
Abstract
Shared medical decision making is a collaborative process that allows patients and providers to make health care decisions together, taking into account medical evidence, patient’s values, and preferences. 1 Shared medical decision making is often viewed as an intermediate between paternalistic and consumeristic approaches. 2 In a paternalistic style, the provider makes decisions for the patient balanced between what they consider to be the optimal treatment and their perception of the patient’s values and desires. In a consumeristic decision style, the patient directs their care; the provider’s role is to provide information and fulfill patient care requests.
Although patients vary in their preferences for making decisions,3,4 most prefer shared decision making, followed by consumerism; less than 10% prefer paternalistic styles.5–9 Patients preferring paternalism tend to be older.9,10 Most patients report that their doctor matches their preferred style of decision making.6,7 Concordance between patient decision-making style preference and perception of degree of decision making experienced has been associated with higher patient satisfaction. 11 Higher income and having a regular doctor who is perceived as being excellent are associated with a higher likelihood of experiencing the patient’s preferred decision-making style. 7
On the other hand, physicians report that paternalism is their most common approach. 12 One study of medication decision making using videotapes suggested that both physicians and patients overestimated the degree of shared decision making. 13 A systematic review of studies assessing providers’ views of decision making showed that common barriers to shared decision making include time pressures and lack of perceived applicability due to patient circumstances, whereas facilitating factors include provider motivation, attitude, and belief that it will improve patient outcomes. 14
Numerous observational studies have examined the nature of shared medical decision making. A systematic review of 33 studies found that provider use of shared medical decision making was inconsistent and that, in general, few providers engaged patients in shared medical decision making. 15
Our study’s purpose was to triangulate patients’ preferred style of decision making with patient preferences using patient and clinician postencounter reports as well as objective measures of communication and to assess the impact of shared decision making on patient-centered outcomes.
Methods
This study uses direct observation of audiotaped patient encounters and periencounter surveys of patients and physicians from a randomized trial designed to improve medical decision making (NCT01606930); full details are reported elsewhere. 16 Our study sample was powered to demonstrate a clinically meaningful improvement in adherence to hypertensive medications. Adult patients presenting for routine primary care at Walter Reed Army Medical Center, with an established primary care relationship (defined as at least 2 visits in the previous year with the same physician) and at least 3 comorbid medical conditions, were eligible to participate. We surveyed patients before the visit, immediately after the visit, and at 4 weeks after the visit. Previsit surveys assessed their expectations for care, 17 functional status (Medical Outcomes Study SF6), 18 level of stress, somatization (Patient Health Questionaire-15), 19 mood and anxiety disorders (PRIME-MD), 20 pain severity (0–10 scale), adherence (using both a pill count and the Morisky scale 21 ), literacy, 22 and health locus of control 23 using validated measures. Blood pressure was measured by our research personnel, with participants seated for 5 min before the first of 3 measurements, each taken 5 min apart, using the average of these measurements.
In addition, patients were asked to provide their preferred style of shared decision making about new and ongoing medical problems (Figure 1) using a validated visual analog scale (VAS). 2 This instrument is anchored at one end with the doctor making all the decisions, in the middle with decision making equally shared, and at the other with the patient making all the decisions. We measured the point at which the patient marked the VAS and converted that value to a 0- to 20-point scale with the beginning of the scale (doctor makes all the decisions) given a value of 0, the middle a 10 (doctor explains options, asks what I think, and we equally share in making decisions), and a 20 at the end (doctor explains options and I make all the decisions).
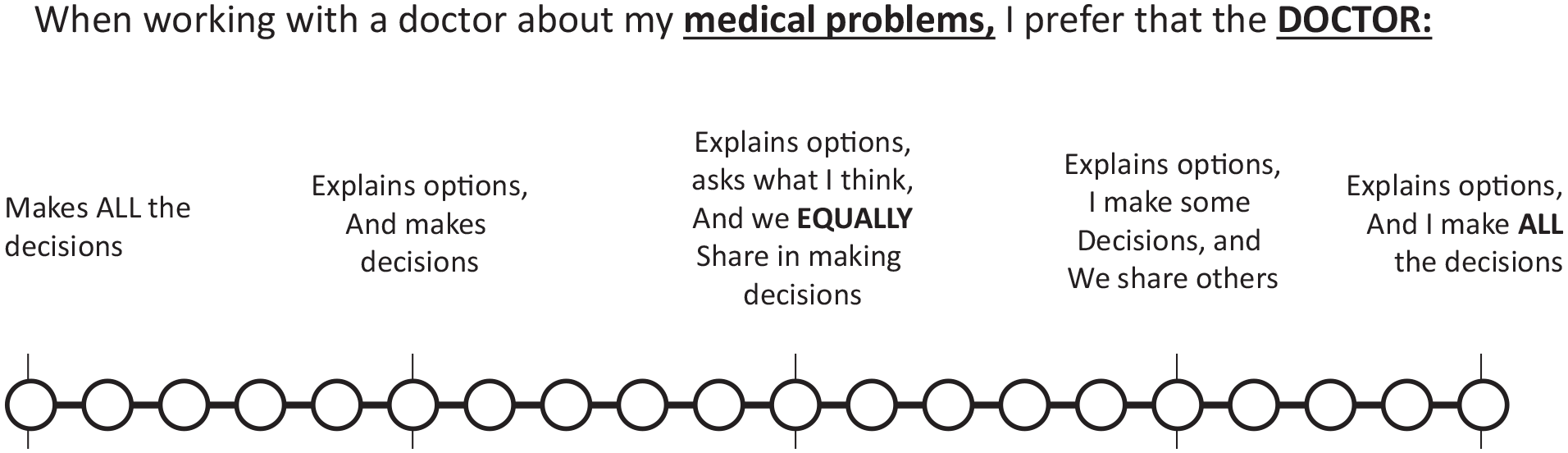
Shared medical decision question.
