
Abstract
Background
Plant stanol esters in spreads have demonstrated efficacy in reducing serum cholesterol. The cost-effectiveness of plant stanol esters in the prevention of coronary heart disease, however, has remained unevaluated.
Design
A Bayesian modelling approach was applied to synthesize clinical evidence and evaluate the cost-effectiveness (€/quality-adjusted life years) of plant stanol esters in spread in the prevention of coronary heart disease based on published FINRISK and 4S risk functions.
Results
The regular use of plant stanol esters reduced total serum cholesterol by −0.362 mmol/l [95% credibility interval (CrI) −0.31 to −0.41]. The corresponding placebo-adjusted reduction attributable to stanol esters when combined with statin was −0.385 mmol/l (95% CrI −0.18 to −0.61). The cost-effectiveness estimations were assessed for men and women separately at four different initial ages at which the regular use of stanol esters was assumed to be started. The base case cost per quality-adjusted life years gained by using stanol esters regularly ranged from €7436 to €20 999 in men and from €34 327 to €112151 in women based on the initial starting age. According to uncertainty analysis, there is over a 90% probability that the use of plant stanol esters is cost-effective for men inclusively and for 60-year-old and older women assuming that decision-makers' maximum willingness to pay per quality-adjusted life year is €50000.
Conclusions
A recommendation that plant stanol ester-containing spreads be used as a part of daily diet replacing regular spread could be viewed as potentially cost-effective public health policy in the prevention of CHD in all adult men and in older age-groups of women with total serum cholesterol levels of 5 mmol/l or greater.
Introduction
Coronary heart disease (CHD) is a major cause of death in many Western countries and is becoming an important cause of morbidity and mortality worldwide [1]. In Finland, CHD is the leading cause of death for both men and women and it accounts for a substantial share of healthcare costs. In 2003, the total healthcare costs attributable to CHD were estimated to be €286 million [2].
One of the major risk factors that predispose an individual to CHD is an elevated serum cholesterol concentration, a risk which can be modified by changes in diet. Incorporating foods enriched with plant stanols or sterols into the daily diet can substantially enhance the cholesterol-lowering effect of diet. Controlled trials have demonstrated that daily intake of 2 g of stanols or sterols can reduce low-density lipoprotein (LDL) cholesterol by about 10% [3, 4]. Considered from both the viewpoint of the individual patient and the whole population, this reduction is significant. A meta-analysis of cohort studies showed that a long-term reduction in serum cholesterol concentration of 0.6 mmol/l (i.e. about 10%), lowers the risk of ischemic heart disease by 50% at age 40, falling to 20% at age 70 [5].
The cost-effectiveness of prevention strategies for CHD has been widely studied. The evaluated interventions have included primary prevention with statins [6], smoking cessation counselling [7], dietary advice [8] and exercise [8, 9]. The cost-effectiveness of plant stanol and sterol esters, however, has remained unevaluated though the use of spreads containing plant stanol or sterols as part of a healthy diet could potentially help to reduce the incidence of CHD and in that way impact on the associated healthcare costs.
In the present study, we have evaluated the cost-effectiveness (€/quality-adjusted life years; QALY) of plant stanol ester incorporated in spread in the prevention of CHD without and with the combination of 3-hydroxy-3-methylglutaryl coenzyme A inhibitors (statins). In the current study, cardiovascular prevention is understood as a reduction of absolute risk for CHD, irrespective of clinical stage. We assessed the cost-effectiveness of plant stanol ester enriched daily diet compared with a normal daily diet from society's point of view. Productivity changes due to the intervention are not considered, however, in our analysis.
Methods
Clinical efficacy
We carried out two meta-analyses, which were based on systematic literature reviews. The first concentrated on studies examining total cholesterol reduction with plant stanol ester added to the spread. The second review was carried out to obtain information about reducing total cholesterol with the combination of plant stanol ester-added spread and statin drug treatment. We selected the change in total cholesterol as a primary endpoint in meta-analyses, since all our CHD risk prediction algorithms applied in a model included total cholesterol as a risk factor.
We identified the trials from Medline and the Cochrane collaboration database (to December 2004), and previous review articles [3, 4]. We included all randomized placebo-controlled trials, irrespective of participants' sex, age or disease. Participants in most trials were healthy with above average lipid concentrations. We excluded trials that used free stanols or some other product than spread, or participants that were children or had ileostoma. Trials using plant stanol ester and statin treatment in combination were utilized only in the second meta-analysis. The efficacy of plant stanol ester was defined as the reduction in serum total cholesterol concentration, expressed as the change from the placebo period in the treated group in cross-over studies or versus placebo groups in studies with parallel design.
