
Abstract
The diagnostic workup in patients with ischaemic stroke often includes testing for prothrombotic conditions. However, the clinical relevance of coagulation abnormalities in ischaemic stroke is uncertain. Therefore, we reviewed what is presently known about the association between inherited and acquired coagulation disorders and ischaemic stroke, with a special emphasis on the methodological aspects. Good-quality data in this field are scarce, and most studies fall short on epidemiological criteria for causal inference. While inherited coagulation disorders are recognised risk factors for venous thrombosis, there is no substantial evidence for an association with arterial ischaemic stroke. Possible exceptions are the prothrombin G20210A mutation in adults and protein C deficiency in children. There is proof of an association between the antiphospholipid syndrome and ischaemic stroke, but the clinical significance of isolated mildly elevated antiphospholipid antibody titres is unclear. Evidence also suggests significant associations of increased homocysteine and fibrinogen concentrations with ischaemic stroke, but whether these associations are causal is still debated. Data on other acquired coagulation abnormalities are insufficient to allow conclusions regarding causality. For most coagulation disorders, a causal relation with ischaemic stroke has not been definitely established. Hence, at present, there is no valid indication for testing all patients with ischaemic stroke for these conditions. Large prospective population-based studies allowing the evaluation of interactive and subgroup effects are required to appreciate the role of coagulation disorders in the pathophysiology of arterial ischaemic stroke and to guide the management of individual patients.
Introduction
Stroke is an important cause of death and disability in Western societies (1 2). In about 40% of all ischaemic strokes, no definite cause can be identified, despite extensive ancillary investigations (3). The diagnostic workup in patients with ischaemic stroke often includes testing for thrombophilic conditions. However, the clinical significance of inherited or acquired coagulation abnormalities found in ischaemic stroke patients is uncertain (4–6). For many of the coagulation disorders, a causal relation with arterial ischaemic stroke has not been definitely established, and it is still argued whether and how these conditions should be treated to prevent (recurrent) stroke. In this article, we will review what is presently known about the association between coagulation disorders and arterial ischaemic stroke, with a special emphasis on the methodological quality of the available evidence, and discuss the usefulness of laboratory testing for prothrombotic conditions in ischaemic stroke patients.
Methodological considerations
Several points are of importance when assessing the strength of the evidence in favour of a true causal relation between a certain coagulation abnormality and ischaemic stroke. Evidently, the supposed association should be biologically plausible. Furthermore, a causal link is more likely when the data suggest a dose–response relationship, i.e. an increasing probability of stroke with increasing severity of the potential risk factor. In genetic studies, additional proof of causality may emerge from relating gene variations to the levels or function of the gene product. Other key issues in interpreting and weighing results from the literature are the design and the size of the study. The research in this field largely consists of case–control studies, which are prone to several methodological pitfalls such as reversed causality and inappropriate selection of controls. Most of the available data have been obtained in relatively small studies that are probably underpowered to detect modest effects. Limited statistical power due to low numbers in individual studies can be partly overcome by meta-analyses. Still, negative results have a lower probability of appearing in print than statistically significant associations, leading to a publication bias. Unfortunately, the majority of the studies on coagulation disorders and ischaemic stroke are inadequate with respect to many of the above-mentioned points, thus hampering causal inference.
Inherited coagulation disorders
Inherited prothrombotic coagulation disorders are caused by mutations in genes encoding for factors involved in the coagulation cascade, in particular, anticoagulant proteins and coagulation factors. Most of these hereditary prothrombotic conditions were consistently found to be associated with an increased risk of venous thrombotic and thromboembolic events. Yet, for arterial thrombosis including ischaemic stroke, the findings have been far less consistent and a causal association is still disputed.