Immediately after the visit, patient surveys assessed the degree of shared decision making they experienced during the encounter (using the same scale as before the visit), patient satisfaction (Rand-9 item survey), 24 and trust (Trust in Clinician 7-item instrument). 25 Immediately after each visit, physicians rated how difficult the encounter was (Difficult Doctor Patient Relationship Questionnaire) 26 and rated the amount of shared decision making that occurred during the encounter using the same scale as the patient.
Patients were seen 1 month after the visit, when blood pressure was remeasured and medication adherence was assessed using pill counts and the Morisky instrument. 16 In addition, patient surveys at 4 weeks assessed functional status, stress, pain, and trust. Patients at this site are similar to community patients in terms of their demographics 27 and case mix of medical conditions, including rates of mental disorders. 28
Visits were audiotaped, transcribed, stripped of personal identifiers, and coded. We coded decisions as basic, intermediate, or complex, following the method of Braddock (Table 1). 29 Basic decisions were those that had minimal effect on the patient, minimal medical controversy, and clear, simple outcomes (e.g., basic laboratory evaluations or timing of follow-up). Intermediate decisions had a moderate effect on patients, with broad consensus and moderately uncertain outcomes (e.g., starting a new medication). Complex decisions had extensive effects on the patient, with medically controversial and uncertain outcomes (e.g., prostatic specific antigen testing).
Categorization of Decision Complexity

We assessed the quality and degree of shared medical decision making using OPTION-5.30,31 We assessed the interactive nature of communication using the Roter Interactive Assessment System (RIAS). 32 RIAS codes patient-provider communication in 26 mutually exclusive and comprehensive categories of communicative interactions. Coding was done in duplicate (RIAS: D.B., J.L.J., OPTION-T: D.S., J.L.J.) with good interrater reliability (intraclass correlation coefficient: RIAS: 0.86, OPTION-5: 0.83).
All participants (both physicians and patients) provided informed consent, and this study was approved by the Walter Reed Institutional Review Board. We followed STROBE guidelines in reporting our outcomes. 33 We calculated the difference between the patient’s previsit desire for shared medical decision making and their postvisit report of the decision-making experience as well as the difference between patient and physician reports of experienced shared decision making. We defined differences of more than 4 points to be clinically significant, as this was 2 standard deviations different from the mean. We transformed the patient and provider ratings of shared medical decision making by taking the squared difference between the midpoint (“perfectly shared”) and the rated values and used linear regression to correlation OPTION-5 ratings with patient ratings. Univariate comparisons were done using either Student’s t tests or chi-square, and multivariate comparisons were performed using either linear or logistic regression. For multivariate comparisons, we adjusted for clustering on physicians. Interrater reliability was done using intraclass correlation coefficients. All analyses were performed using STATA (v 15.2, College Station, TX).