Due to perceived differences in the trial designs, methods and patient characteristics, we applied a Bayesian random effects model to estimate the summary measure for the placebo-adjusted effect size for total cholesterol [10, 11]. To adopt a full Bayesian approach, we specified prior distributions for the overall pooled effect size parameter and the between-trial heterogeneity parameter. We used non-informative prior distributions, however, to ensure that the data from the trials dominated the final inferences. Furthermore, we used the random effects meta-regression approach to determine whether other recorded factors, such as trial size, dose, trial duration, age, and the baseline cholesterol level of participants would modify the effect size for total cholesterol [12].
Decision model
We constructed a discrete-state discrete-time Markov model to estimate the expected costs and health outcomes in terms of gains in QALYs associated with a plant stanol ester-enriched daily diet and normal daily diet among hypothetical cohorts of Finnish men and women at a specific age who were initially without established CHD. We carried out the estimations for men and women separately at four different initial ages (30, 40, 50 and 60 years) at which the regular use of plant stanol ester as a part of daily diet was assumed to be started.
The structure of the Markov model was based on a previously published CHD model [13]. The simplified flow chart of the Markov model is illustrated in Fig. 1 Our Markov model used an annual cycle length. Each year, the hypothetical cohort of men or women without established CHD were at risk of having of a fatal non-cardiovascular event, a fatal CHD event, an acute non-fatal CHD event, or they might survive to the next year without the occurrence of any CHD event. After that year, the subjects' risk factors were updated based on Finnish age and sex-specific risk factor profile data and the Markov model was run again until all subjects in the cohort were entered into terminal states or until 100 years of age was reached. The age of 100 years was determined to be the maximum allowed subject age in the Markov model.
Assessing the risks of coronary heart disease and non-coronary heart disease events
We used data derived from the FINRISK [14, 15] and Health 2000 [16] studies to determine age and sex-specific risk factor profiles (including total serum cholesterol level, mmol/l; systolic blood pressure, mmHg; high-density lipoprotein cholesterol level, mmol/l; smoking prevalence, %; and diabetes prevalence, %) for the cohorts of interest in the Markov model. We estimated the age and sex-specific annual risk of non-CHD death cause by subtracting down the total mortality (derived from Finnish standard all-cause mortality life-tables by age and sex) by the fraction of deaths due to cardiovascular diseases (ICD-10 I20-I25, I46, R96, and R98) [17, 18]. We estimated the annual total risk of initial non-fatal CHD event (ICD-10: I20-I21) or CHD death (ICD-10: I20-I25) using the modified (i.e. the risk of events were estimated per annum instead of over 10-year periods) FINRISK risk function [19]. We used age and sex-specific probabilities obtained from the National Cardiovascular Disease Register to allocate the total FINRISK risk function predictions into the two health states (hospitalization due to non-fatal CHD event or CHD death) in the Markov model [18]. After the initial occurrence of the non-fatal CHD event, the model was programmed to transit subjects to the secondary prevention part of the Markov model (i.e. the history of CHD event health state). We estimated the annual risk of the subsequent events using a risk function derived from the 4S study [20]. Finally, we combined the pooled estimates of reduction in total serum cholesterol (mmol/l) from the meta-analyses with FINRISK and 4S risk functions to estimate reduction in the annual risk of CHD events in subjects using plant stanol ester.
Costs
We estimated all costs from a societal perspective including the direct costs of prevention and morbidity. All costs were estimated in year 2001 Euros. When CHD developed in subjects, the model tracked the costs due to hospitalization and other treatments. The average age and sex-specific costs of hospitalization and outpatient care were based on a Finnish dataset comprising 9226 patients [21].
We programmed the Markov model assuming that after the discharge subjects received a prescription for chronic CHD or dyslipidemia medication. In year 2001, the average annual medicine cost of treating chronic CHD was €163 in both men and women based on National Agency for Medicines' and the Social Insurance Institution's databases [22]. The average annual costs for treating dyslipidemia associated with chronic CHD were €438 in men and €416 in women [22]. For modelling purposes, we estimated the average annual medicine costs. The average annual medicine costs were estimated by weighting the average costs by the proportion of recorded patients in both medicine categories in Finland [22]. The weighted average annual costs of medicines were €239 and €225 in men and women, respectively.
