
Abstract
Background
Exercise training reduces mortality in patients with coronary artery disease (CAD); however, the impact of habitual physical activity level (PAL) on vascular endothelial function and circulating endothelial progenitor cells (EPCs) remain unknown.
Methods
We assessed habitual PAL using a validated International Physical Activity Questionnaire in 116 patients (67.8 ± 9.5 years; 81% male) with stable CAD and preserved left ventricular ejection fraction ≥ 45%. The number of circulating CD34/KDR+ and CD133/KDR+ EPCs was determined by flow cytometry, and brachial artery flow-mediated dilation (FMD) was measured.
Results
The mean PAL of CAD patients with 1644 MET min/week (where MET is metabolic equivalents). With higher habitual PAL tertiles, there were significant linear trends of increased FMD (P = 0.001) and CD133/KDR+ EPCs (P = 0.03), but not of CD34/KDR+ EPCs. Patients with the highest tertile of PAL were associated with an absolute increase of 1.89% in FMD (relative increase 68%, P = 0.003) and 0.12% in CD133/KDR+ EPCs (relative increase 44%, P = 0.01) compared with those in the lowest tertile of PAL, after adjusting for age, sex, presence of hypertension, diabetes mellitus, hypercholesterolemia, smoking, and the use of medications including statins. However, neither CD34/KDR+ nor CD133/KDR+ EPCs significantly correlated with FMD.
Conclusion
This study showed that higher habitual PAL in patients with CAD was associated with higher FMD and EPC count. Nonetheless, FMD only significantly correlated with increased PAL, but not EPC, suggesting that increased physical activity improves endothelial function through mechanisms other than increasing EPC count.
Introduction
Coronary artery disease (CAD) is a major cause of morbidity and mortality in developed countries. Exercise can play a vital role in primary and secondary prevention of CAD. Several meta-analyses have shown that exercise training reduces total and cardiovascular mortality in patients with CAD [1, 2]. Endothelial dysfunction is known to be precursor of atherosclerosis and can predict future cardiovascular events [3]. Earlier studies have shown that regular physical activity attenuates the age-related decline in endothelial function in healthy individuals [4], and physical training improves endothelial function in patients with CAD [5–9]. However, the relationship between the level of habitual physical activity level (PAL) and endothelial function in patients with CAD remains unclear. Recent studies suggest that circulating endothelial progenitor cells (EPCs) contribute to the vascular repair and maintenance of endothelial function [10]. The level of circulating EPC is associated with the severity of CAD and cardiovascular outcome [11, 12]. Furthermore, exercise training increased circulating EPC numbers and migratory activity [13–15], but there is limited evidence for the link between habitual physical activity and EPC count.
We hypothesized that a higher habitual physical activity is associated with an increased circulating EPC, which improve vascular endothelial function in patients with CAD. Therefore, we investigated the relationships between habitual physical activity and brachial flow-mediated dilation (FMD), a measure of endothelial function, and circulating CD34/KDR+ and CD133/KDR+ EPC numbers in patients with stable CAD.
Methods
Study population
Consecutive patients with stable CAD having greater than 50% stenosis in at least one of the major coronary arteries as documented by coronary angiogram were recruited from the Cardiac Clinic in Queen Mary Hospital, Hong Kong. All patients received stable medications for at least 6 months before enrollment. Patients with recent acute coronary syndrome or percutaneous coronary intervention in the past 3 months, significant valvular heart disease, left ventricular ejection fraction less than 45%, exacerbated chronic obstructive pulmonary disease, significant renal or hepatic dysfunction, and severe orthopedic conditions that prohibit exercise, were excluded from the study. The study was approved by the local institutional review board, and all participants provided informed consent.
Study design
Baseline demographic data and cardiovascular medications were documented in all the participants. Cardiovascular risk factors, including tobacco smoking, diabetes mellitus, hypercholesterolemia, hypertension, and family history of cardiovascular diseases diagnosed in first-degree relatives before 55 years of age were assessed. The body height and weight, blood pressure and body mass index of all the participants were measured as described earlier [16]. Hypertension was defined as either systolic or diastolic blood pressure ≥ 140/90 mmHg at two different clinical visits or the use of medications. Diabetes mellitus was defined as fasting serum glucose of ≥ 7.0 mmol/l or treatment with hypoglycemic medications. Hypercholesterolemia was defined as a fasting total serum cholesterol level of ≥ 4.9 mmol/l or treatment with lipid-lowering medications. Smoking status was recorded as either smoker (past or current) or nonsmoker.
Fasting blood samples were obtained from all the participants to determine serum creatinine, glucose and lipid levels, including total cholesterol, low-density lipoprotein cholesterol (LDL-C), high-density lipoprotein cholesterol (HDL-C), triglyceride, apolipoprotein A-I, apolipoprotein B and lipoprotein (a). Plasma high sensitivity C-reactive protein (hsCRP) level was measured by using a Hitachi 747 analyzer (Boehringer Mannheim, Mannheim, Germany) and a particle-enhanced immunoturbidimetric assay (Roche Diagnostics, Mannheim, Germany) as described earlier [17].
Flow cytometry
The circulating EPCs were defined by the expression of surface markers CD34/KDR+ and CD133/KDR+ and their numbers were measured by fluorescence-activated cell analysis of peripheral blood sample as described earlier [16]. In brief, 100 μl of peripheral blood was incubated with a phycoerythrin-conjugated monoclonal antibody against human KDR (Sigma, St Louis, Missouri, USA), followed by a fluorescein isothiocyanate (FITC)-conjugated CD34 and CD133 antibodies (Beckman Coulter, Fullerton, California, USA). FITC-labeled anti-human CD45 antibody was used for differential gating during flow analysis. FITC-labeled IgG1a (Beckman Coulter) and phycoerythrin-labeled IgG2b (Becton Dickinson, Franklin Lakes, New Jersey, USA) served as the isotypic control for color compensation. Analysis was performed with an automated fluorescence-activated cell counter (Elite; Beckman Coulter) in which 1 000 000 events were counted. The percentages of all the measured components defined as the absolute cell counts divided by the lymphocyte counts were calculated. The intraobserver variability testing found an intraclass correlation coefficient of 0.9 (P < 0.001).
