
Abstract
Objectives:
We sought to better characterize spindle cell carcinoma (SpCC) of the upper aerodigestive tract, a rare and aggressive variant, through comparison of a large cohort of head and neck SpCCs against a cohort of conventional head and neck squamous cell carcinoma (SCC) patients.
Methods:
We compared epidemiologic and clinicopathologic characteristics of 341 SpCCs with 67 882 SCCs of the head and neck, drawing data from the SEER national database. We also compared disease-specific survivals (DSS) for SpCC and SCC based on tumor site and mode of treatment.
Results:
SpCCs were predominantly laryngeal (46.4%, P < .001) and were more likely to be high grade (P > .001). SpCCs were also more likely than SCCs to present at an early stage (P < .001 to P < .05). Rates of distant metastasis were similar between the tumor types. DSS was similar between SpCCs and SCCs, although site-specific survival rates were higher for SpCCs of the larynx (P = .017) and lower for those of the oral cavity (P = .008).
Conclusion:
SpCC of the head and neck is more likely than SCC to present at an early stage, with fewer nodal metastases. Survival rates appear to depend on anatomic site as well.
Spindle cell carcinomas (SpCCs) are rare neoplasms of mixed composition, containing variable proportions of carcinomatous and sarcomatous components. The tumors are found mainly in the upper aerodigestive tract (UADT), with roughly half of all SpCCs arising in the larynx and most others occurring in the oral cavity or oropharynx. 1 Their gross appearance is typically that of a pedunculated mass, often with an ulcerated surface that is covered with a vegetative exudate. 2 SpCC is by definition biphasic, typically consisting of both squamous carcinoma and spindle cells, although there may be elements of nearly any connective tissue present. 3 This observed cellular pleomorphism has led to a long and rather confusing list of names including sarcomatoid carcinoma, pleomorphic carcinoma, spindle cell carcinoma, and carcinosarcoma. 4 The heterogeneous nature of SpCC has also presented considerable diagnostic challenges for the surgical oncologist and pathologist alike; biopsies of insufficient size and depth are prone to capturing exclusively 1 cellular component, and even an adequate biopsy can bear a striking histopathologic resemblance to other neoplasms including atypical fibroxanthoma and desmoplastic melanoma, as well as various sarcomas, low-grade tumors, or reactive/infectious lesions.4-7
SpCC has typically been regarded as a more aggressive neoplasm than conventional squamous cell carcinomas (SCCs) of the head and neck, with higher rates of recurrence and metastasis, and poorer survival rates.8,9 Cases in prior series have often been particularly refractory to primary or adjuvant radiotherapy.9,10 However, due to the rarity of these tumors, previous studies have been too limited in size to produce clear guidelines for the treatment of SpCC. Earlier studies that have demonstrated disappointing responses to radiotherapy were either of limited size and scope, drawn from nonrepresentative populations, or lacking the data to make certain inferences about treatment and outcomes. Although perhaps the most comprehensive evaluations to date, 2 separate series, published by Spector et al 9 and Viswanathan et al, 11 consisted of only 48 and 103 patients, respectively, each from individual tertiary referral centers. Much of the remaining literature regarding such tumors is limited to even smaller series or case reports. The largest prior series to date, published by Thompson et al, 10 reviewed 187 patients with SpCCs of the UADT, drawn from the Armed Forces Institute of Pathology. However, robust conclusions could not be drawn about the impact of treatment modality on survival due to incomplete data.
In the following study, we utilized the SEER national cancer database to conduct a retrospective analysis of 341 cases of head and neck SpCC, comparing various epidemiologic and clinicopathologic factors against those of typical SCC. We also compared disease-specific survivals for SpCC and SCC based on primary tumor site and mode of treatment, evaluating responses to surgery, radiation, and combination therapy. To our knowledge, this is the largest SpCC series to date.
Methods
Data Source
The Surveillance, Epidemiology, and End Results (SEER) Program of the National Cancer Institute is a coordinated system of population-based cancer registries that is widely used to study a large variety of malignancies. Strategically located across the United States, the SEER registries routinely collect data on patient demographics, primary tumor site, tumor morphology, stage at diagnosis, first course of treatment, and follow-up vital status. Site-specific histology coding rules containing detailed histology coding instructions are applied uniformly across all registries. The SEER program performs continuous quality control activities to ensure the collection of high quality data, including case finding, recoding, and reliability studies, conducted by off-site auditors every 2 years. Collectively, the 17 registries included in our analysis represent an estimated 26% of the United States population from several geographic regions. 12 Since SEER data are completely deidentified and publically available, this study was exempt from formal review by the Medical University of South Carolina Institutional Review Board.
Patient Selection
The SEER database was queried for patients diagnosed with SCC and SpCC of the UADT based on International Classification of Diseases for Oncology (ICD-O-3) anatomic site and histology codes, between the years 2000 and 2008. Only cases with conventional and spindle SCC were included in the cohort (ICD-O-3 codes 8070/3: squamous cell carcinoma, NOS; 8071/3: squamous cell carcinoma, keratinizing; 8074/3: squamous cell carcinoma, spindle cell variant). Patients without a histologically confirmed diagnosis were excluded, as well as cases diagnosed at autopsy. Patients were then classified into the following tumor location subgroups: oral cavity, nasopharynx, oropharynx, hypopharynx, larynx, sinonasal. Patients with tumor locations that were recorded as “overlapping lesion of tongue,” “tongue, NOS,” “overlapping lesion of palate,” “palate, NOS,” “pharynx, NOS” could not be classified by head and neck subsite and were excluded from site-specific analysis.
