
Abstract
Introduction
Creatine (α-methyl-guanidinoacetic acid) is regraded as a conditionally essential nutrient, sourced exclusively from animal-based foods. It primarily functions as a key compound in replenishing cellular phosphagen energy stores (Ostojic and Forbes, 2022). Adequate creatine consumption appears beneficial across the lifespan and in various conditions (for a detailed review, see Balestrino and Adriano, 2019 and Ostojic, 2021a), with extensive data confirming its safety in human nutrition (Kreider et al., 2022). Still, the potential links between creatine and carcinogenesis remain unclear, with studies suggesting that creatine may possess both cancer-suppressive and cancer-promoting properties (Zhang and Bu, 2022). Several reports suggest potential cytotoxic effects of creatine, possibly due to its role in facilitating the formation of food-borne chemical carcinogenic compounds such as heterocyclic amines (HCAs) (Overvik et al., 1989), acrylamide (Yaylayan et al., 2004), and formaldehyde (Yu and Deng, 2000). For example, creatine is suggested to be a major dietary constituent involved in the formation of HCAs through the Maillard reaction during the thermal processing of protein-containing foods, such as meat and dairy products (Gibis, 2016). A preliminary small-scale human study indicated that creatine itself was not the primary nutritional factor responsible for the formation of HCAs (Pereira et al., 2015). However, no studies have yet examined whether creatine intake is associated with HCAs and other carcinogens in the general population. This cross-sectional study aims to investigate the relationship between creatine consumption and various carcinogenic biomarkers in blood and urine among individuals aged 18 years and older, utilizing data from the 2013–2014 National Health and Nutrition Examination Survey (NHANES).
Methods
The NHANES is a cross-sectional survey research program conducted annually by the National Center for Health Statistics, starting in 1999, to assess the health and nutritional status of children and adults in the United States. The NHANES integrates interviews, physical examinations, and laboratory tests among the noninstitutionalized civilian resident population. Since only the NHANES 2013–2014 round included laboratory data on all relevant carcinogenic concentrations (HCAs, acrylamide, and formaldehyde), this paper exclusively examined the population from that cycle. We extracted data for participants aged 18 years and older who provided dietary intake information and underwent laboratory tests measuring at least one carcinogenic biomarker. Daily creatine intake was assessed using the Dietary Data databases, which were compiled from individual in-person 24-h food recall interviews. The calculation was based on the average creatine content found in various creatine-rich sources, such as meat and dairy, as described previously (Todorovic et al., 2023). Total daily intake did not include creatine obtained from dietary supplements or pharmacological sources. The concentrations of carcinogenic compounds were extracted from NHANES 2013–2014 Laboratory Data database. Blood hemoglobin adducts of acrylamide, glycamide (the primary metabolite of acrylamide), and formaldehyde were measured by high-performance liquid chromatography coupled with tandem mass spectrometry (LC/MS/MS). The lower limits of detection (LLOD) were 3.90 pmol/g Hb for acrylamide, 4.90 pmol/g Hb for glycamide, and 0.67 nmol/g Hb for formaldehyde. Heterocyclic amines in urine were measured by an isotope-dilution high-performance liquid chromatography/electrospray ionization tandem mass