
Abstract
Background:
An initial anterior cruciate ligament (ACL) tear can be treated with surgical reconstruction or focused rehabilitation. The KANON (Knee Anterior cruciate ligament, NON-surgical versus surgical treatment) randomized controlled trial compared rehabilitation plus early ACL reconstruction (ACLR) to rehabilitation plus optional delayed ACLR and found no difference at 2 years by an intention-to-treat analysis of total Knee injury and Osteoarthritis Outcome Score (KOOS) results.
Purpose:
To compare the cost-effectiveness of early versus delayed ACLR.
Study Design:
Economic and decision analysis; Level of evidence, 2.
Methods:
A Markov decision model was constructed for a cost-utility analysis of early reconstruction (ER) versus rehabilitation plus optional delayed reconstruction (DR). Outcome probabilities and effectiveness were derived from 2 sources: the KANON study and the Multicenter Orthopaedic Outcomes Network (MOON) database. Collectively, these 2 sources provided data from 928 ACL-injured patients. Utilities were measured by the Short Form–6 dimensions (SF-6D). Costs were estimated from a societal perspective in 2012 US dollars. Costs and utilities were discounted in accordance with the United States Panel on Cost-Effectiveness in Health and Medicine. Effectiveness was expressed in quality-adjusted life-years (QALYs) gained. Principal outcome measures were average incremental costs, incremental effectiveness (as measured by QALYs), and net health benefits. Willingness to pay was set at $50,000, which is the currently accepted standard in the United States.
Results:
In the base case, the ER group resulted in an incremental gain of 0.28 QALYs over the DR group, with a corresponding lower overall cost to society of $1572. Effectiveness gains were driven by the low utility of an unstable knee and the lower utility for the DR group. The cost of rehabilitation and the rate of additional surgery drove the increased cost of the DR group. The most sensitive variable was the rate of knee instability after initial rehabilitation. When the rate of instability falls to 51.5%, DR is less costly, and when the rate of instability falls below 18.0%, DR becomes the preferred cost-effective strategy.
Conclusion:
An economic analysis of the timing of ACLR using data exclusively from the KANON trial, MOON cohort, and national average reimbursement revealed that early ACLR was more effective (improved QALYs) at a lower cost than rehabilitation plus optional delayed ACLR. Therefore, early ACLR should be the preferred treatment strategy from a societal health system perspective.
The 2 primary treatments that exist for anterior cruciate ligament (ACL) tears are surgical reconstruction or focused rehabilitation. Early reconstruction is utilized more commonly in the United States to facilitate the return to sport and to protect the meniscus and articular cartilage. Focused rehabilitation is reserved for lower demand and older patients. While ACL reconstruction (ACLR) outcomes are well documented and generally excellent,23,24 until recently, a direct comparison of the 2 treatments did not exist. A recent randomized controlled trial reported by Frobell et al, 7 the Knee Anterior cruciate ligament, NON-surgical versus surgical treatment (KANON) study, compared rehabilitation plus early ACLR to rehabilitation plus optional delayed ACLR using the primary outcome measure of the Knee injury and Osteoarthritis Outcome Score (KOOS) by an intention-to-treat analysis. The group undergoing rehabilitation plus optional delayed ACLR demonstrated a high crossover rate (39%) and clinical instability (32%) at 2 years compared with very little clinical instability (3%) in the ACLR group. Nearly two thirds of the patients underwent knee arthroscopic surgery to treat meniscus tears without ACLR. As a result, Frobell et al 7 found no significant difference between the early and delayed reconstruction groups at 2 years as determined by the total KOOS.
Frobell et al 7 concluded that the treatment strategy of rehabilitation with optional delayed reconstruction could reduce the utilization of ACLR. This trial and conclusion have the potential to alter the treatment paradigm for this common acute knee injury, as there are estimates of up to 250,000 new ACL injuries occurring annually. 10 Furthermore, because early osteoarthritis has been linked to ACL tears, 13 the future effects to patients and society could be substantial. A treatment shift such as this requires a complete evaluation of the societal impact, which must include an economic analysis. 22 However, the KANON trial 7 lacked a comprehensive economic evaluation. A cost-effectiveness analysis is the primary tool of an economic analysis. The purpose of this study was to compare the cost-effectiveness of early ACLR with rehabilitation plus optional delayed ACLR.
We had 2 principal aims in this cost-effectiveness analysis: The first was to compare the incremental quality-adjusted life-years (QALYs) between early reconstruction (ER) versus delayed reconstruction (DR), and the second was to compare the direct costs between these 2 groups from a societal viewpoint. We hypothesized that ER would result in both improved QALYs and less direct expenses.