Patient demographics, including age at diagnosis, sex, and ethnicity, as well as tumor factors were obtained. Ethnicity was categorized as white, black, Asian/Pacific Islander, American Indian/Alaska native according to SEER’s “race recode” variable. Tumor factors queried included size, grade, extension, and extent of disease (ie, regional and/or distant metastases). Tumor grade was classified as low (well to moderately differentiated) or high (poorly differentiated or undifferentiated). AJCC T, N, and M stage is recorded according to the sixth edition of the AJCC Staging Manual for patients diagnosed after 2003; therefore, stage classification was compared only among patients diagnosed in or after 2004. Data were obtained from all 17 US cancer registries participating in the SEER program using SEER*Stat version 7.0.4 (www.seerstat.gov/).
Statistical Analysis
Differences in clinicopathologic characteristics between patients with spindle cell SCC and conventional-type SCC were compared using the chi-square test (categorical variables), and the student’s t test or nonparametric rank sum test (continuous variables).
Kaplan–Meier survival analyses were used to compare 5-year disease-specific survival (DSS) between patients with spindle cell SCC and SCC. The log-rank test assessed statistical differences between survival curves. Survival time was provided as the number of months between date of diagnosis and date of death, date last known to be alive, or December 31, 2008, whichever occurred first. Because the endpoint for our analysis was 5-year DSS, patients surviving more than 60 months were coded as censored at 60 months. Patients lost to follow-up before 60 months were censored at time of last contact.
To determine the independent effect of potential prognostic factors in the SpCC group, univariable and multivariable Cox regression analyses were used to calculate hazard ratios (HRs) with 95% confidence intervals (CIs). Factors were included in the multivariable model if P < .25 on univariable analysis.