spectrometry. Briefly, urine samples were fortified with internal standards and hydrolyzed under basic conditions at 70°C for 5 h. The samples were then subjected to solid-phase extraction, followed by elution and analysis via LC/MS/MS. Analyte-specific ion transitions were monitored for quantification, confirmation, and internal standards, respectively. Concentrations were determined by comparing the ratios of native to isotope-labeled ions in the samples against standard curves. A total of 10 HCAs were detected, including 2-Amino-9H-pyrido[2,3-b]indole (A-a-C, LLOD 0.62 pg/mL), 2-Amino-6-methyldipyrido[1,2-a:3’,2'-d]imidazole (Glu-P-1, LLOD 0.31 pg/mL), 2-Aminodipyrido[1,2-a:3’,2'-d] imidazole (GLU-P-2, LLOD 0.83 pg/mL), 1-Methyl-9H-pyrido[3,4-b]indole (Harman, LLOD 4.59 pg/mL), 2-Amino-3-methyl-3H-imidazo[4,5-f]quinoline (IQ, LLOD 0.37 pg/mL), 2-Amino-3-methyl-9H-pyriodo[2,3-b]indole (MeA-a-C, LLOD 0.33 pg/mL), 9H-Pyrido[3,4-b]indole (Norharman, LLOD 12.6 pg/mL), 2-Amino-1-methyl-6-phenylimidazo[4,5-b]pyridine (PhIP, LLOD 0.34 pg/mL), 3-Amino-1,4-dimethyl-5H-pyrido[4,3-b]indole (Trp-P-1, LLOD 0.79 pg/mL), and 1-Methyl-3-amino-5H-pyrido[4,3-b]indole (Trp-P-2, LLOD 0.63 pg/mL). Detailed information on laboratory methods used is available elsewhere (National Center for Health Statistics, 2019). Additionally, we examined the NHANES 2013–2014 Demographics Data, Dietary Data, Examination Data, and Laboratory Data components to obtain information regarding participants’ characteristics relevant to the study. All files were merged using respondent sequence numbers and subsequently analyzed. Ethical approval for the NHANES 2013–2014 round was granted by the US National Center for Health Statistics Research Ethics Review Board (Continuation of Protocol # 2011–2017), and informed consent was obtained from all respondents. Extreme outliers for total creatine intake and carcinogenic biomarkers were identified using the 3×IQR rule (Hubert and Van der Veeken, 2008) and excluded from further analysis. Linear regression analyses were performed to explore the association between dietary creatine intake and carcinogenic biomarkers, with unstandardized (B) and standardized (β) regression coefficients reported in the results. The regression models were adjusted for a predetermined set of covariates, including biomarkers of creatine turnover (Model 1: serum and urinary creatinine), demographics (Model 2: gender, age at screening, race/ethnicity, education level, annual household income, body mass index, smoking status, sedentary activity), and nutritional variables (Model 3: energy, protein, total free sugars, total fat, alcohol). Serum creatinine was measured using the Jaffee method (Beckman UniCel DxC800 Synchron, Brea, CA), while urinary creatinine was determined enzymatically (Cobas 6000 Analyzer, Roche Diagnostics, Indianapolis, IN). Relevant demographic and nutritional covariates that may contribute to carcinogen formation were identified from previous studies (Chen et al., 2020; Oz et al., 2023). Data analysis was performed using SPSS Statistics for Mac (Version 24.0), with a significance level set at p ≤ 0.05.
Results
The final analysis included 1763 adult respondents, of whom 907 (51.4%) were female. Table 1 illustrates the characteristics of the study sample. Creatine was sourced from meat and meat products by 1481 participants (84.0%), while dairy served as a source for 1153 participants (65.4%). A total of 32 participants (5.2%) reported no consumption of creatine-containing foods. The mean daily creatine intake was 0.83 ± 0.77 grams (95% CI, ranging from 0.80 to 0.87).
Characteristics of the study participants.
