry skiing, rowing, long-distance running) [22] is based on the recognition of normal LV systolic function, absence of segmental wall motion abnormalities, and normal LV diastolic filling (by Doppler) and TDI pattern. Indeed, LV cavity dilation in normal athletes is associated with superior physical performance, as assessed by cardiopulmonary test. The criteria that may be clinically useful for differential diagnosis between DCM and physiologic LV remodelling of the ‘athlete's heart’ are reported in Table 3.
In selected cases, LV cavity dilation in athletes is associated with only mildly reduced ejection fraction (i.e. ejection ≥ 50, < 60%); in these instances it may be useful to assess LV function during exercise (by echocardiography or radionuclide imaging), which induces a significant increase in the ejection fraction (> 60%) in athletes. Absence of significant improvement at peak exercise is, on the contrary, in favour of pathological LV dilatation.
Molecular genetics
Although a commercial genetic test is already available for the selected genes implicated in the genesis of familial DCM [19] (such as the gene encoding lamin A/C), implementation of a genetic test for clinical diagnosis is currently hampered by locus and allelic heterogeneity of the disease, and the significant proportion of cases that are not attributable to any of the known genes. Larger series of patients will be required to understand gene penetrance, genotype–phenotype correlations, and the true incidence and prevalence of familial DCM, which will greatly improve genetic counselling.
Criteria for the differential diagnosis of dilated cardio-myopathy (DCM) from athlete's heart
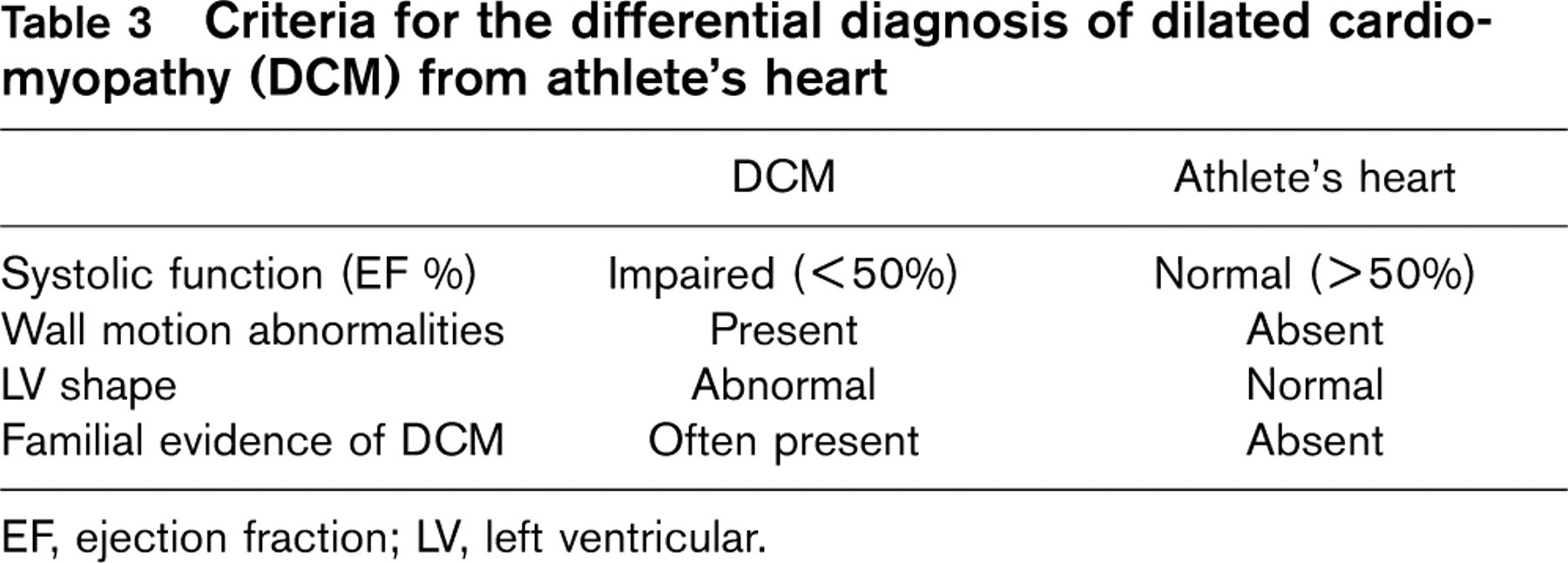
EF, ejection fraction; LV, left ventricular.
