
Abstract
Introduction
Thoracic endovascular aortic repair (TEVAR) has become an accepted treatment for thoracic aortic disease. However, the principal complications relate to coverage of the thoracic aortic wall and deliberate occlusion of aortic branches over a potentially long segment. Complications include risk of stroke, spinal cord ischaemia (SCI) and arterial insufficiency to the left arm (left arm ischaemia (LAI)). This study specifically scrutinised the development of SCI and LAI after TEVAR for interventions for thoracic aortic disease from 1999 to 2020. In particular, those who underwent extra-anatomical bypass (both immediate and late) were compared to the length of thoracic aortic coverage by the stent graft.
Materials and methods
Ninety-eight patients underwent TEVAR. The presenting symptoms, pathology, procedural and follow-up data were collected prospectively with particular evidence of stroke, SCI and LAI both immediate onset and after 48 h of graft placement.
Results
Fifty underwent TEVAR for an aneurysm (thoracoabdominal aortic aneurysm), 22 for dissection, 19 for acute transection and 7 for intramural haematoma/pseudoaneurysm of the thoracic aorta. Twenty-nine (30%) required a debranching procedure to increase the proximal landing zone (1 aorto-carotid subclavian bypass, 10 carotid/carotid subclavian bypass and 18 carotid/subclavian bypass). Ten patients (10%) died within 30 days of TEVAR. Twenty-four grafts covered the left subclavian artery origin without a carotid/subclavian bypass. Five required a delayed carotid/subclavian bypass for LAI (4) and SCI (1). Six developed immediate signs of SCI after TEVAR and these 11 (group i) had a mean (SD) length of coverage of the thoracic aorta of 30.2 (10.6) cm compared to 21.5 (11.2) cm (group g) in those who had no LAI or SCI post TEVAR, p < 0.05.
Conclusions
In this series, delayed carotid/subclavian bypass may be required for chronic arm ischaemia and less so for SCI. The length of coverage of thoracic aorta during TEVAR is a factor in the development of delayed SCI and LAI occurrence. Carotid subclavian bypass is required for certain patients undergoing TEVAR (particularly if greater than 20 cm of thoracic aorta is covered).
Introduction
As endovascular abdominal aortic aneurysm repair (EVAR) became established to treat abdominal aortic aneurysms (AAA), inevitably the natural progression was to treat thoracic aortic disease by a similar technique. One early report for stent grafting of thoracic aortic pathology was in 1994, and since then, there has been worldwide interest in the concept. 1 The initial indication for thoracic endovascular aortic repair (TEVAR) was to treat aneurysmal disease (thoracoabdominal aortic aneurysm (TAAA)) and soon expanded to treat type B aortic dissections (TBADs) and acute transections (ATs).
For durable sealing, proximally and distally, a suitable ‘landing zone’ within the thoracic aorta is required. This has meant the proximal landing zone (PLZ) often needs to include the thoracic aorta where vital branches arise to perfuse the brain and upper limbs. To prevent endoleaks, a durable sealing zone proximal to the commencement of the aortic wall pathology needs a coverage of 2 cm of normal aorta. There is no doubt the inominate and left common carotid artery must be revascularised if their origins are covered by a stent graft as a PLZ. However, this is not the case for the left subclavian artery (LSA) due to extensive natural collateralisation.
The thoracic aorta has been classified into zones to aid with nomenclature for describing the PLZ for a stent graft which needs to be deployed and vital branches which will be occluded (Figure 1). When a stent graft is positioned proximally in zones 0 or 1, then a revascularisation procedure has to be performed to perfuse the inominate and left common carotid arteries.2,3 However, for stents placed proximally in zone 2, only the LSA is covered and there are varying opinions in the literature regarding the need to routinely perform LSA revascularisation either pre- or post-TEVAR deployment.4–6

Thoracic aorta classified according to the proximal landing zones (PLZ).
Importantly, the blood supply for the anterior aspect of the upper spinal cord arises from a single longitudinally running anterior spinal artery which is a branch of each vertebral artery. Furthermore, distally, the vertebral arteries supply the cerebellum via the anterior and posterior inferior cerebellar arteries, and 20% of the cerebral blood supply is from these paired arteries. The distal branches of the proximal LSA are the internal thoracic, thyrocervical and costocervical trunk before continuing its course distally as the axillary artery then ultimately the brachial artery to supply the left arm. Many patients do not require routine LSA revascularisation after TEVAR as there appears to be adequate collateral circulation to maintain perfusion to the upper spinal cord, posterior cerebral circulation and the arm. However, there is no reliable preoperative assessment in the literature which can reliably predict who actually require LSA revascularisation.