Brachial endothelial function
Vascular ultrasound was performed with a high-resolution ultrasound system (Agilent Sonos 5500; Philips, Andover, Massachusetts, USA) with the use of a 7.5-MHz linear array transducer by two experienced operators without the knowledge of the participants. All of the scanned images were stored digitally and analyzed offline by the same operators, who were blinded to the identity of studied participants. All participants were studied in the fasting state, and all vasoactive medications were withheld for ≥ 12 h before the study. As described earlier [18], longitudinal scans of the brachial artery were obtained at rest, and then brachial FMD was induced by inflation of a pneumatic tourniquet placed on the forearm to a pressure of 250 mmHg for 5 min. The diameter of the brachial artery was allowed to return to baseline. Finally, the diameter of the brachial artery was obtained 5 min after the administration of 400 μg sublingual nitroglycerin spray. FMD was calculated as the percentage change in diameter from baseline to the diameter at 60s of reactive hyperemia. The FMD measurements were reproducible, as evidenced by interobserver variability study in 25 patients showing an intraclass correlation coefficient of 0.88 (P < 0.001), whereas the intraobserver variability correlation coefficients for two different operators were 0.90 and 0.84 (both P < 0.001).
Assessment of habitual physical activity level
Habitual PAL was assessed by using a validated International Physical Activity Questionnaire (IPAQ) by a single experienced interviewer. The questionnaire had been validated internationally [19] and its Chinese version had also been validated in Hong Kong Chinese [20] as well as in older Chinese patients [21]. The IPAQ was conducted as described earlier [20, 21]. In brief, participants were asked to report on the time they spent walking, in vigorous-intensity and moderate-intensity activity lasting at least 10 min and in sedentary activity over the last 7 days. Habitual PAL was obtained by estimating the total weekly energy expenditure (MET-min/week; where MET is metabolic equivalents), which was calculated by weighting the reported duration of each activity category performed per week by a MET energy expenditure estimate assigned to each category of activity. The weight for each category of activity was defined as follows: 3.3 METs for walking, 4 METs for moderate activity, and 8 METs for vigorous activity. The intraobserver variability testing found an intraclass correlation coefficient of 0.94 (P < 0.001).
Statistical analysis
Continuous variables were expressed as mean ± SD. Categorical data were presented as frequencies and percentages. Statistical comparisons were performed with the Student's t-test, Pearson's χ2 test, or the Fisher's exact test as appropriate. Comparisons of variables between different tertiles of PAL were performed with one-way analysis of variance (ANOVA) with post-hoc Bonferroni's correction for multiple comparisons and test for linear trend. Absolute changes and 95% confidence intervals of FMD and EPC counts were calculated by using univariate and multivariate linear regression analyses, to determine the effect of higher PAL after the adjustment for potential confounding variables. Based on the data from our previous observational study, we assumed an SD of 3% for FMD; in order to detect a difference of 2% in FMD from any of the three tertiles of PAL with 80% power and a 5% false-positive error rate, we would require at least 102 participants in a one-way ANOVA design. A value of P less than 0.05 was considered statistically significant.
Results
A total of 116 patients with CAD were enrolled. The clinical characteristics of the study population are presented in Table 1. Their mean age was 67.8 ± 9.5 years, and 81% of the participants were men. Among them, 40% of CAD patients had a prior history of myocardial infarction and 83% underwent percutaneous or surgical coronary revascularization.
Effect of habitual physical activity on vascular function and endothelial progenitor cell count
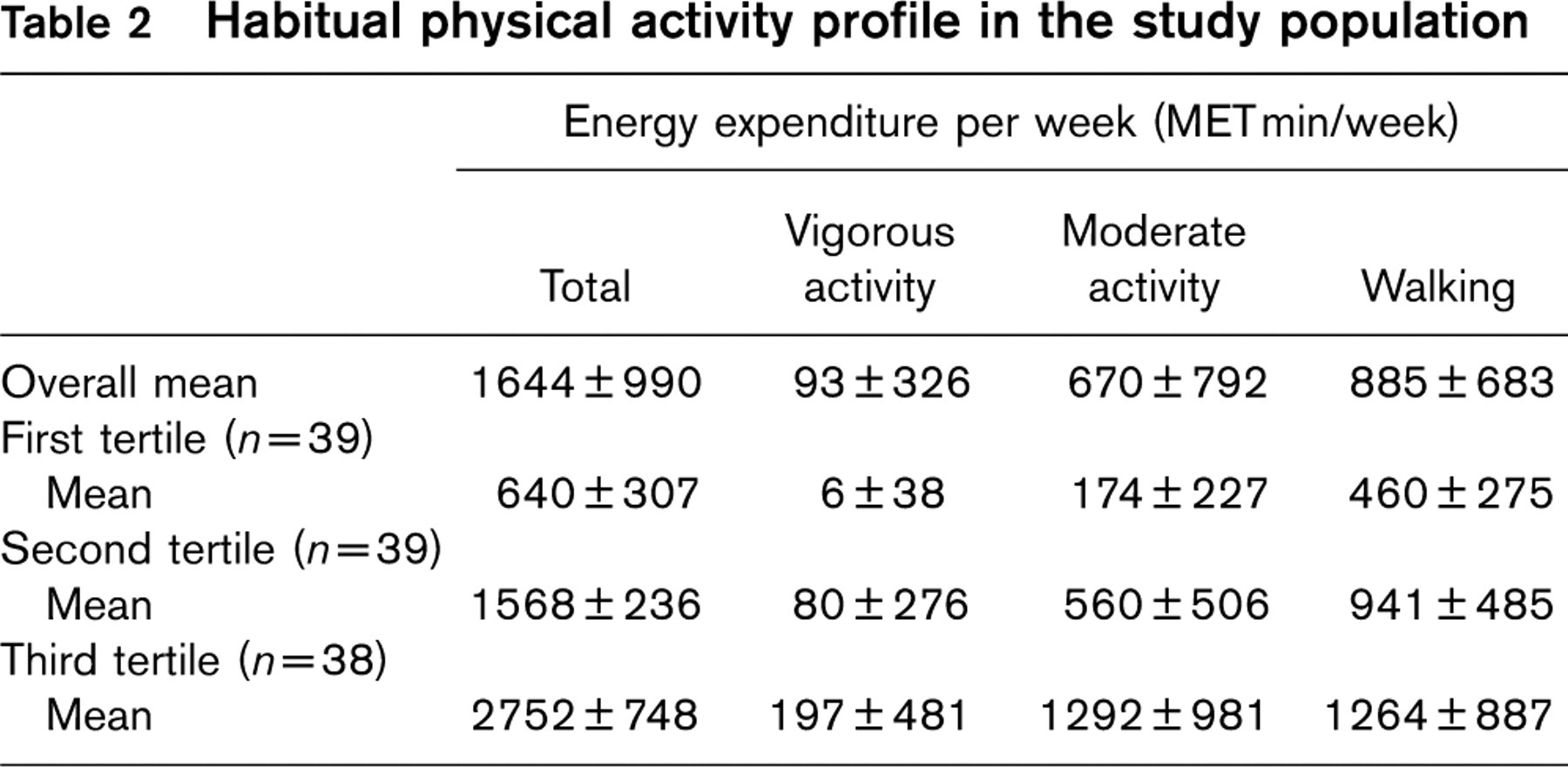
To better delineate the relationship between habitual PAL and different clinical characteristics, the study population was grouped into three tertiles of PAL according to the patients’ total weekly energy expenditure. The mean total physical activity measured was 1644 ± 990 MET min/week. As shown in Table 2, patients in the highest PAL tertile mainly participated in moderate-intensity exercise, and their high volume of physical activity was not solely attributed to the amount they spent on vigorous activity.