Once diagnosis of DCM is established in the single individual, screening of close relatives for familial DCM is required and, if the disease-causing mutation has been identified in an affected family member, molecular genetic testing of asymptomatic at-risk family members may be advisable.
Recommendations for participation in competitive sports (Table 2)
Athletes with a clinical diagnosis of DCM should be excluded from most competitive sports, with the possible exception of those of low intensity (types IA, IB, see Table 6). This recommendation is independent of age, gender and phenotypic appearance, and does not differ for those athletes without symptoms, or prior treatment with drugs or major interventions with surgery, or an implantable defibrillator. (2) The presence of a freestanding AED at sporting events should not be considered either absolute protection against sudden death, or a treatment strategy for DCM, nor a justification for participation in competitive sports in athletes with previously diagnosed DCM.
Exercise in extremely adverse environmental conditions, including a very hot, humid or cold weather.
Exercise programmes (even if recreational in nature) that require systematic and progressive levels of exertion and are focused on achieving higher levels of conditioning and excellence (particularly in sports such as in road running, cycling and rowing).
Intense static (isometric) exertion, such as lifting free weights.
Patients with diseases associated with impaired consciousness (e.g. syncope and near-syncope) are subject to considerably higher risk for traumatic injury while engaged in sports such as diving, rock climbing, free weight and bench-pressing manoeuvres, motorcycling.
Individuals with an implanted ICD should avoid contact sports (see Table 6), due to risk of traumatic injury or inappropriate discharge. However, presence of implanted ICDs does not represent, per se, restriction from amateur, leisure-time physical activity after individual assessment.
Arrhythmogenic right ventricular dysplasia/cardiomyopathy
Arrhythmogenic right ventricular dysplasia/cardiomyopathy (ARVD/C) is a primary myocardial disease characterized histologically by fibro-fatty replacement of the right ventricular (RV) myocardium, and clinically by life-threatening ventricular tachyarrhythmias in young individuals [23, 24]. Advances in molecular genetics have provided new insights in understanding the pathophysiology of ARVD/C, showing that it is a desmosomal disease resulting from defective cell adhesion proteins such as plakoglobin, desmoplakin, plakophilin-2 and desmoglein-2 [25]. It has been hypothesized that the incorporation of mutant protein into cardiac desmosomes may cause detachment of myocytes at the intercalated discs, under condition of mechanical stress (like that occurring during competitive sports activity). As a consequence, there is progressive myocyte death with subsequent repair by fibro-fatty replacement. However, ARVD/C has been linked to other genes unrelated to the cell adhesion complex, such as the gene encoding cardiac ryanodine receptor (RyR2), which is responsible for calcium release from the sarcoplasmic reticulum, and the transforming growth factor ?3-gene (TGF?3) which regulates the production of extracellular matrix components and modulates expression of genes encoding desmosomal proteins. Six additional genes associated with autosomal dominant ARVD/C have been mapped but not identified, and additional loci remain undetermined.
Sudden, unexpected death may occur in young ARVD/C individuals in association with exercise and sports participation, and this disease represents the most common cause of sudden death in young athletes in Italy [23].
Evaluation
Clinical diagnosis of ARVD/C is based on the criteria previously proposed by an expert consensus panel [24]. The ARVD/C phenotype is widely variable and some affected individuals may not meet the strict criteria; however, they may still be at risk for cardiovascular events [25, 26]. According to the task force, the diagnosis of ARVD/C is established in individuals who have two major criteria, or one major and two minor criteria, or four minor criteria [24]. Timely identification of ARVC is, however, challenging in asymptomatic individuals, and largely relies on familial occurrence of the disease, presence of ECG abnormalities, or morphological RV abnormalities detectable with imaging techniques. Incidence of ventricular tachyarrhythmia (such as ventricular tachycardia of right ventricular origin, usually elicited by exercise) represents a substantial contribution to the clinical diagnosis of ARVD/C.