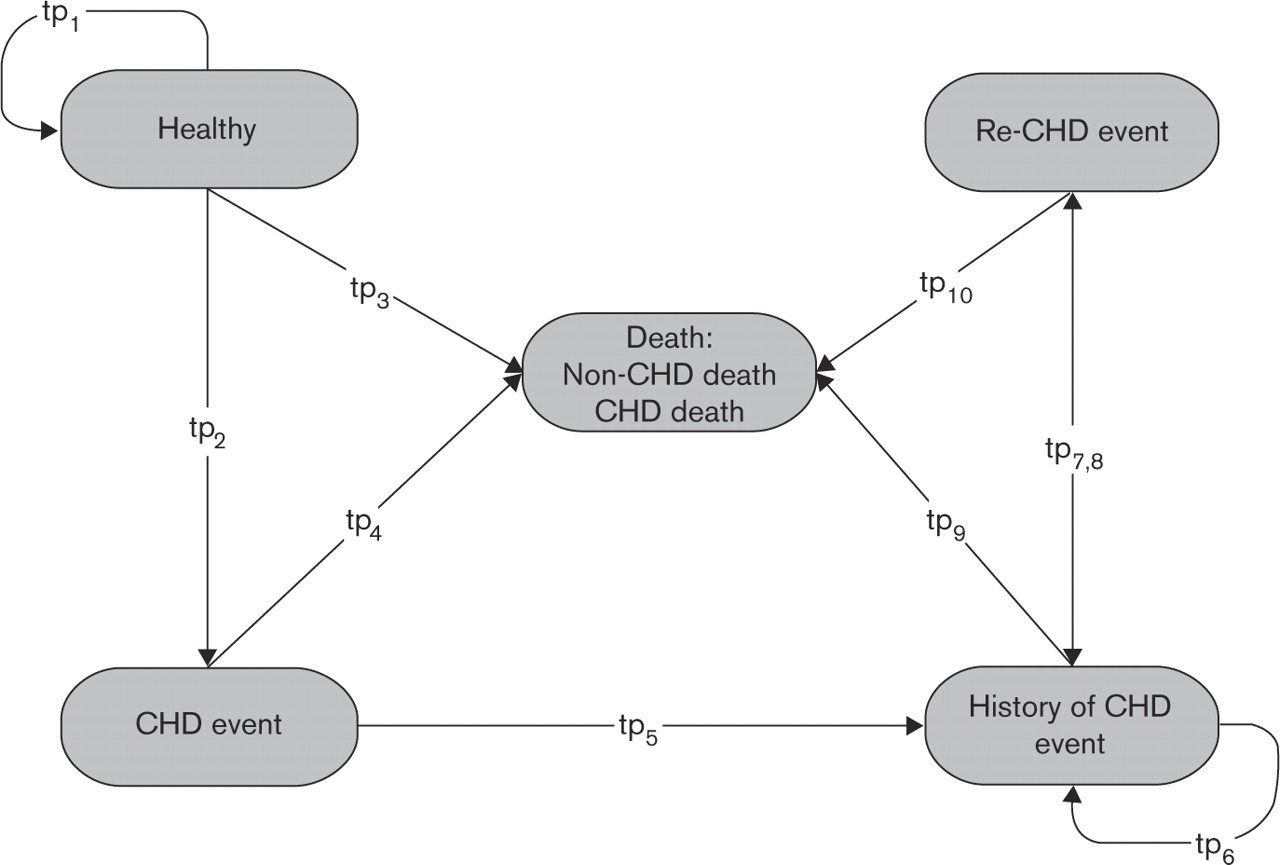
Simplified illustration of the Markov model for outcomes. Transition probabilities conditional to age and sex between defined health states were derived from life-tables and risk functions based on FINRISK and 4S studies. CHD, coronary heart disease; tpn, (annual) transition probability.
In the model, plant stanol ester was assumed to be incorporated into a spread. The cost of plant stanol ester spread (Raisio Benecol; Raisio, Finland) and corresponding regular spread (Raisio Keiju light) were obtained from a survey by The Finnish Consumer Agency and the state provincial offices [23]. The average price for plant stanol ester spread was estimated to be €13.2 per kilogram and the price of recommended daily dose (2 g) €120 per year. The price of using plant stanol ester spread was compared with the price of using regular spread that is equivalent to the plant stanol ester spread but lacks the added plant stanols. The additional cost of using the recommended dose of plant stanol ester spread per day was estimated to be €97 per year.
Quality of life
We obtained the age and sex-specific quality of life for the population of interest without acute CHD events from a Finnish EQ-5D survey (n = 2374) [24]. When a CHD event occurred in subjects, the model tracked the decreases in quality of life due to the CHD event. The disutility due to the initial or subsequent CHD event was estimated to be approximately −0.078 (SD 0.245) in men and −0.127 (SD 0.247) in women as measured by the EQ-5D instrument from a dataset of 615 patients who underwent coronary artery bypass grafting (CABG) or percutaneous transluminal coronary angioplasty (PTCA) in Finland [25].