Clinical characteristics of the study population
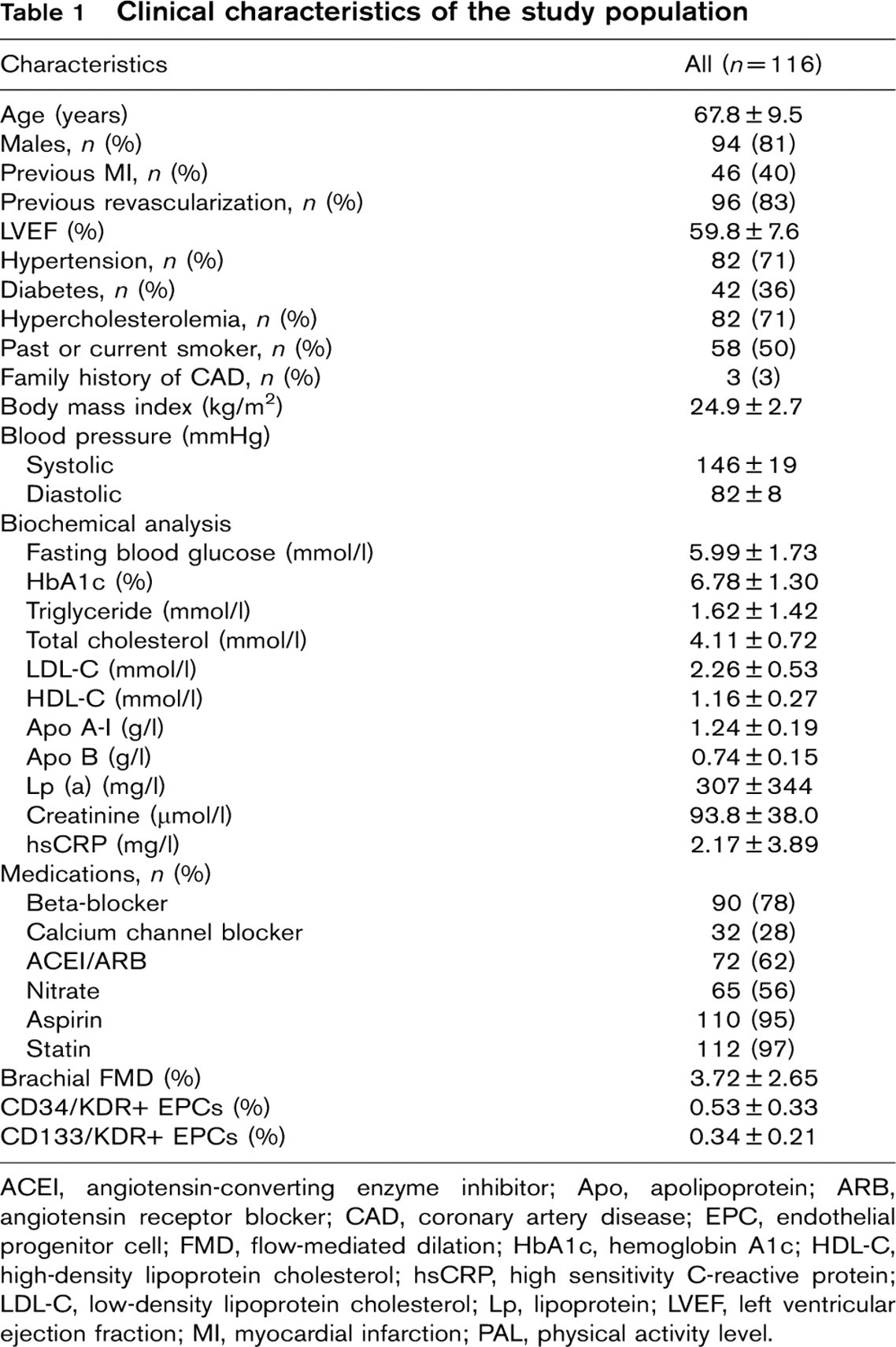
ACEI, angiotensin-converting enzyme inhibitor; Apo, apolipoprotein; ARB, angiotensin receptor blocker; CAD, coronary artery disease; EPC, endothelial progenitor cell; FMD, flow-mediated dilation; HbA1c, hemoglobin A1c; HDL-C, high-density lipoprotein cholesterol; hsCRP, high sensitivity C-reactive protein; LDL-C, low-density lipoprotein cholesterol; Lp, lipoprotein; LVEF, left ventricular ejection fraction; MI, myocardial infarction; PAL, physical activity level.