This is a retrospective study scrutinising all patients undergoing TEVAR in University Hospital of Wales over a 20-year period. Particular scrutiny is made to the length of coverage of the thoracic aorta, any extra-anatomical bypass procedures performed to the supra-aortic vessels, incidence of stroke, spinal cord ischaemia (SCI) and the development of left arm ischaemia (LAI; acute or chronic).
Material and methods
Ninety-eight patients (70 male and 28 female) with a median age (range) of 65 (24–91) years between 1999 and 2020 at the University Hospital of Wales underwent TEVAR. All elective cases were discussed preoperatively as to the optimum surgical management plan at multidisciplinary meetings (MDT). Those presenting as an emergency were discussed retrospectively, and all procedural details were recorded and stored on a secure vascular unit database. The patient data were retrospectively viewed and details were obtained for each patient.
Contrast-enhanced computed tomography (CT) was performed on all patients from the level of the femoral arteries proximally to include the arch of the thoracic aorta and origin of the supra-aortic branches to the arms and brain. Specific images of the internal carotid arteries and Circle of Willis were not routinely performed unless requested after the MDT when more information was requested concerning the intracranial circulation. This was particularly relevant if a left carotid/subclavian bypass (CSB) was proposed and information was required concerning the location and size of both vertebral arteries. All underwent TEVAR with Medtronic graft (Medtronic Inc, Minneapolis, MN). The length of graft (cm) providing coverage of the thoracic aorta was recorded for each patient. Outcomes recorded were all-cause mortality, any posterior or anterior circulation cerebrovascular accident, SCI and symptoms and signs of LAI after the LSA origin was covered.
All patients underwent TEVAR under general anaesthesia with radial artery monitoring of arterial blood pressure (BP). Since 2010, all elective TEVARs underwent cerebrospinal fluid drainage (CSFD) with the catheter remaining in situ for 72 h post TEVAR. For patients requiring landing zone in 0 and 1, they underwent extra-anatomical bypass pre TEVAR. For PLZ 2, the 2009 guidelines for LSA revascularisation was adhered to and a selective policy was undertaken. 7
Imaging – CT
All patients prior to TEVAR underwent thin-slice contrast-enhanced arterial phase CT angiography. At TEVAR, the lengths of each individual deployed covered stent was recorded. If more than one was deployed, then 5 cm was used as the overlap between adjacent stents in order to derive a total length covering the thoracic aortic wall.
Statistical analysis – Data analysis
Data were analysed using the Statistics Package for Social Scientists (IBM SPSS Statistics Version 27). Distribution normality was assessed using repeated Shapiro-Wilk W tests. Data were analysed using a combination of independent samples t-tests and Mann Whitney U tests as the non-parametric equivalent. Significance was established at p < 0.05 for all two-tailed tests with data presented as mean ± SD.
A comparison was performed between the length of thoracic aortic coverage for those developed SCI or LAI following TEVAR (group i) and those who were symptom free (group g). Subgroup analysis also compared those who underwent no bypass (group z) to those who underwent a CSB (group w).
Results
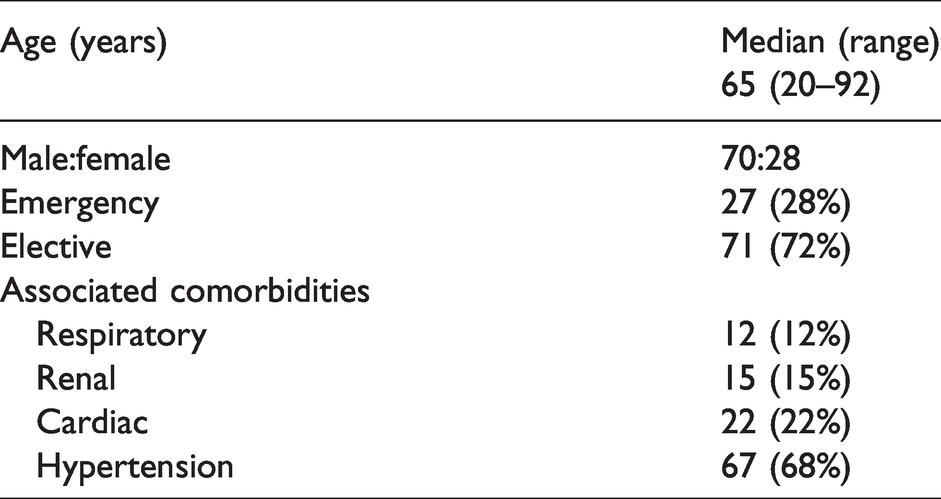
Patient demographics and associated comorbidities are listed in Table 1. The majority of TEVAR procedures (72%) were performed electively with associated comorbidities listed as respiratory, renal, cardiac and hypertension. Any ongoing treatment for these conditions was included as an associated comorbidity.