Results
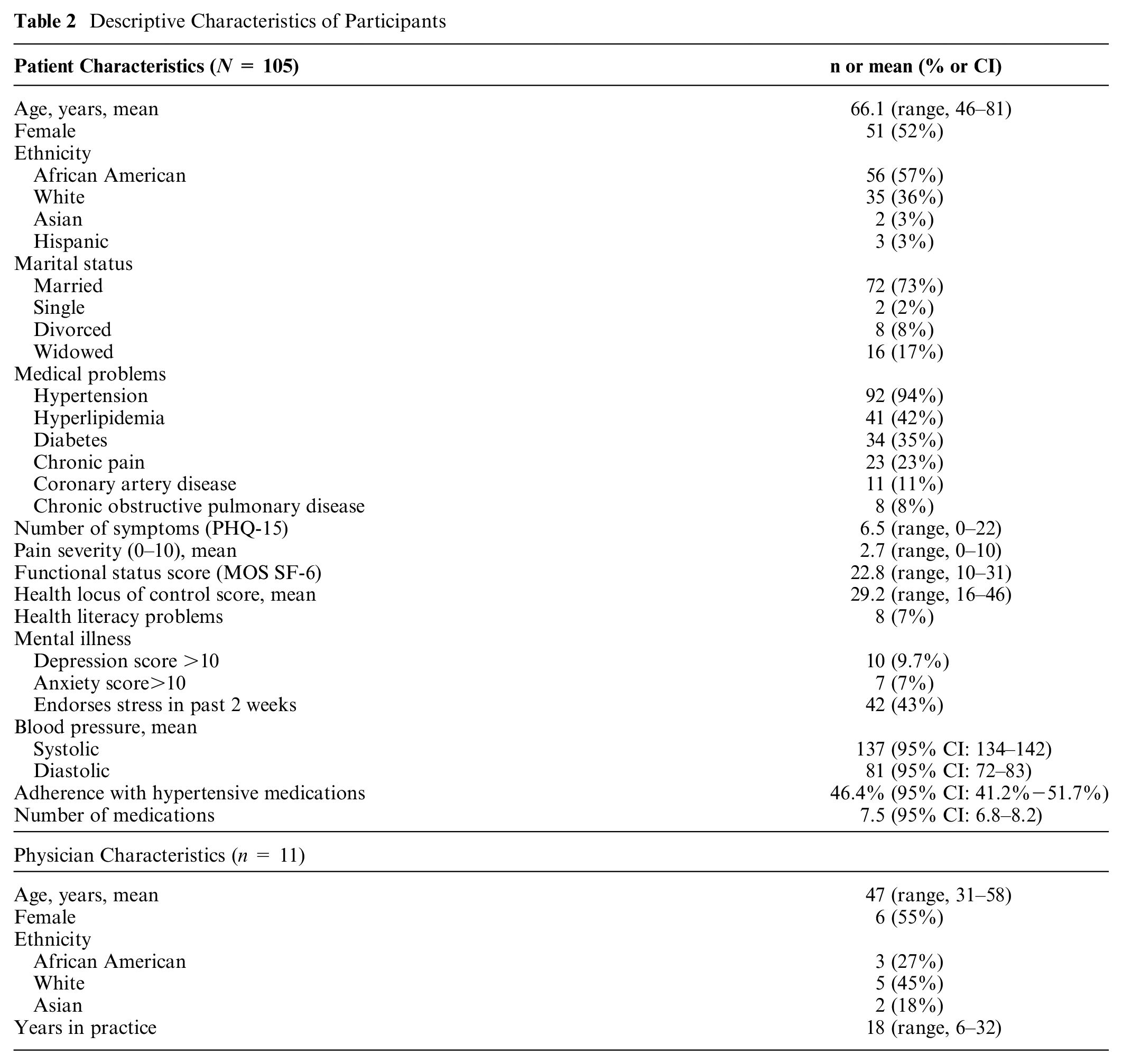
One hundred five patients, averaging 65.9 years (53% female, 57% black, 36% white) participated. The most common medical problems were hypertension, hyperlipidemia, and diabetes (Table 2). Patients were taking on average 7.5 daily medications; fewer than half (46.4%) were fully adherent to them. Nearly 10% screened positive for major depression and 7% for an anxiety disorder. Seven percent reported literacy problems, and most reported an external locus of control for health problems. On average, participating physicians saw 10 study patients. Physicians were mostly white (45%), averaged 47 years of age, and had been practicing for 18 years (range, 6–32 years; Table 2). Visits averaged 29 min in duration.