12-Lead ECG and Holter monitoring
The 12-lead ECG can be of particular value in raising suspicion for ARVD/C, considering that ECG abnormalities may be present in > 50% of patients and precede the clinical onset of the disease. Inverted T waves in the right precordial leads (V2 and V3) in individuals older than age 12 years (in the absence of a right bundle branch block), incomplete right bundle branch block and epsilon wave (electrical potentials at the end of the QRS complex) are the most common ECG changes [27, 28].
Premature ventricular ectopic beats and ventricular tachyarrhythmia (sustained, or non-sustained) have LBBB morphology and are often associated with exercise [27, 28].
Certain ECG changes observed in young ARVD/C patients may also mimic those found in the athlete's ECG, and should be differentiated (Table 4).
Echocardiography and cardiac magnetic resonance
In ARVD/C patients dilation of the right ventricle with reduction of RV function with no (or only mild) LV impairment is the diagnostic hallmark of the disease. However, in the early stages of the disease only localized RV morphological abnormalities are present, such as aneurysms, dilatation or thinning of the RV free wall. Trabecular disarray has also been reported in these patients [27, 28]. Echocardiographic assessment of RV morphology is difficult in several cases, due to inadequate acoustic windows and the localized extent of the morphological anomalies. Detection of regional RV wall motion abnormalities in these instances is of diagnostic value.
Criteria for the differential diagnosis of arrhythmogenic right ventricular cardiomyopathy (ARVC) from athlete's heart
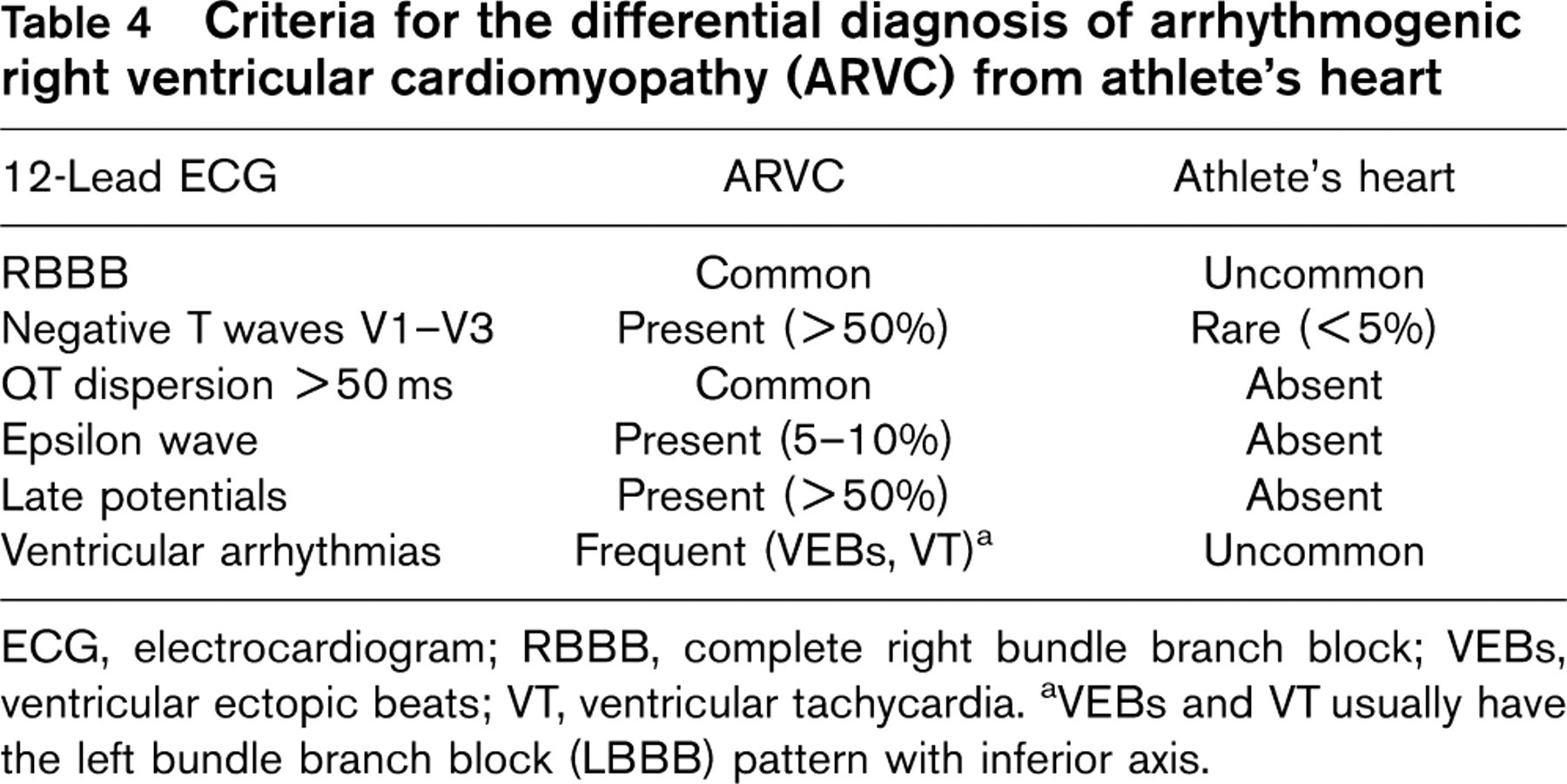
ECG, electrocardiogram; RBBB, complete right bundle branch block; VEBs, ventricular ectopic beats; VT, ventricular tachycardia.
aVEBs and VT usually have the left bundle branch block (LBBB) pattern with inferior axis.
The evaluation of morphological RV abnormalities is better performed by CMR [29]. Indeed, CMR is able to identify areas of altered signal intensity consistent with fibro-fatty replacement of the RV free wall.
Endurance athletes may show enlarged RV cavity, in association with enlarged LV cavity, as a consequence of cardiac remodelling due to intensive training, but several criteria may help in the differentiation, including presence in athletes of a normal RV wall thickness, without segmental RV wall thinning or aneurysm, with normal global RV function and the absence segmental wall motion abnormalities.