Statistical significance was set at P < .05. All tests were 2-sided. Stata version 10.0 (StataCorp, College Station, Texas, USA) statistical software was used for all statistical analysis.
Results
Study Population
A total of 67 882 patients with conventional SCC and 341 patients with SpCC were identified. Table 1 describes patient demographics and the distribution of tumor location in each group. SpCC presented at a slightly later age than SCC (mean age 67 vs 63, P = .0004), although no statistically significant differences in either sex or ethnic distributions were found between the 2 groups. In terms of primary site distribution, significant differences were observed between SpCC and SCC. Far more SpCC tumors presented in the larynx (46.4%) than in either the oropharynx (18.0%) or oral cavity (20.4%), while tumors were more evenly distributed between the oropharynx (31.0%), larynx (32.8%), and oral cavity (35.0%) in conventional SCC (P < .001). An analysis of subsite distribution also revealed differences between the 2 tumor classes (Table 2). Within the larynx, SpCCs were more likely to arise in the glottis (78.7% vs 59.9%, P < .001), while SCC was more likely to be found in the supraglottic region (38.3% vs 17.7%, P < .001). Oropharyngeal SpCCs were more likely to occur in the tongue base/lingual tonsil (58.8% vs 43.4%, P = .002), while SCCs were more often found in the palatine tonsil (48.7% vs 29.4%, P = .002). Subsite distributions within the oral cavity were similar for both tumor types.
Clinicopathologic Characteristics of Patients With Spindle Cell and Conventional-type Squamous Cell Carcinoma.
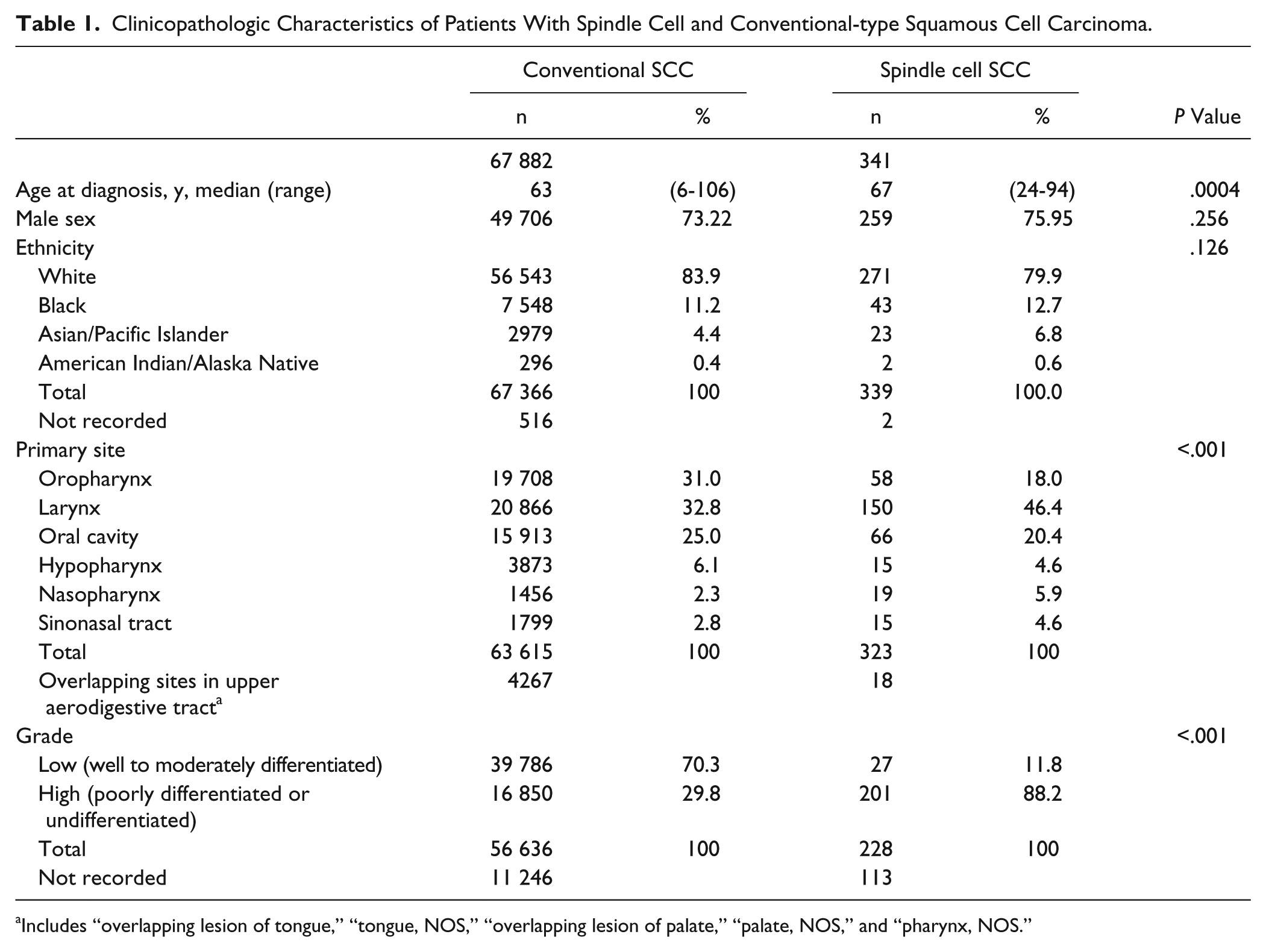
Includes “overlapping lesion of tongue,” “tongue, NOS,” “overlapping lesion of palate,” “palate, NOS,” and “pharynx, NOS.”
Subsite Frequency Distribution for Patients With Spindle Cell and Conventional-type SCC.
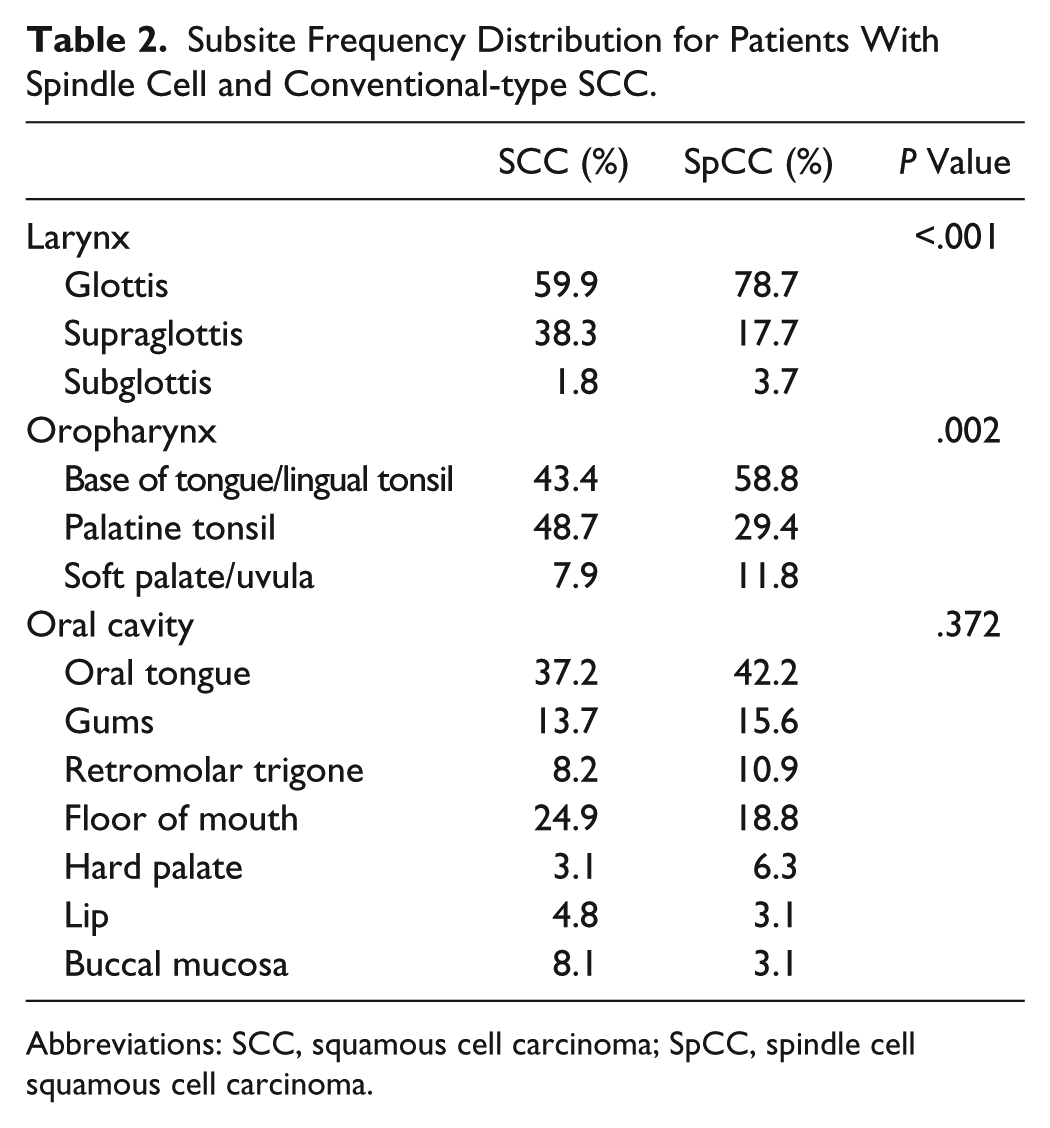
Abbreviations: SCC, squamous cell carcinoma; SpCC, spindle cell squamous cell carcinoma.