We assumed that after 12 months, the postoperative quality of life had linearly improved to the same level as in the age and sex-matched general population [25]. The use of plant stanol ester as such was not assumed to affect the quality of life.
Discounting
In the base case scenario, we discounted costs and quality-adjusted life years at 3.5% per annum to generate the present value of future costs and health benefits [26]. In terms of sensitivity analyses, the results are presented also when costs and health benefits are discounted at 0% and 5% (as recommended by the Finnish health economic guidelines) per annum.
Uncertainty analysis
We performed the meta-analyses and uncertainty simulations within a Bayesian modelling framework. The Bayesian modelling framework offers a coherent approach to synthesize all available sources of evidence into a single model [27]. The advantages of the Bayesian modelling framework have been discussed in more detail elsewhere [28, 29]. We estimated the joint posterior distribution of the model parameters by simulation using the Gibbs sampler programmed in WinBUGS software (version 1.4; MRC Biostatistics Unit, Cambridge, UK). Final posterior parameter estimates were based on a total of 10000 Markov Chain Monte Carlo (MCMC) samples. The first 2000 samples were discarded to ensure stability of the posterior sampling procedure. Results are reported with 95% credibility intervals (CrIs), analogous to confidence intervals from a frequentist approach.
The decision as to whether the use of plant stanol ester incorporated in spread is cost-effective in the prevention of CHD depends on the decision-makers' maximum willingness to pay for additional QALY gained with the use of plant stanol ester-added spread. To illustrate this decision uncertainty, we constructed cost-effectiveness acceptability curves for the cost per QALY gained [30].
Results
Clinical efficacy
The primary clinical outcome was a reduction in total serum cholesterol levels (mmol/l) (Table 1 [31–53]. The first meta-analysis included a total of 19 randomized trials [31–49]. All these trials were placebo controlled and their design was either parallel or crossover. The trials included a total of 1192 subjects from Europe, Australia, Canada, and Japan with the trial durations ranging from 3 to 52 weeks, and stanol doses of 0.8 to 3.4 g/day. The random effect meta-analysis indicated a mean difference of 0.362 mmol/l (95% CrI 0.31–0.41) when comparing the effect of plant stanol ester and placebo in lowering the total cholesterol level. A corresponding mean percentage change in total cholesterol level was 6% (95% CrI 5.1–6.8). Based on the results of random effect meta-regression, none of the selected trial-level covariates were significant confounders. Thus, these results ensured the appropriateness of data synthesis for the pooled analysis.
The second meta-analysis included five trials of reducing total cholesterol with the combination of plant stanol ester and statin treatment (Table 1 [40, 50–53]. Of the studies, three trials were placebo controlled and in two studies, the effect of plant stanol ester and statin treatment was compared with the baseline diet. The studies included 191 subjects from Europe and USA. The statins used in the studies were simvastatin, pravastatin, atorvastatin and lovastatin at doses of 10–40 mg/day. Pooled results from the combination treatments showed that the plant stanol ester was able to decrease total cholesterol levels more efficiently when combined with statin treatment in comparison with a single drug or plant stanol ester therapy alone. The mean placebo-adjusted decrease in total cholesterol level was 0.385 mmol/l (95% CrI 0.18–0.61). The corresponding mean percentage change in total cholesterol was 6.2% (95% CrI 2.9–9.9).