Materials and Methods
General Model Overview
We investigated the cost-effectiveness of early ACLR (<10 weeks; ER group) compared with rehabilitation plus optional delayed reconstruction (DR group) using a Markov cohort decision model, which is presented in Figure 1. Cost-effectiveness was estimated from a societal perspective. After obtaining institutional review board approval, we obtained outcome and state transition probabilities from 2 primary sources: the prospective cohort of primary ACLR from the Multicenter Orthopaedic Outcomes Network (MOON; unpublished Short Form–36 [SF-36] outcomes) and the KANON study. 7 In Markov models, patients move through the model to various health states at defined intervals or cycle lengths and probabilities. The cycle length for this model was 1 year, and the model was run for 6 years, which is consistent with the average follow-up in the MOON cohort. All transition probabilities up to 2 years were taken from the KANON trial. Only long-term conversion to ACLR and ACLR retear rates were taken from the MOON data. The primary effectiveness outcome was expressed in QALYs, and costs were estimated in 2012 US dollars. Both costs and utilities were discounted at 3% to reflect their present values. The model and analysis were performed in accordance with the consensus-based recommendations for the conduct of cost-effectiveness analyses advocated by the Panel on Cost-Effectiveness in Health and Medicine20,21,26 and using a general decision analysis software package (TreeAge Pro Suite 2011, TreeAge Software Inc, Williamstown, Massachusetts, USA).
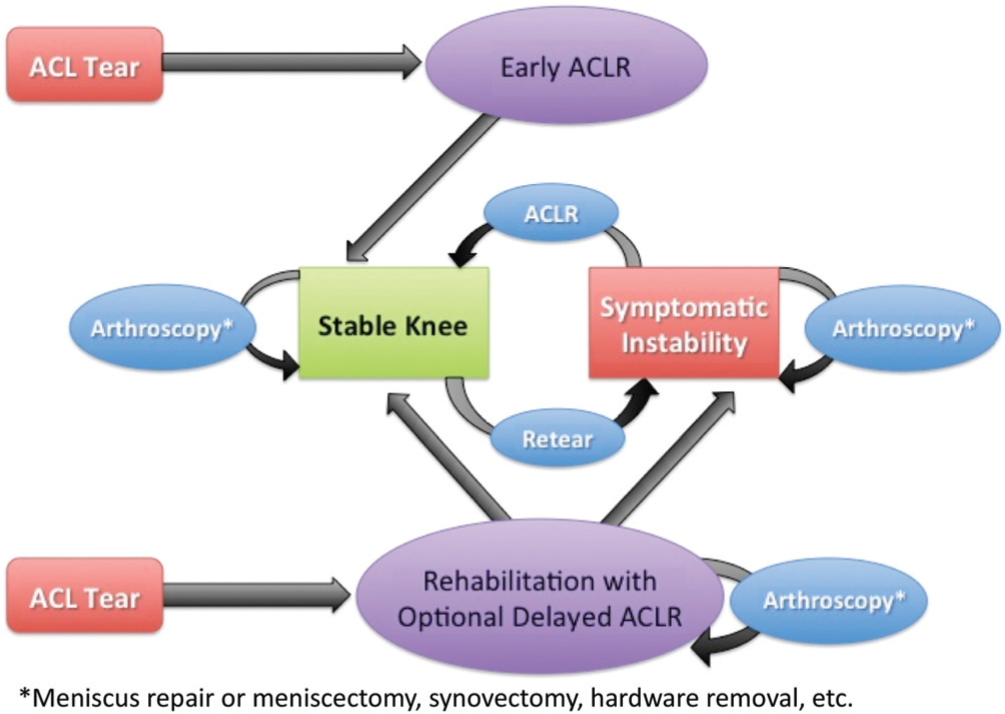
Health state diagram. The diagram demonstrates the clinical pathway of patients within the decision model. Health states include either a stable or unstable knee, while patients can undergo a reoperation consisting of meniscus repair, meniscectomy, manipulation under anesthesia, or hardware removal.
Model Structure
Our decision tree consisted of 2 primary treatment arms (ER and DR), as described above. Patients in the ER group entered a postprocedure state for 1 year, while those in the DR group entered an initial rehabilitation state for 1 year. All patients in the ER arm were assumed to have a stable knee at the end of year 1. Patients in the DR group could undergo arthroscopic surgery without ACLR for meniscus treatment. Thereafter, these patients could be in 1 of 3 health states: (1) stable knee with surgery, (2) stable knee with rehabilitation, or (3) symptomatic instability. The patients could undergo additional surgeries consisting of (1) meniscectomy, (2) meniscus repair, (3) manipulation under anesthesia, (4) removal of hardware, or (5) basic knee arthroscopic surgery. These reoperation rates were taken from the KANON trial. Patients were estimated to retear their ACL graft at rates consistent with those in the MOON cohort. 27
In the DR arm, patients could have a stable or unstable knee at the end of year 1 based on rates from the KANON trial. If initially successful with rehabilitation, they were assumed not to develop instability in the next 5 years of the model. Conversely, once symptomatic, patients remained symptomatic until they chose to undergo ACLR.
Model Parameters
As mentioned above, the 2 primary input sources came from the MOON database and KANON study (Table 1). The MOON cohort consisted of 807 primary ACL tears with a minimum follow-up of 6 years, while the KANON study had 121 patients (n = 62 in ER group; n = 59 in DR group), with a minimum follow-up of 2 years (unpublished data, in preparation).