Protein C deficiency
Protein C is a vitamin-K-dependent protein, which circulates in the blood in an inactive form. Activated protein C (APC) inhibits clot formation by proteolytic degradation of activated coagulation factors V and VIII (7). Inherited deficiency of protein C, which is estimated to occur in 0.2–0.5% of the general population, results in a hypercoagulable state and is associated with an increased risk of venous thrombotic events (8). Many different mutations have been identified in the gene encoding for protein C, resulting in several types of protein C deficiency. Most patients have a heterozygous protein C deficiency, with a protein C level of around 50% of normal. A limited number of studies have investigated protein C levels or protein C deficiency in relation to ischaemic stroke. A few case reports and smaller case–control studies have suggested an association between protein C deficiency and ischaemic stroke (9 10), but in a larger case–control study, no significant association was observed (5). In the prospective ARIC study, lower levels of protein C seemed to be related to an increased risk of incident ischaemic stroke, but the results were not statistically significant (Table 1) (11). It is noteworthy that only single measurements of protein C antigen concentration were analysed and that the levels were truly deficient in just a few participants in this cohort. In the same study, baseline protein C was also associated with cerebral infarcts on MRI at follow-up, although baseline MRIs were not available (12). Most other studies on protein C deficiency and ischaemic stroke involve paediatric patients. A prospective study among 301 children with a first ischaemic stroke showed a significantly increased risk of recurrent ischaemic stroke in children with hereditary protein C deficiency (13). A meta-analysis of 11 case–control studies also reported a significant association between protein C deficiency and first arterial ischaemic stroke in children (14).
Published meta-analyses and prospective studies (cohort studies or nested case–control studies) on the relation between hereditary coagulation disorders and ischaemic stroke
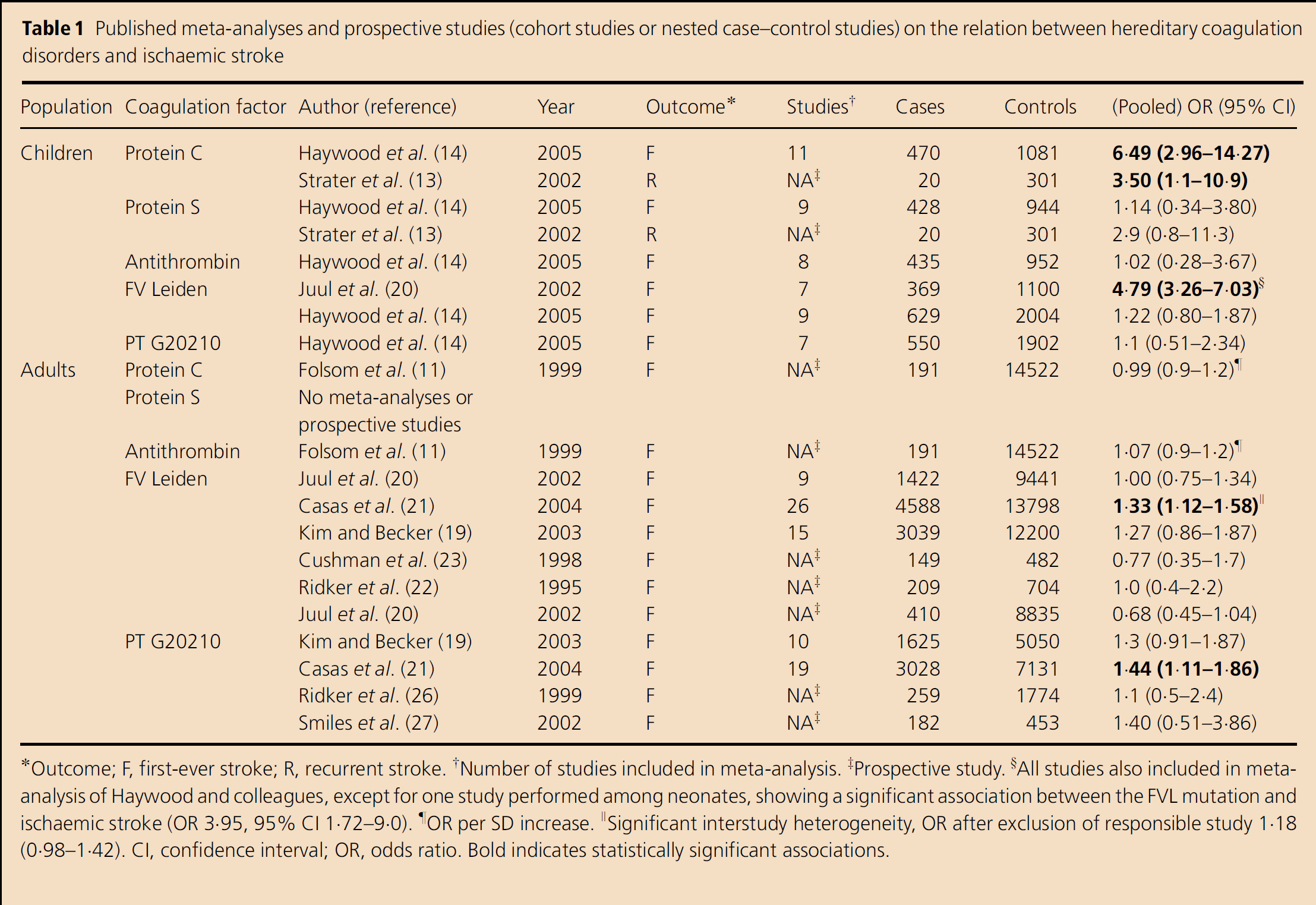
Outcome; F, first-ever stroke; R, recurrent stroke
Number of studies included in meta-analysis
Prospective study
All studies also included in meta-analysis of Haywood and colleagues, except for one study performed among neonates, showing a significant association between the FVL mutation and ischaemic stroke (OR 3·95, 95% CI 1·72–9·0)
OR per SD increase
Significant interstudy heterogeneity, OR after exclusion of responsible study 1·18 (0·98–1·42)
CI, confidence interval; OR, odds ratio. Bold indicates statistically significant associations.