Molecular genetics
At the moment, the defective PKP2 gene appears to be a major cause of ARVD/C, with a prevalence of mutations among unrelated index cases as high as 43%. Therefore, molecular genetic diagnosis of ARVD/C is going to be feasible in a significant proportion of patients by screening for mutations in the PKP2 gene and more broadly in desmosomal protein genes [25].
Once diagnosis of ARVD/C is established in the single individual, clinical screening of close relatives is required and, if the disease-causing mutation has been identified in an affected family member, molecular genetic testing of asymptomatic family members may be advisable. Genetic testing is currently available, however, in only a limited number of laboratories.
Recommendations for participation in competitive sports (Table 2)
Athletes with clinical diagnosis of ARVD/C should be excluded from most competitive sports, with the possible exception of those of low intensity (class IA, see Table 6), proven absence of arrhythmias (even with treatment or ICD) and no incidence of exercise-related symptoms. This recommendation is also independent of age, gender and phenotypic appearance and does not differ for those athletes without symptoms, or treated with drugs, or surgical interventions, catheter ablation or implantable defibrillator.
The presence of a free-standing AED at sporting events should not be considered either absolute protection against sudden death, or treatment strategy, nor a justification for participation in competitive sports in athletes with previously diagnosed ARVD/C.
Recommendations for amateur and leisure-time sport activities in patients with cardiomyopathies
The clinician is frequently confronted with the dilemma of designing non-competitive exercise programmes for individuals with HCM or other cardiomyopathies after disqualification from competitive sport, as well as for those patients with such conditions who do not aspire to organized sports participation, but aspire to a physically active lifestyle to take advantage of the many documented benefits of exercise and who wish to participate in recreational and leisure-time activities. At present, however, the risk of habitual non-competitive physical activity in young patients and adults with such genetically transmitted cardiac disease is undefined [30].