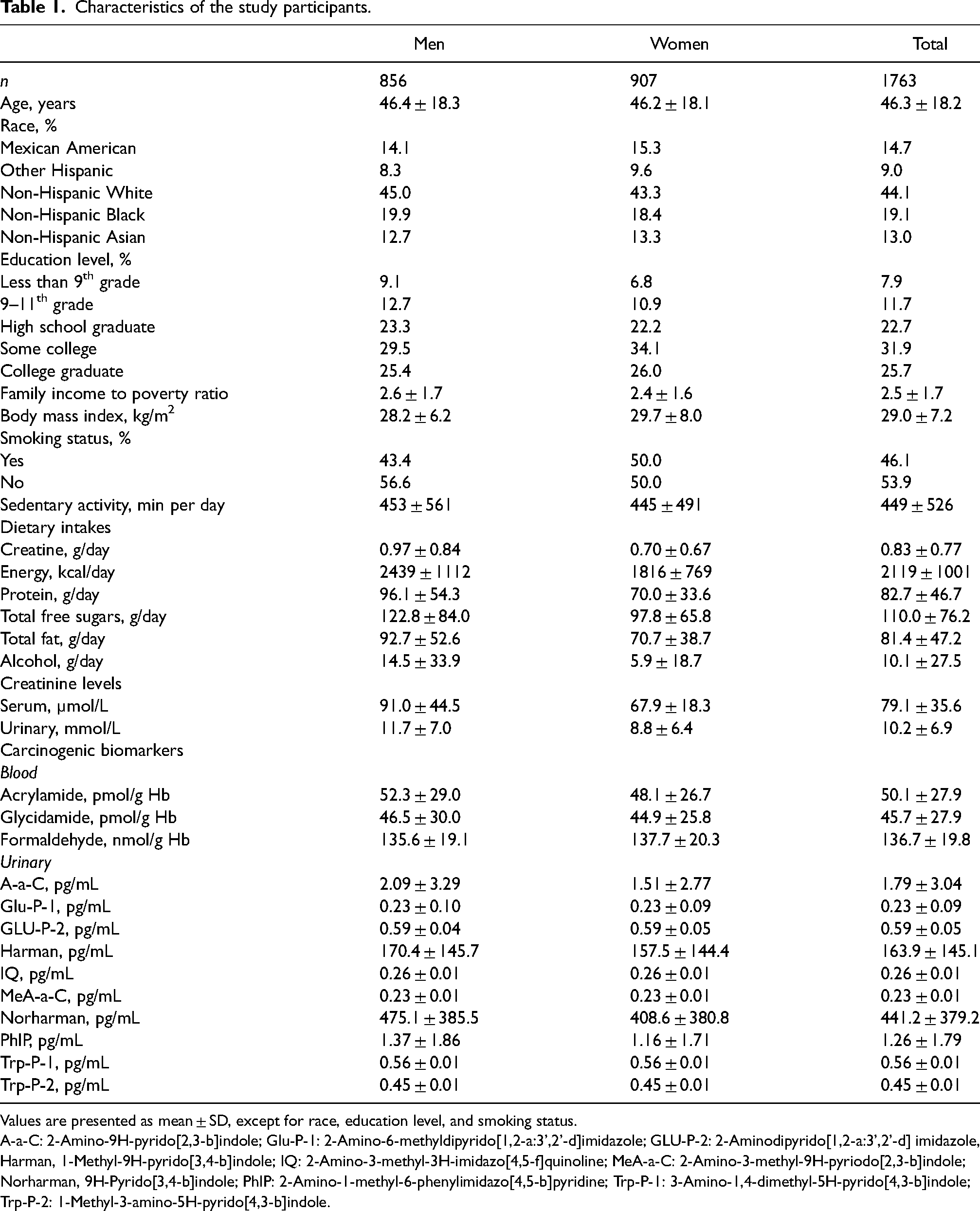
Values are presented as mean ± SD, except for race, education level, and smoking status.
A-a-C: 2-Amino-9H-pyrido[2,3-b]indole; Glu-P-1: 2-Amino-6-methyldipyrido[1,2-a:3’,2'-d]imidazole; GLU-P-2: 2-Aminodipyrido[1,2-a:3’,2'-d] imidazole, Harman, 1-Methyl-9H-pyrido[3,4-b]indole; IQ: 2-Amino-3-methyl-3H-imidazo[4,5-f]quinoline; MeA-a-C: 2-Amino-3-methyl-9H-pyriodo[2,3-b]indole; Norharman, 9H-Pyrido[3,4-b]indole; PhIP: 2-Amino-1-methyl-6-phenylimidazo[4,5-b]pyridine; Trp-P-1: 3-Amino-1,4-dimethyl-5H-pyrido[4,3-b]indole; Trp-P-2: 1-Methyl-3-amino-5H-pyrido[4,3-b]indole.
Model 1 revealed no significant relationship between daily creatine intake and most carcinogenic biomarkers, except for a significant correlation between creatine intake and acrylamide levels (B = −3.999, ß = −0.088, p = 0.05) (Table 2). This indicates that participants consuming more creatine had lower levels of circulating acrylamide after adjusting for biomarkers of creatine turnover. Model 2 (demographics) confirmed a significant relationship between daily creatine intake and circulating acrylamide (B = −3.490, ß = −0.077, p = 0.02), as well as for blood levels of glycidamide (B = −2.992, ß = −0.068, p = 0.05) and urinary PhIP (B = 0.190, ß = 0.088, p = 0.03). However, no correlation between creatine consumption and any carcinogenic biomarkers remained significant after adjusting for nutritional factors (Model 3).
