
Abstract
Endothelial progenitor cells (EPCs) are circulating precursor cells that have been implicated recently in vascular and cardiac regeneration. There is an ongoing discussion on the immunocytological definition of EPCs, based on various surface markers, and currently different cell types are included in the term ‘EPC’. This review summarizes the mechanisms that influence function, survival, mobilization and differentiation of EPCs. Furthermore, there are several reports on the clinical use of EPCs for the treatment of cardiovascular diseases. We have focused specifically on the influence of physical activity on EPC function.
Introduction
Endothelial dysfunction and a decline of endothelial cells are pathophysiological alterations that are common in the very early stages of a number of diseases, for example, atherosclerosis, erectile dysfunction, stroke (for a review see [1]) and kidney disease [2]. There is therefore a substantial need for therapies counteracting the progression of endothelial decline. The activation of endogenous mechanisms for endothelial repair may be a promising therapeutic option. In recent years a number of studies have provided evidence that stem cells may be able to substitute for the damaged endothelium [3, 4]. This review focuses on endothelial progenitor cells and their implication in (cardio)vascular function and regeneration.
Stem and progenitor cells: which is which?
An adult stem cell is an undifferentiated cell found among the differentiated cells of a tissue or organ that can renew itself and can differentiate to yield the major specialized cell types of the tissue or organ. The primary roles of adult stem cells in a living organism are to maintain and repair the tissue in which they are found (http://stemcells.nih.gov/info/basics/basics4.asp). Progenitor cells in general are pluripotent derivatives of adult stem cells. They possess a similar regeneration potential to adult stem cells but are terminated regarding their future function. However, this termination is still reversible. In contrast to adult stem cells, progenitor cells do not possess a self-renewing capacity. In recent years, progenitor cells have been found in several tissues, including heart, muscle, fat and skin. It is still under discussion whether multipotent stem cells survive in all self-renewing organs for a lifetime (so-called ‘tissue-specific’ progenitor cells, Fig. 1, lower part) or whether continuous supply from a central pool of stem cells (e.g. the bone marrow) takes place [5, 6]. It is possible that every self-renewing organ contains a small pool of tissue-specific stem cells that can meet the normal turnover of tissue-specific cells. However, if an injury occurs, this small pool can no longer produce sufficient amounts of tissue-specific cells. In this situation, stem cells/progenitor cells may be mobilized from the bone marrow (central pool) and directed to the injured tissue or organ.
Endothelial progenitor cells
Endothelial progenitor cells (EPCs) have been shown to derive from bone marrow and are considered to share common stem/progenitor cells with hematopoietic stem cells, that is, with bone marrow-derived stem cells responsible for development of red and white blood cells (for reviews see [7, 8]). It has become clear that at least two types of endothelial-lineage cells can be obtained by the in-vitro culture of mononuclear cells (Fig. 1).