Model Parameter Inputs a
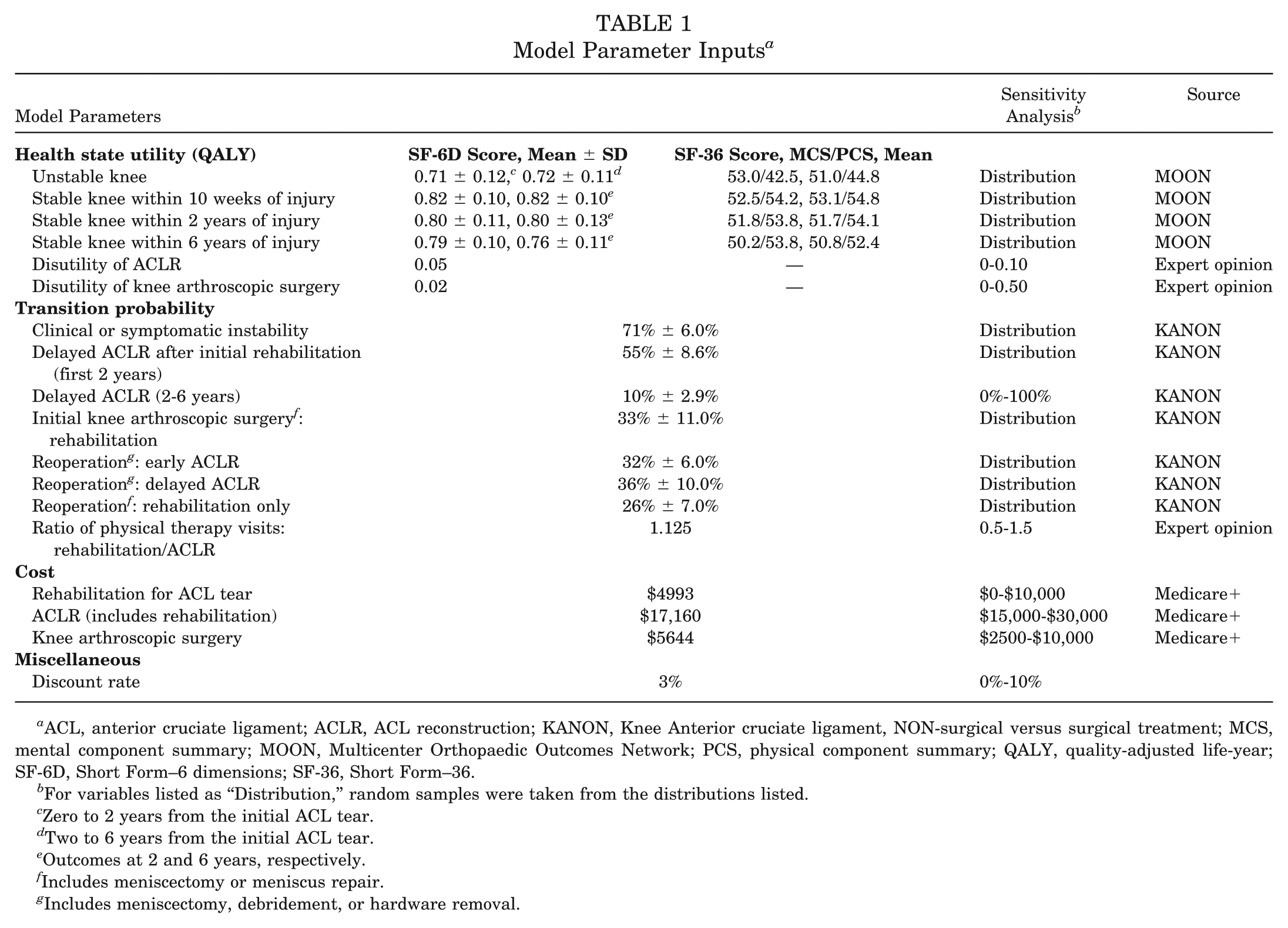
ACL, anterior cruciate ligament; ACLR, ACL reconstruction; KANON, Knee Anterior cruciate ligament, NON-surgical versus surgical treatment; MCS, mental component summary; MOON, Multicenter Orthopaedic Outcomes Network; PCS, physical component summary; QALY, quality-adjusted life-year; SF-6D, Short Form–6 dimensions; SF-36, Short Form–36.
For variables listed as “Distribution,” random samples were taken from the distributions listed.
Zero to 2 years from the initial ACL tear.
Two to 6 years from the initial ACL tear.
Outcomes at 2 and 6 years, respectively.
Includes meniscectomy or meniscus repair.
Includes meniscectomy, debridement, or hardware removal.