Descriptive Characteristics of Participants
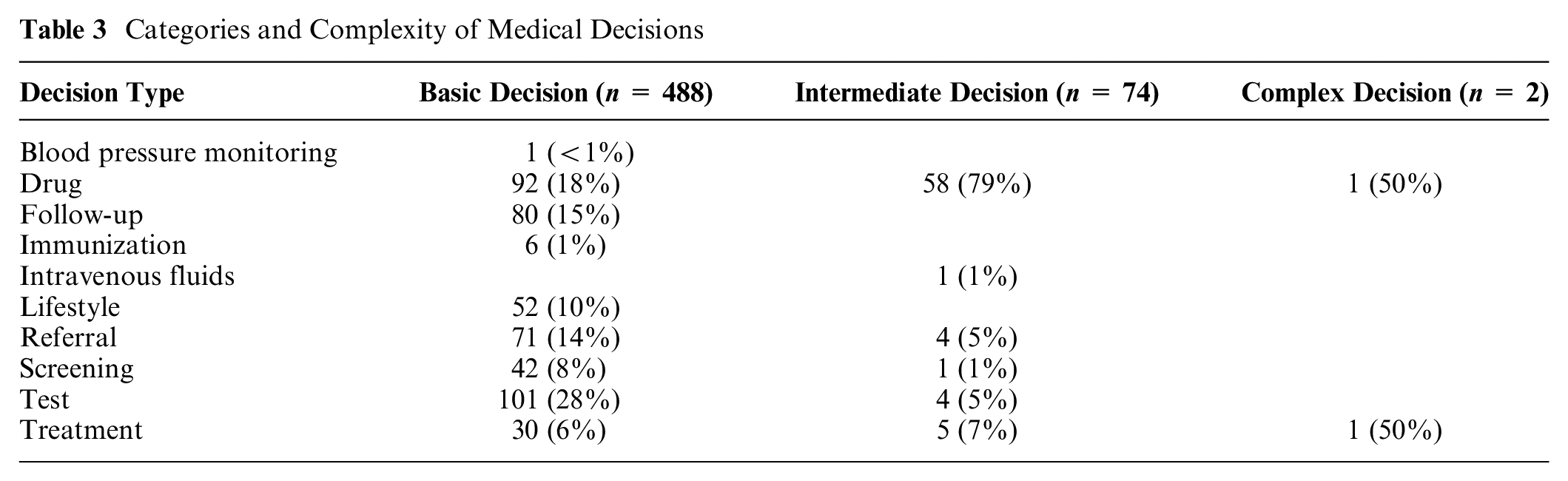
Overall, we observed 598 decisions, with an average of 7.4 decisions per visit (range, 1–15). Common decision types included diagnostic tests (26%), medications (25%), follow-up (13%), referrals (13%), lifestyle changes (9%), and nonpharmacologic treatments (6%). Most medical decisions (97%) involved chronic medical problems and were classified as basic decisions (87%). Seventy-four decisions (12%) were intermediate, and only 2 (<1%) decisions were coded as complex (Table 3).
Categories and Complexity of Medical Decisions
Patient Outcomes at Four Weeks

Before the visit, 54% of patients expressed a desire for equally shared medical decision making, 24% desired that doctors dominate decision making, and 18% preferred that they make all the decisions (Figure 2). On a 0- to 20-point scale, where 10 is perfectly shared decision making, the patient’s mean score was 9.9 (3.6) for “old problems” and 9.6 (SD 3.2) for “new problems.” There was no difference in the desire for shared decision making between “old” and “new” problems (P = 0.28). The preferred decision-making style did not differ by age (P = 0.67), gender (P = 0.13), ethnicity (P = 0.58), health literacy (P = 0.37), underlying mental disorders (P = 0.63), or locus of control (P = 0.63).
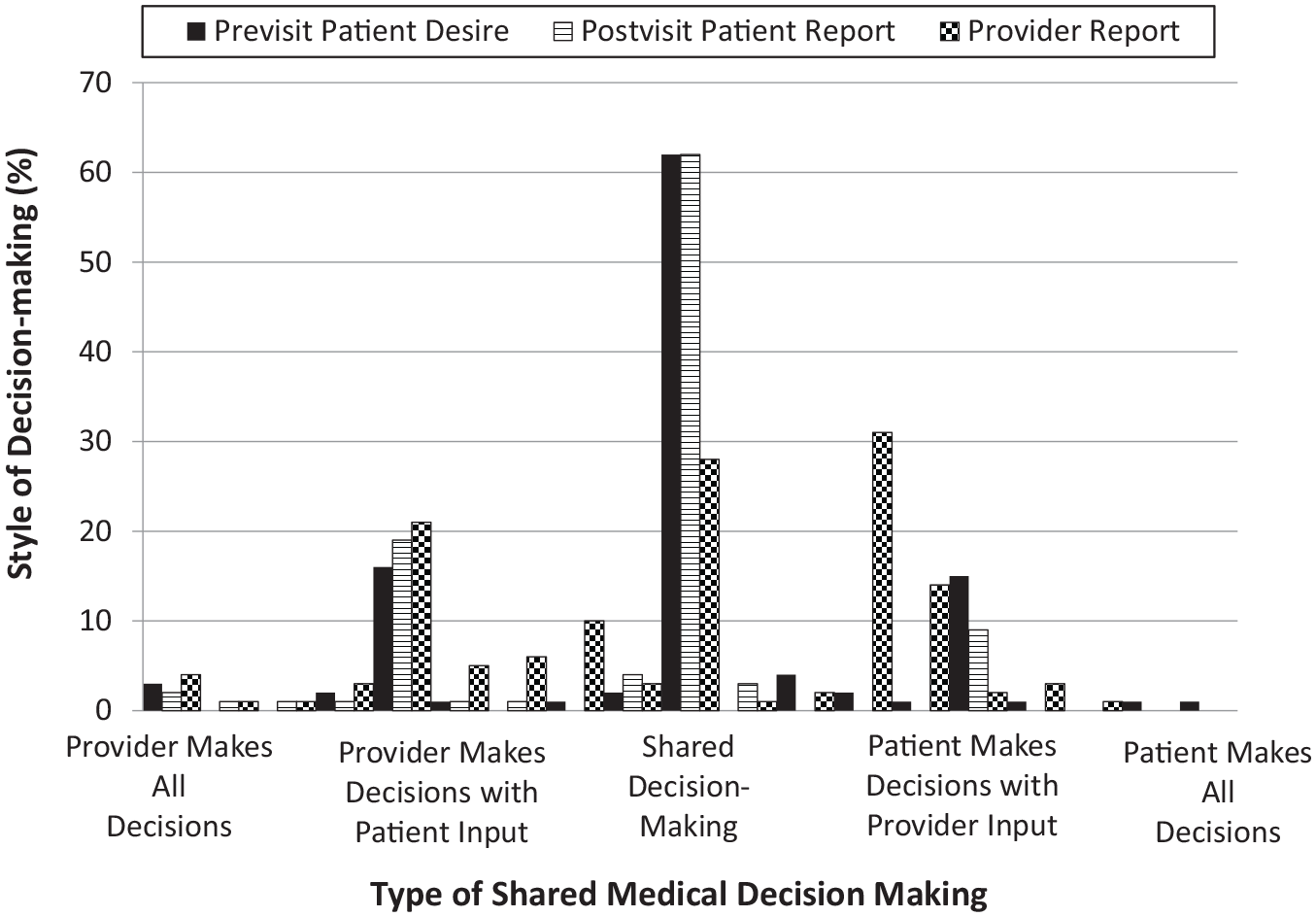
Patient preferences for shared decision-making.