Protein S deficiency
Protein S, another vitamin-K-dependent protein, is a co-factor in the process of the proteolytic inactivation of factor Va and VIIIa by APC, and thus exerts an inhibiting effect in the coagulation cascade (8). Several mutations have been described that cause hereditary protein S deficiency. A few cases with homozygous or compound heterozygous protein S deficiency have been reported, displaying a severe form of thrombosis at a young age. Heterozygous protein S deficiency is more frequent and has been linked to an elevated risk of venous thromboembolic events in many studies (8 15).
The relationship between protein S deficiency and the risk of ischaemic stroke in adults has hardly been investigated systematically (Table 1). Published reports include small studies, case reports or patient series without controls (8 16 17). Prospective studies have not been performed. One relatively large case–control study did not demonstrate a significant association between protein S deficiency and the risk of ischaemic stroke (5). In their meta-analysis of nine case–control studies, Haywood et al. (14) did not find a significant association in children either.
Antithrombin deficiency
Antithrombin is a serine protease inhibitor that inactivates thrombin, as well as other coagulation enzymes, including activated factors X, IX, XI and XII (8). It thus functions as a natural anticoagulant. Several mutations in the antithrombin gene have been identified that can cause antithrombin deficiency. The inheritance pattern is usually autosomal dominant. The deficiency of antithrombin results in a hypercoagulable state and is associated with an increased risk of venous thromboembolism (8). As yet, no substantial evidence has been obtained for an association between antithrombin deficiency and the risk of arterial ischaemic events, including stroke (Table 1). A large case–control study (5) and one prospective study (11) both failed to demonstrate an association with ischaemic stroke of hereditary antithrombin deficiency and antithrombin levels, respectively. Studies performed in paediatric patients were also negative; a meta-analysis of eight case–control studies did not show an association between antithrombin deficiency and the risk of incident ischaemic stroke in children (14).
Factor V Leiden (FVL) mutation
The FVL mutation is a common mutation (1691 G>A) in the gene coding for coagulation factor V, resulting in factor Va being resistant to degradation by APC (18). Activated protein C resistance, either due to the FVL mutation or caused by other genetic or acquired factors, is the most frequently known independent risk factor for venous thrombosis. The risk of venous thrombosis is estimated to be increased by a factor 5–7 in heterozygous carriers and a factor 50–100 in homozygous carriers (7). It is debated whether the FVL mutation is also associated with the occurrence of arterial thrombosis. No significant association between the FVL mutation and the risk of ischaemic stroke in adults was found in two meta-analyses of nine and 15 case–control studies, respectively (Table 1) (19 20). A third meta-analysis including 26 case–control studies on the FVL mutation demonstrated an association with ischaemic stroke, but the result was no longer statistically significant after one study was excluded, which caused a significant interstudy heterogeneity (21). In a nested case–control study within the prospective Physicians’ Health Study as well as in the large prospective Cardiovascular Health Study, there was no association between the FVL mutation and the occurrence of stroke (22 23). Some, but not all studies performed in children suggest that the FVL mutation might be a risk factor for ischaemic stroke in this subgroup (14 24).