Utilities
Utilities in this model were derived from the SF-36 with use of the Short Form–6 dimensions (SF-6D). The SF-6D uses the SF-36 to generate utility by adding patient preferences; it was developed by British health economist John Brazier and has been validated in many disease states. 2 The SF-36 values were taken from the MOON cohort. A clinically stable knee ascertained through rehabilitation was assigned the same utility as a stable knee after surgical reconstruction, 0.82 at 2 years and 0.82 at 6 years and beyond, although the patient who underwent surgical reconstruction was assumed to experience a disutility of surgery to account for the time in a worse health state than an unstable knee when recovering from surgery. These values were relatively low because of the low morbidity of arthroscopic knee surgery and were estimated by expert opinion. Unfortunately, there are little objective data to estimate the disutility and required estimation by expert opinion. The experts were the clinician authors of this study, who are all fellowship trained in sports medicine and would be considered high-volume ACL surgeons. The general approach was to assume 2 weeks in a health state worse than baseline, which accounts for postoperative pain followed by 10 weeks at the preoperative utility. We assumed the improved utility from surgery would be reached at 12 weeks postoperatively. This assumption was for ACLR. Knee arthroscopic surgery was assumed to constitute exactly half of this recovery (1 week for recovery from surgery and 5 more weeks of recovery, reaching an improved utility at 6 weeks postoperatively). A clinically unstable knee was assigned the utility for a preoperative knee undergoing reconstruction in the MOON cohort (Table 1). Unstable knees are those with findings of either subjective instability by the patient or objective instability by the clinician (positive pivot shift). Stable knees are those without either of these findings.
Knee Stability
From the KANON trial, 71% of patients with an ACL tear either chose to undergo ACLR (39%) or had clinically detectable or symptomatic instability at 2 years (32%). This value was used in our model to estimate the number of patients undergoing rehabilitation who were stable and unstable. A sensitivity analysis was performed on the progression to instability beyond 2 years. From the MOON cohort, 3.0% of patients 2 years from reconstruction experienced a retear, so an annual retear rate of 1.5% was used in the model (all 6 years). 27
Procedure Rates
The rate of primary ACLR in the DR group was taken from the KANON trial. Thirty-nine percent (39%) of the initial cohort or 55% of the unstable patients chose to undergo surgical reconstruction by the 2-year follow-up in the KANON trial. This assumption clearly leaves patients in the symptomatic instability health state in the final 4 years of the model. Ten percent (10%) of the remaining unstable patients were assumed to choose reconstruction for the remainder of the model. This is consistent with the MOON cohort in which 11% of all patients underwent ACLR 2 years or more after their initial injury. Other ACLR series in the literature support this assumption, and it was subjected to a rigorous sensitivity analysis.1,5,6 The rates of reoperation were taken from the KANON trial. The specific numbers of physical therapy visits for both postoperative and nonoperative rehabilitation were not available in the article or appendix of the KANON trial. As such, the best practices of the authors were used to estimate this variable: 2 visits per week for 16 weeks were used for postoperative rehabilitation after ACLR. The KANON trial reported that the structured rehabilitation treatment program lasted 24 weeks. We assumed 2 visits per week for the first 12 weeks and 1 visit per week for the final 12 visits. Two visits for 6 weeks were used for rehabilitation after subsequent knee surgeries.
Costs
Because this model is performed from a societal perspective, as is recommended by the Panel on Cost-Effectiveness in Health and Medicine, the costs used in the model are those that are accrued to society rather than to an individual hospital or practice. Although this method may not account for all the itemized differences in cost seen by an individual hospital or surgical practice, it permits a more global comparison between the treatment strategies and avoids the pitfalls of regional cost differences. Therefore, the costs for rehabilitation, ACLR, knee arthroscopic surgery, and revision procedures were estimated starting with the national average Medicare reimbursements for the procedures in 2012 US dollars. Reimbursement for the outpatient facility and professional fees for each procedure were summed to create the total reimbursement. Facility fees were assumed to be 60% ambulatory surgery centers (ASCs) and 40% hospital-based outpatient units. Current Procedural Terminology codes were used to estimate the professional costs.
Cost estimates based on Medicare payment rates may underestimate payments made by private insurers and overestimate payments made by Medicaid and self-insured and uninsured patients. To reconcile these differences, we adjusted our estimates of direct medical costs using payment rates of other insurers (as a percentage of the Medicare rate) and then weighted them by the national distribution of payers for the treatment of ACLR. The payment rate of Medicaid and self-paying patients was set as 80% and 50% of the Medicare rate, respectively. For private insurers, the payment rates reported in the literature were used. 9 Ginsburg 9 reported private insurer payments as a percentage of the Medicare rates for outpatient services in selected areas, ranging from 193% in Cleveland to 368% in San Francisco in 2008. The median of the reported range (280%) was used to adjust the costs of outpatient services. The Medicare Payment Advisory Committee 17 estimated that the private rate for physician services was, on average, 123% of the Medicare rate across all services and areas in 2003. For all other patients, including those paid by workers’ compensation, we assumed that their rate was the same as the average rates of Medicare and private insurers. These costs are shown in Table 1.
Cost-Effectiveness Analysis
The Markov cohort model was used to conduct a cost-effectiveness analysis of the present-day value of the expected costs and QALYs gained over the lifetime of a theoretical patient cohort for each treatment strategy. Outcome measures included average costs, effectiveness (QALYs), as well as the cost-effectiveness ratio for each strategy. A QALY is an outcome measure equal to the expected gains in life expectancy associated with a treatment option, downwardly adjusted for any limitations in quality of life. A year in perfect health is worth 1 QALY, and a year of imperfect health is worth some fraction of 1 QALY.