For the purpose of this document, recreational sports activities are defined in juxtaposition to competitive sports and refer to a wide range of physical activities, from modest to vigorous on either a regular or inconsistent basis, not requiring systematic training or pursuit of excellence, nor involving the same pressure to excel against others which is characteristic of competitive sports.
Finally, it is not the objective of this panel to restrict all physical activity that could conceivably be associated with some risk in patients with cardiomyopathies, but to develop a reasonable balance between the risk and the benefits. Given the relative paucity of scientific evidence in this area, therefore, it is likely that a certain degree of risk will be associated with participation in amateur and leisure-time sport activities. However, this panel believes that potential risk of exercise should not exclude a large proportion of patients with HCM (and other genetic cardiac disease) and create a completely sedentary population deprived of the many benefits afforded by exercise for cardiovascular health.
The implementation of exercise recommendations ultimately depends on the interaction between physician and patient. It may often be necessary for clinicians to individualize exercise prescription for particular patients, balancing the clinical status with the physical activity under consideration. The clinician should teach participants in recreational physical activities (particularly in individual sports) to take reasonable control over their level of exertion, by assessing heart rate (devices assessing heart rate are commercially available and efficient) and being aware of impending cardiac symptoms. Patient education is, therefore, important. Finally, clinical decisions regarding the structure of exercise programmes are also influenced by other issues, including legal responsibility of the physician, the possibility that recommendations may be (deliberately) ignored by some patients, and the variable tolerance for exposure to cardiac risk among patients and their families [30].