Habitual physical activity profile in the study population
Unadjusted effect of habitual physical activity on FMD and EPC numbers using ANOVA
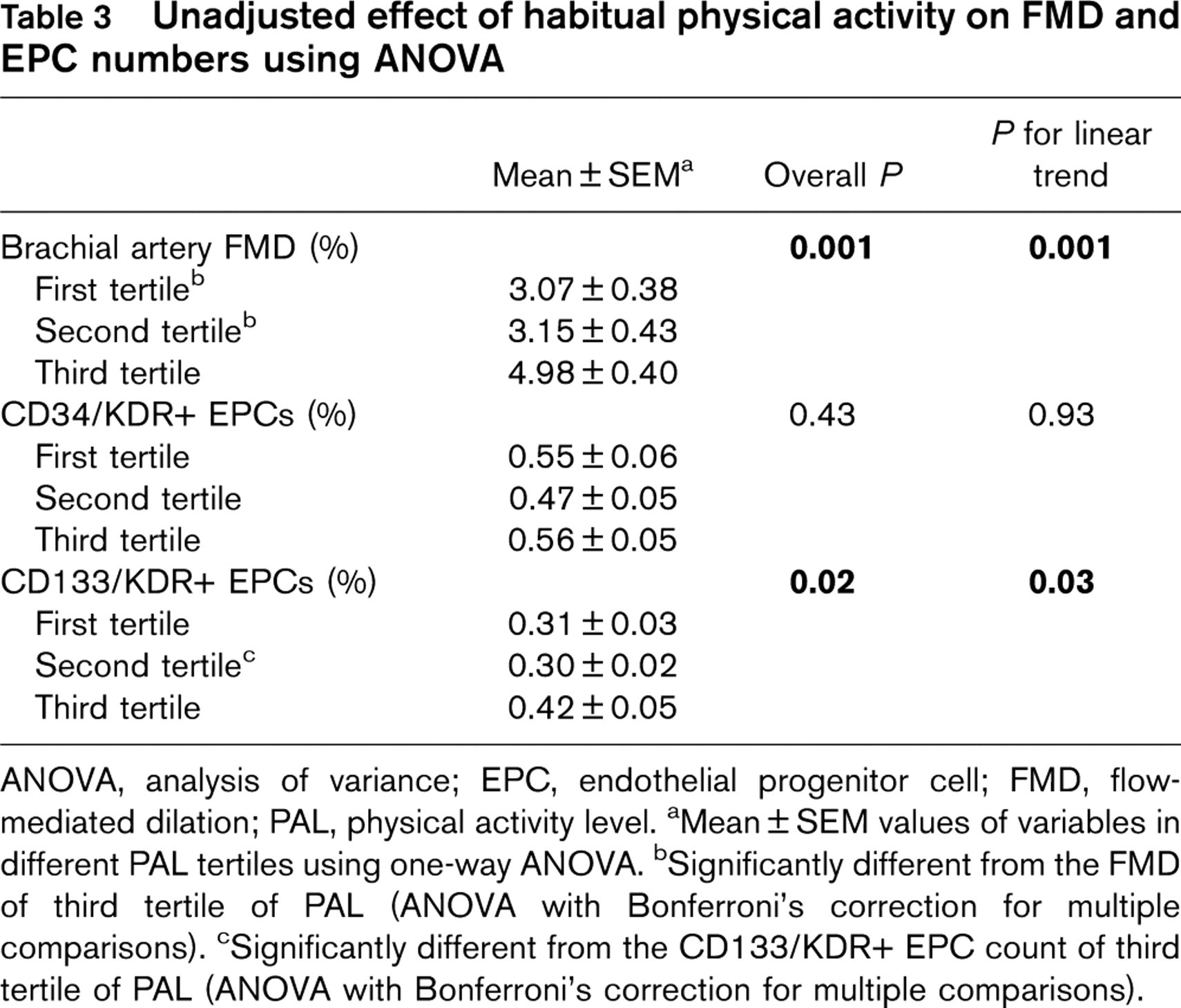
ANOVA, analysis of variance; EPC, endothelial progenitor cell; FMD, flow-mediated dilation; PAL, physical activity level. aMean ± SEM values of variables in different PAL tertiles using one-way ANOVA. bSignificantly different from the FMD of third tertile of PAL (ANOVA with Bonferroni's correction for multiple comparisons). cSignificantly different from the CD133/KDR+ EPC count of third tertile of PAL (ANOVA with Bonferroni's correction for multiple comparisons).
The effect of PAL tertiles on FMD and two populations of EPCs were analyzed by ANOVA with post-hoc test for linear trend and Bonferroni's correction for multiple comparisons was performed on the differences in FMD and EPCs. As shown in Table 3, there were significant trends of increased FMD (P = 0.001) and CD133/KDR+ EPCs (P = 0.03), but not of CD34/KDR+ EPCs with increasing tertiles of habitual physical activity. Participants in the third tertile of habitual physical activity had a significantly higher FMD than those in the first and second tertiles (P < 0.05, Fig. 1). Furthermore, patients in the third tertile of habitual physical activity had a significantly higher CD133/KDR+ EPC count than those in the second but not in the first tertile (P < 0.05, Fig. 2).
Adjusted effects of physical activity level on vascular endothelial function and endothelial progenitor cell count
Multivariate linear regression was used to analyze the adjusted effects of PAL on FMD and CD133/KDR+ EPC count. The effect of habitual PAL on FMD was adjusted for age, sex, hypertension, diabetes mellitus, hypercholesterolemia, smoking status, and use of medications including β-blockers, angiotensin-converting enzyme inhibitors or angiotensin receptor blockers and statins, as these factors are known to affect FMD (Table 4). The second compared with the first PAL tertile was associated with an absolute increase in FMD of 0.15% (adjusted P > 0.05), which was statistically insignificant; whereas the third compared to the first PAL tertile was associated with a significant absolute increase of 1.89% in FMD (adjusted P = 0.003), accounting for a relative increase of 68% in FMD. Nevertheless, the amount of vigorous or moderate physical activity alone was not predictive of changes in FMD (all P > 0.05).