The incremental costs and effectiveness were also calculated and represent the relative difference between the 2 alternative strategies. The principal outcome measurement calculated was the incremental cost-effectiveness ratio (ICER), which is the ratio between the difference in costs and difference in QALYs of each strategy. In terms of this model, the ICER is expressed as

The ICERs of less than $50,000 per QALY gained were considered to be cost-effective based on a willingness of the health care system to pay (WTP) value of $50,000. In this cost-effectiveness analysis, the preferred treatment strategy was the more effective strategy if ICER < WTP.
One-, 2-, and 3-way sensitivity analyses were performed on all variables in the model. A sensitivity analysis is a process in which model results are repeatedly estimated using modified versions of the model. The ranges of values taken by the output provide a measure for how sensitive a finding is to the model’s underlying assumptions. Variables deemed “sensitive” were those that when changed across a reasonable range also changed the preferred strategy. If the preferred strategy did not change, then the variable was termed “robust.” Data from the MOON cohort were available in distributions, and therefore, a probabilistic sensitivity analysis was used to identify the effect of uncertainty in utility on the preferred outcome. These distributions were normal and defined by the mean ± standard deviation (Table 1). We used a Monte Carlo analysis with microsimulation and a probabilistic sensitivity analysis to generate 95% confidence intervals for the outcomes. A Monte Carlo analysis involves running the model a specified number of times and randomly selecting a value from the distribution as opposed to using the mean as is performed in a Markov cohort analysis.
Results
The model was internally validated against the results of the KANON trial, but external validation was not possible because of the lack of availability of similar studies. Results of the base case are shown in Table 2. For this cohort, over 6 years, the ER group resulted in an average incremental cost of $1572 less than that of the DR group while providing an incremental QALY gain of 0.28 compared with that of the DR group. The cost-effectiveness ratio associated with the ER group was $3881 per QALY versus $4434 per QALY for the DR group. In cost-effectiveness analyses, a treatment strategy is “dominated” when the analysis indicates that it is more costly and less effective than the alternative. Based on the outcomes of the base case analysis, the DR treatment strategy was dominated by the ER strategy, and no ICER value was necessary to compare the two.
Results of Analysis for Base Case a
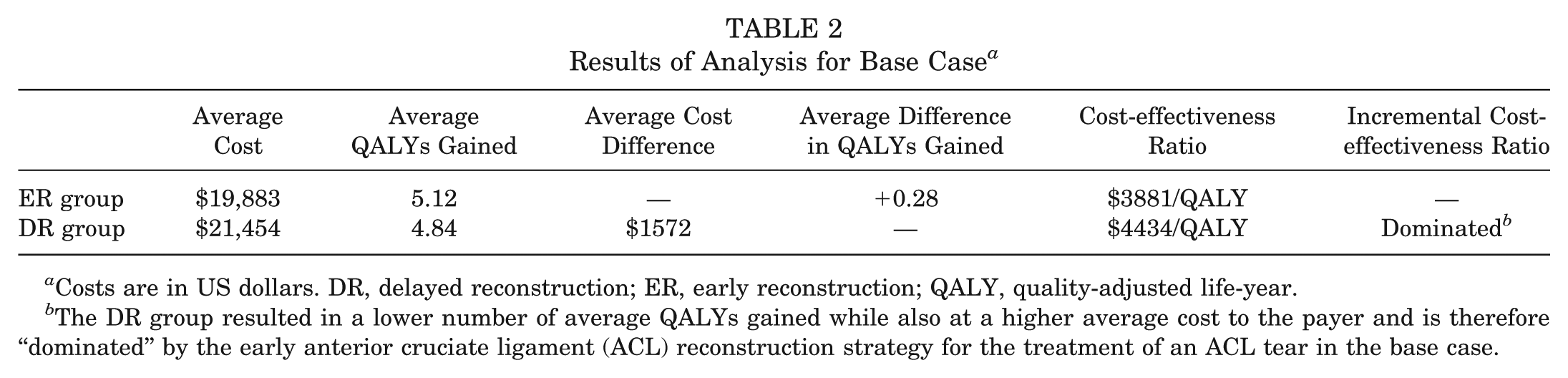
Costs are in US dollars. DR, delayed reconstruction; ER, early reconstruction; QALY, quality-adjusted life-year.
The DR group resulted in a lower number of average QALYs gained while also at a higher average cost to the payer and is therefore “dominated” by the early anterior cruciate ligament (ACL) reconstruction strategy for the treatment of an ACL tear in the base case.
Sensitivity Analyses
Probabilistic Sensitivity Analysis
A Monte Carlo simulation utilizing a probabilistic sensitivity analysis to assess the effect of parameter uncertainty and microsimulation to represent individual patient variability reported that the average (±standard deviation) cost for early ACLR was $19,883 ± $158, with a median of $19,880. The average cost of rehabilitation plus optional delayed ACLR was $21,454 ± $398, with a median of $20,432. The utility of each strategy showed less variability, with an average of 5.12 ± 0.42 and median of 5.16 for early ACLR and an average of 4.84 ± 0.33 and a median of 4.85 for rehabilitation plus optional delayed ACLR. Early ACLR was the preferred cost-effective strategy for 78% of patients, while rehabilitation plus optional delayed reconstruction was preferred for 22% of patients. The incremental cost and benefit of early ACLR compared with rehabilitation plus optional delayed ACLR for each trial are shown in Figure 2. The ellipse captures the 95% confidence interval for the differences between each strategy.