This panel expresses specific recommendations in terms of a graded scale (i.e. activities generally not advised or strongly discouraged, activities which should be advised on an individual basis and activities generally permitted). Therefore, these recommendations are necessarily subjective and represent only a starting point for clinical judgement in individual asymptomatic (or very mildly symptomatic) patients with cardiomyopathies (Table 5).
In addition, it is important to express specific recommendations about exercise that should be avoided by patients with clinically diagnosed cardiomyopathies.
Explosive exertion, characterized by short time, high-intensity exercise, such as sprinting short distances with rapid acceleration and deceleration.
Recommendation for amateur and leisure-time sport activities in individuals with cardiomyopathies
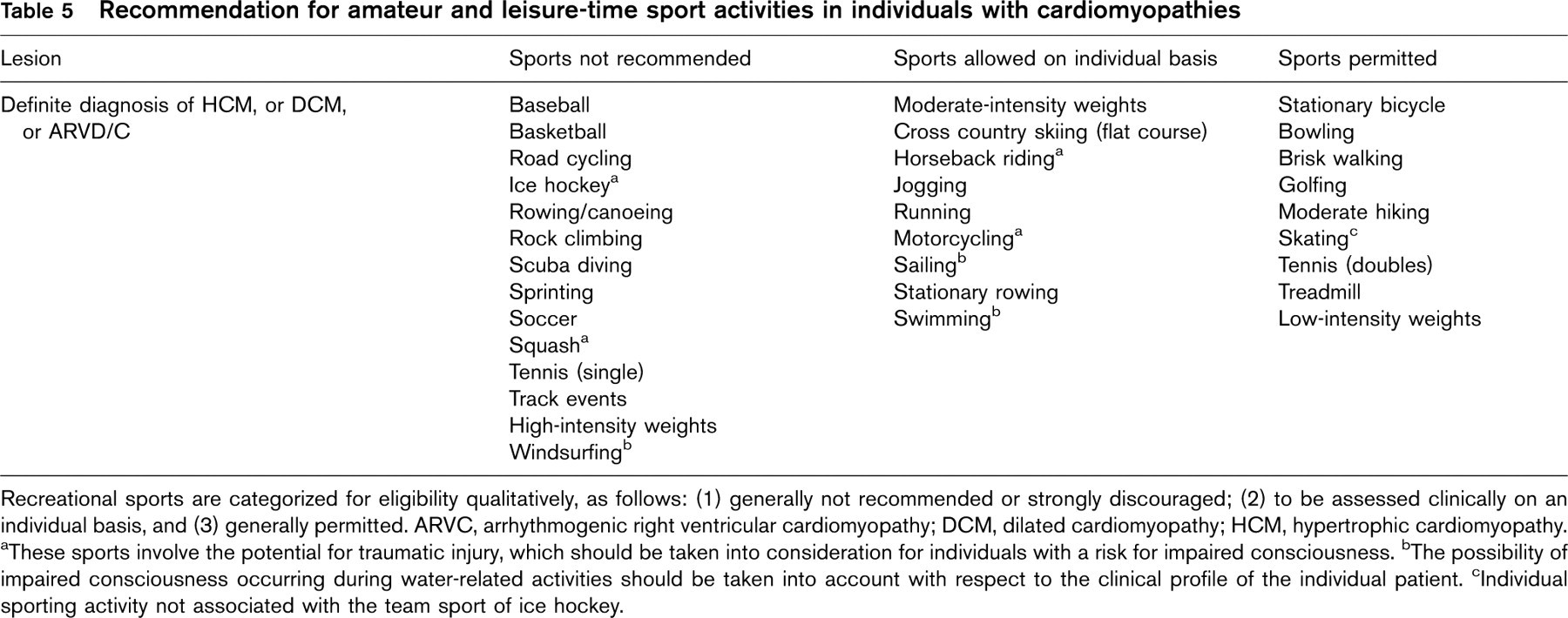
Recreational sports are categorized for eligibility qualitatively, as follows: (1) generally not recommended or strongly discouraged; (2) to be assessed clinically on an individual basis, and (3) generally permitted. ARVC, arrhythmogenic right ventricular cardiomyopathy; DCM, dilated cardiomyopathy; HCM, hypertrophic cardiomyopathy.
aThese sports involve the potential for traumatic injury, which should be taken into consideration for individuals with a risk for impaired consciousness.
bThe possibility of impaired consciousness occurring during water-related activities should be taken into account with respect to the clinical profile of the individual patient.
cIndividual sporting activity not associated with the team sport of ice hockey.
Classification of sports
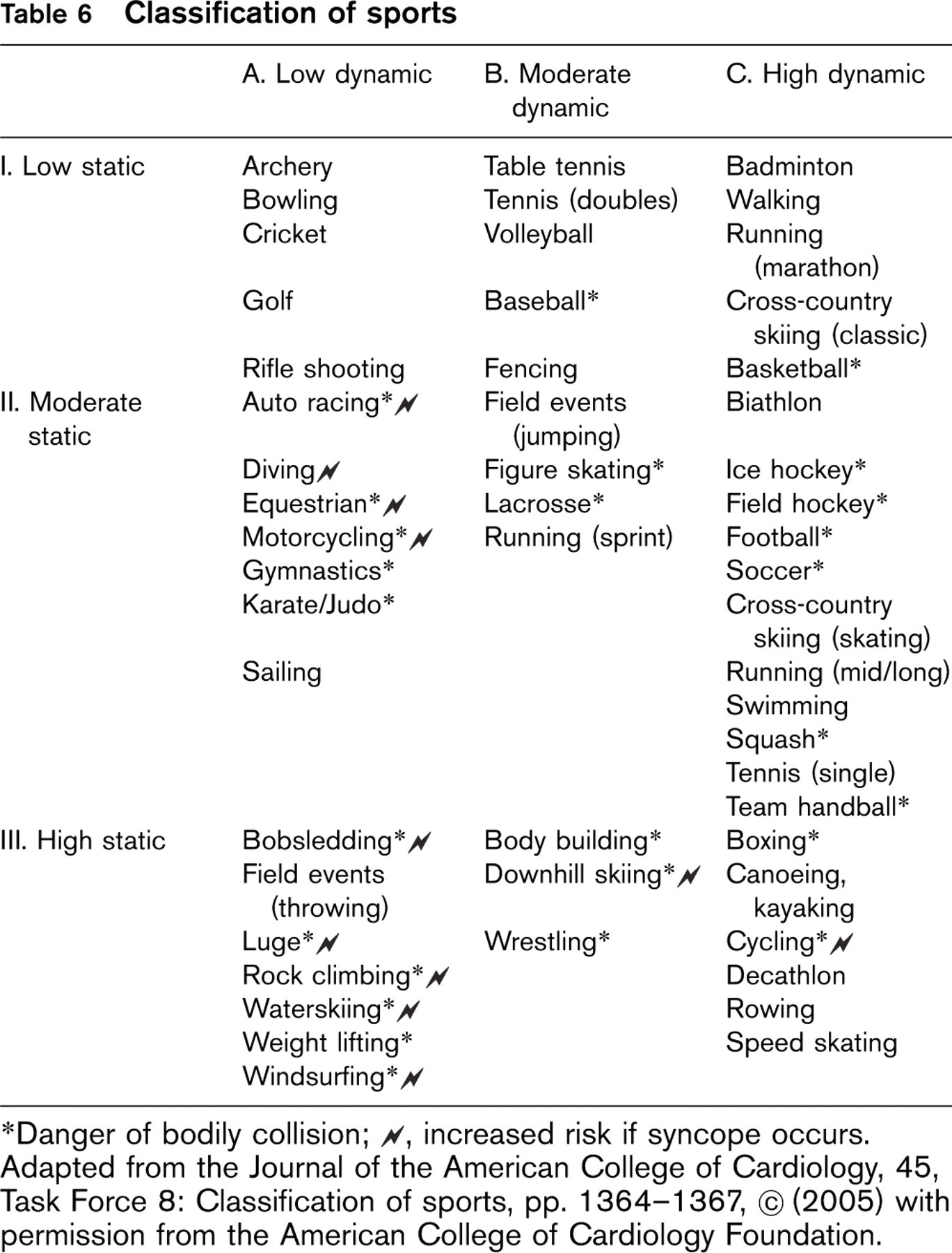
∗Danger of bodily collision;
‡increased risk if syncope occurs.
Adapted from the Journal of the American College of Cardiology, 45, Task Force 8: Classification of sports, pp. 1364–1367, ‡ (2005) with permission from the American College of Cardiology Foundation.
Physical education classes for young patients with cardiomyopathies