Tumor Characteristics
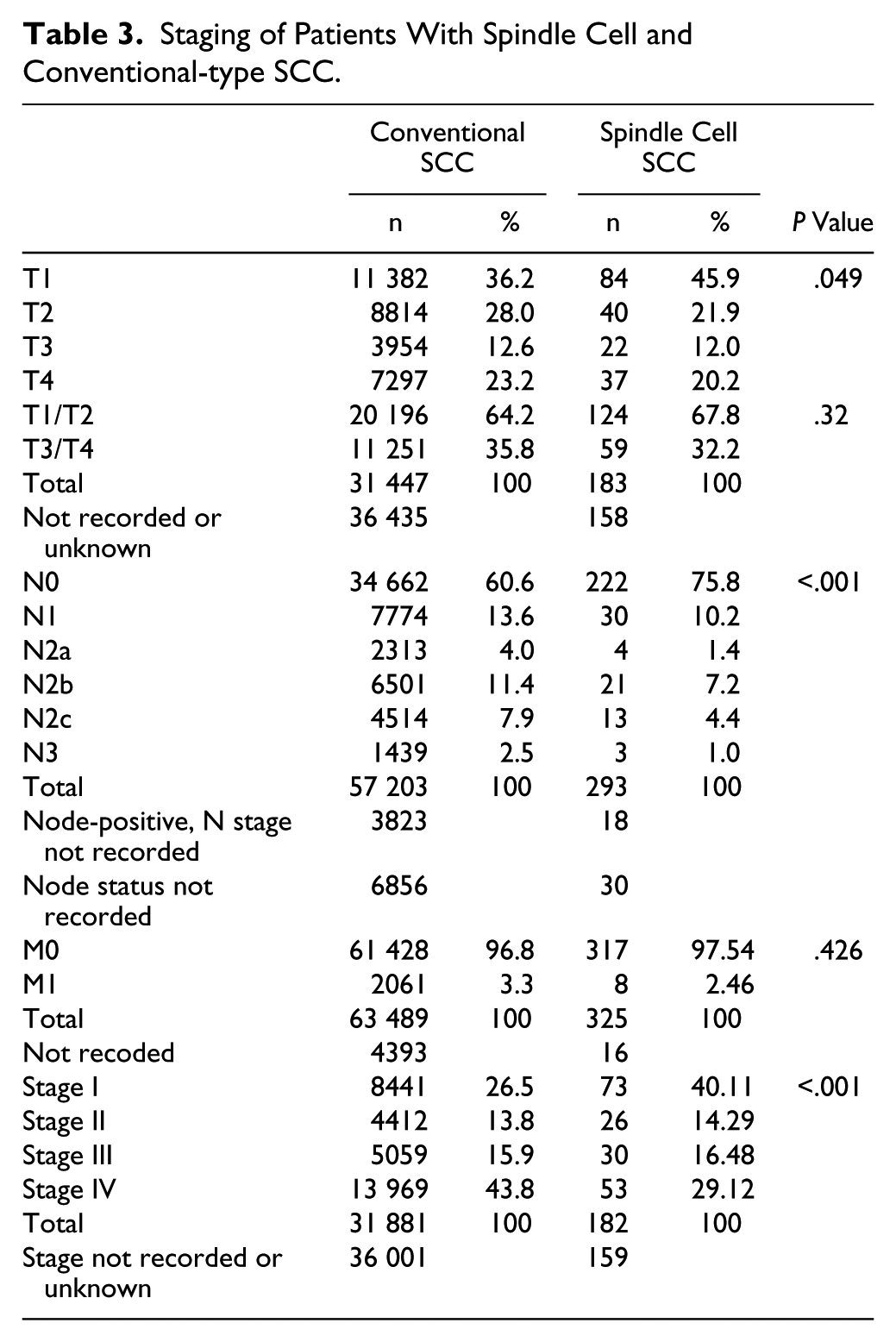
Table 3 summarizes the data describing tumor grade and staging. Nearly all SpCC tumors were considered high grade (88.2%), while the majority of SCC tumors were considered low grade (70.3%). SpCC was more likely to be diagnosed at the earliest stage (T1) than was SCC (45.9% vs 36.2%, P = .049). However, there were no significant differences in the overall likelihood of locally advanced disease (T3/T4). In terms of regional disease, SCC patients were more likely to harbor nodal metastases (39.4% vs 24.2%, P < .001). However, both groups had similar rates of distant metastasis at presentation. Taken as a whole, patients with SCC were more likely to present with advanced stage disease (stage III/IV) than were patients with SpCC (59.7% vs 45.6%, P < .001).
Staging of Patients With Spindle Cell and Conventional-type SCC.