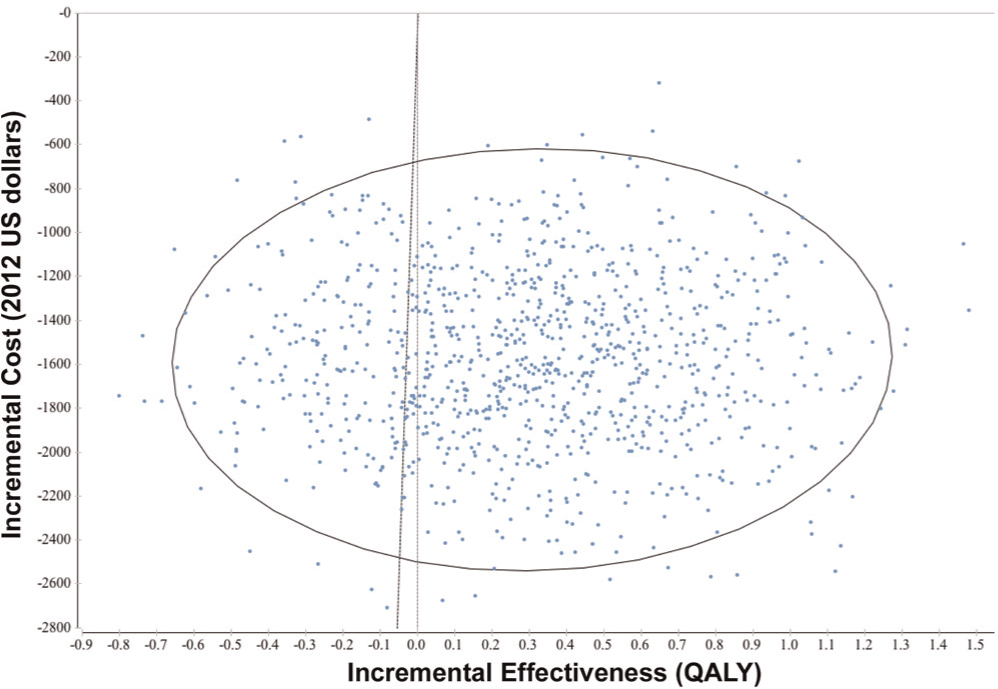
Incremental cost and effectiveness of early anterior cruciate ligament reconstruction (ACLR) compared with rehabilitation plus optional delayed ACLR. Each dot represents an individual patient trial, and the spread of the trials demonstrates the variability due to parameter uncertainty and individual patient variability. Incremental quality-adjusted life-year is found on the x-axis, while cost is on the y-axis. The numbers consider the baseline of early ACLR compared with rehabilitation plus optional delayed ACLR.
Threshold Analysis
One-, 2-, and 3-way sensitivity analyses were performed on all variables in the model. With cost-effectiveness as the outcome measure, 1-way sensitivity analyses of the base-case input variables identified only 1 “sensitive” variable: the rate of instability after initial rehabilitation. With cost only as the outcome, 3 additional variables were found to be sensitive: (1) the proportion of physical therapy visits for rehabilitation compared with surgical recovery, (2) the number of patients choosing delayed reconstruction, and (3) the cost of ACLR. The threshold values for these variables are reported in Table 3. Robust variables, or those in which variation of the inputs did not affect the outcomes of the model, were utility of an unstable knee, costs of rehabilitation and ACLR, disutility of surgery, and the discount rate.