Cost-effectiveness
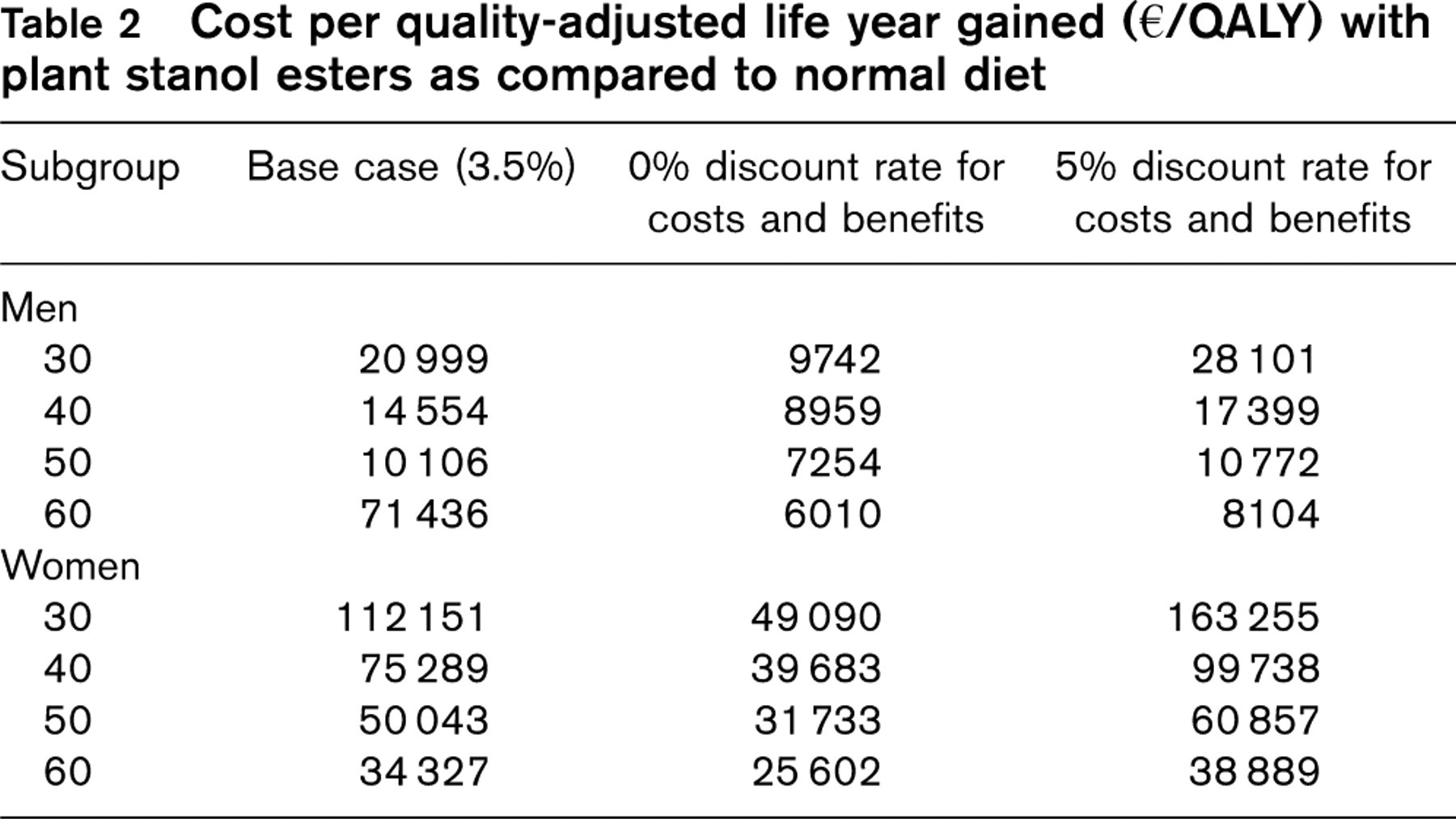
The primary economic outcome was cost (€) per QALY. Table 2 shows the mean cost per QALY estimates in different age groups for men and women. The use of different discount rates for both costs and benefits markedly altered the cost per QALY gained by 19–56% (9–46%) this being dependent on age and sex. The costs of plant stanol esters were partly offset due to savings in the healthcare sector. Discounted lifetime cost savings in the healthcare sector ranged approximately from €20.4 to €124 per subject conditional on age and sex, if the cost of plant stanol ester was ignored. These saving estimates are real savings to healthcare providers, since the cost of the plant stanol ester spread is actually paid by the consumer.
