
Abstract
Background
Most commonly used diffusion-weighted imaging (DWI) models include intravoxel incoherent motion (IVIM), diffusion kurtosis imaging (DKI), stretched exponential model (SEM), and mono-exponential model (MEM). Previous studies of the four models were inconsistent on which model was more effective in distinguishing cervical cancer from normal cervical tissue.
Purpose
To assess the performance of four DWI models in characterizing cervical cancer and normal cervical tissue.
Material and Methods
Forty-seven women with suspected cervical carcinoma underwent DWI using eight b-values before treatment. Imaging parameters, calculated using IVIM, SEM, DKI, and MEM, were compared between cervical cancer and normal cervical tissue. The diagnostic performance of the models was evaluated using independent t-test, Mann–Whitney U test, receiver operating characteristic (ROC) curve analysis, and multivariate logistic regression analysis.
Results
All parameters except pseudo-diffusion coefficient (D*) differed significantly between cervical cancer and normal cervical tissue (P < 0.001). Through logistic regression analysis, all combined models showed a significant improvement in area under the ROC curve (AUC) compared to individual DWI parameters. The model with combined IVIM parameters had a larger AUC value compared to those of other combined models (P < 0.05).
Conclusion
All four DWI models are useful for differentiating cervical cancer from normal cervical tissue and IVIM may be the optimal model.
Keywords
Introduction
Diffusion-weighted imaging (DWI) is a commonly used method of magnetic resonance imaging (MRI) that can provide quantitative information about the Brownian motion of water molecules in normal or abnormal tissue, which is closely related to tissue microenvironment (1). In general, solid tumors are associated with the over-growth of tumor cells, resulting in decreased extracellular space. Hence, the random diffusion of water molecules within the extracellular space is more restricted, which will enhance the signal in DWI. An apparent diffusion coefficient (ADC), obtained from DWI with a mono-exponential model (MEM) (2), is the most widely used DWI parameter. However, ADC values may not reflect water molecular diffusion accurately in vivo because it is influenced by capillary microcirculation (3).
DWI has been shown to be highly sensitive for detecting acute ischemic stroke (4) and for diagnosing malignancy (5–7). Some previous studies have suggested that the intravoxel incoherent motion model (IVIM), stretched exponential model (SEM), and diffusion kurtosis imaging (DKI) might provide more accurate information about water molecular diffusion (8–10). IVIM can estimate both diffusion and perfusion parameters simultaneously, SEM aims to evaluate the intravoxel heterogeneity of water molecular diffusion, while DKI considers the distribution of water molecular diffusion, which could be non-Gaussian in case of tumor tissue.
Cervical cancer is one of the most common cancer types in women worldwide, particularly in developing countries (11). Different DWI models have been shown to provide statistically significantly different information between cervical cancer and normal cervical tissue (12–15). However, there are evident discrepancies across studies. Li et al. (16) showed that DKI was superior to MEM for prostate cancer discrimination. Wang et al. (12) reported that DKI showed no clear added value over conventional DWI for the characterization of cervical carcinoma. Lin et al. (13) reported that, compared with MEM, diffusion parameters from IVIM and SEM may offer additional information in cervical carcinoma diagnosis. Zhang et al. (17) compared the value of MEM, IVIM, SEM, and DKI models for differentiating renal solid masses, and found that diffusion heterogeneity index (α) might provide additional information for differentiation between benign and malignant renal masses. However, ADC remained the most valuable parameter for differentiating renal cell carcinoma subtypes and for clear cell renal cell carcinoma grading.
The aim of the present study was to assess the diagnostic performance of the derived parameters of four DWI models for characterizing and differentiating cervical cancer from normal cervical tissue, and to determine which mode is the best for cervical cancer diagnosis.
Material and Methods
The study protocol was approved by the ethics review board of the Second Affiliated Hospital of Wenzhou Medical University (LCKY2019-287). Written informed consent was obtained from each patient before participation. All of the procedures were performed in accordance with the Declaration of Helsinki and relevant policies in China.
Patients
Fifty-eight female patients with clinically suspected cervical carcinoma by cervical smear or vaginoscopy, who underwent MRI between April 2016 and July 2017, were enrolled in this study. We excluded patients who had undergone radiotherapy and chemotherapy before MRI scanning and operation (n = 1), had no pathological results (n = 6), or had poor image quality with obvious artefacts (n = 4). Thus, of 58 cases, 47 were finally enrolled (32 cases of cervical carcinoma and 15 cases of cervical intraepithelial neoplasia II–III grade by postoperative pathology).
Imaging protocol
All scans were performed using a 3.0-T MRI scanner (Discovery 750; GE Healthcare, Chicago, IL, USA). All patients were imaged using the following sequences: a transverse axial fast spin-echo (FSE) T1-weighted (T1W) sequence (repetition time [TR]/echo time [TE] = 704/8 ms, field of view [FOV] = 320 × 320 mm, slice thickness/gap = 5/1 mm), axial fat-suppression, fast recovery, fast spin echo (FRFSE) T2-weighted (T2W) sequence (TR/TE = 3435/78 ms, FOV = 320 × 320 mm, slice thickness/gap = 5/1 mm), sagittal fat suppression FRFSE-T2W sequence (TR/TE = 3493/68 ms, FOV = 260 × 260 mm, slice thickness/gap = 5/1 mm), coronal FSE T2W sequence (TR/TE = 3534/68 ms, FOV = 280 × 280 mm, slice thickness/gap = 5/1 mm).