Patient demographics and associated comorbidities.
Indications for TEVAR and description of extra-anatomical bypasses performed
Fifty (51%) underwent TEVAR for TAAA, 22 (22%) for TBAD, 19 (20%) for AT and 7 (7%) for acute intramural haematoma and mycotic TAAA (Table 2). Of the 29 (29%) who underwent an extra-anatomic bypass graft, 24 were performed at the same time as the TEVAR was performed with 5 at a later date. Eighteen TEVARs were performed for TAAA with 1 aorto-carotid subclavian bypass, 10 carotid-carotid subclavian bypass and 7 CSB/subclavian-subclavian bypass (SSB) (1 delayed). For those undergoing TEVAR for TBAD, eight underwent a CSB (three delayed). Nineteen underwent TEVAR for acute AT with two receiving a CSB (one delayed). Twenty-nine underwent an extra-anatomical bypass where the length of thoracic aortic wall coverage was 25.7 (11.7) cm – group w.
Indications for TEVAR and description of extra-anatomical bypasses performed.
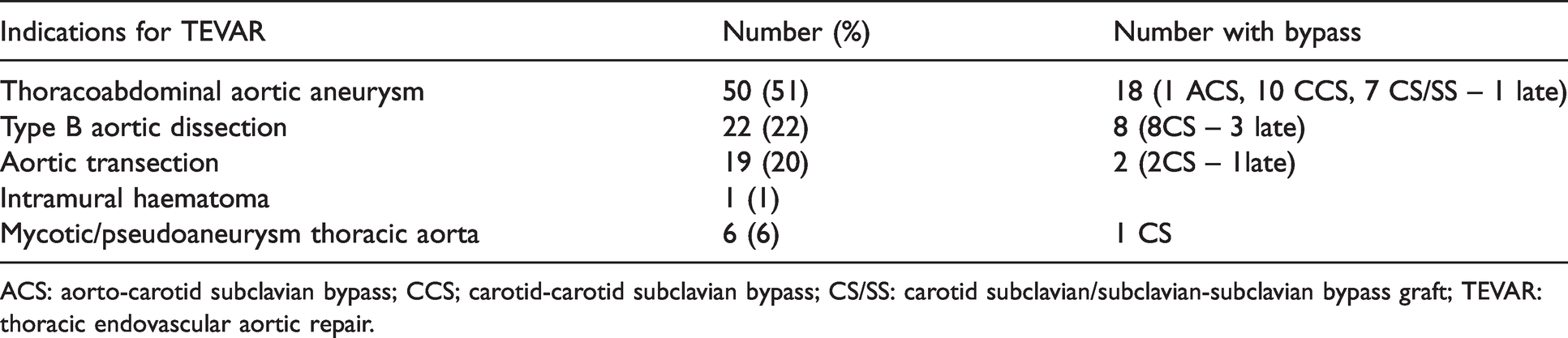
ACS: aorto-carotid subclavian bypass; CCS; carotid-carotid subclavian bypass; CS/SS: carotid subclavian/subclavian-subclavian bypass graft; TEVAR: thoracic endovascular aortic repair.
Length of coverage of thoracic aorta in those who developed complications (SCI and LAI) compared to those who did not
Mean (SD) for the length of thoracic aortic coverage was 24 (5.8) cm in the five patients who underwent delayed CSB post TEVAR – group d (Tables 3 and 4). This compared to 35 (9.9) cm in the six patients who developed signs of immediate SCI/stroke – group f (Table 5). When combined, group d and group f, these 11 (group i) had a mean (SD) of 30.2 (10.6) cm compared to 21.5 (11.2) cm (group g) in those who did not develop any symptoms or signs of LAI or SCI post TEVAR, p < 0.05. Both internal iliac arteries (IIAs) were patent in five undergoing TEVAR. The remaining one had an occluded right IIA but a patent left IIA.
LSA covered and underwent delayed extra-anatomical bypass due to LAI/SCI – group d.