Prothrombin G20210A mutation
The G20210A mutation in the 3’ untranslated region of the prothrombin gene results in elevated plasma levels of prothrombin (factor II), the precursor of thrombin. Persons carrying this mutation, in particular homozygous individuals, were found to have an up to threefold increased risk of venous thrombosis (25). The relation between the prothrombin G20210A mutation and the risk of ischaemic stroke has been evaluated prospectively in two large population studies. In the Physicians’ Health Study as well as the Cardiovascular Health Study, no significant association was observed between the presence of the prothrombin mutation and the occurrence of ischaemic stroke (Table 1) (26 27). Of the retrospective case–control studies that have been published, a significant association was seen in only two, whereas the majority did not demonstrate a relationship (4). However, while in a meta-analysis of 10 studies, the summary estimate was not statistically significant (19), a larger meta-analysis of 19 case–control studies showed a modest but statistically significant association (21).
Protein Z
Protein Z is a vitamin-K-dependent glycoprotein that functions as a cofactor in the inhibition of activated coagulation factor X by a protein Z-dependent protease inhibitor (28). Pathophysiological studies suggest that protein Z may exert anticoagulant as well as procoagulant effects (29 30). The results of several case–control studies did not support the theory of a link between protein Z levels and venous thrombosis (28). A number of case–control studies examined the association between protein Z levels and arterial stroke, with quite contradictory findings. In some studies, low plasma levels of protein Z were associated with an increased risk of ischaemic stroke (30 31), while other groups found an increased risk of stroke with elevated protein Z levels (32–34), or no relation at all (35). In the large prospective ARIC study, there was no statistically significant association between protein Z levels and stroke (36). Two polymorphisms (G79A and G103A) of the gene encoding for protein Z have been evaluated in relation to the occurrence of arterial stroke in a few case–control studies, but the results were not consistent (30 34 37).
Acquired coagulation disorders
A number of acquired conditions are also associated with a hypercoagulable state. Some of these disorders seem to be linked to an increased risk of both venous and arterial thrombosis, although the evidence for a causal relation is uncertain.
Antiphospholipid antibodies
Antiphospholipid antibodies are acquired autoantibodies directed against phospholipids or phospholipid–protein complexes (38). The antiphospholipid syndrome (APS) is a systemic autoimmune disorder characterised by elevated levels of antiphospholipid antibodies in combination with at least one clinical episode of arterial, venous or small-vessel thrombosis in any tissue or organ, or pregnancy morbidity (unexplained foetal death, premature birth due to (pre)-eclampsia or placental insufficiency or repeated unexplained spontaneous abortions). According to the updated international consensus criteria, laboratory findings should be present on two or more occasions at least 12-weeks apart (39). The prothrombotic state in APS that is associated with an increased risk of recurrent venous and arterial thromboembolic events is still debated, but is thought to be mainly caused by the activation of endothelial cells and platelets by antiphospholipid antibodies (38). Moderately and often transiently elevated titres of antiphospholipid antibodies can also be found in patients with infections or certain medication. The clinical significance of antiphospholipid antibodies in the absence of other criteria for APS is unclear. Furthermore, studies are hampered by the considerable degree of heterogeneity of available laboratory tests to detect antiphospholipid antibodies and the ongoing debate on the serological criteria of APS (40 41). Although in many case–control studies a relation between antiphospholipid antibodies and an increased risk of ischaemic stroke was found (42–44), others did not demonstrate such an association (45 46). Prospective studies have yielded inconsistent results as well (47–50). In the largest prospective study, elevated titres of anticardiolipin antibodies were significantly associated with future ischaemic stroke, but only in women (50). A prospective study on recurrent stroke found no association between the presence of antiphospholipid antibodies at the time of the initial stroke and the risk of subsequent thrombo-occlusive events (49). Several studies have suggested that the presence of antiphospholipid antibodies is associated with ischaemic stroke specifically in the subgroup of young adults (51).