Questions related to participation in recreational exercise often arise with regard to compulsory physical education classes in elementary or junior high school. Many components of such classes may be truly recreational and clearly cannot be regarded as competitive in nature. We suggest that parents undertake a review of physical education class requirements in concert with school officials and their physician, and participation in physical education classes should be individualized as much as possible. In consideration of the relevance of social and educational aspects of physical exercise for children and young individuals, this panel suggests avoiding unnecessary prohibition for participation in school gym classes.
Myocarditis
Myocarditis is defined as an inflammatory process of the myocardium, with histological evidence of myocyte degeneration and necrosis of non-ischaemic origin, associated with inflammatory infiltration [31]. Myocarditis can be diagnosed by established histopathological, histochemical or molecular criteria, but is challenging to identify clinically. Suspicion may be raised by symptoms such as chest pain, exertional dyspnoea, fatigue, syncope, palpitations, or ECG changes including ventricular tachyarrhythmias, ST–T changes or conduction abnormalities. Myocarditis may evolve into a chronic inflammation, often with a subclinical course, and eventually progress into dilated cardiomyopathy; it is of ultimate importance, therefore, to respect an adequate period of athletic rest, until the disease has completely resolved. This is valid for competitive and amateur/leisure time athletes.
Evaluation
The clinical evaluation of athletes with suspected myocarditis includes personal and family history, physical examination, 12-lead ECG and echocardiography. Additional testing (such as 24-h ECG monitoring) may be required according to the specific case.
History
The clinical picture usually starts with upper respiratory or gastrointestinal symptoms, but palpitations, fatigability, exertional dyspnoea or syncope can occur. Evidence of a flu-like illness, or epidemiological circumstances supporting previous viral infection should be assessed.