Association between dietary creatine intake and carcinogenic biomarkers.
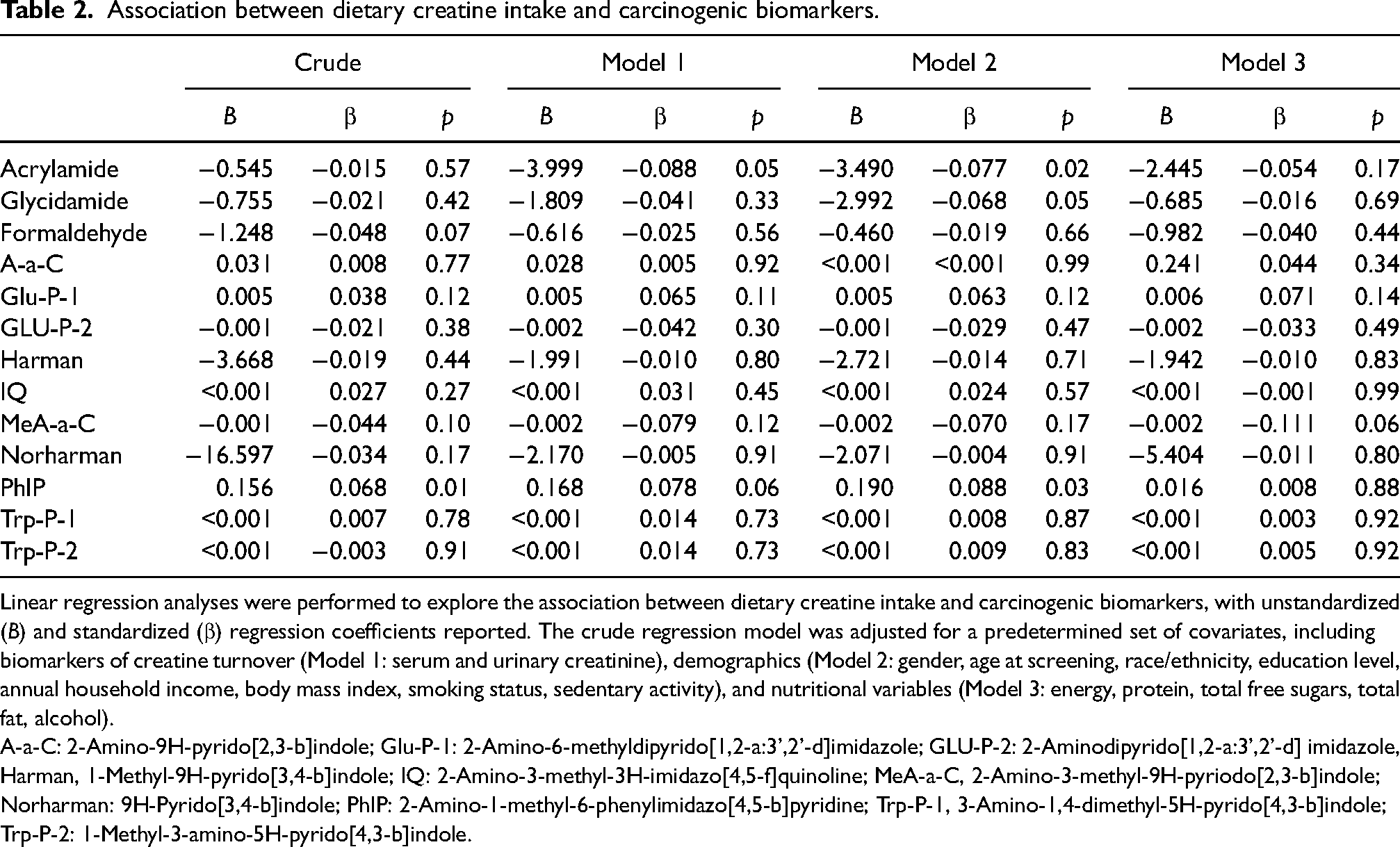
Linear regression analyses were performed to explore the association between dietary creatine intake and carcinogenic biomarkers, with unstandardized (B) and standardized (β) regression coefficients reported. The crude regression model was adjusted for a predetermined set of covariates, including biomarkers of creatine turnover (Model 1: serum and urinary creatinine), demographics (Model 2: gender, age at screening, race/ethnicity, education level, annual household income, body mass index, smoking status, sedentary activity), and nutritional variables (Model 3: energy, protein, total free sugars, total fat, alcohol).