Description of the studies included in the meta-analysis
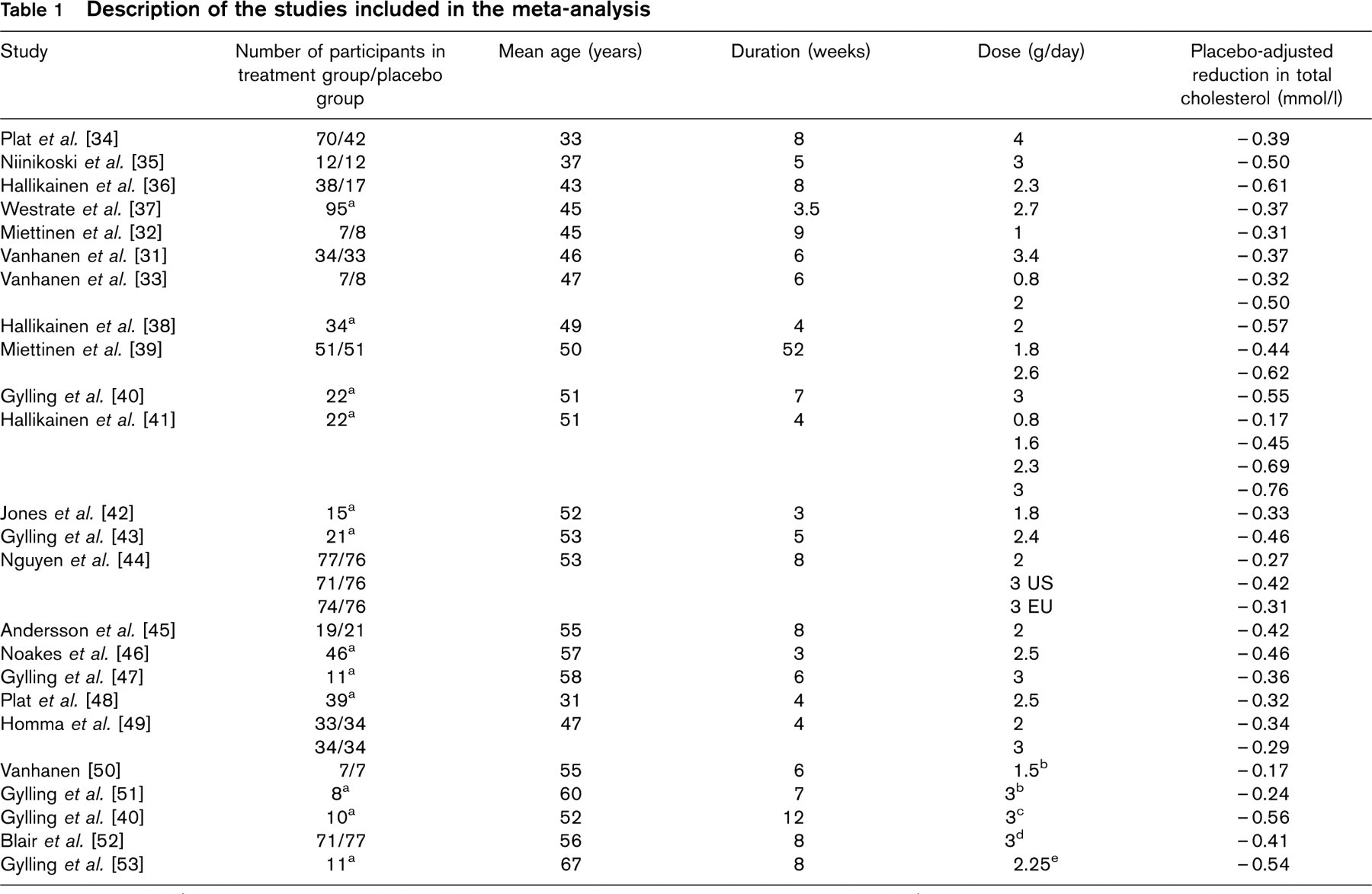
aCross-over studies.
bCombined with pravastatin 40 mg/day.
cCombined with simvastatin 10–20 mg/day.
dCombined with lovastatin, pravastatin, simvastatin or atorvastatin, doses/day not available.
eCombined with simvastatin 20 mg/day.
Cost per quality-adjusted life year gained (€/QALY) with plant stanol esters as compared to normal diet
Figures 2 and 3 show the cost-effectiveness acceptability curves in different age groups for men and women in the base case. An incremental cost-effectiveness ratio (ICER) of about €30000-€50 000 per QALY gained is likely to be considered cost-effective by the National Institute for Health and Clinical Excellence (NICE) in the UK [54]. If the decision-makers' maximum willingness to pay per QALY gained is assumed to be this upper value, then the use of plant stanol ester is cost-effective for men in all age groups. For women at the age of 50years and younger there is a less than 15% probability, whereas at the age of 60 years and older there is an over 90% probability, that the use of plant stanol ester would be considered cost-effective, if the NICE scale of willingness to pay is used.
Discussion
Our study suggests that the use of plant stanol ester incorporated in spread is a cost-effective option in the prevention of CHD in all adult males and in women in older age-groups with average total serum cholesterol levels of 5 mmol/l or higher. The study results show that the regular use of plant stanol ester in the prevention of CHD yields an ICER which ranges from €7436 to €112 151, conditional on age and sex. The cost-effectiveness of plant stanol ester increases in older age groups, since age is the single strongest predictor of CHD risk [55]. Actually, it seems that, at least in Finland, plant stanol ester spread is mostly used by those age groups in which the cost-effectiveness is highest (i.e. the average user is aged 55 years or over) [56]. The use of plant stanol ester reveals significantly lower ICERs for men than for women in all age groups. No difference in the cholesterol-lowering response to plant stanol administration between sexes, however, has been reported [31–33]. The sex difference in ICER is probably due to the fact that CHD is markedly more common in men than in women [57]. For both sexes, CHD risk increases with age but the increase is sharper for women which can be also seen in the results of this analysis.
