
Abstract
Objective
Examine the relation between IQ in early adulthood and later coronary heart disease (CHD) mortality, and assess the extent to which established risk factors measured in middle-age might explain this gradient.
Design
Cohort study of 4316 male former Vietnam-era US army personnel with IQ scores (mean age 20.4 years), risk factor data (mean age 38.3 years) and 15 years mortality surveillance.
Results
In age-adjusted analyses, lower IQ scores were associated with an increased rate of CHD mortality (hazard ratio per SD decrease in IO; 95% confidence interval: 1.34; 1.00, 1.79). Adjustment for later chronic disease (1.22; 0.91, 1.64), behavioural (1.29; 0.95, 1.74) and physiological risk factors (1.19; 0.88, 1.62) led to some attenuation of this gradient. This attenuation was particularly pronounced on adding socioeconomic indices to the multivariable model when the IQ–CHD relation was eliminated (1.05; 0.73, 1.52). A similar pattern of association was apparent when cardiovascular disease was the outcome of interest.
Conclusion
High IQ may lead to educational success, well remunerated and higher prestige employment, and this pathway may confer cardio-protection.
Introduction
Lower IQ test results from early in life when such scores are likely to be premorbid are associated with an elevated risk of all-cause mortality in populations followed for up to six decades [1]. Studies relating early IQ with cause-specific mortality, such as coronary heart disease (CHD), are scarce. Although these few studies have generally found an inverse gradient for IQ in relation to CHD [2–6], the role of potential mediating risk factors (e.g. smoking, inactivity, raised blood pressure, lung function, obesity, psychiatric and somatic illness, socioeconomic disadvantage) has not been examined thoroughly. With the exception of a solitary study [3], either such intermediary risk factors were not available in studies of IQ and CHD [2,4], or were measured simultaneously with IQ and therefore do not temporally lie between IQ and CHD assessments [5,6] and cannot, therefore, be considered as genuine mediating variables. The Vietnam Experience Study [7] is rare in providing early life IQ scores and subsequent assessments of both these potential mediating factors and CHD outcomes. To our knowledge, the range of potential mediating variables in this study is unprecedented in those examining the IQ–CHD link.
Design and methods
The Vietnam Experience Study has been described in detail elsewhere [7–9]. In brief, 18313 former US army personnel – entering the service in the Vietnam era between 1965 and 1971– qualified for inclusion in the study cohort. Data on IQ (assessed using the validated Army General Technical Test), service income and ethnicity were retrospectively extracted from service records for a period when the men were around 20 years of age. At around 38 years of age (in 1985/1986), the men participated in a telephonic survey. A random sample (N = 4462) of the original cohort then attended a medical examination during which a range of physiological, behavioural, psychological and socioeconomic risk data were collected using standard protocols [7]. Among the data collected were resting heart rate and adult height, which, although under a certain degree of genetic control, are regarded as markers of physical activity [10] and early life socioeconomic circumstances [11], respectively. On completion of these surveys, study participants were followed for mortality experience for 15 years. After testing that the proportional hazards assumption had not been violated, hazards ratios with accompanying 95% confidence intervals were computed for the relation between IQ and CHD using Cox regression analysis [12]. In these analyses, we grouped collateral variables into potential confounding and mediating factors, with the latter category subdivided into chronic disease (psychiatric and somatic), physiological, behavioural and socioeconomic. CHD mortality was coded according to version 9 (410–414; 429.2) or 10 (120–125) of the International Classification of Disease (ICD) manuals.
Results
Fifteen years of follow-up of 4316 men gave rise to 43 deaths from CHD. In age-adjusted analyses (Table 1), IQ was inversely related to CHD mortality (hazard ratio per one SD decrease in IQ = 1.34; 1.00, 1.79), although confidence intervals included unity. Adjustment for potential confounding variables (age, army rank, height and ethnicity) attenuated this relation (1.23; 0.89, 1.71). Next, we controlled for potential mediating variables. Controlling for health behaviours (1.29; 0.95, 1.74) had a modest impact on this relation, whereas adjustment for indicators of all measured chronic diseases (1.22; 0.91, 1.64) (particularly psychiatric) and physiological risk factors (1.19; 0.88, 1.62) had a more marked effect. The greatest attenuation of the IQ–CHD association, however, was seen when socioeconomic factors were added to the multi-variable model when any suggestion of a gradient was lost (1.05; 0.73, 1.52). In analyses where cardiovascular disease was the outcome of interest (63 deaths) – ICD codes 390–434 and 436–459 (version 9) and 100–199 (version 10) – the pattern of association was very similar.