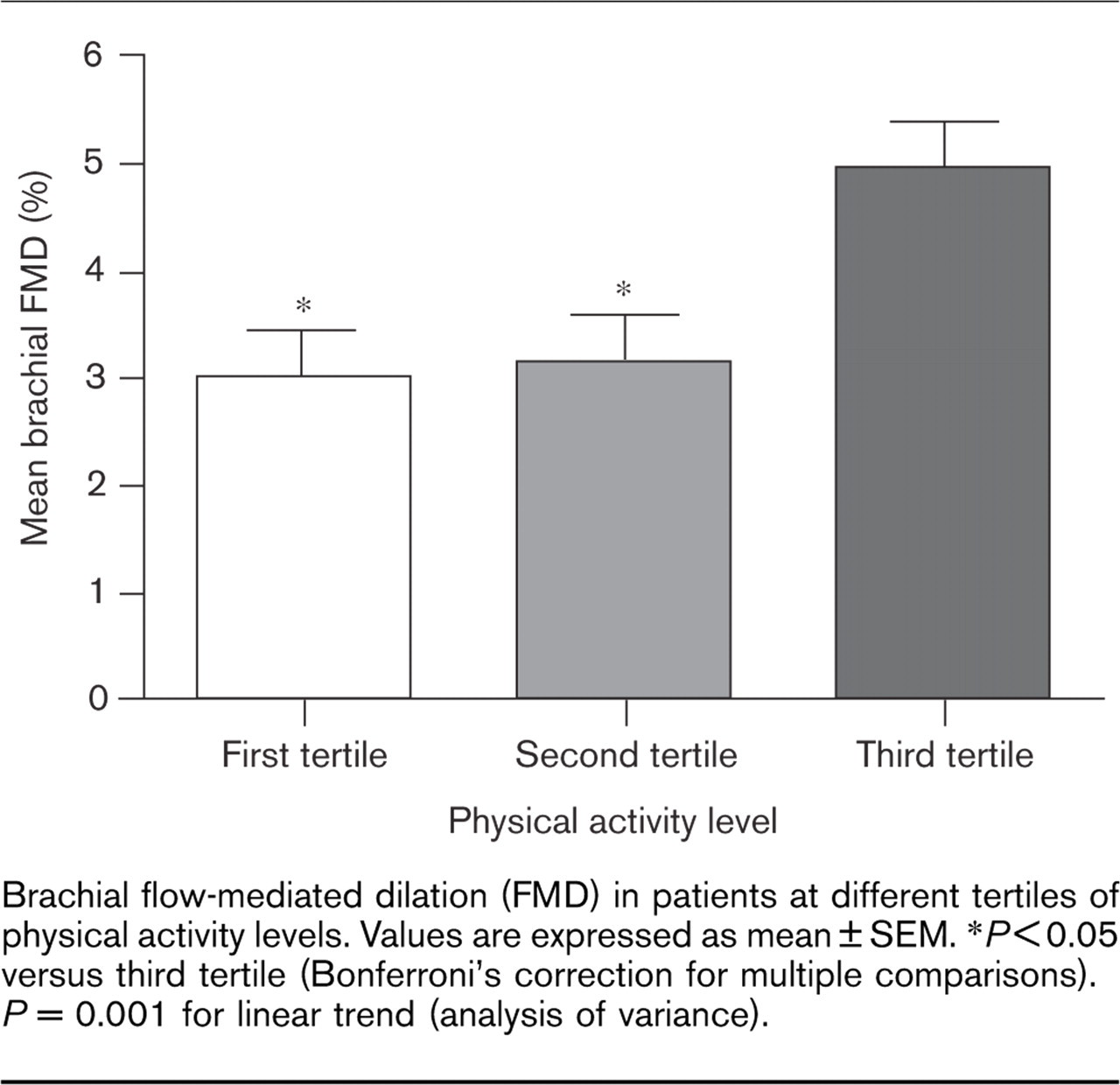
Brachial flow-mediated dilation (FMD) in patients at different tertiles of physical activity levels. Values are expressed as mean ± SEM. ∗P < 0.05 versus third tertile (Bonferroni's correction for multiple comparisons). P = 0.001 for linear trend (analysis of variance).
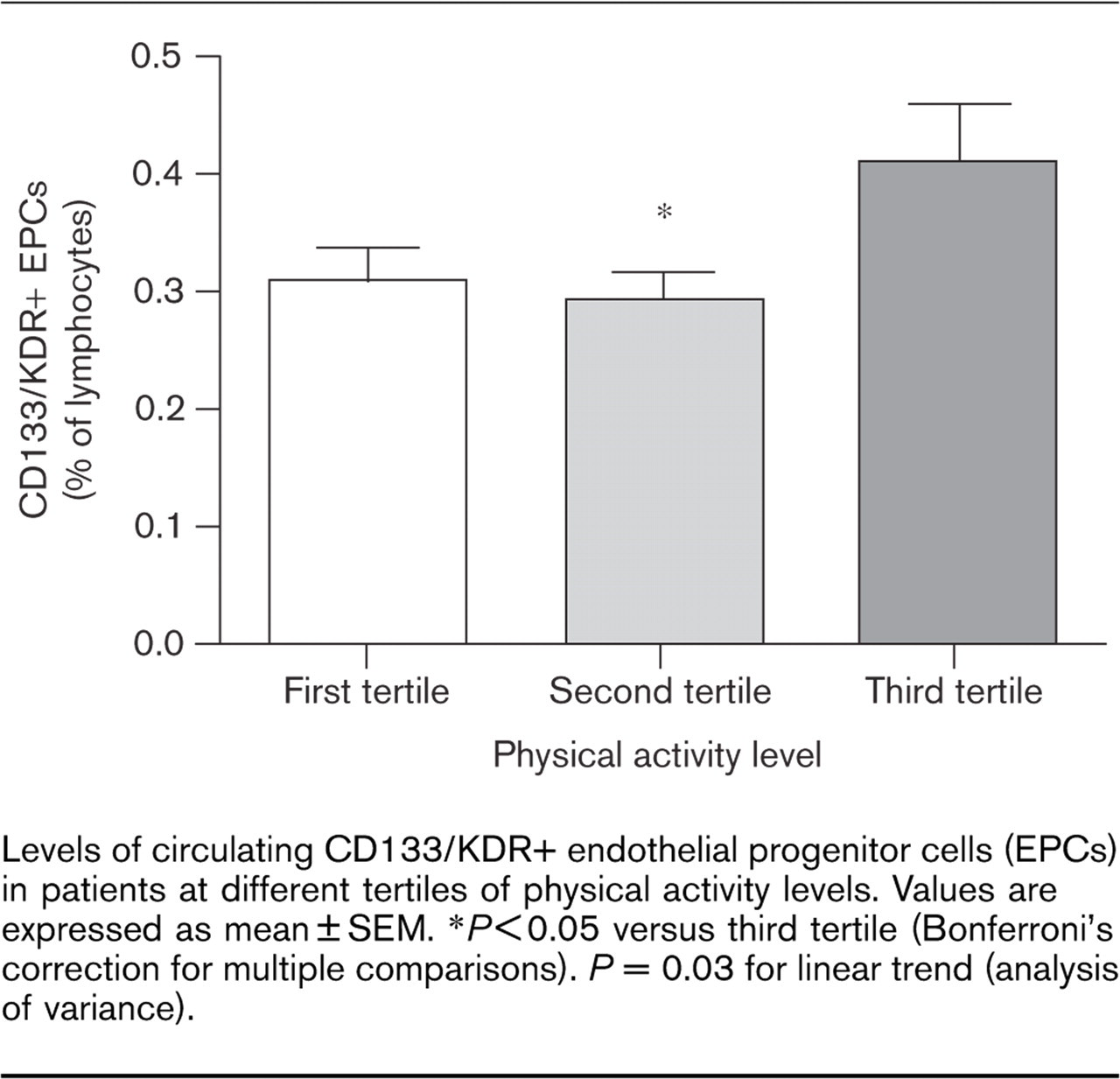
Levels of circulating CD133/KDR+ endothelial progenitor cells (EPCs) in patients at different tertiles of physical activity levels. Values are expressed as mean ± SEM. ∗P < 0.05 versus third tertile (Bonferroni's correction for multiple comparisons). P = 0.03 for linear trend (analysis of variance).