Coagulation disorders associated with cancer
Several publications have suggested that stroke occurs more frequently in patients with malignant disease as compared with the general population (52–54), although others could not replicate this observation (55). A variety of mechanisms might underlie the potentially higher incidence of stroke in cancer patients, including direct tumour effects (tumour embolism, vessel compression), therapy-related factors (surgery, radiotherapy-induced vasculopathy, hormonal therapy) and coagulation disorders. Malignant disease may induce a low-grade systemic activation of coagulation, which is related to an increased risk of venous thromboembolic events (56 57). Findings from several studies also suggest an association between cancer-related coagulation disorders and arterial ischaemic stroke. In an autopsy study of 3426 patients who died of systemic cancer, evidence of a hypercoagulable state was found in over half of the patients with symptomatic stroke (53). A smaller retrospective case–control study comparing ischaemic stroke patients with and without cancer showed a trend towards more thrombotic events in patients with malignant disease (58). In another retrospective study, coagulation abnormalities were present in a considerable proportion of patients in whom ischaemic stroke was the first manifestation of an underlying malignancy (59). However, without any results from large prospective series, there is no definite proof of an elevated risk of arterial ischaemic stroke related to coagulation abnormalities in malignancies.
Hyperhomocysteinaemia
Homocysteine is a nonessential amino acid that is metabolised by two major pathways: remethylation to methionine, requiring folate and vitamin B12, and transsulphuration to cystathionine, with vitamin B6 as a cofactor. In the 1960s, several patients were reported with extremely high plasma levels of homocysteine who developed venous and arterial thrombosis at very young ages. These children displayed evidence of premature atherosclerosis as well as characteristics of a hypercoagulable state. The strongly increased levels of homocysteine (>100 μmol/l) were later found to be caused by a number of rare inborn errors of homocysteine metabolism (60 61). As opposed to these uncommon genetically determined forms of hyperhomocysteinaemia, a mildly elevated homocysteine concentration (>15 μmol/l) is more frequent and is often due to the dietary deficiency of B-vitamins, older age or renal failure (62). Evidence from the last two decades suggests that mild hyperhomocysteinaemia is also associated with an increased risk of venous and arterial thrombotic disease. Numerous epidemiological studies have shown a positive association between homocysteine concentration and the risk of cardiovascular disease, including stroke. A meta-analysis of 12 prospective and 18 retrospective studies showed that a 25% lower total homocysteine concentration was associated with a significantly lower risk of stroke, after adjustment for cardiovascular risk factors (63). Another meta-analysis, based on eight prospective studies, also demonstrated a statistically significant relation between elevated homocysteine levels and the risk of stroke. Furthermore, the same authors reported an increased risk of stroke associated with the MTHFR 677TT genotype, which causes a mild hyperhomocysteinaemia (64). Supplementation with folate, vitamin B12 and vitamin B6 has been shown to reduce homocysteine concentrations (65). Yet, several large randomised trials have failed to demonstrate an effect of vitamin supplementation on the risk of cardiovascular disease or atherosclerosis, despite successful lowering of homocysteine (66–69). Disappointing trial results initially raised the question as to whether hyperhomocysteinaemia is truly causally related to cardiovascular risk or rather an epiphenomenon or a marker of other pathological processes such as deficiencies of B-vitamins (65 70) However, recent evidence indicates that there might be an effect of supplementation specifically on the risk of stroke. The results of the large HOPE-2 trial were negative for the primary composite study endpoint, but for stroke, a 24% risk reduction associated with vitamin supplementation was found (66). This fits the results from two meta-analyses of trials on vitamin supplementation, showing insufficient evidence for an effect on cardiovascular disease, but a borderline significant effect on stroke risk (71 72). Laboratory studies indicate that homocysteine has both atherogenic and thrombogenic properties (65), but the exact biological mechanisms that underlie the relation between elevated homocysteine concentration and ischaemic stroke are not well understood.