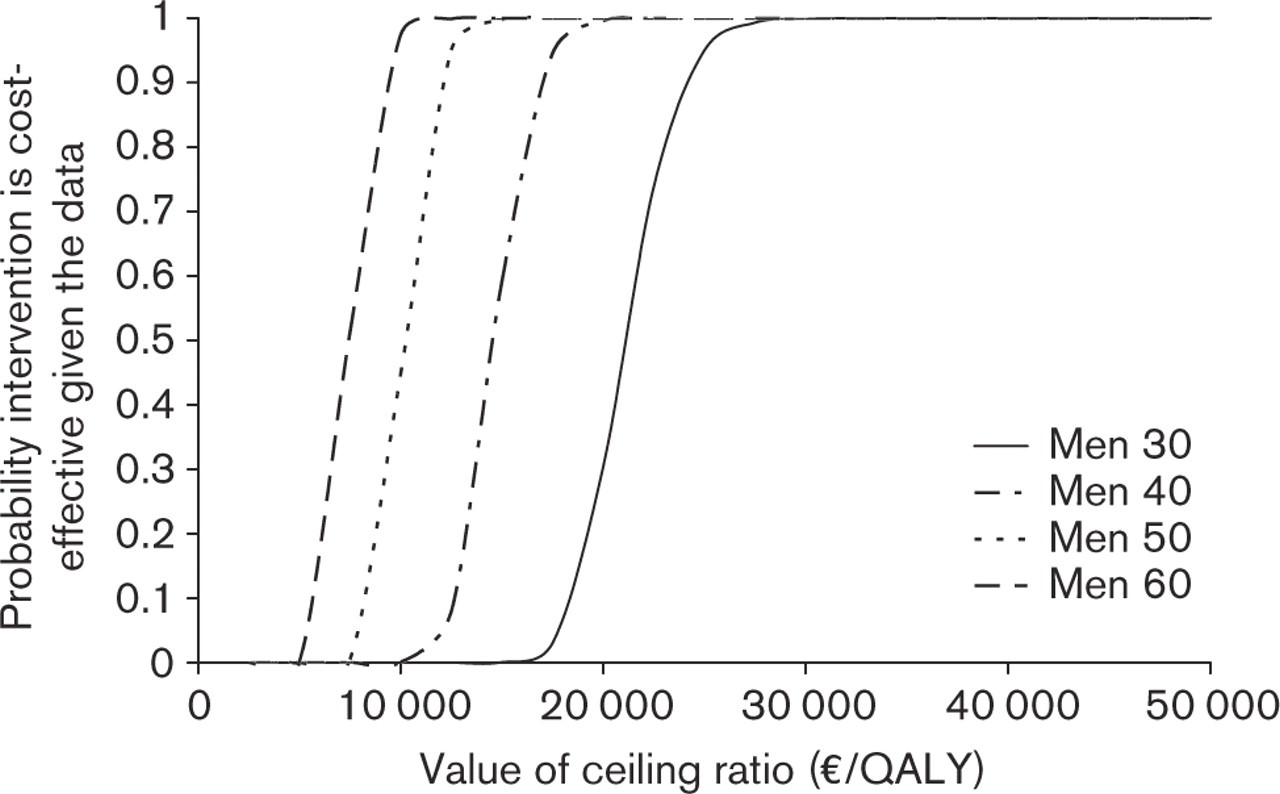
Cost-effectiveness acceptability curves for men applying 3.5% discount rate. Cost-effectiveness acceptability curve shows probability that plant stanol ester in spread is cost-effective as compared to daily diet with regular spread for a range of decision-makers' maximum willingness to pay (a ceiling ratio) for a quality-adjusted life year (QALY).