Unadjusted and adjusted effects of habitual PAL on FMD in univariate and multivariate linear regression analysis
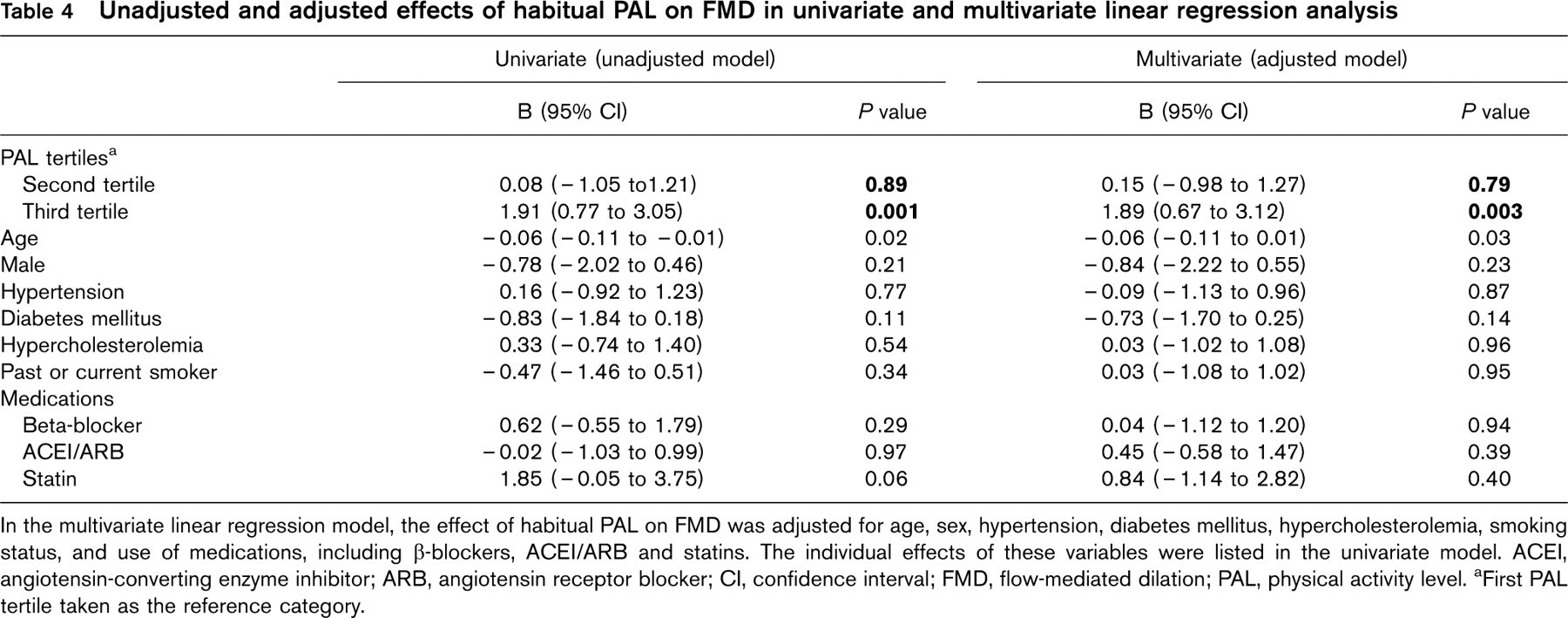
In the multivariate linear regression model, the effect of habitual PAL on FMD was adjusted for age, sex, hypertension, diabetes mellitus, hypercholesterolemia, smoking status, and use of medications, including β-blockers, ACEI/ARB and statins. The individual effects of these variables were listed in the univariate model. ACEI, angiotensin-converting enzyme inhibitor; ARB, angiotensin receptor blocker; CI, confidence interval; FMD, flow-mediated dilation; PAL, physical activity level. aFirst PAL tertile taken as the reference category.
Unadjusted and adjusted effects of CD34/KDR+ EPCs and CD133/KDR+ EPCs on FMD using linear regression

CI, confidence interval; EPC, endothelial progenitor cell; FMD, flow-mediated dilation. aThe effect of CD34/KDR+ EPCs on FMD was analyzed by linear regression analysis, adjusting for age, sex, hypertension, diabetes mellitus, hypercholesterolemia, smoking status, and use of medications, including β-blocker, angiotensin-converting enzyme inhibitor/angiotensin receptor blocker, and statins. Similarly, the effect of CD133/KDR+ EPCs was analyzed adjusting for the above variables.
Unadjusted and adjusted effects of habitual PAL on CD133/KDR+ EPC count in univariate and multivariate linear regression analysis
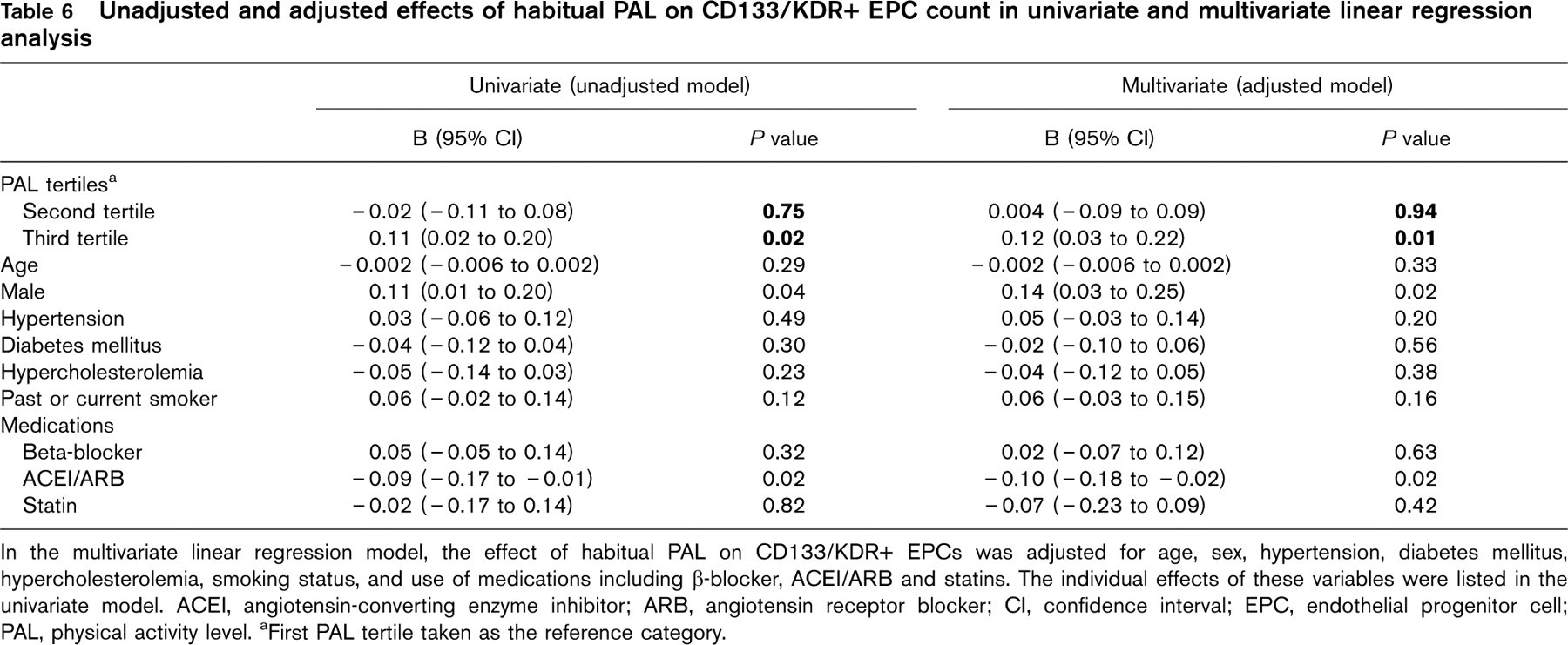
In the multivariate linear regression model, the effect of habitual PAL on CD133/KDR+ EPCs was adjusted for age, sex, hypertension, diabetes mellitus, hypercholesterolemia, smoking status, and use of medications including β-blocker, ACEI/ARB and statins. The individual effects of these variables were listed in the univariate model. ACEI, angiotensin-converting enzyme inhibitor; ARB, angiotensin receptor blocker; CI, confidence interval; EPC, endothelial progenitor cell; PAL, physical activity level. aFirst PAL tertile taken as the reference category.