The DWI sequences with eight b-values between 0 s/mm2 and 2000 s/mm2 were acquired transversely through the cervix for assessment of DWI models. The protocol for this sequence was as follows: single-shot spin-echo echo-planar imaging (SE-EPI), using the same spatial coverage as that for the non-enhanced axial pre-saturated fat-suppression FRFSE T2W sequence (TR/TE= 2400/73 ms, slice thickness = 5 mm, slice gap = 5 mm, FOV = 360 × 360 mm, b values = 0, 30, 100, 200, 400, 1000,1500, and 2000 s/mm2, number of slices = 10). The total scan time for DWI was approximately 2 min 36 s.
Image processing
All image analyses were performed using commercially available software (MItalytics, FITPU Healthcare, Singapore). The regions of interests (ROIs) were manually drawn on each consecutive slice by two experienced radiologists with more than 10 years of experience in gynecological radiology. Normal ROIs were selected in the normal cervical tissue, away from the lesions. Necrotic, cystic, and hemorrhage regions were avoided when drawing the lesion ROIs. For each patient case, ROIs of tumor and normal cervical tissue were manually drawn on consecutive DWI slices (Fig. 1). Following DWI parameters were derived: ADC from MEM, diffusion coefficient (D), pseudo-diffusion coefficient (D*), and perfusion fraction (f) from IVIM, apparent diffusion coefficient (Dapp) and apparent kurtosis (Kapp) from DKI, and distributed diffusion coefficient (DDC) and diffusion heterogeneity index (α) from SEM. Representative parameter maps are illustrated in Fig. 2.
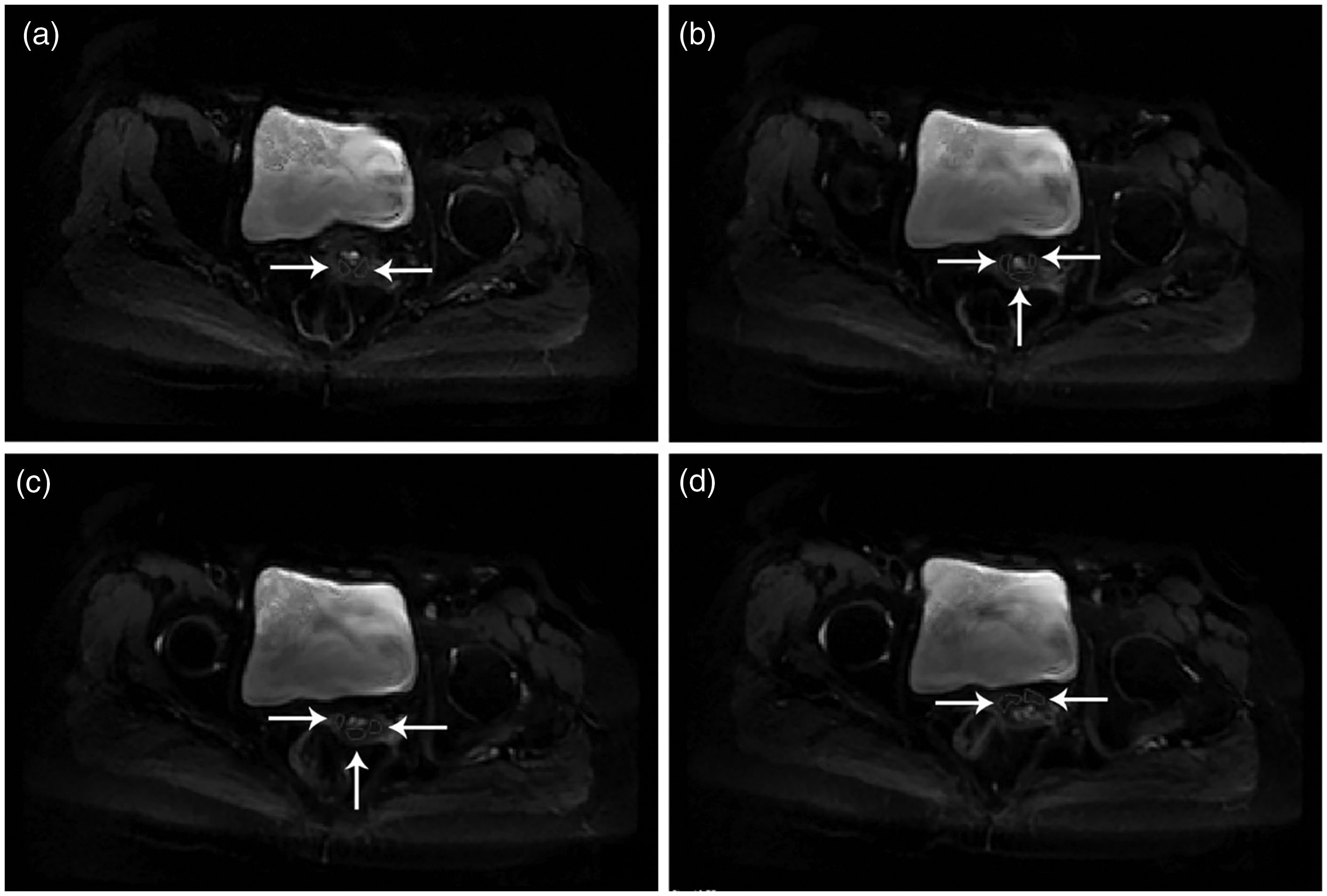
The diffusion-weighted magnetic resonance images of a 45-year-old woman with cervical intraepithelial neoplasia II–III grade. (a–d) The normal ROIs (white arrows) were manually drawn on each consecutive slice.