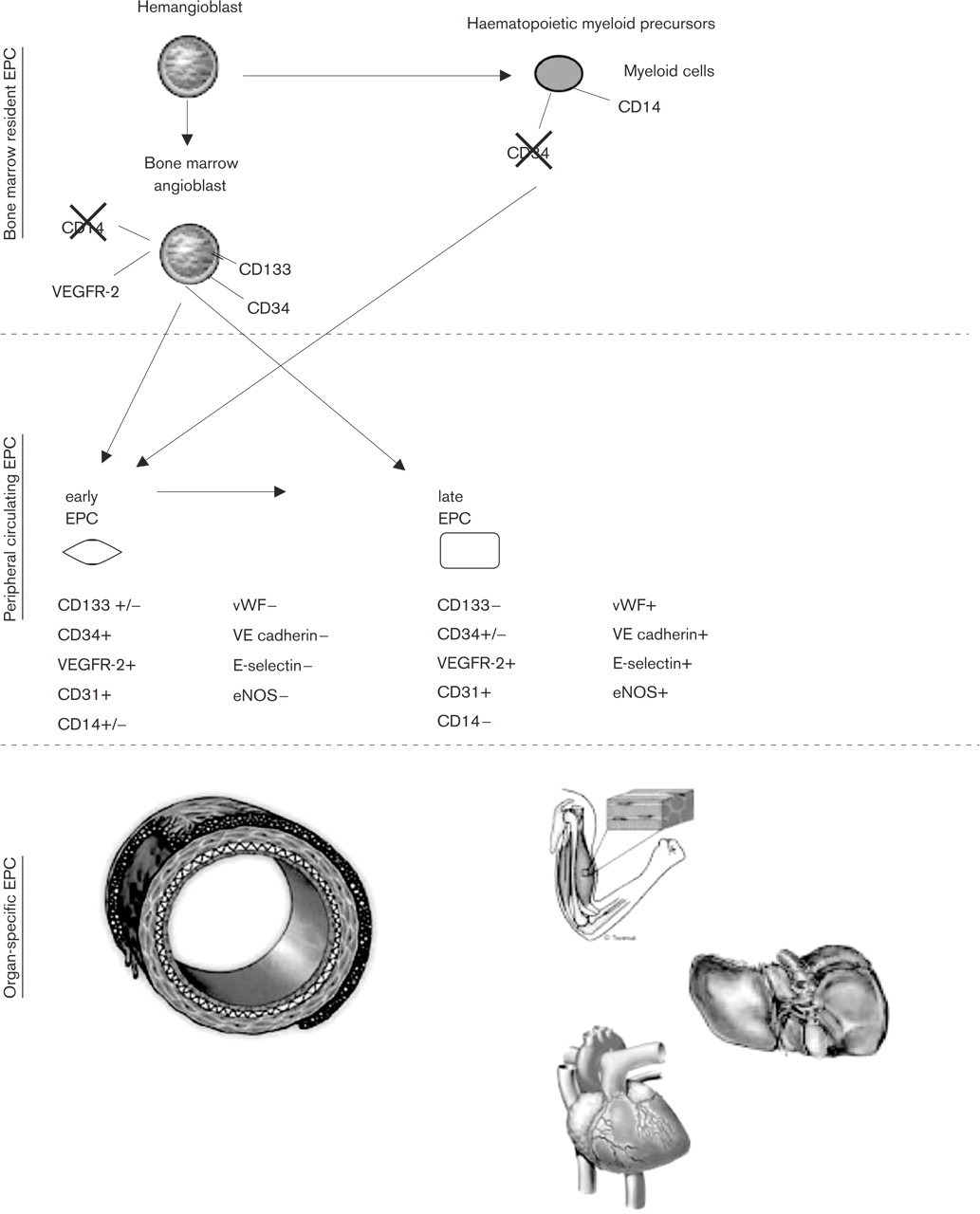
Scheme of the different endothelial stem cell and progenitor types.
A number of research groups define EPCs as the Ulex europaeus agglutinin (UEA) lectin and acetyl low-density lipoprotein (acLDL) double-positive spindle-shaped cells obtained after short-term in-vitro culture of the mono-nuclear cell fraction [9–11]. These monocyte-derived ‘early’ EPCs have a peak growth in culture after 2–3 weeks and die after 4 weeks in vitro [12]. Due to the short life cycle of the early EPCs, it has been suggested that their therapeutic effects may be mediated by the release of growth factors [9]. In addition, early EPCs have been shown to secrete a number of angiogenic, anti-angiogenic and neuroregulatory cytokines [13].
Additionally, so-called ‘late’ EPCs have been characterized. These cells grow from mononuclear cells after 2–3 weeks in culture and have a cobblestone-shaped morphology. Late EPCs show an exponential growth at 4–8 weeks and can be maintained in culture up to 12 weeks [14]. This means that these cells are growth regulated, which may be an advantage for the application of progenitor therapy, since it may avoid tumor formation [8]. Late EPCs release a smaller level of cytokines than early EPCs [12].