Immediately after their visit, patients reported that they experienced shared decision making in 57% of encounters, doctor-dominated decision making in 31%, and patient-dominated decision making in 11% of encounters, with a mean score of 9.0 (SD 3.0; Figure 2). In 54% of encounters, patients reported a perfect match between desired and received shared decision making (Figure 3). In contrast, physicians reported that they dominated decisions 50% of the time, and patients dominated 24% of encounters, with shared decision making occurring only 26% of the time.
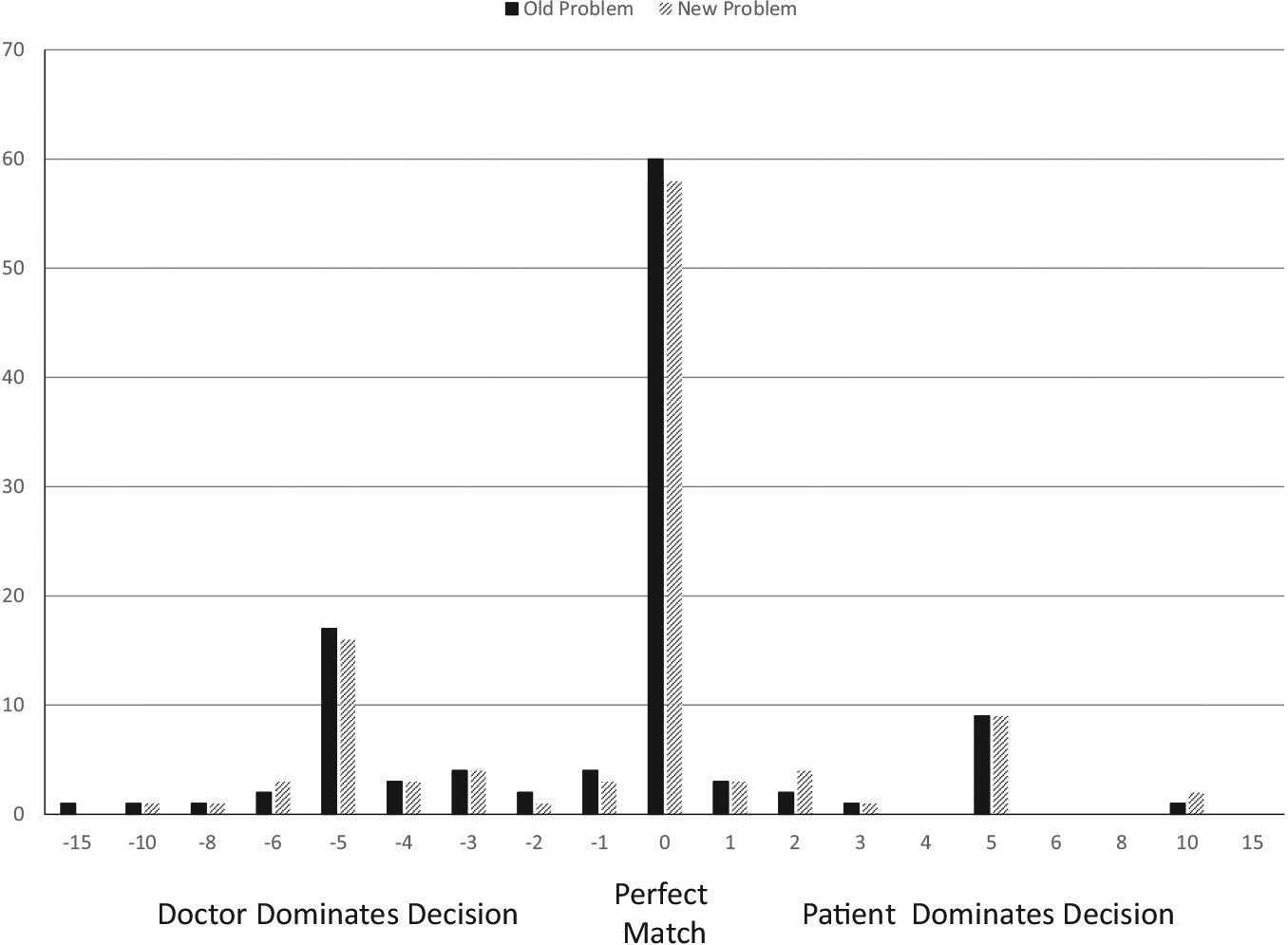
Discordance between patient desired and experienced shared decision-making.