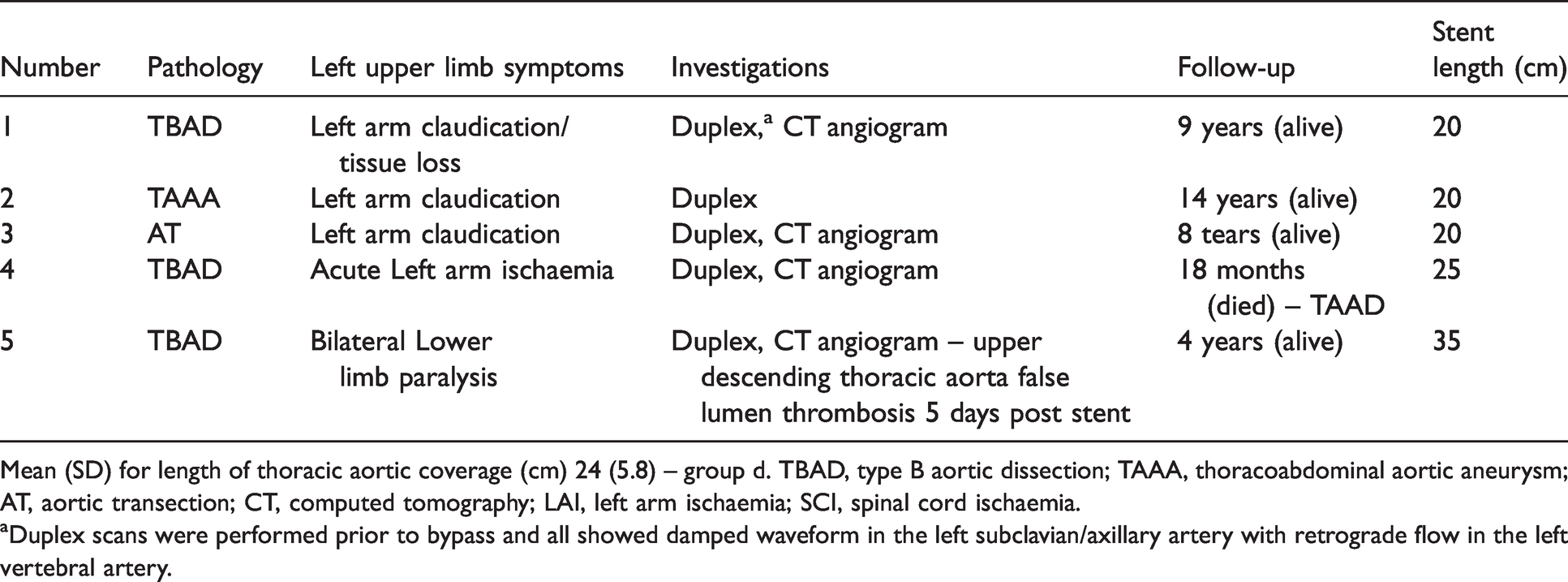
Mean (SD) for length of thoracic aortic coverage (cm) 24 (5.8) – group d. TBAD, type B aortic dissection; TAAA, thoracoabdominal aortic aneurysm; AT, aortic transection; CT, computed tomography; LAI, left arm ischaemia; SCI, spinal cord ischaemia.
aDuplex scans were performed prior to bypass and all showed damped waveform in the left subclavian/axillary artery with retrograde flow in the left vertebral artery.
Indications for delayed extra-anatomical bypass – group d.