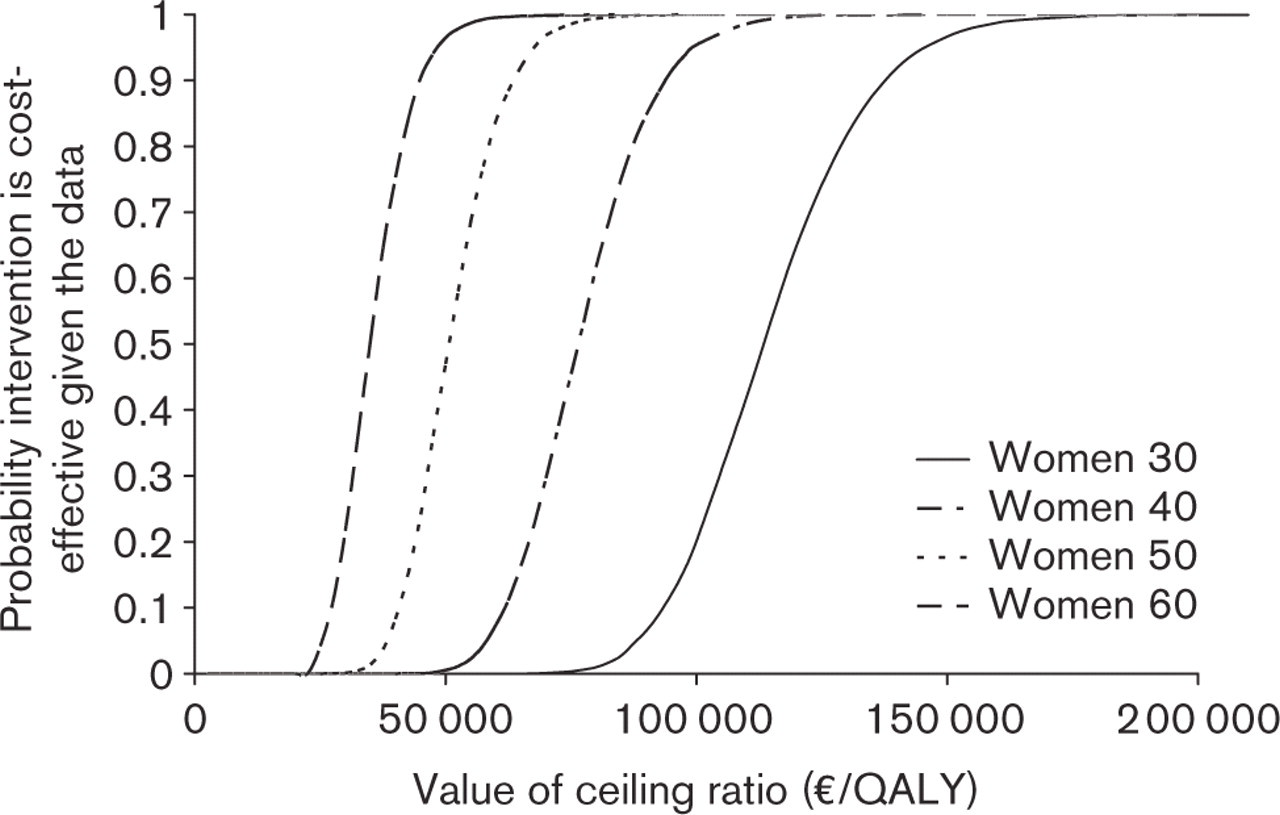
Cost-effectiveness acceptability curves for women applying 3.5% discount rate
For the purposes of this study, the adherence to using plant stanol ester spread was not examined and the consumed amount was assumed to be 25g daily (2 g stanol/day). The adherence in normal practice is likely to be less than perfect [58]. Changing from regular spread to plant stanol ester spread as the daily spread is a very minor change in dietary habits, however, when compared to many other interventions recommended to reduce CDH risk factors (e.g. smoking cessation, increasing physical activity) that require an active effort to modify the lifestyle. The effect of somewhat poorer adherence may be balanced, to some extent, by the fact that 5% of the Finnish adult population uses butter as their spread and 16% use mixtures of butter and plant oils [14]. When used as a substitute for butter, plant stanol ester spread will evoke an even greater reduction in cholesterol levels.
The current analysis was based on a Finnish healthcare setting and, therefore, the study results might not be directly transferable to other countries. Cost-effectiveness estimates might vary between countries, due, for example, to differences in CHD risk profiles, healthcare resource use, unit costs, and health state utilities. We believe, however, that the study results are at least somewhat relevant to other Western countries having populations with intermediate CHD mortality rates [59].
The study results are based on the assumption that changes in serum cholesterol levels could be converted to changes in the incidence of CHD events via the CHD risk equations. It is generally the case that economic models are able to predict fairly accurately the incidence of CHD events experienced by hypothetical individuals fulfilling selected entry criteria [60]. In the future, however, it would be valuable if the long-term cost-effectiveness of plant stanol ester could also be proved in a controlled and randomized trial.
Conclusion
Based on the results presented here, the recommendation that plant stanol ester incorporated in spread be used as a part of daily diet instead of regular spread could be viewed as cost-effective public health policy in the prevention of CHD in all adult males and in older age-groups of women with total serum cholesterol levels of 5 mmol/l or greater. The use of plant stanol ester in spread could also be seen as a potentially cost-effective option in the prevention of CHD when compared with previously published cost-utility estimates [61].