The nature of shared decision making, per patient report, varied according to the complexity of decision making. More complex decisions tended to be more polarized, with a greater percentage of decision-making styles at each extreme (Figure 4). For basic decisions, 36% were rated as shared equally, with 15% slightly consumeristic and 40% slightly paternalistic. Only 3% of basic decisions were rated as mostly consumeristic and 6% as paternalistic. For intermediate or complex decisions, 73% were rated as shared equally, 11% were consumeristic, and 16% were paternalistic (Figure 3; P < 0.0005 for comparison). There was less of a difference between desired and experienced decision-making style for encounters with complex decision making than with basic decision making (P = 0.003). These findings were not influenced by patient functional status, mental health, health locus of control, or difficulty of the encounter from the physician’s perspective. There was no impact of concordance of decision-making style on patient trust, visit satisfaction, or 1-month medication adherence.
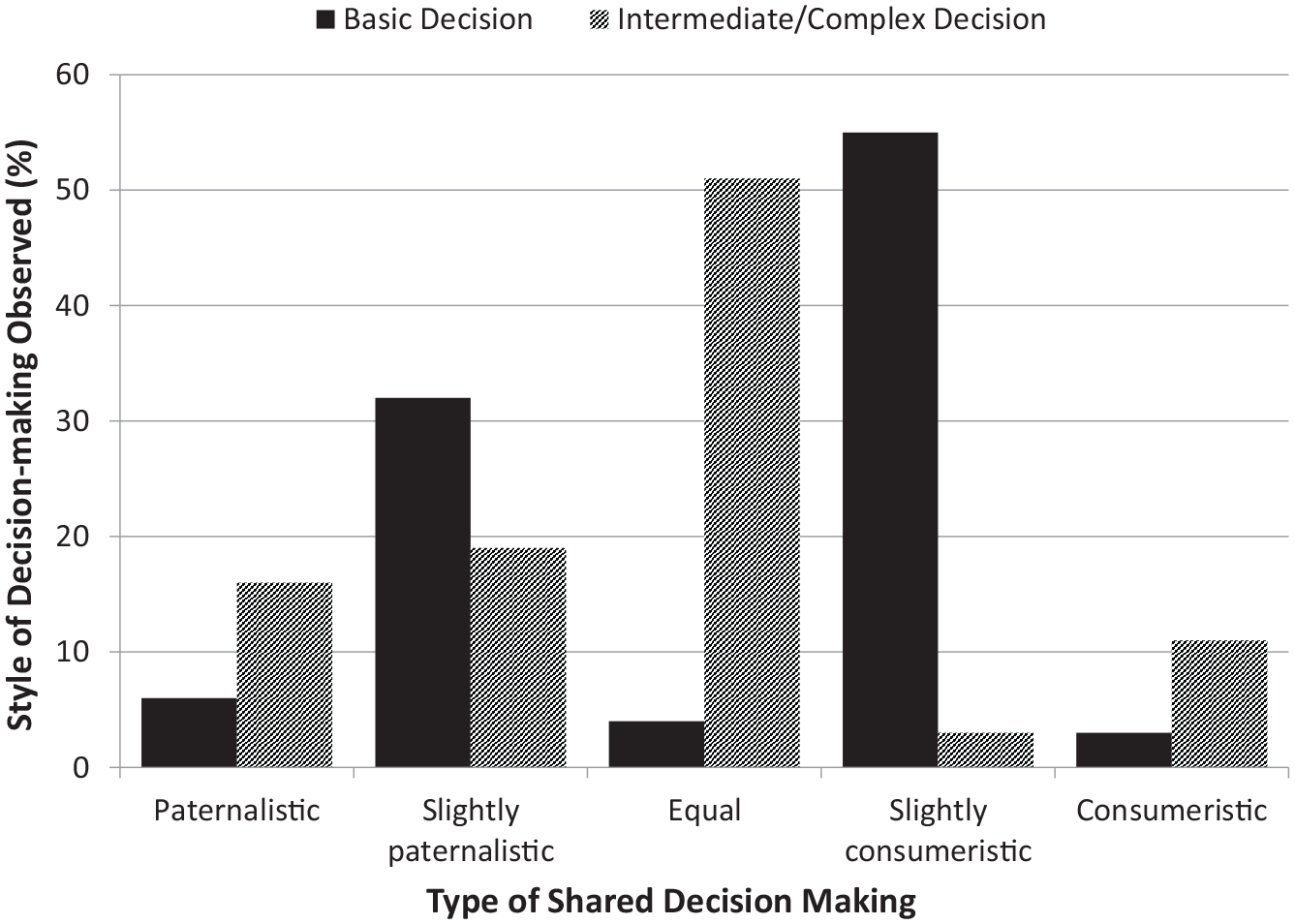
Comparison of style of shared medical decision making stratified by decision type.