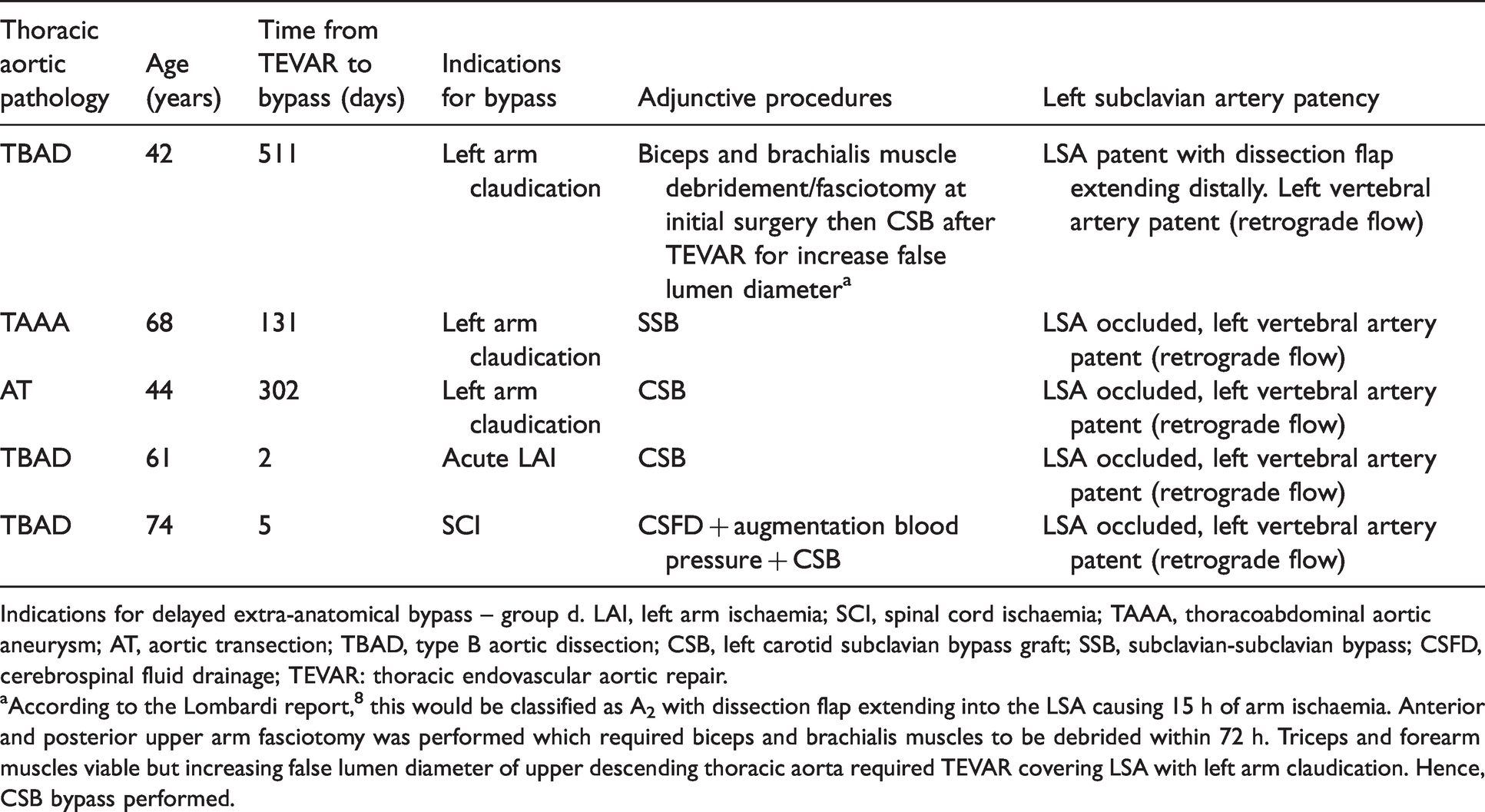
Indications for delayed extra-anatomical bypass – group d. LAI, left arm ischaemia; SCI, spinal cord ischaemia; TAAA, thoracoabdominal aortic aneurysm; AT, aortic transection; TBAD, type B aortic dissection; CSB, left carotid subclavian bypass graft; SSB, subclavian-subclavian bypass; CSFD, cerebrospinal fluid drainage; TEVAR: thoracic endovascular aortic repair.
aAccording to the Lombardi report, 8 this would be classified as A2 with dissection flap extending into the LSA causing 15 h of arm ischaemia. Anterior and posterior upper arm fasciotomy was performed which required biceps and brachialis muscles to be debrided within 72 h. Triceps and forearm muscles viable but increasing false lumen diameter of upper descending thoracic aorta required TEVAR covering LSA with left arm claudication. Hence, CSB bypass performed.
Patients developing immediate lower limb neurology/stroke after TEVAR.