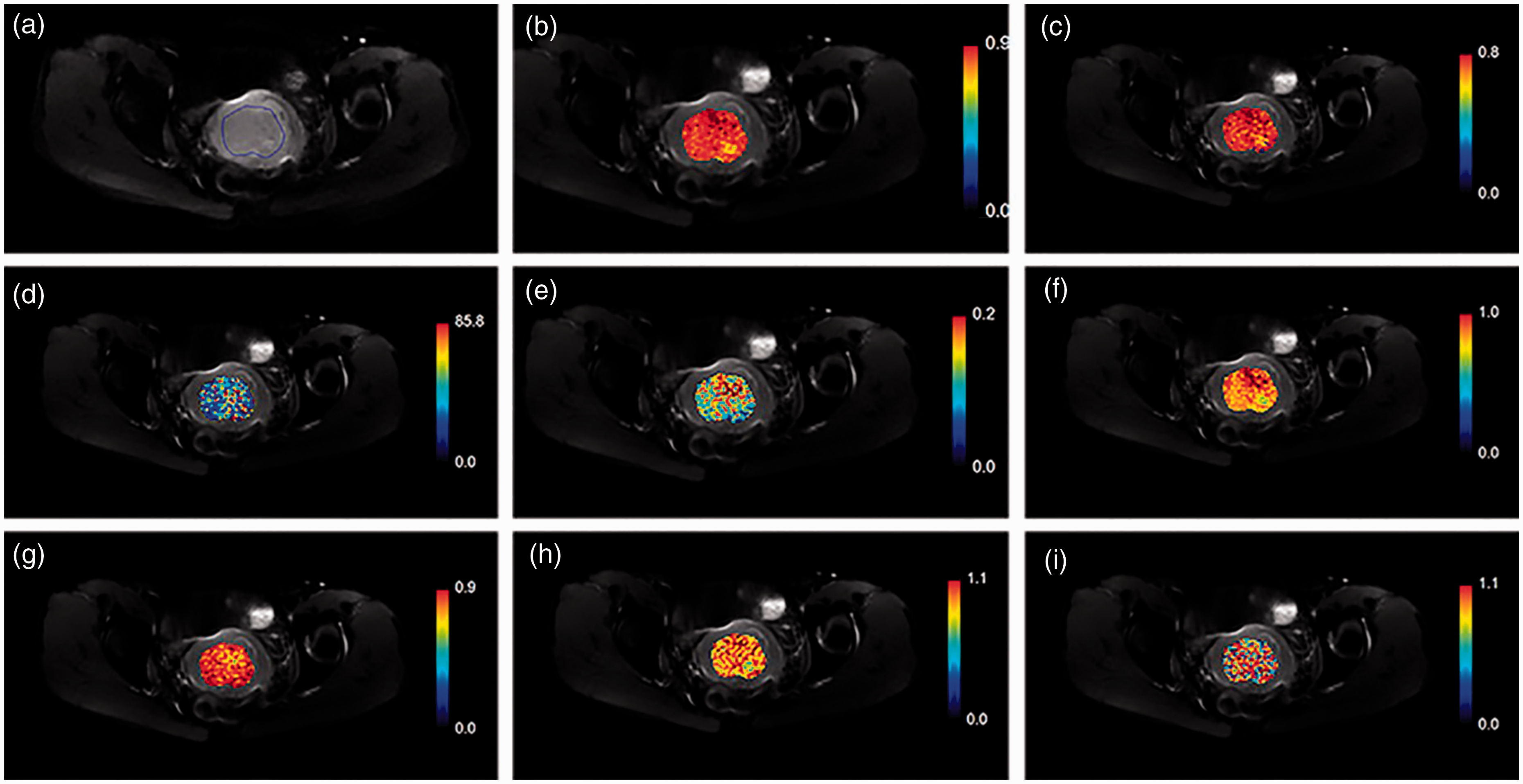
A case of cervical squamous cell carcinoma. (a) A lobulated mass with high signal intensity image with b value of 400 s/mm2, and the ROI on this slice. (b–i) apparent diffusion coefficient, diffusion coefficient, pseudo-diffusion coefficient, perfusion fraction, distributed diffusion coefficient, α, Dapp, and Kapp maps.