In addition, it has been proposed that endothelial cells can be generated directly from bone marrow-derived progenitor cells that are positive for the marker AC133/CD133 [15] (Fig. 1). These primarily bone marrow resident progenitor cells may correspond to the EPC pool residing in bone marrow, which can be mobilized rapidly upon a pro-angiogenic signal [most likely vascular endothelial growth factor (VEGF) via matrix metalloproteinase 9 (MMP9) induction] [15].
Endothelial progenitor cells and cardiovascular disease
Coronary artery disease is the most frequently occurring vascular disease in Western countries and leads to vessel occlusion and organ damage [16]. Since resident endothelial cells proliferate infrequently [17], it has been postulated that there are other sources of vascular replenishment in response to continuous damage [18]. These may be, for example, bone marrow-derived EPCs, which circulate in the peripheral blood and have been implicated in neoangiogenesis after tissue ischemia has occurred [19–22]. In line with this, the number and the activity of EPCs is increased in patients with myocardial infarction [23, 24].
However, the accumulation of cardiovascular risk factors, or an increased overall risk of coronary artery disease, is associated with dysfunction and decreased numbers of endothelial progenitor cells [25, 26]. It has been shown that the number and the activity of EPCs is decreased in chronic smokers [26–28] and patients with diabetes [29] or hypercholesterolemia [30].
In a recent study [31] it was shown that a single measurement of EPCs is a useful tool to predict cardiovascular outcomes in coronary artery disease (CAD) patients. Thus, there seems to be a close relationship between cardiovascular disease and the number of EPCs circulating in the blood. However, although early myocardial infarction or early stages of congestive heart failure may be linked to an increase in EPCs, there is also evidence that the EPC function is impaired [32]. Therefore, an autologous application/transplantation or a pharmacological mobilization/activation of EPCs may be future possibilities for the treatment of cardiovascular disease.
Exogenous endothelial progenitor cell transplantation
Monocyte-derived ‘late’ EPCs can be reliably and safely generated in vitro from autologous peripheral blood, and rapidly expanded in cell culture. Data on EPCs from animal models of neovascularization [21, 33] were followed by phase I clinical trials with ex-vivo cultivated autologous EPCs in patients with cardiovascular disease (TOPCARE-AMI study) [34]. However, the underlying mechanisms still remain to be defined.
The concept of therapeutic angiogenesis by the delivery of autologous EPCs or ‘crude’ bone marrow cells is currently being investigated in several trials. Early data from Stamm and co-workers [35] demonstrate the feasibility of the injection of isolated AC133+ bone marrow-derived cells in the border zone of myocardial infarction from patients undergoing bypass surgery. A very recent report from the randomized BOOST-study [36] showed that the intracoronary transfer of autologous bone marrow cells can result in improvement of left ventricular systolic function in patients after acute myocardial infarction. Further studies show an improvement of cardiac function after EPC injection [37] and a first blinded, randomized human study demonstrates that endothelial function improves after the application of EPCs in patients after recanalization of chronic coronary total occlusion [38]. However, the underlying mechanisms responsible for this success remain to be elucidated.
Endogenous endothelial progenitor cell activation
Endogenous mobilization of EPCs from the bone marrow may be an alternative way to improve endothelial regeneration, angiogenesis or neovascularization. In this context, VEGF and stromal-derived factor 1 (SDF-1), both of which have been shown to be released by ischemic tissue, seem to have important roles for mobilization of EPCs [39–41]. In line with this, it has been shown that recombinant VEGF increases circulating progenitor cells in humans [21]. In addition, some cytokines have been shown to mobilize EPCs and hematopoietic progenitor cells. This includes granulocyte monocyte colony-stimulating factor (GM-CSF) and granulocyte colony-stimulating factor (G-CSF), which is used for bone marrow transplantation. However, G-CSF also promotes inflammation by inducing a profound increase in the number of circulating leukocytes [42] and may thus induce the development of atherosclerotic lesions and restenosis, as shown in the MAGIC trial [43].