Furthermore, the effects of CD34/KDR+ EPCs and CD133/KDR+ EPCs on FMD were studied using multivariate linear regression analysis, with adjustment for the factors that are known to affect FMD as listed above (Table 5). However, the two populations of EPCs did not correlate with FMD in the adjusted models, respectively (adjusted P > 0.05). Subsequently, the effect of habitual PAL on CD133/KDR+ EPC count was analyzed using multivariate linear regression correcting for confounding factors (Table 6). The second compared with the first PAL tertile was associated with an absolute increase of 0.004% in CD133/KDR+ EPC count (adjusted P > 0.05) but it was statistically insignificant; whereas the third compared with the first PAL tertile accounted for a significant absolute increase of 0.12%, or a relative increase of 44% (adjusted P = 0.01), in circulating CD133/KDR+ EPCs. Nevertheless, the amount of vigorous or moderate physical activity alone was not predictive of changes in EPC count (all P > 0.05).
Effect of habitual physical activity on blood pressure, lipids, lipoproteins, and inflammation
The effects of habitual physical activity on blood pressure, lipids, lipoproteins, and hsCRP level were examined using linear regression analysis (Table 7). Adjusting for age and sex, hsCRP did not change with tertiles of physical activity (P = 0.15). However, there was a significant trend for lower diastolic (P = 0.05) but not systolic blood pressure (P = 0.39) with higher tertiles of physical activity after adjusting for age, sex, and antihypertensive use. Nevertheless, serum triglyceride level, total cholesterol, HDL-C and LDL-C levels, and apolipoprotein A-I, apolipoprotein B and lipoprotein (a) levels did not change with increasing tertiles of physical activity, after adjusting for age, sex, and statin use (P > 0.05 for all).
Unadjusted and adjusted effects of habitual PAL on blood pressure, lipids, lipoproteins, and hsCRP
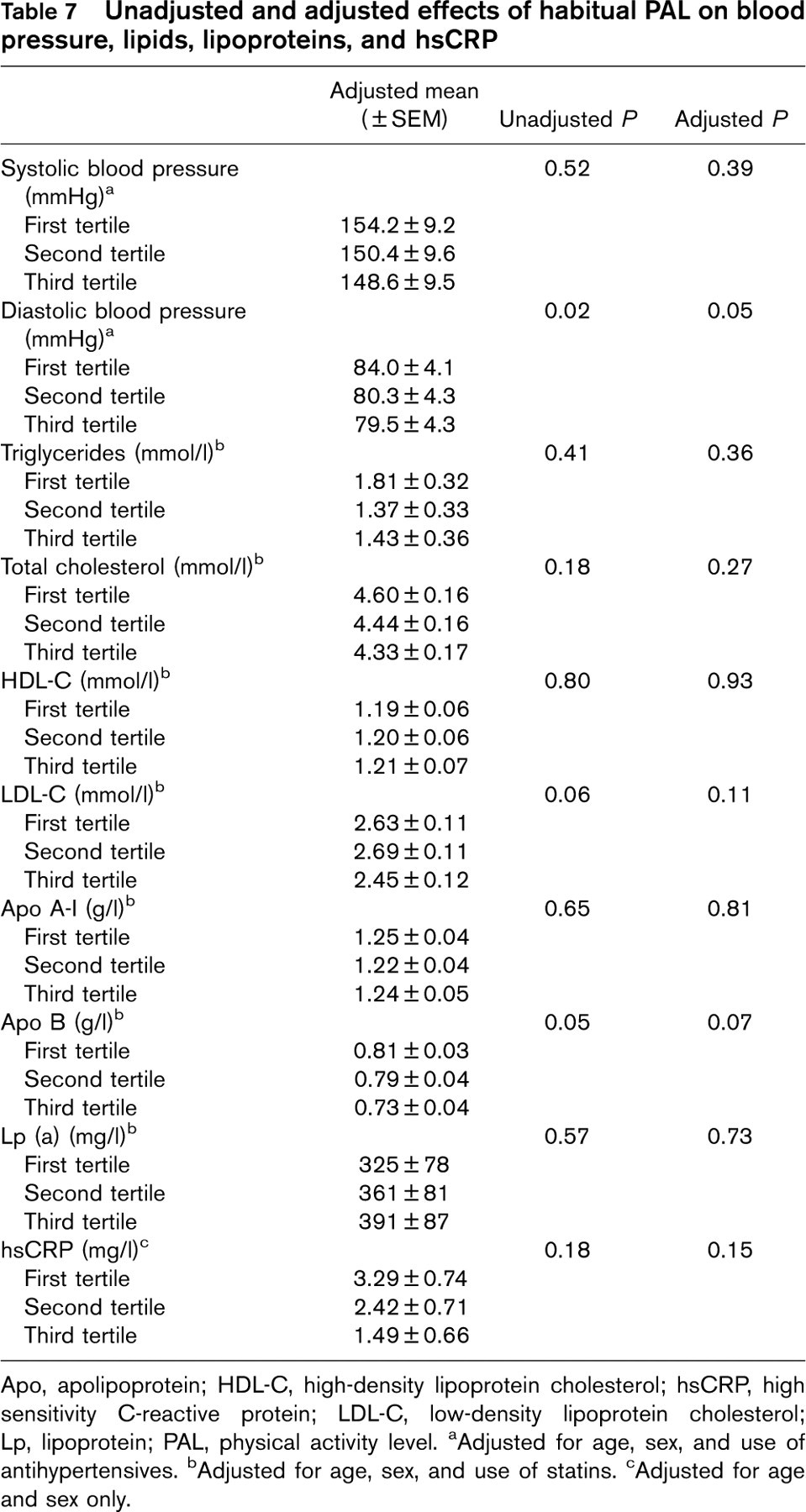
Apo, apolipoprotein; HDL-C, high-density lipoprotein cholesterol; hsCRP, high sensitivity C-reactive protein; LDL-C, low-density lipoprotein cholesterol; Lp, lipoprotein; PAL, physical activity level. aAdjusted for age, sex, and use of antihypertensives. bAdjusted for age, sex, and use of statins. cAdjusted for age and sex only.