The DWI models were described as follows:
The standard ADC was calculated by fitting a MEM (Eq. 1) with all eight b-values:

IVIM is given by

Considering that D* is markedly larger than D, the above equation is reduced to a mono-exponential equation at b-values > 200 s/mm2. First, D was calculated by mono-exponentially fitting signal intensities at b-values > 200 s/mm2. Then, D* and f were estimated by fitting signal intensities at all b-values in the bi-exponential equation.
DKI fits data using

SEM is described as

Statistical analysis
SPSS Statistics (version 21.0, IBM Corp., Armonk, NY, USA) and MedCalc (version 15.2.2, Ostend, Belgium) were used for statistical analysis. The median values of each parameter acquired from every ROI were used for statistical analysis. The Kolmogorov–Smirnov test was conducted to analyze the normality of parameter distribution. Comparisons between lesion and normal cervix were performed using independent t-test for parameters with a normal distribution and Mann‒Whitney U test for parameters with a non-normal distribution.
Receiver operating characteristic (ROC) curves were plotted for all parameters, and the area under the ROC curve (AUC) was employed to quantify the power of different DWI model parameters in distinguishing the lesion from normal tissue. The Youden index (18), which defines the maximum potential effectiveness of a biomarker by giving equal weights to sensitivity and specificity, was utilized to determine the optimal cut-off value for each parameter for cervical cancer tissue recognition. Parameters in different DWI models were used as input variables for multivariate logistic regression analysis to calculate prediction probabilities. ROC analysis was performed for each combined model. AUC was compared between combined models and independent parameters. P < 0.05 was considered statistically significant.
Results
DWI data from 47 patients were used for the study. A total of 343 ROIs on DWI images were finally identified by two experienced gynecological radiologists together. There were 164 lesion ROIs (mean size = 290.7 ± 288.3 mm2, range = 21.8–1532.7 mm2) and 179 normal ROIs (mean size = 103.0 ± 72.6 mm2, range = 21.8–423.2 mm2).
Table 1 showed the comparison of model parameters between the lesion and the normal ROIs. All parameters except for D* were statistically significantly different between cervical cancer and normal cervical tissue (P < 0.001). The values of diffusion parameters (ADC, D, DDC, and Dapp) for cervical cancer estimated by all models were all significantly lower than those for normal cervical stroma (P < 0.001). Among the perfusion parameters, the value of f in the lesion was significantly lower than that in normal cervical tissue (P < 0.001), and there was no significant difference in the value of D* between the lesion and normal cervical tissue (P = 0.428). In cervical cancer, α and Kapp were significantly higher than in normal cervical stroma (P < 0.001).
Comparison of DWI parameters between cervical cancer and normal cervical stroma.
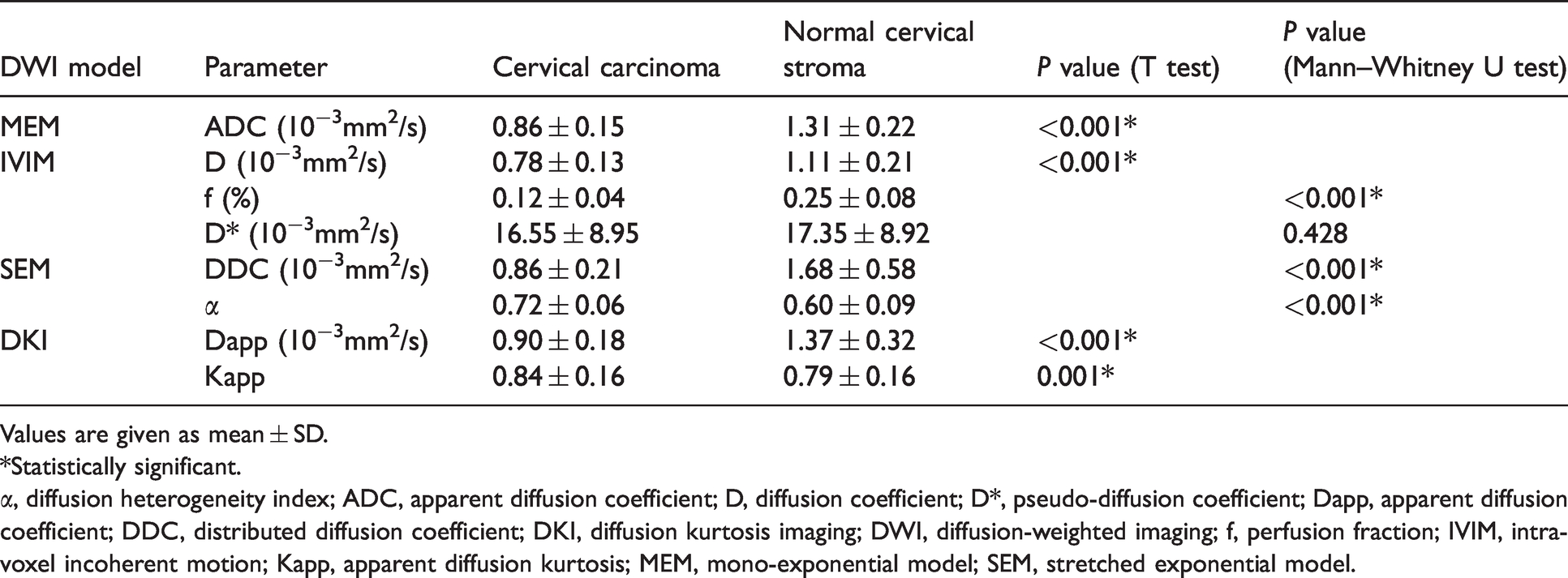
Values are given as mean ± SD.