In contrast, the objective measure of the quality of shared decision making (OPTION-5) found that the quality of shared medical decision making was low, with an average standardized score of 27.5 (range, 0–70). Objective assessment of the quality of shared decision making did not match patient ratings of the quality of shared decision making. Encounters that were rated as perfectly shared decisions between patients and physicians did not have higher OPTION-5 scores (28.7 v. 26.6, P = 0.47). There was no relationship between OPTION-5 scoring and the squared difference between perceived perfectly shared medical decision-making ratings by the patients (P = 0.58). However, there was a relationship between OPTION-5 and provider self-rating of the quality of shared medical decision making (β = −0.34, P = 0.03), although the variance explained was low (r2 = 0.04). The level of complexity of the decision (simple v. intermediate/complex) did not affect this finding.
Using RIAS, encounters averaged 30 min, with 635 utterances; doctors spoke more than patients did (356 utterances v. 279, P = 0.0001). There was no difference in the duration of the encounters (29.4 v. 29.9 min, P = 0.85) or in the number of patient (P = 0.61) or physician (P = 0.62) utterances with more complex decisions. Encounters with higher objective measurement of shared decision making had higher degrees of positive scores for physicians giving biomedical information to patients (β = 0.13, 95% confidence interval [CI]: 0.09–0.19), patient rapport (β = 0.12, 95% CI: 0.06–0.18), but also had higher scores for doctor dominance of the conversation (β = 47.9, 95% CI: 11.1–84.9).
Most patient ratings of decision making desired versus received were minimally different (60%). There was no difference in age, gender, race, or decision complexity for discordance. Encounters in which patient ratings of pre- and postencounter decision making were discordant had lower patient ratings of satisfaction (24 v. 22.3, P = 0.01) and trust (33.5 v. 31.4, P = 0.01). Physicians did not rate these encounters as more difficult (22.4 v. 23.3, P = 0.67). For discordant encounters, there was no difference in the duration of the encounters (27.5 v. 30.5 min, P = 0.21), but there was higher doctor dominance of the encounter (55.6 v. 59.8, P = 0.002) and lower ratings of doctor rapport (10.4 v. 5.9, P = 0.007). There was no difference in objective measures of the quality of shared medical decision making between concordant and discordant patient ratings (28.5 v. 25.9, P = 0.38). In contrast, encounters with discordance between patient and physician ratings of shared decision making had no differences in satisfaction, trust, difficulty, duration, doctor dominance, or rapport. There was no impact of gender or race concordance between the patient and the physician on any of our assessed measures.
Patients had low adherence (46.4%) to their antihypertensive medications at baseline (Table 1). There was no improvement in adherence or diastolic blood pressure values at 4 weeks (Table 3), although both systolic blood pressure (137 mm Hg v. 132 mm Hg, P = 0.005) and functional status improved (22.3 v. 23.9, P = 0.04) slightly. There was no relationship between the rating of shared medical decision making by patients, providers, or OPTION-5 and these changes. There was also no relationship between a clinically significant better quality of shared medical decision making and any of these outcomes.
Discussion
In this observational study of clinical encounters between complex adult patients and their physicians in an internal medicine clinic, most patients preferred shared decision making, with about one-quarter desiring that providers make the decisions and about one-fifth preferring to make decisions themselves. There was high concordance between patient previsit preferences and what they reported experiencing during the encounter. These findings did not vary by age, gender, race, health literacy, presence of mood or anxiety disorders, or health locus of control. Provider ratings of these encounters were slightly more paternalistic than patient ratings but generally had high concordance with patient ratings. Interestingly, while objective measures of decision making did not match patient reports of the degree of decision making, physician ratings were slightly more accurate, although the correlation was weak. In general, the quality of shared decision making in these encounters was poor.
Patients who had a significant difference between desired and perceived decision making had lower levels of satisfaction and trust. These encounters also had greater provider dominance of the discussion. On the other hand, differences between patient and provider ratings of the encounters had no impact on any of these measures.