Results of Threshold Analyses a
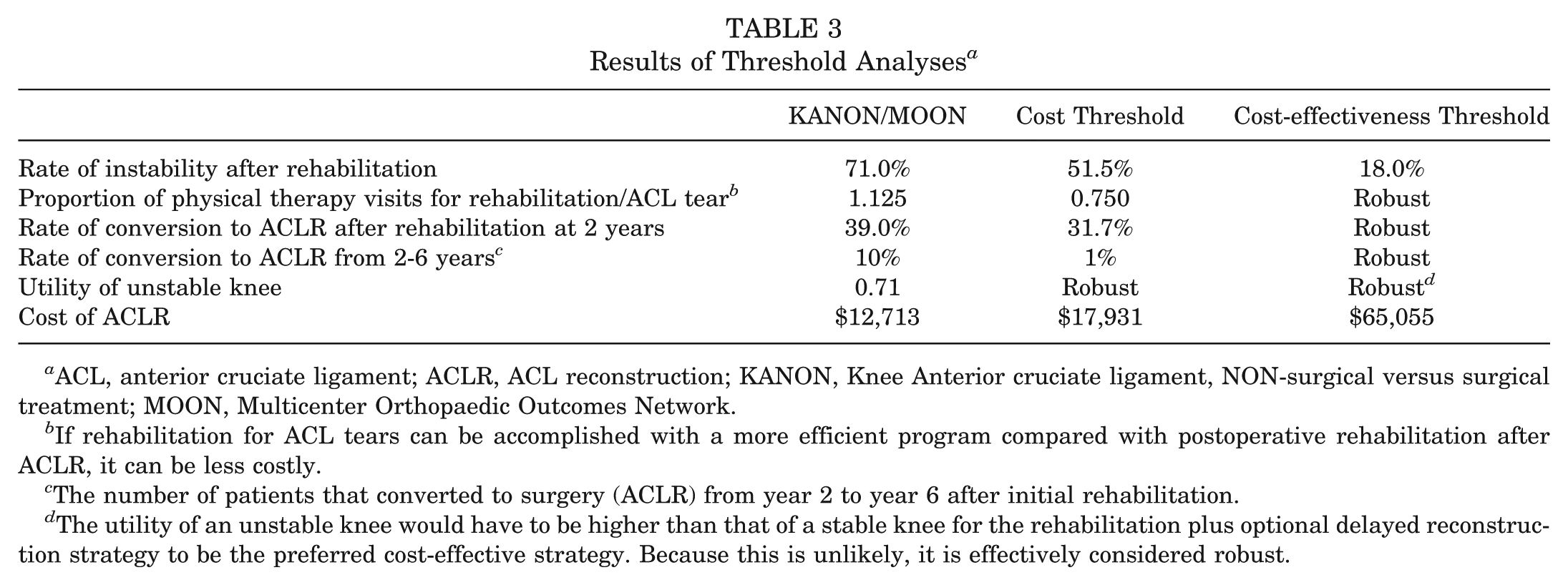
ACL, anterior cruciate ligament; ACLR, ACL reconstruction; KANON, Knee Anterior cruciate ligament, NON-surgical versus surgical treatment; MOON, Multicenter Orthopaedic Outcomes Network.
If rehabilitation for ACL tears can be accomplished with a more efficient program compared with postoperative rehabilitation after ACLR, it can be less costly.
The number of patients that converted to surgery (ACLR) from year 2 to year 6 after initial rehabilitation.
The utility of an unstable knee would have to be higher than that of a stable knee for the rehabilitation plus optional delayed reconstruction strategy to be the preferred cost-effective strategy. Because this is unlikely, it is effectively considered robust.
Knee Stability and Choice to Undergo ACLR
The most sensitive variable in the model was the rate of instability after initial rehabilitation. When the rate of instability falls to 51.5%, DR is less costly, and when the rate of instability falls below 18.0%, DR becomes the preferred cost-effective strategy (Table 3). The proportion of patients who choose ACLR after initial rehabilitation is not sensitive with cost-effectiveness as the outcome but does influence cost alone, especially beyond 2 years. At the conclusion of the KANON trial, 32% of the initial group had clinical instability. If none of these patients choose ACLR, early ACLR costs $115 more, but if all of them eventually choose ACLR, the rehabilitation plus optional delayed ACLR strategy results in an average of nearly a $6000 additional cost per patient. The number of physical therapy visits has important effects at the margin, with cost only as the outcome. If the number of physical therapy visits for structured rehabilitation is equal to or below that for rehabilitation after ACLR, then structured rehabilitation is less costly.
Cost
The cost of ACLR is robust with cost-effectiveness as the outcome. With cost as the outcome, early ACLR becomes less costly below $17,931. The model is highly sensitive to cost for the assumptions made to payer mix and the facility where the ACLR is performed. These results are put into context under different assumptions of payer mix and facility type in Figure 3.
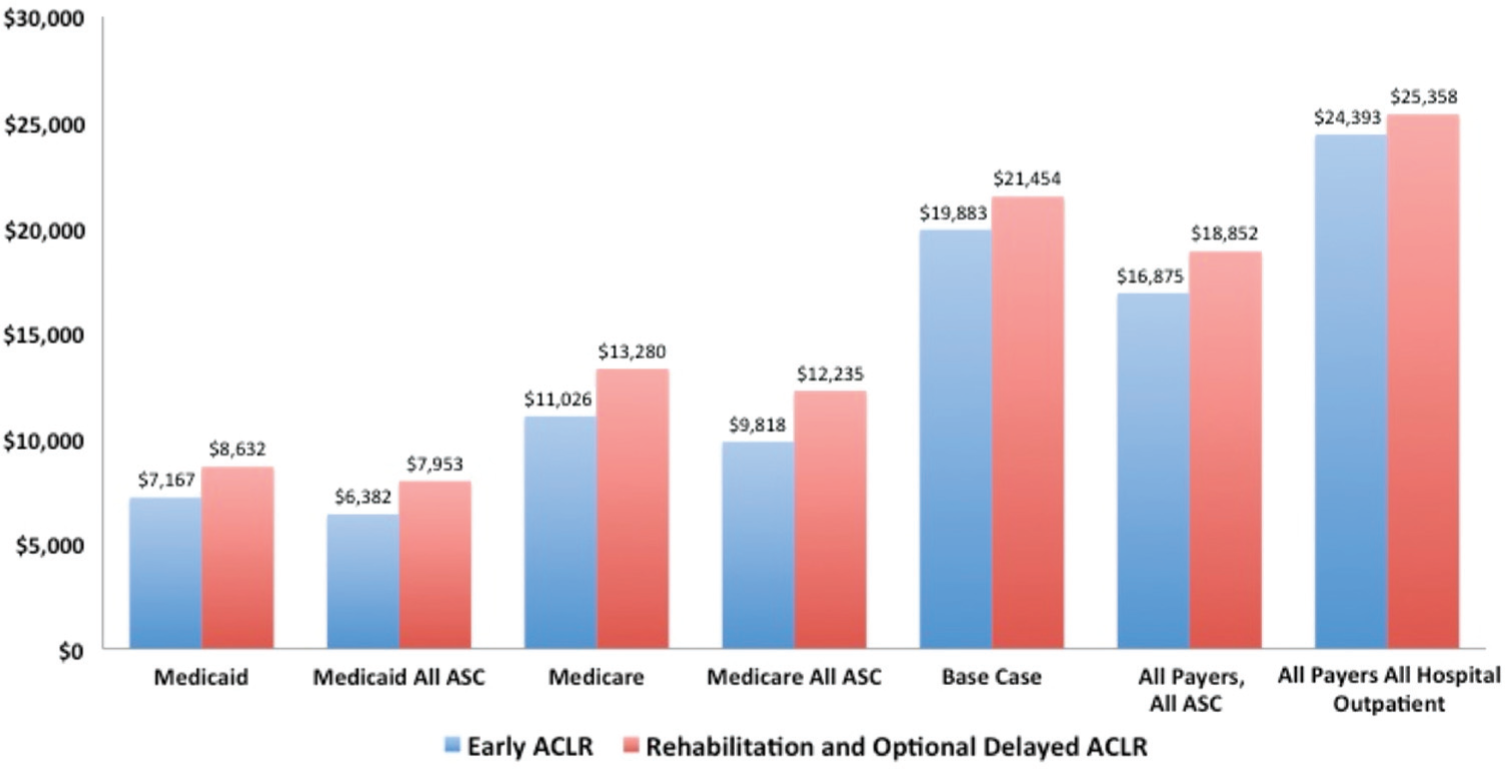
Costs for each strategy across different payers and facilities. ACLR, anterior cruciate ligament reconstruction; ASC, ambulatory surgery center.
Discussion
Conclusions from the KANON trial suggest that rehabilitation plus optional delayed ACLR can achieve equal KOOS outcomes while avoiding surgical reconstructions, thus suggesting that this strategy would utilize fewer resources; however, a complete economic analysis was not performed to support these conclusions. In this study, an economic analysis of the timing of ACLR using data exclusively from the KANON trial, MOON cohort, and national average reimbursement, we found that early ACLR was both less costly and more effective than rehabilitation plus optional delayed ACLR. These findings suggest that when considering optimal societal health care delivery, early ACLR is the preferred treatment strategy.