A-a-C: 2-Amino-9H-pyrido[2,3-b]indole; Glu-P-1: 2-Amino-6-methyldipyrido[1,2-a:3’,2'-d]imidazole; GLU-P-2: 2-Aminodipyrido[1,2-a:3’,2'-d] imidazole, Harman, 1-Methyl-9H-pyrido[3,4-b]indole; IQ: 2-Amino-3-methyl-3H-imidazo[4,5-f]quinoline; MeA-a-C, 2-Amino-3-methyl-9H-pyriodo[2,3-b]indole; Norharman: 9H-Pyrido[3,4-b]indole; PhIP: 2-Amino-1-methyl-6-phenylimidazo[4,5-b]pyridine; Trp-P-1, 3-Amino-1,4-dimethyl-5H-pyrido[4,3-b]indole; Trp-P-2: 1-Methyl-3-amino-5H-pyrido[4,3-b]indole.
Discussion
This is arguably the first population-based study to examine the relationship between dietary creatine intake and relevant carcinogenic biomarkers (acrylamide, glycidamide, formaldehyde, HCAs) in humans. Our findings indicate no correlation between creatine consumption, excluding dietary supplements, and carcinogenic biomarkers measured in the blood and urine of the U.S. adults after adjusting for biomarkers of creatine turnover, key demographic factors, and nutritional variables. Therefore, the consumption of dietary creatine may be considered safe and not associated with increased levels of these carcinogens.
The notion that creatine may induce carcinogenesis largely stems from a handful of opinion articles, review papers (Wyss and Kaddurah-Daouk, 2000; Brudnak, 2004), and food processing studies (Felton et al., 1994; Murkovic and Pfannhauser, 2000), suggesting a potential role of this compound in the generation of chemical toxicants with carcinogenic potential in cooked meat and dairy. Creatine, alongside amino acids, glucose, nitrogenous bases, and nucleosides, serves as the primary chemical precursor required for the generation of HCAs during food preparation (Chen et al., 2002), and N-methylacrylamide through the acrylic acid pathway (Yaylayan et al., 2004). Additionally, creatine can be metabolized to methylamine, which is further converted to formaldehyde by semicarbazide-sensitive amine oxidase (Yu and Deng, 2000). These creatine-derived chemicals are recognized as hazardous, with acrylamide categorized as probably carcinogenic to humans (Group 2A) and several HCAs as possibly carcinogenic to humans (Group 2B) by the International Agency for Research on Cancer (International Agency for Research on Cancer, 2024). However, whether dietary creatine consumption affects the levels of these carcinogens in vivo has been poorly addressed in human trials so far. To our knowledge, only a single small-scale human trial evaluated the effects of creatine consumption on blood and urinary production of selected carcinogens (Pereira et al., 2015). The authors from the University of Sao Paulo demonstrated that both short- and medium-term creatine intake does not significantly contribute to the formation of four HCAs, including PhIP, 2-amino-3,8-dimethylimidazo[4,5-f]quinoxaline (8-MeIQx), 2-amino-(1,6-dimethylfuro[3,2-e]imidazo[4,5-b])pyridine (IFP), and 2-amino-34,8-trimethylimidazo[4,5-f]quinoxaline (4,8-DiMeIQx), indicating no contribution of creatine to HCAs formation in healthy men and women (Pereira et al., 2015). Our data align with this study and extend previous research by utilizing a population-based approach, a larger sample size, a more extensive profile of carcinogenic biomarkers, and controlling for a range of confounding variables. We found that consuming creatine was not associated with elevated circulating and urinary concentrations of 13 different carcinogenic biomarkers in adult men and women when controlled for relevant covariates that may contribute to creatine turnover and carcinogen formation. Interestingly, consuming more creatine tended to be nonsignificantly associated with reduced levels of urinary MeA-a-C (p = 0.06), with each additional gram of creatine reducing MeA-a-C levels by 0.002 pg/mL. MeA-a-C ranks among the most prevalent HCAs detected in grilled or pan-fried meat, showing carcinogenicity in preclinical studies and the ability to form covalent DNA adducts in vitro and in vivo (Pfau et al., 1997). Notably, creatine may exert a mild suppressive effect on the accumulation of this carcinogenic compound. This secondary finding aligns with prior investigations involving clinical patients (Norman et al., 2006: Lønbro et al., 2013) and the general population (Ostojic et al., 2023), which suggest a potential cancer-protective effect of dietary creatine. Our findings, along with other human trials, challenge the long-standing notion that dietary creatine increases cancer risk by stimulating the formation of carcinogenic compounds. Instead, creatine warrants scrutiny as a potential cancer-protective nutrient.