Treatment
Complete treatment data were available for 306 (90%) and 58 193 (86%) patients with SpCC and SCC, respectively (Table 4). SCC patients more frequently underwent radiotherapy alone (44.8% vs 32.4 %, P < .001), while SpCC patients were more likely to receive combined treatment with surgery and radiation (42.5% vs 29.4%, P < .001). Rates for treatment with primary surgery were similar for both groups.
Treatment of Patients With Spindle Cell and Conventional-type SCC.
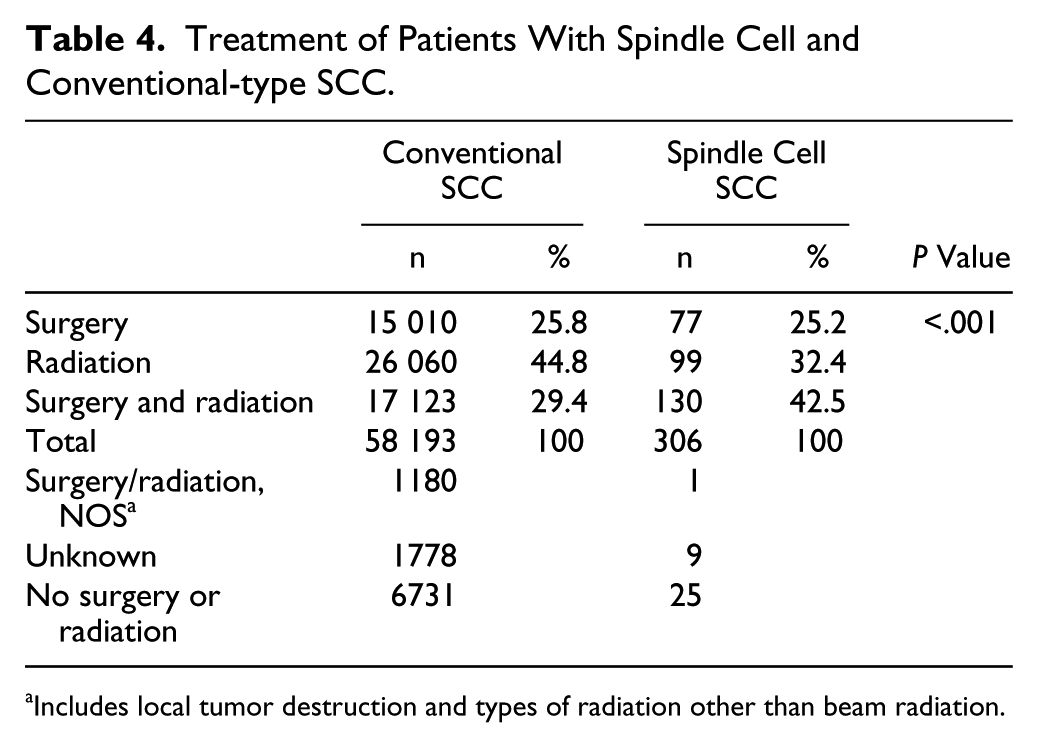
Includes local tumor destruction and types of radiation other than beam radiation.
Survival Analysis
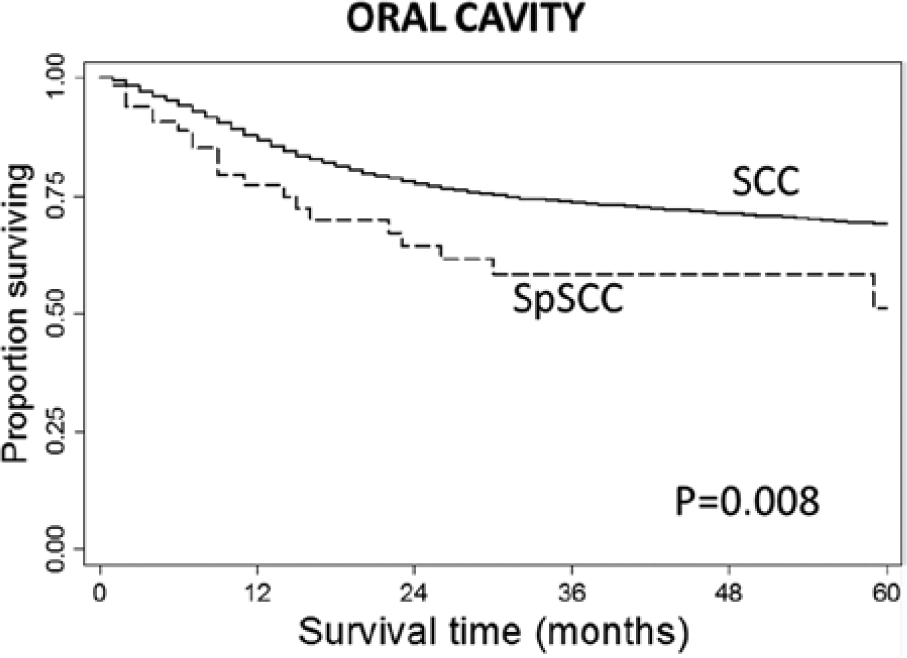
The effect of tumor histology on survival is illustrated in Figure 1. Median follow-up was 24 and 22 months in the SCC and SpCC groups, respectively (P = .52). The overall 5-year DSS was similar among patients with SpCC and conventional SCC (P = .748). However, when analyzing site-specific survival rates, several differences were observed between the 2 groups (Figures 2-4). Oral cavity SpCC carried a worse prognosis than SCC of the oral cavity (P = .008), while laryngeal SpCC had a more favorable prognosis than SCC of the larynx (P = .017). SpCC of the oropharynx also displayed a trend toward a poorer 5-year survival rate, although not statistically significant (P = .109). Due to the differences in subsite distribution between laryngeal SCC and SpCC, the 5-year DSS results were stratified based on laryngeal subsite to ensure that results were not skewed (Figure 4). A marginally significant improvement in DSS was seen for SpCC of the glottis (P = .047), and the relative increase in the prevalence of SpCC at this subsite may have enhanced overall laryngeal survival rates. This stratification was not done for oral cavity DSS because subsite distributions were similar between the 2 tumor types.