Disturbances of primary haemostasis
Von Willebrand factor (vWF) is a glycoprotein that plays an important role in primary haemostasis by stimulating platelet adhesion and aggregation. It has been suggested that high vWF levels may have a pathogenetic role in cardiovascular disease (73). In one case–control study, high levels of vWF antigen and activity were indeed associated with an increased risk of first-ever ischaemic stroke (74). The large vWF multimers are cleaved into smaller, less active forms by the metalloprotease ADAMTS13 (A Disintegrin And Metalloprotease with ThromboSpondinmotifs). A recent case–control study showed that lower plasma levels of ADAMTS13 were related to an increased risk of cardiovascular disease in young individuals (75). A complete deficiency of ADAMTS13 is seen in thrombotic thrombocytopaenic purpura (TTP), a thrombotic microangiopathy characterised by occlusive microvascular thrombosis, microangiopathic haemolytic anaemia, consumptive thrombocytopaenia and organ dysfunction. Insufficient processing of vWF multimers results in continuing vWF-dependent intravascular platelet aggregation, eventually causing microvascular thrombosis. Diffuse neurological symptoms such as behavioural changes, disturbed consciousness or convulsions are commonly seen in TTP, due to the occlusion of small vessels in the brain. These symptoms and associated radiological findings are usually transient (76). In a study of 48 patients diagnosed with TTP or haemolytic uraemic syndrome (HUS; another thrombotic microangiopathy), neurological abnormalities were found in 73% (77), a proportion similar to that in another small study of 16 TTP patients (76). Ischaemic stroke does not seem to be the main complication of thrombotic microangiopathies, as neurological complications were mostly suggestive of microvascular occlusive changes and focal deficits were only seen in a minority of these patients. A number of case reports have been published of ischaemic stroke or persisting focal lesions on MRI occurring in TTP or HUS (78–80), but systematic studies including a control group have not been carried out.
Several polymorphisms of genes encoding for platelet receptors have been evaluated in relation to ischaemic stroke occurrence, including the PlA1/A2 polymorphism of the platelet glycoprotein IIb/IIIa receptor, and variations in the purinergic receptor P2YG-protein-coupled 12 (P2RY12) gene, but thus far, no evidence has been observed for an association with ischaemic stroke (81–83).
Disorders of fibrin formation and fibrinolysis
Fibrinogen, the central protein in the coagulation cascade, is a soluble acute-phase protein that is converted into insoluble fibrin by thrombin. Fibrin is then cross-linked by coagulation factor XIIIa to form blood clots. High fibrinogen levels have consistently been associated with an increased risk of ischaemic stroke in prospective studies. A large meta-analysis of data from 31 population-based prospective studies confirmed the significant association between plasma fibrinogen and arterial ischaemic stroke (84). However, it is still unclear whether raised plasma fibrinogen contributes directly to the occurrence of ischaemic stroke or rather reflects general inflammation or severity of atherosclerosis, resulting in an increase of inflammatory markers (44 85). To further evaluate the nature of the association, studies of genetic variations as markers for fibrinogen levels have been performed, some of which indeed suggested a relation between various polymorphisms or haplotypes and the occurrence of ischaemic stroke (44 86).
The levels or the activity of coagulation factor XIII reportedly are influenced by genetic variation, but studies on the relation between several variants of the genes encoding for the A and B subunits of factor XIII and ischaemic stroke have been inconsistent (87–89).
Impaired fibrinolysis has also been suggested to be associated with arterial thrombosis, including ischaemic stroke (90). In a recent case–control study, increased clot lysis times, indicative of hypofibrinolysis, were found in patients with arterial thrombotic disease at a young age, with a trend towards elevated clot lysis times in the subgroup of patients with ischaemic stroke (91). Several case–control studies have demonstrated an association between plasma levels of thrombin-activatable fibrinolysis inhibitor (TAFI) and ischaemic stroke (92–94). One of these also revealed an association between the 325Thr/Ile polymorphism of the TAFI gene and arterial thrombosis. A recent meta-analysis including about 2500 cases and 3500 controls demonstrated strong evidence of an association with ischaemic stroke of the 4G/5G promoter polymorphism of the gene encoding for another inhibitor of fibrinolysis, plasminogen activator inhibitor-1 (PAI-1), with a large heterogeneity across studies (95). Unfortunately, almost all studies reported on genotype only, instead of genotype and levels simultaneously. In one case–control study evaluating both the 4G/5G polymorphism and the PAI-1 antigen levels, no association was found between PAI-1 levels and first ischaemic stroke (96).
Interactive effects
Arterial thrombosis including ischaemic stroke is increasingly considered a multifactorial disease, similar to venous thrombosis, which is thought to result from an interaction between genetic and nongenetic (environmental or behavioural) risk factors (1 7 25). Most individuals with a single coagulation disorder do not develop thrombosis, and in many cases of venous thrombosis, more than one predisposing factor is involved, e.g. an inherited thrombophilia in combination with another risk factor such as pregnancy, surgery, trauma or immobilisation. For many of the coagulation disorders, the effect on arterial ischaemic stroke, if any, is only modest. However, some studies indicate that coagulation disorders that individually have no or limited influence are associated with an increased risk of stroke in coexistence with another risk factor.