*Statistically significant.
α, diffusion heterogeneity index; ADC, apparent diffusion coefficient; D, diffusion coefficient; D*, pseudo-diffusion coefficient; Dapp, apparent diffusion coefficient; DDC, distributed diffusion coefficient; DKI, diffusion kurtosis imaging; DWI, diffusion-weighted imaging; f, perfusion fraction; IVIM, intravoxel incoherent motion; Kapp, apparent diffusion kurtosis; MEM, mono-exponential model; SEM, stretched exponential model.
Comparison of ROC curves between cervical cancer and normal cervix with DWI models.
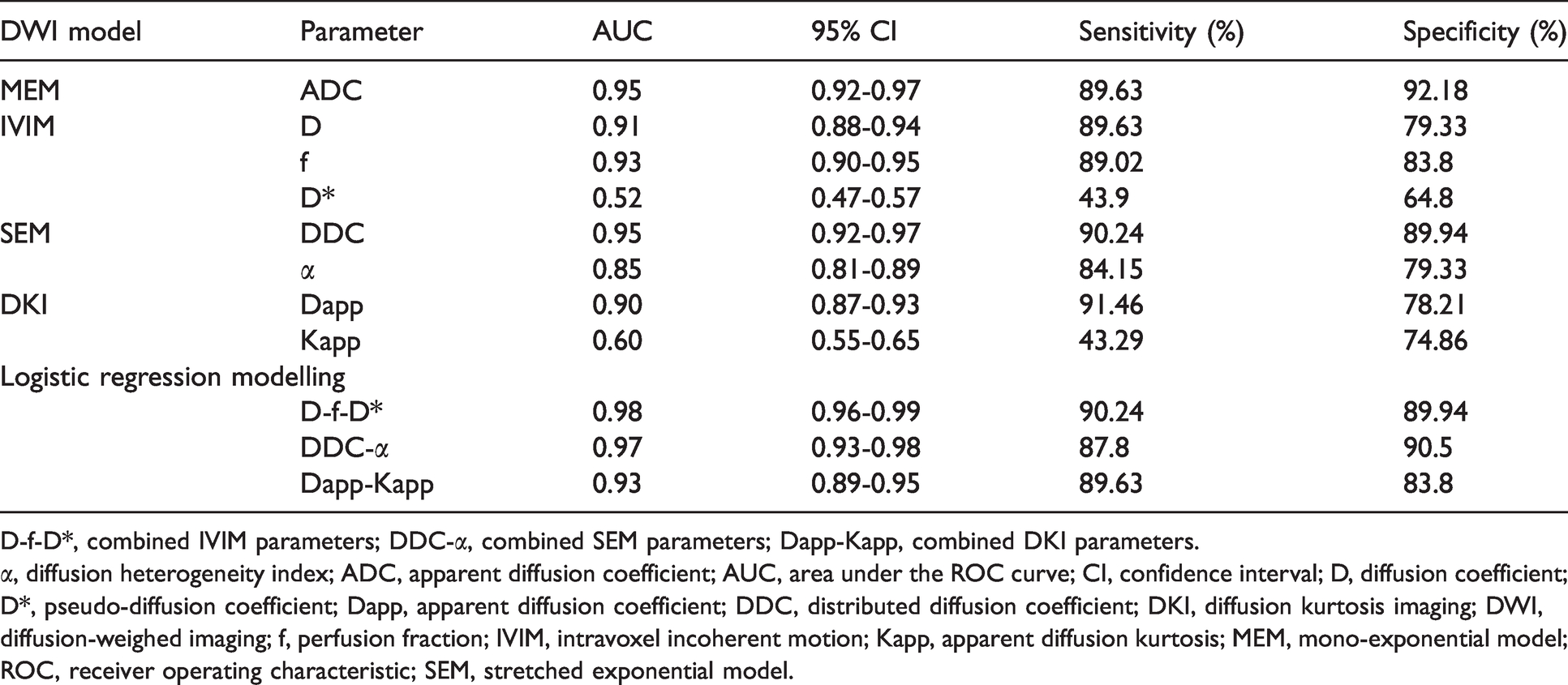
D-f-D*, combined IVIM parameters; DDC-α, combined SEM parameters; Dapp-Kapp, combined DKI parameters.
α, diffusion heterogeneity index; ADC, apparent diffusion coefficient; AUC, area under the ROC curve; CI, confidence interval; D, diffusion coefficient; D*, pseudo-diffusion coefficient; Dapp, apparent diffusion coefficient; DDC, distributed diffusion coefficient; DKI, diffusion kurtosis imaging; DWI, diffusion-weighed imaging; f, perfusion fraction; IVIM, intravoxel incoherent motion; Kapp, apparent diffusion kurtosis; MEM, mono-exponential model; ROC, receiver operating characteristic; SEM, stretched exponential model.