12-Lead ECG
The electrocardiographic abnormalities include frequent and/or complex ventricular and/or supraventricular arrhythmias, ST–T segment alteration (usually depression; rarely elevation), T wave inversion and, occasionally, LBBB or AV blocks [32].
Echocardiography
Global LV enlargement and dysfunction can be evident in certain cases [33]; however, localized wall motion abnormalities (usually in the apex), mildly enlarged LV cavity and borderline depression of systolic function are common. Tissue Doppler imaging may be useful to detect regional abnormalities of LV relaxation, suggestive of the presence of an inflammatory lesion [34]. Modest pericardial effusion may be present, associated with increased reflectivity of the pericardial leaflets.
Histology
Biopsy is not usually performed in the routine diagnostic course and may be reserved for selected circumstances. When clinical judgement suggests the presence of myocarditis, endomyocardial biopsy may clarify an otherwise ambiguous clinical profile. Because of the patchy distribution of inflammatory cells, biopsies are often insensitive and frequently yield false-negative histological results. However, histology testing can be enhanced by molecular analysis with polymerase chain reaction amplification of the viral genome, which may yield a definitive diagnosis [35].
Recommendations for participation in competitive sports (Table 2)
Athletes with clinical diagnosis of myocarditis should be temporarily excluded from competitive and amateur leisure-time sports activity. This recommendation is independent of age, gender and does not differ for athletes with only mild symptoms, or those under treatment with drugs. After resolution of the clinical picture (at least 6 months after the onset of the disease), clinical reassessment is indicated prior to resuming competitive sports.
Other myocardial diseases
A number of other uncommon diseases of the myocardium deserve consideration as potential causes of sudden death in athletes. These include primary non-hypertrophied restrictive cardiomyopathy, systemic infiltrative diseases with secondary cardiac involvement such as sarcoidosis, and also isolated non-compaction of LV myocardium with or without systolic dysfunction. Few data are presently available regarding the relative risks of athletic training and competition in athletes with the aforementioned myocardial diseases.
Recommendation
Until more information is available in this regard, recommendations regarding participation in sports and leisure-time activities should be tailored to the individual case after expert cardiovascular evaluation.
Pericarditis
Pericarditis is defined as an inflammatory process of the pericardium, which may also affect the subepicardial layers of myocardium.
Evaluation
The assessment of athletes with suspected pericarditis includes personal and family history, physical examination, 12-lead ECG and echocardiography.
History
Pericarditis usually starts with upper respiratory or gastrointestinal symptoms, but clinical presentation may include chest pain, increased fatigability or exertional dyspnoea. The onset of the disease may also be concealed, and the clinical course characterized by only transient fever, without significant symptoms.
12-Lead ECG
ECG in patients with pericarditis includes a spectrum of abnormalities, with the most common ST/T wave alterations mimicking ischaemic heart disease, and ventricular or supraventricular tachyarrhythmias.
Echocardiography
Often a pericardial effusion is present at the onset of the disease, with increased reflectivity and separation of the pericardial leaflets.
Recommendations for participation in competitive sport (Table 2)
Athletes with clinical diagnosis of pericarditis should be temporarily excluded from competitive and amateur sports activity. This recommendation is independent of age and gender, and does not differ for those athletes with only mild symptoms, or under treatment with drugs. After resolution of the clinical picture (at least 3 months after the onset of the disease), clinical reassessment is indicated before resuming competitive sports. Athletes can return to full sports activity when there is no longer evidence of active disease and serum markers of inflammation have returned to normal.
For pericarditis associated with evidence of myocardial involvement, eligibility recommendations should be based on the course of myocarditis.
Chronic pericardial disease that results in constriction disqualifies the patient from all competitive sports.
Addendum: classification of sports
A classification of the different sports is provided in Table 6. Sports activities are classified into two main categories (i.e. dynamic and static) and intensity is roughly divided into low, moderate and high. This classification is intended to provide a schematic indication of the CV demand associated with different sports, with an additional notification of those disciplines associated with increased risk of bodily collision and those associated with an enhanced risk if syncope occurs (which should be avoided in certain cardiac patients).