Patent foramen ovale
Patent foramen ovale (PFO), a persisting opening in the septum between the left and the right atrium of the heart, is estimated to be present in over 25% of the general population (97). Several case–control studies and one meta-analysis found a higher frequency of PFO in patients with cryptogenic stroke as compared with the control group, in particular, in the younger age groups (97–99). In a prospective study among 581 ischaemic stroke patients aged 18–55-years, the presence of both PFO and atrial septal aneurysm, but not PFO alone, was significantly associated with an elevated risk of recurrent stroke (100). However, it is still disputed whether PFO and ischaemic stroke are causally related, and if so, what might be the underlying mechanism. A number of theories have been proposed, the idea of a paradoxical embolism from the peripheral venous system through the PFO to the brain being the oldest and best known. Yet, deep venous thrombosis, either with or without accompanying Valsalva manoeuvre, is very rare in patients with PFO who suffer ischaemic stroke. Alternatively, it has also been suggested that the PFO tunnel itself might be a source of thrombi or that the PFO might induce thrombus formation due to transient arrhythmias (97 101). The presence of a hypercoagulable state is assumed to increase the risk of ischaemic stroke in patients with PFO by promoting the formation of venous thromboemboli or enhancing the risk of direct embolisation from the PFO. A number of case–control studies indeed suggest that the presence of the prothrombin G20210A or the FVL mutation is associated with an increased risk of ischaemic stroke in patients with PFO (101–104). Prospective studies investigating the interaction between PFO and coagulation abnormalities in relation to ischaemic stroke have not been published thus far.
Oral contraceptive use
There is still disagreement whether the use of oral contraceptives should be considered an independent risk factor for ischaemic stroke, as results from studies evaluating this relationship have been contradictory. However, in a large meta-analysis of 16 case–control studies, current contraceptive use was significantly associated with the occurrence of ischaemic stroke, with evidence of a dose–response relationship (105). A limited number of studies have examined the interaction between coagulation disorders and oral contraceptive use. A small case–control study showed that the risk of cryptogenic ischaemic stroke was most marked in women who used oral contraceptives and had either the FVL or the prothrombin G20210A mutation (106). In other case–control studies, an increased risk of stroke was observed in women using oral contraceptives who also carried the FVL mutation, the MTHFR 677TT genotype or had hyperhomocysteinaemia (107–109). A definite pathophysiological explanation for these synergistic effects is lacking, but it has been found that the use of oral contraceptives causes acquired resistance to activated protein C and decreased concentrations of free and total protein S, although the biological basis of this finding is unknown (110).
Atherosclerotic lesions
There is evidence that the presence of atherosclerotic lesions, in particular, vulnerable plaques prone to rupturing, is related to platelet activation, initiation of the coagulation cascade and an increased fibrin turnover (111). Therefore, it has been hypothesised that the presence or the severity of atherosclerosis might affect the risk of thrombotic events in the venous system. Proof for this hypothesis comes from a case–control study showing that asymptomatic carotid artery atherosclerosis as measured by ultrasonography was more frequent in patients with a deep venous thrombosis of unknown origin than in those with secondary thrombosis and in control subjects (112). However, in two prospective population-based cohort studies, no association was found between measures of subclinical atherosclerosis (carotid intima–media thickness or the presence of atherosclerotic plaques) and the occurrence of venous thromboembolic events during follow-up (113 114). It is conceivable that the simultaneous existence of atherosclerotic lesions, especially disrupted plaques, and a coagulation disorder might exert a synergistic effect on the risk of arterial ischaemic stroke. Although this interaction has not been evaluated systematically thus far, it offers an interesting basis for future research now that noninvasive techniques such as multislice CT and MRI have become available to evaluate the burden of carotid atherosclerotic disease (115).