Discussion
In patients with CAD, impaired endothelial function and depletion of EPCs are both independent predictors of future cardiovascular events [3, 11]. Although supervised exercise training programs have been proven to exert a beneficial effect on FMD [5–9] and EPC count [13–15] in patients with CAD, there are very limited data on the impact of habitual PAL on these cardiovascular prognostic markers. This study showed that higher habitual physical activity in patients with stable CAD was also associated with higher FMD and EPC count.
The mechanistic pathways through which regular exercise improves endothelial function have been described. Nitric oxide (NO) is probably the most important vasodilator produced by endothelial cells, through endothelial NO synthase. Reduced bioavailability of NO has been implicated in cardiovascular diseases [22]. In CAD patients, it has been shown that exercise exerts shear stress on the vascular wall, and induces Akt-dependent endothelial NO synthase phosphorylation, resulting in augmented NO synthesis [23].
Recent studies have also suggested that the depletion of circulating EPCs may also be implicated in the mechanisms of endothelial dysfunction [10]. Cardiovascular risk factors inflict continuous injury to the endothelial cell, causing endothelial dysfunction, and EPCs are mobilized from the bone marrow and home to the site of injury, contributing to vascular repair by regeneration of damaged endothelium [10, 24]. Physical training increased EPC numbers and migratory activity [13–15], which may be mediated through upregulation of NO and vascular endothelial growth factor as well as a reduction in EPC apoptosis [10, 25, 26]. Recent studies have shown that the increase in EPC count by exercise training correlated with the improvement in FMD [15]. Nevertheless, our findings showed that FMD only significantly correlated with increased PAL but not EPC count in multivariate linear regression. This suggests that higher habitual PAL may improve endothelial function through mechanisms other than increasing the EPC count.
In this study, EPCs are identified by the coexpression of surface markers such as CD34, CD133, and KDR. Both CD133 and CD34 are hematopoietic stem cell markers, but CD133 is no longer present as the EPC matures, whereas CD34 is still expressed on mature endothelial cells at a lower level, such that CD133/KDR+ and CD34/KDR+ cells may reflect immature and mature EPCs, respectively [24]. The result of this study showed that higher habitual physical activity increased CD133/KDR+ but not CD34/KDR+ EPCs. Recent studies suggested that different subpopulations of EPCs might confer different properties [27]. It is possible that higher habitual physical activity enhances the mobilization of the more immature, angioblast-like CD133/KDR+ EPCs, which might have a more prominent effect on angiogenesis than endothelial repair compared with mature CD34/KDR+ EPCs. Indeed, recent studies have shown that coronary endothelial function is more correlated with CD34/KDR+ EPC than CD133/KDR+ EPC [28]. This might account for the lack of relationship between FMD and CD133/KDR+ EPC in this study.
Exercise training has been shown to improve blood lipid profile [29], reduce blood pressure [30], and systemic inflammation [31]. Therefore, the effect of habitual physical activity on blood pressure, lipids, lipoproteins, and inflammation were also investigated in this study. Our results showed that increasing tertiles of PAL was associated with a significant reduction of diastolic blood pressure, after adjusting for age, sex, and antihypertensive use. However, there were no changes in other variables such as systolic blood pressure, total, HDL-C and LDL-C, and hsCRP. Nevertheless, there were no significant relationships between diastolic blood pressure with FMD and EPC count (P = 0.11 and P = 0.12 respectively, data not shown). These findings suggest that increased habitual physical activity did not alter the lipid profile nor attenuate inflammation, and at the same time it improved FMD and EPC levels independent of its antihypertensive effect.
In this study, both FMD and EPC count showed similar increasing trends with higher tertiles of PAL. However, significant differences in FMD and EPC count were only observed in the highest tertile of physical activity, suggesting a possible threshold level of habitual physical activity for its vascular protective effects. The participants who attained a significant improvement in FMD and EPC levels were engaged in a mean PAL of 2752 METs min/week. This threshold level could be translated into 2 h of daily walking exercise, or 1.5 h of moderate exercise such as bicycling or carrying light loads, or 50 min of vigorous activity per day. It is also worthwhile to point out that only the total volume of habitual physical activity was related to the difference in FMD and EPC levels, but the amount of vigorous physical activity alone was not predictive of changes in FMD and EPC count. Similarly, the amounts of moderate activity or walking exercise also did not determine such parameters, indicating that higher habitual physical activity modulates FMD and EPC count independent of exercise intensity.
As endothelial dysfunction is an independent predictor for future cardiovascular events, a higher habitual PAL in these high-risk patient populations may have a beneficial effect in reducing cardiovascular morbidity and mortality.
Study limitations
First, the functional and proliferative activities of EPC were not determined in this study. Therefore, it is unknown whether the PAL can affect endothelial function by improving EPC function. Second, a direct causality of the PAL and endothelial function cannot be established in this cross-sectional study. Future randomized controlled studies will be needed to confirm these potential beneficial effects of increased habitual PAL on the endothelial function in high-risk CAD patients.
Footnotes
Acknowledgements
The authors thank Dr Duncan Macfarlane, Institute of Human Performance, University of Hong Kong, for the use of the Chinese version of IPAQ in this study. This study was supported by the CRCG Small Project Funding of University of Hong Kong (Project No. 200507176137), and Sun Chieh Yeh Heart Foundation.