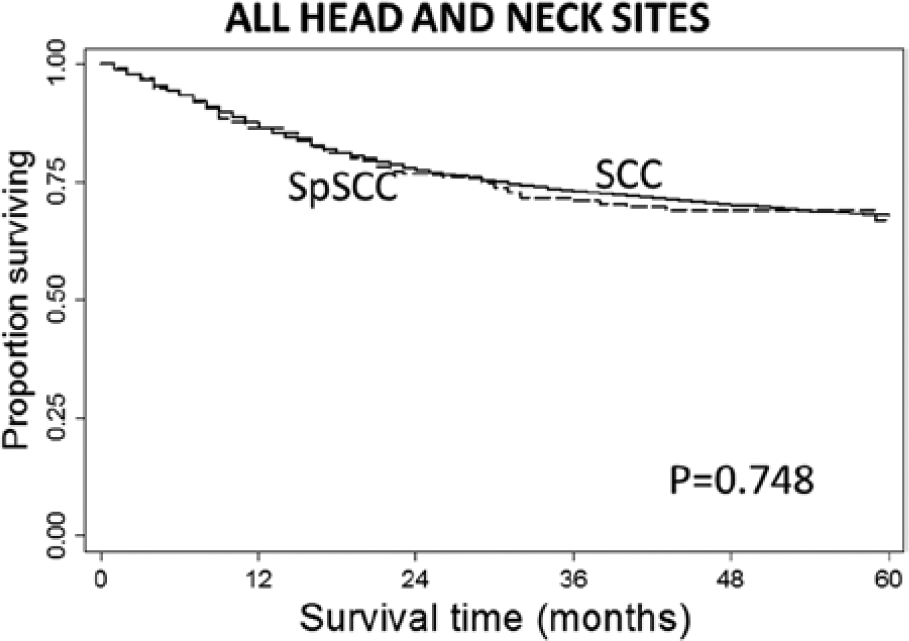
Disease-specific survivals for spindle cell carcinoma and squamous cell carcinoma of all head and neck sites.

Disease-specific survivals for spindle cell carcinoma and squamous cell carcinoma of the oral cavity.
Disease-specific survivals for spindle cell carcinoma and squamous cell carcinoma of the oropharynx.
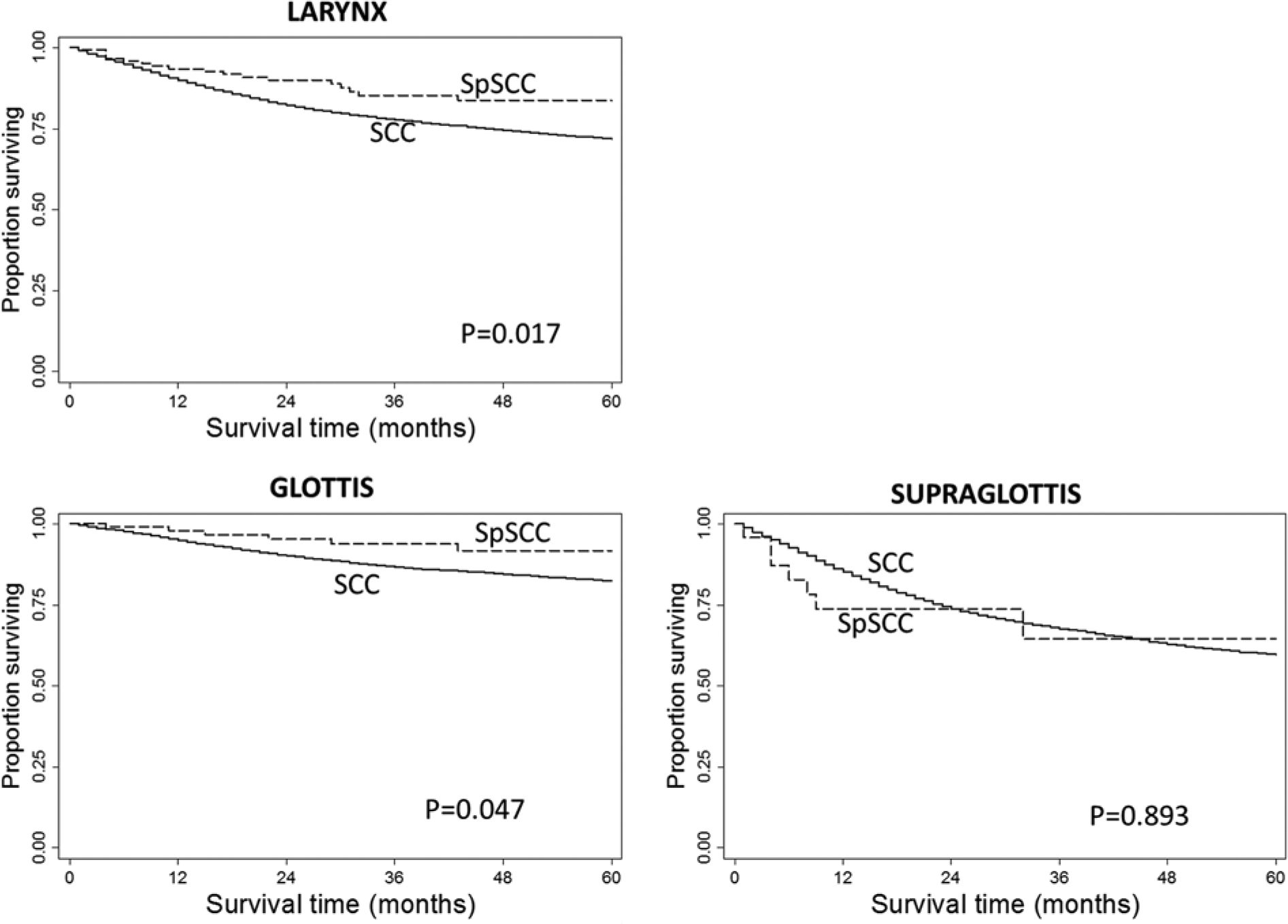
Disease-specific survivals for spindle cell carcinoma and squamous cell carcinoma of the larynx (a), glottis (b), and supraglottis (c).