An alternative cytokine with a lower proinflammatory profile is erythropoietin (EPO), which has been shown to increase the number of endothelial cells in vitro [44, 45] and to stimulate the mobilization of circulating EPCs in peripheral blood in humans [46]. The serum concentration of EPO has been shown to be an independent predictor of EPC number and function in patients with coronary heart disease [47]. However, the application of EPO is associated with a number of side effects, for example, elevated blood pressure and thrombosis (for a review see [48]), and thus may not be indicated for the treatment of cardiovascular patients.
Pharmacological interventions on endothelial progenitor cell function
Several pharmacological substances have been shown to increase EPC numbers, e.g. statins induce the mobilization of EPCs from bone marrow [49, 50], which is linked to an increase in endothelial nitric oxide synthase (eNOS) activity [51]. Similar to the statins, the antidiabetic and anti-inflammatory peroxisome proliferator–activator receptor-γ agonists promote differentiation and mobilization of angiogenic progenitor cells and improve re-endothelialization after vascular intervention [52]. There is also evidence that the angiotensin receptor antagonists significantly increase EPC numbers after 4 weeks of therapy in patients suffering from diabetes [53].
Physical exercise as an endogenous mechanism for endothelial progenitor cell activation
Physical activity is associated with a decrease in vascular events [54, 55]. In addition, it has been shown that regular exercise training improves endothelial function and collateralization in patients with coronary artery disease [56, 57] and heart failure [58, 59]. There is evidence from experimental animal studies that a voluntary running wheel exercise in mice increased the number of circulating EPCs [60]. An increase in peripheral circulating EPCs was also measured in patients with stable coronary artery disease after 4 weeks intervention with bicycle ergometer training and moderate muscle training (lower-limb muscle training by shuttle device) or after a exercise-induced ischemia [61]. However, from these studies it cannot be differentiated whether the physical activity is the important stimulus for EPC mobilization or whether exercise-induced ischemia results in an EPC increase.
Further studies in healthy young men and women have shown that running exercise increases the number of EPCs, possibly due to an increase in nitric oxide bioavailability during exercise as a mediator for EPC release [62, 63]. In this context, it may be discussed whether endogenous nitric oxide liberation in bone marrow is modulated by physical activity. Although the basal release of nitric oxide is very high in bone marrow, further release of nitric oxide was achieved under hypobaric conditions [64]. These results may suggest that transient ischemia, such as may occur under physiological conditions during physical exercise or pathophysiological events (e.g. heart attack), may be a stimulus for EPC activation and mobilization from the bone marrow.
However, the training-mobilized EPC experiments were performed in young healthy volunteers who were exercising at either 82% max Vo2 (intense endurance training) or at 68% Vo2 max (moderate endurance exercise) [62]. It has to be mentioned that these protocols cannot be performed in patients at cardiovascular risk. There is evidence from endurance studies in marathon runners [63] and from patients with cardiovascular risk and coronary artery disease [65] that there is an increase in circulating EPCs linked to improved vascular function and nitric oxide release in the cardiovascular patients [65]. It has been demonstrated that ischemia seems to be important for the number of EPCs, whereas the function of EPCs (migration and incorporation into vascular structures) is improved by exercise training without ischemia [66]. Nevertheless, further studies have to be performed to provide evidence-based data on whether physical exercise, as performed in the context of cardiological rehabilitation, may improve EPC and thus endothelial function.
In conclusion (Table 1), EPC function and activity are impaired during the early stages of cardiovascular diseases and may, in the long term, contribute to the development of atherosclerosis. Specific pharmacological interventions may improve EPC function and may thus contribute to a restoration of vascular function. Stem-cell therapy with autologous EPCs may be a future therapeutic option. However, the underlying mechanisms contributing to the improvement of cardiovascular function need further examination. Physical exercise may be beneficial for the mobilization of EPCs. However, the underlying mechanisms have not yet been clearly elucidated. In addition, studies are needed to confirm whether the results obtained for healthy volunteers under optimal or moderate physical exercise conditions can be repeated in cardiovascular patients.