While encounters had numerous decisions, most of these were simple decisions, such as obtaining routine tests or renewing medications. To get full credit for an informed decision, the provider had to alert the patient that there was a decision to be made, provide information about the decision, support patient information seeking, and elicit and then integrate patient preferences. More than 80% of the “decisions” that were made during these encounters were routine, such as refilling prescriptions or obtaining routine follow-up labs. It is possible that neither the patient nor the providers considered these to be decisions or were satisfied with the limited interactions that occurred. Typically, patients were asked if they needed any medications refilled and if they were having any problems with them, or they were asked when they wanted to follow-up. Given the time limits faced by primary care physicians, it is possible that they reserve more formal decision-making conversations about new decisions or ones with greater risks and benefits. Our sample had only 2 complex decisions, and we found that these decisions had higher-quality decision-making conversations. The encounters with higher decision-making had a tone of more patient rapport but also included a greater number of utterances made by the provider. This may not be surprising because the task of providing information as well as eliciting and integrating patient preferences may take more doctor statements to accomplish than merely asking when a patient wants to follow-up.
Providers reported that they were slightly more dominating than perceived by patients. Objective measurement of the visit encounter found that most visits included numerous decisions, although most decisions were basic ones about medication renewal, routine diagnostic testing, and follow-up, for example, a provider asking if the patient needs a medication refill or their annual mammogram. Basic decisions were very balanced, with 90% being relatively shared. More complex decisions had more diversity in objective ratings of decision making; a greater percentage was at both extremes, with a greater role being played either by the patient or the provider. However, although more extreme styles of decision making occurred, the decision-making style in these encounters closely matched the style desired by the patient.
Our findings are similar to previous works. Braddock et al. found that most decisions were basic, but they noted the content of these interactions generally did not fulfill their criteria for informed decision making. 29 Similarly, we found that decisions were mostly basic, with physicians making the decision and patients acknowledging or agreeing with them. Our objective ratings of the quality of shared medical decision making are also similar to values reported in other primary care studies.15,30 OPTION-5 rates the quality of shared decision making in 5 domains. It is probably not necessary to address all aspects of shared medical decision making for basic decisions, particularly routine decisions that have been made previously. For example, deciding to renew a blood pressure medicine that the patient has been on for years, a basic decision, likely does not need the same level of interaction as starting a new medication or discussing riskier decisions. In addition, it is possible that the relationship between the physician and patient offers benefits that are not measured by instruments such as OPTION-5. It is also possible that we are focused on precisely measuring what are essentially transactional and not relational factors or placing too little emphasis on the importance of nonverbal communication in these measures.
A systematic review found that patient perception of shared medication decision making resulted in improved affective-cognitive outcomes but not behavioral or other health outcomes. 34 This is similar to the findings of our study. We found a decrease in affective outcomes (satisfaction and trust), with discordance between expected and received shared medical decision making among patients, but no impact on functional status, adherence, or blood pressure readings at 4 weeks.
Our data are limited by several factors. First, these are established patient-provider dyads. It is not surprising that over time, patient desires for and provider decision-making styles become concordant. Patients would likely seek providers with decision-making styles that match their preference. It is likely that experienced providers use a variety of decision-making styles, tailored to the patient. In the course of a relationship, providers learn the style preferred by the patient and follow it. Second, these were routine visits with few complex decisions; nearly all the decisions were basic. Whether our findings would generalize to encounters with a higher frequency of complex decisions is uncertain. Third, our sample size was small. It is possible that important associations with some of the descriptive variables were missed. Most of our sample was African American (57%); however, previous studies have not found a difference in desired shared decision making between African Americans and other groups.35–38 Fourth, we did not measure trust at baseline. The relationship between discordance in desired and perceived decision making may not be causal, and patients with lower baseline trust may perceive that decision making was different than desired. Finally, there were differences in the objective measure of shared medical decision making between providers. However, there were no differences in provider self-ratings of shared medical decision making or differences between providers in patient satisfaction or trust or other interactive measures assessed by RIAS. We adjusted for the impact of these potential provider differences in our analyses.
We found that patients generally prefer shared decision making and that they report that their provider’s decision-making style is a close match. Providers report greater dominance in decision making. Decisions were common during these encounters, but most were basic. Actual decision making varied significantly by complexity of the decision, indicating that physicians were flexible in decision-making approaches. Both patients and physicians overstate the degree of shared medical decision making that is occurring during these encounters. Discordance between a patient’s desired and received shared decision making reduced satisfaction and trust. The quality of shared medical decision making did not affect medication adherence or blood pressure levels 1 month after the encounter.
Footnotes
Authors’ Note
All opinions expressed in this manuscript represent those of the authors and should not be construed to reflect, in any way, those of the Department of Veteran Health Affairs, Department of Defense, or the US government.
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The author(s) received no financial support for the research, authorship, and/or publication of this article.