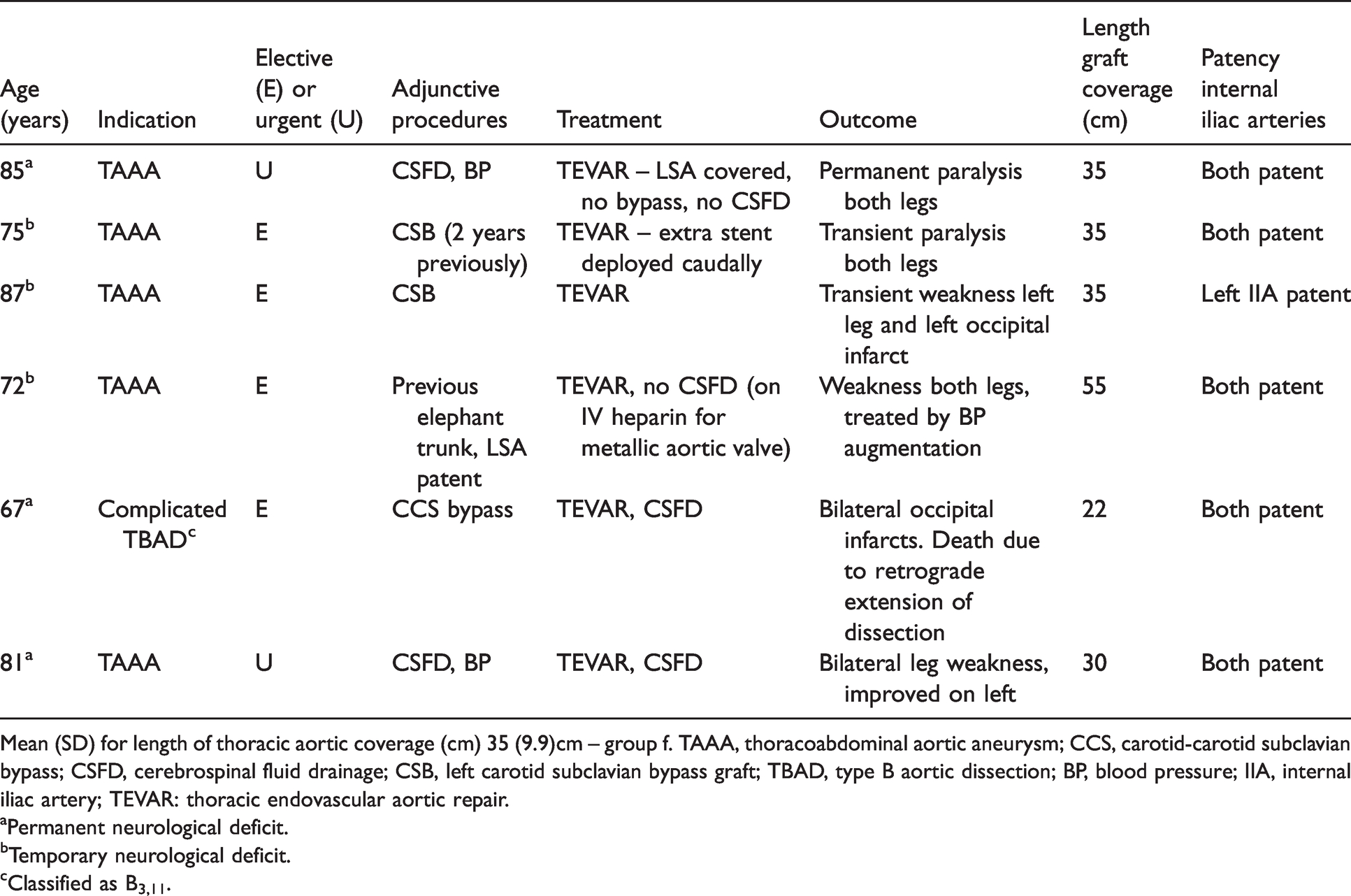
Mean (SD) for length of thoracic aortic coverage (cm) 35 (9.9)cm – group f. TAAA, thoracoabdominal aortic aneurysm; CCS, carotid-carotid subclavian bypass; CSFD, cerebrospinal fluid drainage; CSB, left carotid subclavian bypass graft; TBAD, type B aortic dissection; BP, blood pressure; IIA, internal iliac artery; TEVAR: thoracic endovascular aortic repair.
aPermanent neurological deficit.
bTemporary neurological deficit.
cClassified as B3,11.
Time interval from the TEVAR to extra-anatomical bypass ranged from 2 to 511 days. One patient, a 72-year-old man, after successful TEVAR for a TBAD developed bilateral lower limb weakness four days later. His repeat CT angiogram, post TEVAR, confirmed false lumen thrombosis of the upper descending thoracic aorta but no visualisation of intercostals arteries. Despite his blood pressure being maintained at physiological levels, CSFD was performed with complete resolution of the lower limb neurology. However, after further trial clamping of the spinal drain 24 h later, symptoms of SCI returned and he subsequently underwent left CSB with complete resolution of his symptoms. The remaining four developed LAI. One underwent CSB for acute LAI two days after TEVAR for a TBAD where the length of thoracic aortic coverage was 35 cm. The remaining three underwent CSB for chronic LAI not responding to conservative measures.