Table 2 and Figs. 3 and 4 presented the diagnostic performance of all DWI models for separating lesions from normal tissue. The AUC of ADC was 0.95. The AUC values of IVIM parameters were 0.93 for f, 0.52 for D*, and 0.91 for D. The AUC of combined model D-f-D*(IVIM) was 0.98. The AUCs of DDC and α were 0.95 and 0.85, respectively. The AUC of combined model α-DDC(SEM) was 0.97. The AUCs of Dapp and Kapp were 0.90 and 0.60, respectively. The AUC of combined model Dapp-Kapp(DKI) was 0.93. Through logistic regression analysis, all combined models showed a significant improvement in AUC compared to individual DWI parameters. The model with combined IVIM parameters had a larger AUC value compared to other combined models (P < 0.05).
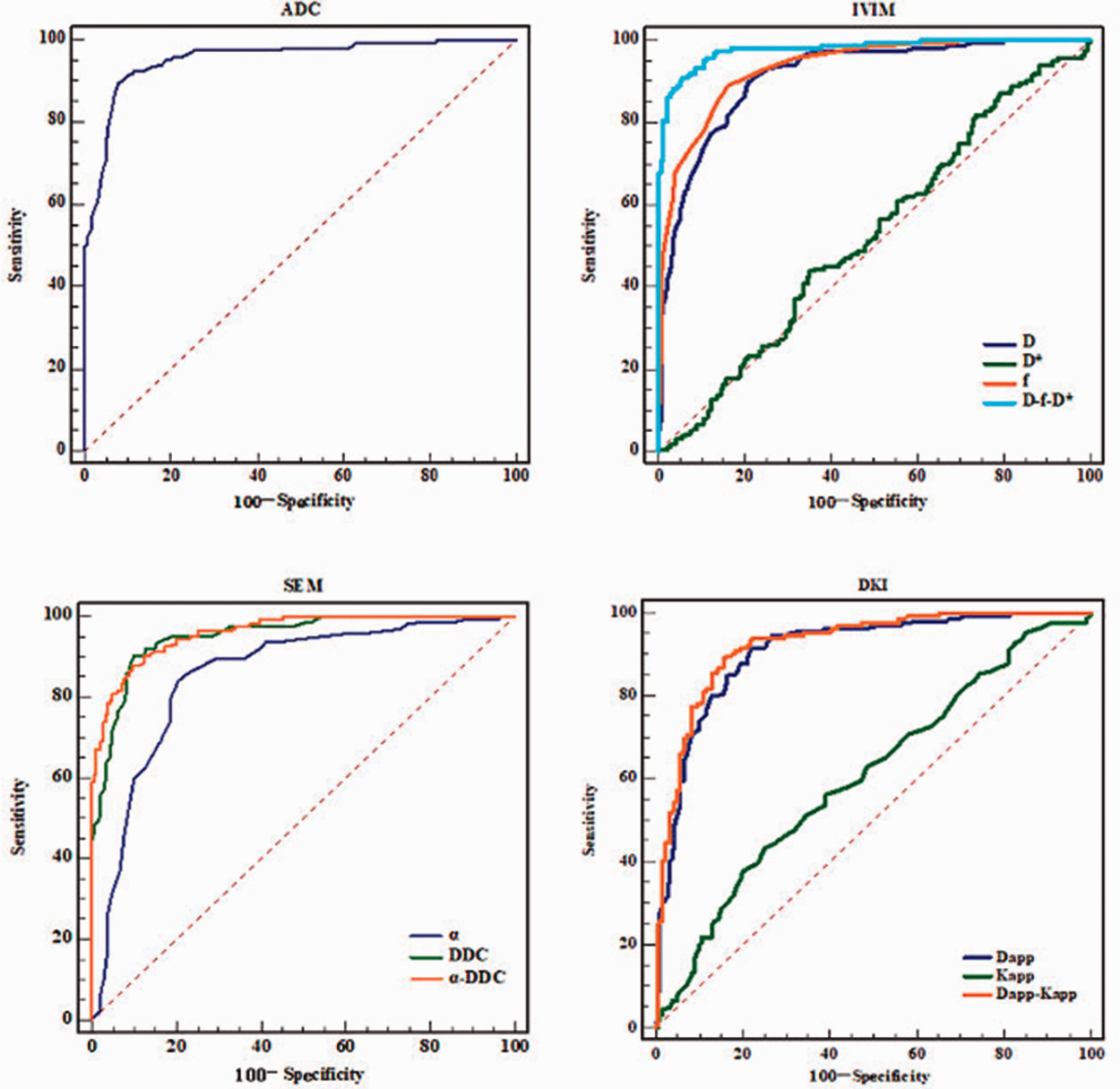
Receiver operating characteristic curves for the diagnosis of cervical carcinoma compared to normal tissue using four diffusion-weighted imaging models.