Discussion
There is a lack of methodologically sound studies on the relation between coagulation disorders and arterial ischaemic stroke. Most of the published research falls short on the criteria for causality that we mentioned in the introduction, and publication bias has almost certainly influenced the literature. Nearly all studies had a retrospective case–control design, which is susceptible to different sorts of bias. Poor selection of controls may lead to biased findings and incorrect conclusions, in particular, in studies concerning specific subgroups such as children or young adults. In addition, reversed causality may have played a role when measurements were carried out after stroke onset, for example of factors that are influenced by inflammation such as fibrinogen or PAI-1. Coagulation abnormalities could be secondary to the occurrence of ischaemic stroke, or due to an acute-phase reaction, and the results of retrospective studies should therefore be interpreted with caution. Limited sample size often results in insufficient statistical power. Especially studies on genetically determined disorders are likely underpowered, as the effects of single genetic variations are expected to be small. This is illustrated by the fact that for some of the inherited coagulation disorders, most individual studies failed to demonstrate a relation to ischaemic stroke, whereas meta-analyses suggest a modest, yet significant association. Large prospective studies are scarce, and some of them also have limitations. In many instances, measurements of protein C, protein S or antithrombin were performed just once, while acquired and transient decreases in the levels of these proteins are far more frequent than hereditary deficiencies (4). Antiphospholipid antibodies may also be transiently elevated due to non-specific causes, but repeated laboratory testing was not performed in most studies either. Furthermore, only a few studies allowed for the evaluation of potential dose–response relationships, and many genetic studies failed to explore the relation between genetic variations and the levels or the function of the gene product. Finally, only a few studies have simultaneously evaluated multiple coagulation abnormalities or potential risk factors for thrombosis, thus allowing the possibility to study interactions between several genetic and nongenetic factors. Moderate effects of coagulation disorders that only occur in the presence of another factor might thus be missed. From this point of view, a case–crossover approach, when technically feasible, could be a promising approach.
Given the methodological shortcomings in the available literature, there is clearly a need for large, prospective population-based studies evaluating the role of coagulation abnormalities in the pathophysiology of arterial ischaemic stroke. In order to allow conclusions regarding causality and to guide the management of individual patients, prospective data are required especially on the hereditary coagulation disorders, the presence of antiphospholipid antibodies without APS and as yet scarcely investigated factors such as vWF, ADAMTS13 and PAI-1. Large intervention studies should solve the issue of whether or not homocysteine lowering might prevent (recurrent) stroke (86), and larger studies are needed to appreciate the role of genetic variations.
There is currently no consensus about the value of screening for coagulation disorders in patients with arterial ischaemic stroke (4–6). Most authors do not recommend routine testing for inherited coagulation disorders, but some state that it might be valuable in younger patients (4 8 116). At present, convincing evidence for a relationship with ischaemic stroke of hereditary deficiencies of protein C, protein S, and antithrombin, the FVL and prothrombin G20210A mutations and protein Z levels is lacking, possibly with the exception of the prothrombin G20210A mutation in adults and protein C deficiency in children. Hence, there is no valid indication for testing all patients with arterial ischaemic stroke for these conditions. The APS is almost by definition associated with an increased risk of ischaemic stroke. Still, data on mildly elevated titres of antiphospholipid antibodies without other features of APS are conflicting. According to some, testing should be conducted in every stroke patient (4), or only in young persons or patients with other features of APS (51), whereas others feel that given the current evidence, it is not appropriate at all (49). The lack of therapeutic implications should topple the balance. Current evidence does not justify diagnostic testing for malignant disease in patients who experienced arterial ischaemic stroke. In spite of the evidence for a significant but modest association between increased homocysteine and ischaemic stroke, routine assessment of homocysteine levels after an ischaemic stroke should not be recommended either, as causality of this association is still debated and definite proof for the effect of treatment with vitamin supplementation is lacking (60). Including fibrinogen measurements in the diagnostic workup of stroke patients would also be premature at this time, given the uncertainty about clinical significance, the proper timing of fibrinogen measurements and appropriate cut-off points (117). Finally, the existing data do not support assessments of vWF, ADAMTS13, TAFI, PAI-1 or genetic variations of factors involved in coagulation. Nevertheless, each individual stroke patient merits a tailor-made diagnostic workup, sometimes including tests for certain coagulation disorders. On the other hand, it should be emphasised that a diagnosis of a coagulation disorder in a patient who suffered an ischaemic stroke does not obviate the necessity of a full diagnostic workup.