TEVAR with no extra-anatomical bypass performed (24 covering LSA)
Overall, 69 of 98 in the series received no extra-anatomical bypass either pre- or post-TEVAR – group z. Mean (SD) length of thoracic aortic coverage of this group was 21.1 (11.2) cm. When compared to the length of thoracic aortic wall coverage in group w (underwent CSB), this was 25.7 (11.7) cm, p (ns). Four developed symptoms of LAI and underwent a Duplex scan which confirmed a damped waveform in the LSA and retrograde flow in the left vertebral artery. All were treated conservatively and none required CSB. Ten had a patent LSA on duplex imaging with seven occlusions but all 17 showing retrograde flow in the left vertebral artery. The remaining three were not imaged (two AT and 1 TAAA) as they died at three days, four weeks and six weeks following TEVAR. Hence, 53 of 98 (54%) underwent TEVAR with at least one the major supra-aortic branches covered.
Overall mortality rates (</>30 days after TEVAR)
Ten (10%) of the 98 patient cohort died within 30 days of the TEVAR (Table 6). Five of these underwent TEVAR for AT and died from associated non-aortic traumatic injuries. Of the other five, one developed a retrograde type A AD following TEVAR with two having myocardial infarctions and one a ruptured TAAA. The other patient died with respiratory failure. Thirty-seven died more than 30 days after TEVAR with 28 having a TEVAR for TAAA.
Early and late mortality rates for those undergoing TEVAR according to aortic pathology and extra-anatomical bypass (brackets).
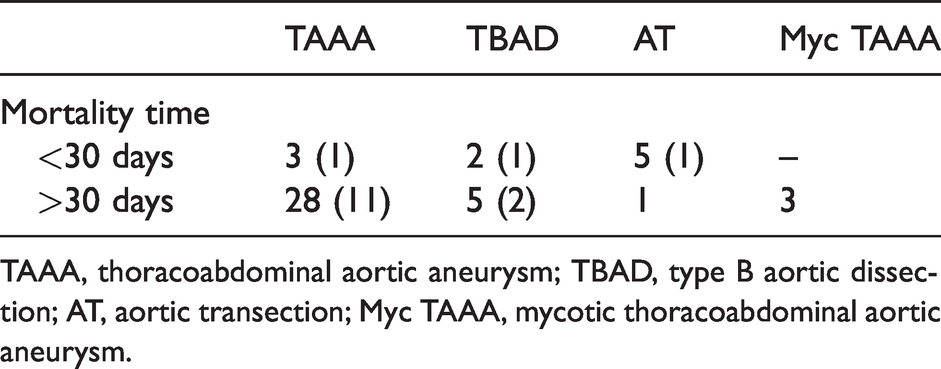
TAAA, thoracoabdominal aortic aneurysm; TBAD, type B aortic dissection; AT, aortic transection; Myc TAAA, mycotic thoracoabdominal aortic aneurysm.
Discussion
This study has two important clinical findings. First, coverage of the LSA when no revascularisation is performed is a well-tolerated procedure as far as significant LAI is concerned. Second, the length of thoracic aortic lumen coverage was significantly longer in those who developed SCI following TEVAR when compared to those who were symptom-free. Also, delayed onset SCI (when treated expeditiously) has a better prognosis as compared to those who developed immediate symptoms and signs of lower limb SCI. 9 However, it may be difficult to conclusively determine whether SCI has occurred periprocedurally or early in the postoperative period. The two patients who developed immediate SCI were performed under general anaesthesia and extubated within 24 h following TEVAR. Other perioperative parameters such as hypotension and anaemia rather than extensive thoracic aortic coverage may be a significant factor in causing SCI. 10 The three others with SCI had symptoms which were temporary and completely resolved with simple elevation of the blood pressure.
The balance between maintaining adequate arterial perfusion of the spinal cord and the development of SCI (however significant) is difficult to assess prior to TEVAR. Optimum blood flow to the upper spinal cord, despite occlusion of the LSA, is dependent on the recruitment of collateral branches to maintain perfusion pressure. Coverage of longer sections of the thoracic aorta may reduce the ability to collateralise (particularly when previous AAA repair may have been performed) and maintain adequate spinal perfusion.11,12 However, if the LSA is occluded without revascularisation, adjunctive measures such as treating hypovolaemia, raised venous pressures and hyperpyrexia excellent outcomes may be observed.13,14 In this series, one patient developed early onset SCI following TEVAR for a TBAD. The LSA was not revascularised at the time of TEVAR, despite 35 cm length of thoracic aortic coverage. Possibly due to early intercostal artery thrombosis, SCI occurred within five days but following CSB the symptoms permanently resolved. Other centres have reported delayed onset of SCI after TEVAR which was successfully treated by CSB.15,16 Similar to this series, one occurred in TBAD where later onset spinal artery thrombosis may have been the cause of the late presentation. 15
Safe lengths of aortic coverage before adjunctive measures are required range from 20 to 40 cm though no definitive minimum measurements have been proposed.5,17,18 Although the length of thoracic aortic coverage by itself is a risk factor for development of SCI, others have shown the specific location of coverage by a stent within the aortic lumen is an important consideration. This is related to vital arterial branches arising from the aorta. The significance of spinal perfusion from the aortic branches at T8 to T12 has also been proposed as an independent risk factors when covered. 19
Four (17%) patients developed symptoms related to LAI following LSA coverage but none required immediate intervention. All presented clinically between 6 and 12 days post TEVAR. The presentation was invariably ‘soft’ signs and included intermittent blue discolouration of the fingertips or a cool periphery where revascularisation was not necessary. A further four required delayed CSB for LAI after TEVAR with all showing retrograde flow in the left vertebral artery with damped LSA waveform with the earliest presentation being two days after TEVAR.