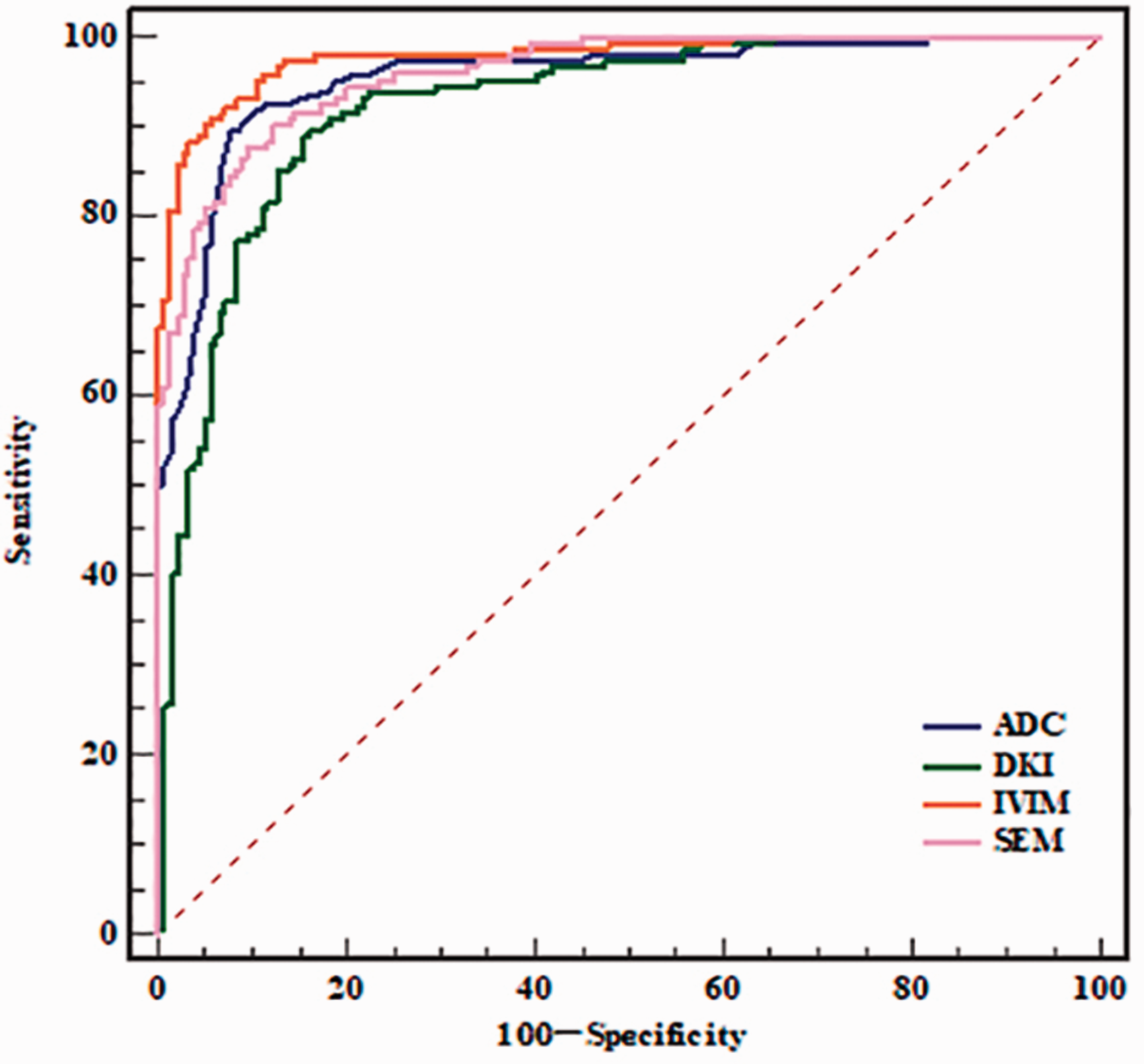
Receiver operating characteristic curves for the diagnosis of cervical carcinoma compared to normal tissue through combing diffusion-weighted imaging model parameters using multivariate logistic regression, where the areas under the curve were 0.98 for combined intravoxel incoherent motion, 0.97 for combined stretched exponential model, and 0.93 for combined diffusion kurtosis imaging.
Discussion
This study compared the discriminatory power of four DWI models in differentiating cervix cancer and normal cervical tissue. The results showed that all four DWI models were useful in making distinctions between cervical cancer and normal cervical tissue. All parameters, except for D*, were statistically significantly different between cervical cancer and normal tissue. Quantitatively, the lesions in the cervical cancer group showed significantly lower ADC, D, f, DDC, and Dapp values, and higher α and Kapp values, than the normal cervical tissue group. Through logistic regression analysis, all combined models showed a significant improvement in AUC compared to individual DWI parameters. The combined IVIM model attained a larger AUC compared to other combined models (P < 0.05). Thus, IVIM may be the optimal model for differentiating cervical cancer from normal cervical tissue.
In previous studies, mean ADC values were significantly lower in cervical cancer than in normal cervical tissue (19–24). The Brownian motion of water molecules in tissue is closely related to tissue microenvironment, such as cellular density. Typically, the over-growth of tumor cells results in elevated cellular density and reduced extracellular space, leading to reduced diffusion of water molecules (25–27). Thus, the ADC of cervical cancer was significantly lower than that of normal cervical tissue.