Overview of some aspects of endothelial progenitor cell (EPC) function and therapeutic options
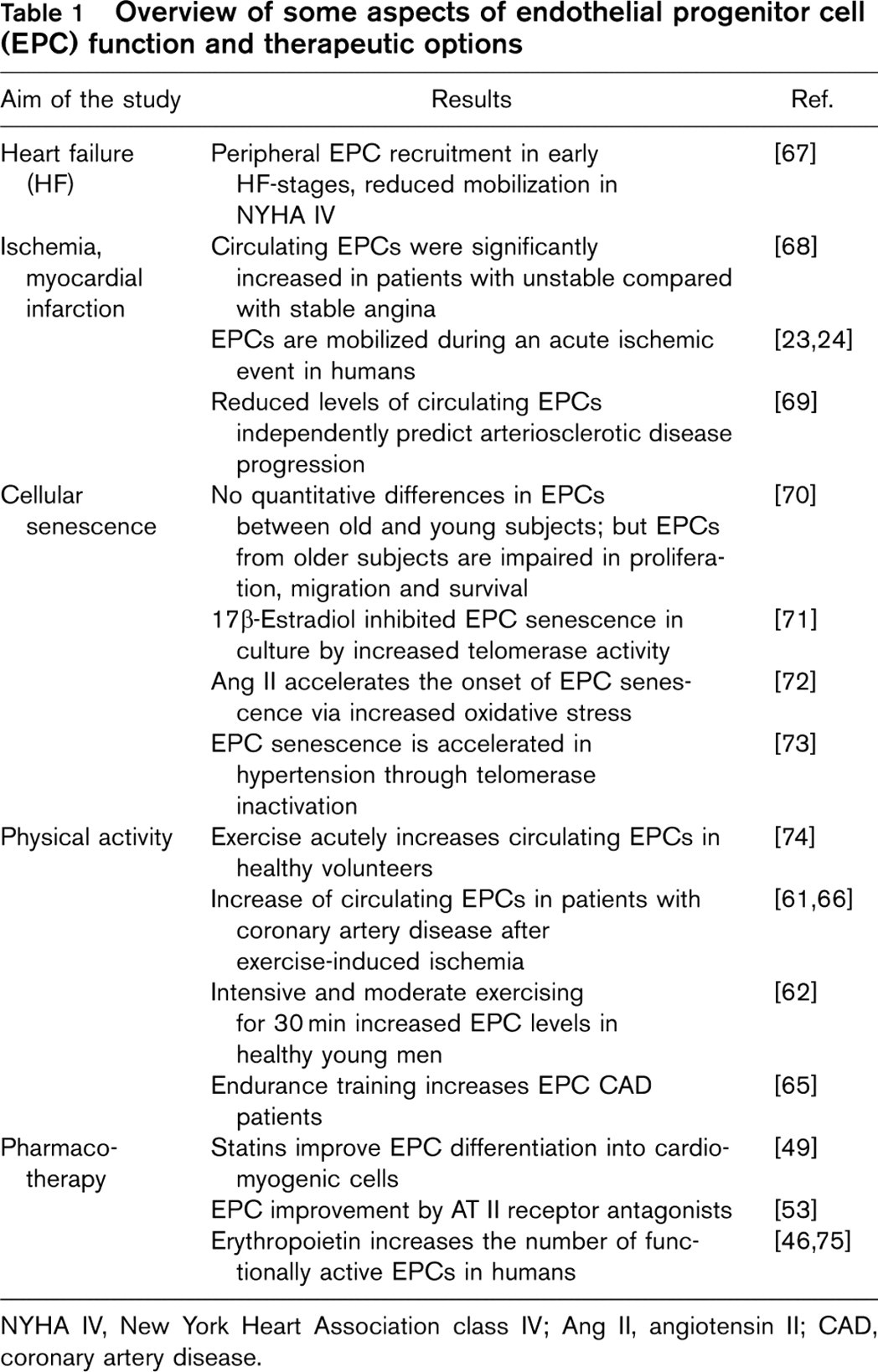
NYHA IV, New York Heart Association class IV; Ang II, angiotensin II; CAD, coronary artery disease.