The results of univariable and multivariable analyses, which evaluated various clinicopathologic factors with respect to DSS, are shown in Table 5. Multivariable analysis controlling for demographics (age at diagnosis, sex, and ethnicity), tumor grade, and overall stage showed that only advanced local (T3/T4), regional (N2/N3), and distant disease (M1) were negative prognostic indicators for SpCC .
Univariable and Multivariable Analysis of Prognostic Factors in Spindle Cell Carcinoma of the Head and Neck.
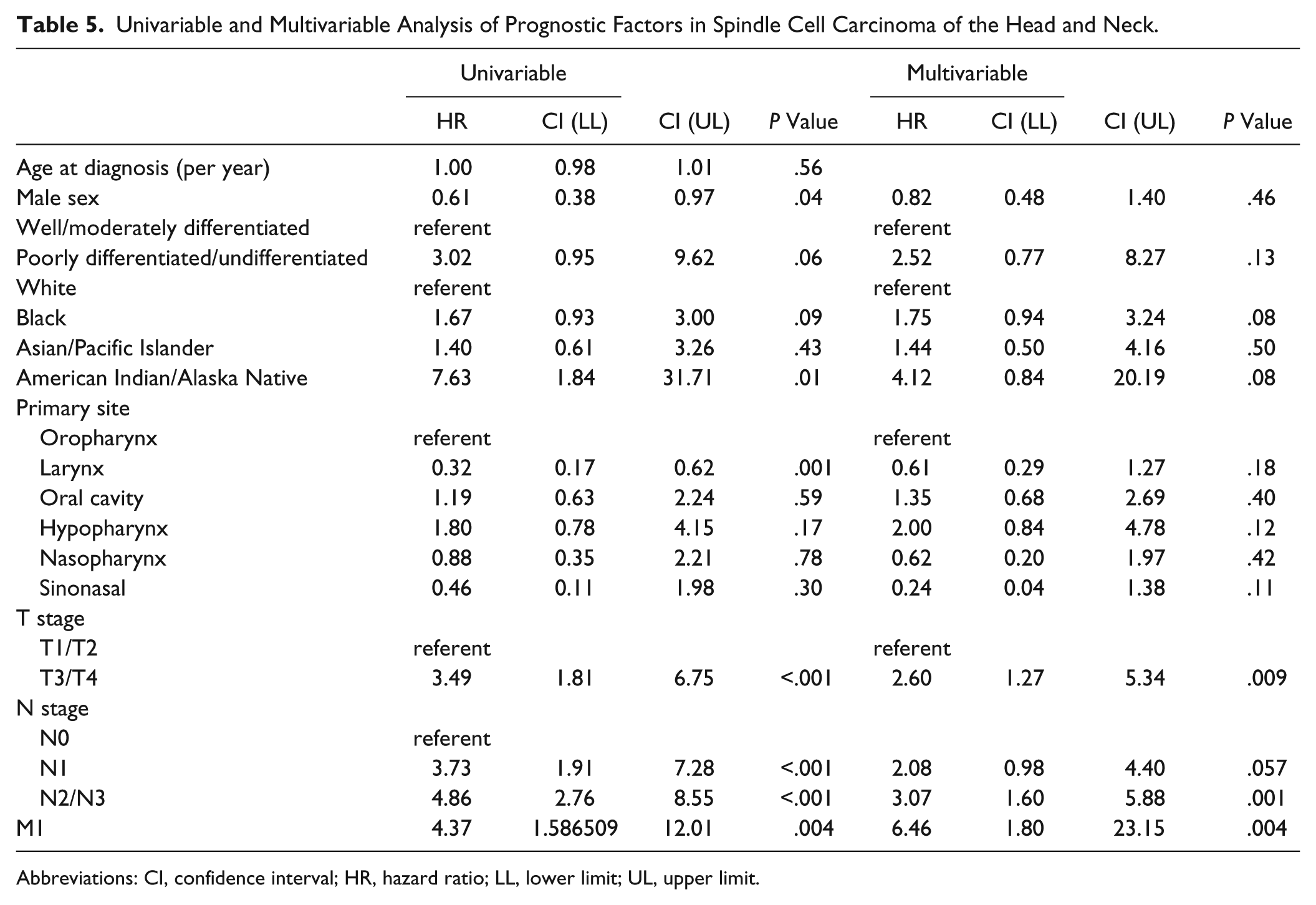
Abbreviations: CI, confidence interval; HR, hazard ratio; LL, lower limit; UL, upper limit.