Our study has several limitations that need to be considered. These include the cross-sectional design, which precludes establishing cause−effect relationships; reliance on self-reported data for assessing creatine intake; limited utility of single-sampled blood and urine assessments for reflecting long-term carcinogenic concentrations; failure to account for additional factors that could potentially influence the association between creatine and carcinogens (e.g., variations in creatine content across different foods, cooking temperatures, cooking durations, the use of flavorings that could mitigate the formation of HCAs, and other foods and food preparations that could affect HCA formation); and the absence of additional molecular biomarkers of carcinogenesis (such as chromosomal abnormalities, targeted sequence mutations, gene fusions, or DNA methylation). For this study, we decided not to include creatine intake from supplements, as they are infrequently used among the general population, with the one-week prevalence of supplemental creatine use in the adult U.S. population estimated to be 0.9% (Kaufman et al., 2002). Additionally, we did not included kidney failure as a covariate, despite its potential impact on urinary creatine excretion, because its prevalence is below 5% in the general population (Ostojic, 2021b). Further studies are required to validate our findings and potentially expand them to long-term, well-sampled, longitudinal randomized controlled trials involving different cohorts, including those with a higher risk of cancer. Ideally, monitoring creatine intake and carcinogenic biomarkers alongside cancer mortality, incidence, and survival rates would furnish much-needed evidence to advance our understanding of the safety of this nutrient.
Conclusion
The consumption of dietary creatine does not correlate with the blood and urinary concentrations of HCAs, acrylamide, and formaldehyde, after adjusting for relevant variables in adult U.S. population. These results indicate that creatine consumption may be deemed safe and not linked to elevated levels of these carcinogens in the general population.
Footnotes
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: State: - SMO serves as a member of the Scientific Advisory Board on Creatine in Health and Medicine (AlzChem LLC). SMO co-owns patent “Supplements Based on Liquid Creatine” at the European Patent Office (WO2019150323 A1) and patent application “Composition Comprising Creatine for Use in Telomere Lengthening” at the U.S. Patent and Trademark Office (# 63/608,850). SMO has received research support related to creatine during the past 36 months from the Serbian Ministry of Education, Science, and Technological Development; Provincial Secretariat for Higher Education and Scientific Research; AlzChem GmbH; ThermoLife International; and Hueston Hennigan LLP. SMO does not own stocks and shares in any organization. SB and EG declare no known competing financial interests or personal relationships that could have appeared to influence the authorship of this paper.
Authors' contributions
SB: Data curation; Formal analysis; Investigation; Methodology; Visualization; Writing-review and editing. EG: Investigation; Methodology; Writing-review and editing. SMO: Conceptualization; Data curation; Formal analysis; Investigation; Methodology; Visualization; Writing-original draft; Writing-review and edit.
Ethical approval
The ethical approval was granted by the U.S. National Center for Health Statistics Ethics Review Board (Continuation of Protocol # 2011-17). Consent to participate statement: Written informed consent was obtained from all respondents to participate in the study. The research was conducted ethically following the World Medical Association Declaration of Helsinki.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.