IVIM allows separation of the diffusion and the perfusion components by means of a single sequence (8,25). Consequently, the D value, which measures pure diffusion, would be lower than the ADC value. Similar to ADC, a lower D value was also obtained for cervical carcinoma than for normal cervical stroma (0.78 × 10−3 mm2/s vs. 1.11 × 10−3 mm2/s).
There are two perfusion-related IVIM parameters: f and D*. The estimated f in this study was nearly half the value reported by Lin et al. (13), but closer to that reported by Lee et al. (15). The parameter f models the weight (in percentage) of “diffusion” driven by the process of flow in the vascular space. In this space, the movement of water molecules is more linked to blood perfusion than to Brownian motion, which is more typical in the interstitial space. A simple interpretation is that the f value could reflect the fractional volume of vascular space, which is modeled as Vp in dynamic contrast-enhanced imaging. Evidently, the estimate of f close to 50% in normal cervical tissue in the study by Lin et al. (13) is an overestimation of the fractional volume of the vascular space in normal cervical tissue. Hiroshi et al. (6) proposed that the over-estimate of f could be because perfusion fraction might not be specific to perfusion only but may also be sensitive to other bulky flow phenomena, such as glandular secretion and fluid flow in the ducts. In addition, the difference could be due to the algorithm used in data fitting, which will be investigated in the future.
The SEM-derived parameters, DDC and α, found in this study were similar to those described by Lin et al. (13). Both studies demonstrated that the value of α in cervical cancer is larger than that in normal cervical tissue. This was similar to the finding of Wu et al. (28), who reported that the α values of metastatic lymph nodes were significantly higher than that of non-metastatic lymph nodes. Although the biological underpinning of α is unclear, it is likely to reflect tissue heterogeneity, which may also influence the DCC measurement (29). It has been hypothesized that tumors could have a higher level of intravoxel diffusion heterogeneity and higher cellular and glandular pleomorphism, leading to a lower α (5). It was argued that this apparent controversy could be due to the anisotropy of the fibrous tissue in the normal cervix, which led to comparatively more heterogeneous diffusion than in the tumor. Essentially, the stretched exponential with
The DKI-derived parameters, Dapp and Kapp, with values of 0.90 ± 0.18 ×10−3 mm2/s and 0.84 ± 0.16 ×10−3 mm2/s for cervical cancer, respectively, were similar to the values reported by Wang et al. (30). There was a significant difference between the Kapp values in cervical cancer and normal cervical tissue in this study (P < 0.001), which was different from the finding by Wang et al. (30), where no significant difference was observed. Wang et al. noted that the ADC value was 0.66 ± 0.0718 ×10−3mm2/s for cervical cancer and 0.71 ± 0.1292 ×10−3mm2/s for normal cervical tissue (30), where the estimated ADC values and the difference in ADC values between cervical cancer and normal cervical tissue were noticeably smaller than those reported in the present study and other studies (13,15).
Using logistic regression analysis, we found that the AUC of IVIM was higher than those of SEM, and DKI. This result was consistent with those of previous studies (31), which also found that non-MEMs were preferred to the MEM in DWI data from cervical tumors. Li et al. (16) showed that DKI was superior to MEM for discrimination of prostate cancer. Wang et al. (12) reported that DKI showed no clear added value over conventional DWI for the characterization of cervical carcinoma. Lin et al. (13) reported that, compared with MEM, diffusion parameters from IVIM and SEM might offer additional information for cervical carcinoma diagnosis. One of the reasons for these contradictory results may be the repeatability of the fitted parameters. The parameters of the SEM have been shown to be very repeatable (coefficient of variation [CV] 4%‒7%), comparable to the repeatability of ADC estimates (32–34), while the repeatability of IVIM parameters, particularly f and D*, were significantly worse (CV > 20%) (32–35). Another reason for these differences may be related to the setting of b-values, including the number of b-values and the maximal b-value. Rosenkrantz et al. (36) suggested that at least three b-values should be acquired for DKI analysis outside of brain, at least two of these should be both above and below b = 1000 s/mm2 to allow robust estimates of mean difference and mean kurtosis. In our study, we used eight b-values (0, 30, 100, 200, 400, 1000, 1500, and 2000 s/mm2), and the largest b-value was 2000 s/mm2, meeting the suggested criteria.
The present study was limited by a single center with a small cohort, where cases were more moderately differentiated, squamous cell carcinoma of stages I–IIa. Further studies involving multiple centers with a large cohort are needed to validate the generalizability of our results.
In conclusion, the present study investigated the performance of state-of-the-art methods for multi-b-value DWI data analysis for differentiating between cervical cancer and normal cervical tissue, and found that all four DWI models were useful for differentiating cervical cancer from normal cervical tissue and IVIM was potentially the optimal model.
Footnotes
Acknowledgements
The authors appreciate the assistance of Dr. Choon Peng Chng (Fitpu Healthcare Ltd, Singapore) in software customization for specific applications in this study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received the following financial support for the research, authorship, and/or publication of this article: The present study was funded by Wenzhou Science and Technology Bureau, China (Y20180765, Y2020816).