The incidence of LAI following TEVAR requiring proximal coverage in PLZ 2 is difficult to determine. The development of stroke and SCI is possibly considered a more important clinical entity due to the long-term consequences and poor outcomes if not treated expeditiously. Furthermore, as seen in this series, presentation of LAI can be non-specific such as a cool or pale hand with motor function largely preserved. Hence, there may be a general tendency to initially treat these conservatively as significant improvement is usually observed. A combination of SCI and LAI was not seen in this series.
Guidelines as to who should undergo LSA revascularisation prior to TEVAR were published in 2009. 7 Indications for ‘routine’ LSA revascularisation include a dominant left vertebral artery, a patent left internal mammary artery graft used for a coronary artery bypass, a functioning arterio-venous fistula for dialysis and previous abdominal aortic aneurysm repair. Other indications included IIA occlusion, stent grafts deployed over greater than 20 cm of the thoracic aorta and also anomalous origin of the left vertebral artery from the aortic arch whereby coverage would be unavoidable following TEVAR. These guidelines have remained unrevised since 2009 but there are more recent publications both for and against routine revascularisation of the LSA during TEVAR. It seems routine LSA revascularisation for every patient pre TEVAR is not necessary as the majority tolerate coverage of the LSA with little effect.
It is therefore difficult to be certain as to how many patients require routine revascularisation of the LSA during TEVAR. There is evidence to suggest unnecessary CSB can be prevented in more than 80% of cases when strict selection criteria is adhered to. 20 Even if a procedural policy is adopted where all TEVAR cases undergo LSA revascularisation, there are inevitably perioperative risks associated with left CSB. Primarily these involve the thoracic duct which terminates at the jugular vein and also the phrenic nerve which is sensitive to even gentle mobilisation and palsies remain not uncommon. 21 The method of LSA revascularisation needs to be considered as to whether a CSB or even LSA transposition be performed. The aim is to maintain antegrade left vertebral flow and whichever method used the LSA must be ligated proximal to the origin of this vessel.
The principal limitations of this series are a relatively small number of patients treated and followed up over a 20-year period. Also, transections account for one-fifth of the indications for TEVAR which invariably mean a younger subgroup of patients who might be expected to tolerate occlusion of the LSA without revascularisation better than those with dissections or aneurysms. However, this vascular unit is the sole provider of TEVAR for the country with a population of little over three million.
This series has shown the length of coverage of the thoracic aorta is a factor in the development of SCI occurring. If the LSA origin is not covered, this has no effect on the perfusion of the left arm but may compromise spinal cord perfusion particularly if >20 cm of the aorta is covered. If the LSA is covered, this may reduce perfusion to the left arm as well as compromising the blood flow to the upper spinal cord (if CSB is not performed). However, it must be realised other factors may also contribute to this development and includes the underlying thoracic pathology being treated and associated comorbidities. Possibly the most important factor is prior open aortic surgery with a graft or endovascular techniques which may reduce any reserve for spinal cord perfusion should a further section be covered – particularly if this exceeds 20 cm.
Conclusion
In this series of 98 patients undergoing TEVAR, 29 underwent an extra-anatomical bypass. Five were performed at least 48 h post TEVAR for delayed symptoms and signs of LAI and SCI. However, coverage of the LSA is generally well tolerated in terms of development of LAI. Delayed LSA was predominantly required for chronic arm ischaemia compared to SCI. The length of thoracic aorta covered is a factor in the development of SCI. Elective CSB should be considered for certain patients undergoing TEVAR (particularly if greater than 20 cm of thoracic aorta is covered).
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Not applicable.
Informed consent
Not applicable.