Hazard ratios (95% CI) for the relation of IQ with coronary heart disease mortality in the VES (N = 4316)
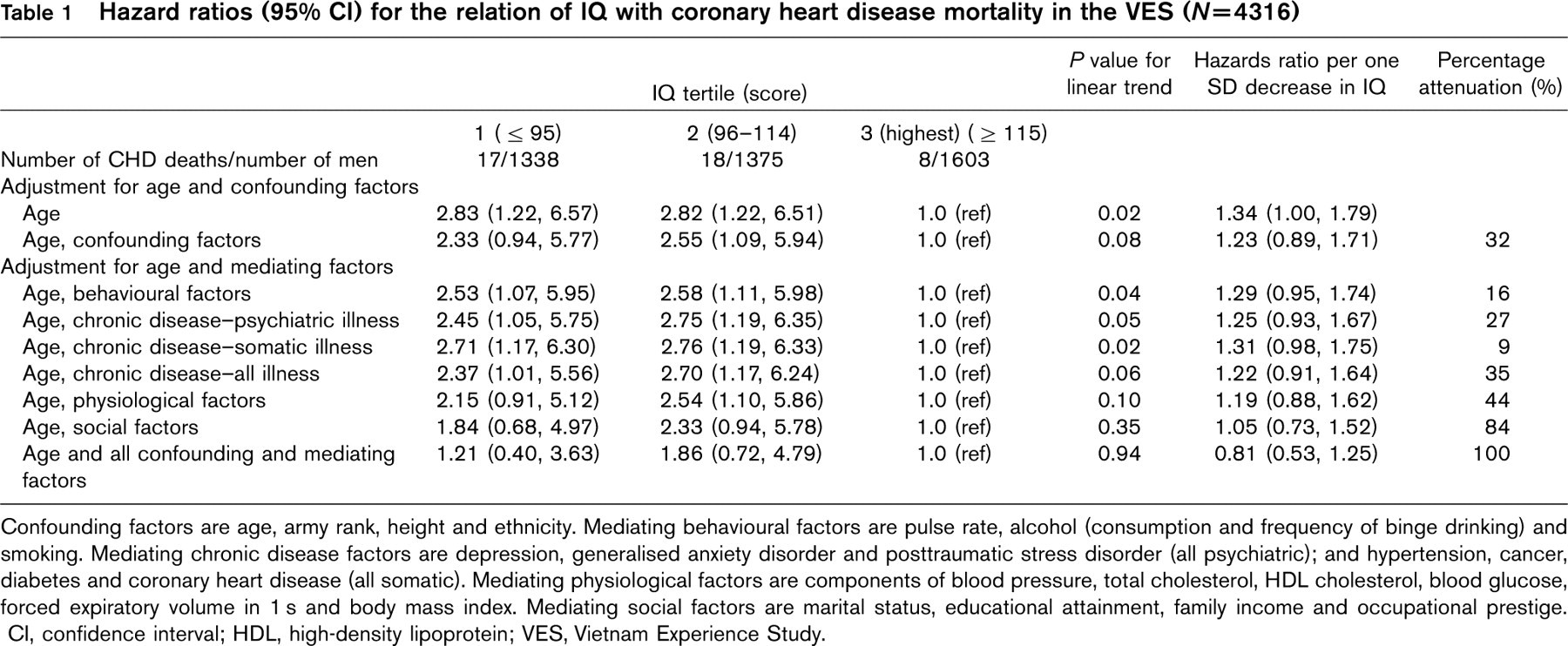
Confounding factors are age, army rank, height and ethnicity. Mediating behavioural factors are pulse rate, alcohol (consumption and frequency of binge drinking) and smoking. Mediating chronic disease factors are depression, generalised anxiety disorder and posttraumatic stress disorder (all psychiatric); and hypertension, cancer, diabetes and coronary heart disease (all somatic). Mediating physiological factors are components of blood pressure, total cholesterol, HDL cholesterol, blood glucose, forced expiratory volume in 1 s and body mass index. Mediating social factors are marital status, educational attainment, family income and occupational prestige. CI, confidence interval; HDL, high-density lipoprotein; VES, Vietnam Experience Study.
Discussion
The main finding of this study was that controlling for a range of social, behavioural, chronic disease and physiological variables markedly attenuated the relation between IQ in late adolescence/early adulthood and future CHD risk. That adjusting for markers of socioeconomic position in adult life – education, income, occupational prestige – led to the greatest reduction in the strength of the IQ-CHD gradient points to a possible causal pathway: high IQ leads to educational success and on to well remunerated, higher prestige employment, and it is the latter which offers protection against CHD. Although this may be the case, the role of early IQ may still be crucial as an early life predictor of later CHD.
In those studies in which risk factor data are collected simultaneously with IQ [5,6], the IQ-CHD relation survives such an adjustment. The so-called mediating variables, however, may not be regarded as actually lying on the causal pathway in these studies. In two cohorts – the Scottish Mental Survey 1932-Midspan studies linkage and this study – in which measurement of risk factor variables proceeds that of the IQ assessment but precedes CHD occurrence, the IQ-CHD gradient was essentially eliminated. More such studies, particularly those with a greater number of CHD events so producing increased statistical power, are required to further investigate potential mechanisms.
The present data are compatible with at least three hypotheses about the association between early life IQ and CHD: that the effect of IQ is mediated especially via socioeconomic factors in adulthood; that socioeconomic variables eliminate the IQ-CHD association because they act together as a proxy measure of IQ; or that some other variable or set of variables, underlying IQ and socioeconomic factors, is a risk factor for CHD.
Footnotes
Acknowledgements
Mortality surveillance of the cohort members was funded by the National Center for Environmental Health in Atlanta, United States of America. David Batty is a UK Wellcome Trust Fellow. Martin Shipley is supported by The British Heart Foundation and Laust Mortensen by The National Institute of Public Health, Denmark. Ian Deary is the recipient of a Royal Society-Wolfson Research Merit Award.