Discussion
SpCCs are known to be quite rare compared with conventional SCC of the head and neck, representing a mere 0.5% of all SCCs in this region. Spector et al 9 reported an incidence of 2.7% among the laryngeal SCC cases pulled from the Armed Forces Institute of Pathology records, although they suspected an actual incidence closer to 1%. It is unclear why such a discrepancy exists between these 2 incidence rates, but the selection of cases exclusively from within the military health care system would necessarily introduce a sampling bias that might be reflected in the observed incidence rate of SpCC, a possibility acknowledged by the current authors. It must be stated however that the inherent difficulties in making accurate and consistent pathologic diagnosis of these lesions would be equally likely to introduce such inconsistencies; the SEER data are not immune to this reality, and error in pathologic diagnosis constitutes an important limitation of this study.
It has long been believed that SpCC was a more aggressive variant of conventional SCC, and several earlier studies have indicated that these tumors were prone to treatment failure, loco regional recurrence, and possibly even distant spread or poorer survival outcomes.8,9 However, earlier studies have not been sufficiently conclusive to inform decisions regarding the treatment of SpCC.9-11 In the current study, by comparing DSS, tumor characteristics, and demographics for patients with head and neck SpCC against those with conventional SCCs, we have shown that in spite of being characterized as a considerably more aggressive variant of SCC, SpCC of the head and neck presented with significantly less locoregional or distant spread than conventional head and neck SCC, with a comparable prognosis observed for both tumor groups (Table 3, Figure 1). This finding would seem at odds with those reported by Thompson et al and others mentioned previously,9-11 where aggressive regional and distant spread were key characteristics of SpCC.
Survival rates varied by anatomic site such that oral cavity SpCC lesions actually carried poorer prognoses than their SCC counterparts, while laryngeal SpCCs fared better (Figures 2-4). This is, we believe, a key finding and one that speaks to the prognostic importance of laryngeal, and particularly glottic location in forecasting an improved outcome with SpCCs. Laryngeal (and particularly glottic) primaries are for obvious reasons associated with earlier symptomatology, and consequently earlier diagnosis, favoring better outcomes. It is perhaps the higher distribution of glottic tumors within the SpCC population that may explain improved survival for laryngeal SpCC as a whole (Figure 4a-c). Although previous studies have investigated the effect of tumor site on DSS, this is the first time that a statistically significant relationship between anatomic location and mortality has been demonstrated. 9 These findings were borne out in the results of univariable and multivariable analyses to identify potential prognostic indicators, comparing DSS according to subgroups defined by patient demographics, tumor grade, and AJCC stage classification. Our analysis revealed that outcomes for SpCC were primarily dependent on tumor stage and histologic grade (Table 5), although again, laryngeal involvement was a key positive indicator.
As an important caveat, it should be noted that comparisons of survival among oropharyngeal cancers are of limited utility in this study, owing to the absence of data regarding HPV status in the SEER database. The authors acknowledge that oropharyngeal SCC represents a unique and heterogeneous mixture of HPV- and non-HPV-associated tumors, each population having well documented differences in behavior and prognosis. Without the benefit of these data, it is impossible to fully evaluate the observed differences in survival for tumors of the oropharynx.
Although statistically significant correlations between mode of treatment and survival were also found, major limitations existed in the depth of detail regarding treatment circumstances within the SEER database, making it difficult to draw meaningful conclusions about treatment for this study. Another key drawback of the SEER database that bears mentioning is its lack of data regarding disease recurrence rates or disease-free survival; a factor particularly relevant to SpCC, with its reputation for recurrence. High local and regional recurrence rates, particularly after radiation therapy, were characteristic findings reported by Viswanathan et al 11 as well as Spector et al. 9 Ultimately, the breadth and depth of the data contained within the SEER database has placed certain limitations on our study. However, the SEER registries harbor a wealth of important data that can provide insight into important demographic and epidemiologic trends in cancer incidence and survival. Perhaps more important, the sheer size of the database allows one to search a vast number of cases, identifying large cohorts even for extremely rare neoplasms. Because the SEER registries are part of a nationwide network covering both a broad geography and a diverse population, studies generated through the database are conferred a greater degree of generalizability and a measure of immunity against regional treatment biases and institutional referral biases.
Conclusion
Our study, which describes the largest cohort of head and neck SpCCs to date, has challenged the traditional view of SpCC as an aggressive variant of SCC. Although typically a higher grade at diagnosis, SpCC was found to exhibit a lower overall tendency toward loco regional spread than that of SCC, while demonstrating a similar overall DSS. Survival rates were site specific, however, with oral cavity lesions harboring worse outcomes relative to conventional SCC, and laryngeal tumors carrying better outcomes. Future research should seek to provide insight into differences in response to various treatment modalities and salvage therapies, as well as local and regional recurrence rates.
Footnotes
Acknowledgements
Logistical support for this work was provided by the Department of Otolaryngology–Head and Neck Surgery, Medical University of South Carolina, Charleston, South Carolina. The authors declare that there are no financial conflicts of interest that would influence the impartiality of this scientific work.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was completed without the expenditure of grant funds. Material support in the form of software and office space was provided by the Medical University of South Carolina, Department of Otolaryngology–Head and Neck Surgery.