A close examination of the specific values in the base case reveals that there is a substantial difference in utility, while the costs of each strategy are only slightly different. The difference in utility over the 6 years of the model is largely driven by 2 factors: the lower utility of an unstable knee and the lower utility of a surgically stabilized knee as the time between injury and ACLR increases. With cost-effectiveness as the outcome, variation in these utility values has little effect on outcomes. In fact, variation across the distribution does not change the preferred outcome. Additionally, the proportion of ACL tears with symptomatic instability after rehabilitation needs to fall below 18% to make rehabilitation with optional delayed ACLR the preferred cost-effective strategy.
The KANON study did not report specific utility values, but it did report no difference in average KOOS values, concluding that rehabilitation with optional delayed reconstruction is a viable strategy to decrease the utilization of ACLR without an appreciable decrease in outcomes. This is in contrast to findings of the current study and data from the MOON cohort, which noted decreased utility in the rehabilitation plus delayed reconstruction group. Two factors may explain this: (1) the MOON cohort has a sample size nearly 10-fold that in the KANON trial, and (2) the initial number of meniscus tears in the ER group in the KANON trial was substantially higher than that in the DR group, indicating more severe disease in the ER group. Other authors reported worse outcomes in patients with ACL tears and meniscus tears compared with no meniscus tear.** This may be a confounding variable affecting the KOOS in the KANON study. Second, data from the MOON cohort suggest inferior outcomes for delayed ACLR compared with early ACLR both at 2 and 6 years from the injury, with outcomes from ACLR being worse the later ACLR is performed after the initial injury (SF-6D scores decreasing from 0.03 to 0.06 over time) (Table 1). This finding may actually be confirmed by the KANON trial, with 48% of patients in the DR group experiencing severely decreased knee-related quality of life compared with 18% in the ER group and 14% in the rehabilitation only group. This last finding, combined with a trend toward a greater number of subsequent meniscus symptoms in the DR group, raises substantial concerns about long-term outcomes.
Cost differences between the 2 strategies are affected by several variables, as reported in Table 3. Attention should be paid to the most uncertain variables. As the KANON trial ended at 2 years, an important assumption in the model was the proportion of patients with unstable knees who ultimately chose ACLR (39%) by their 2-year follow-up. This variable is highly sensitive to early ACLR being more expensive if no patients chose ACLR but saving nearly $6000 per patient if all of these patients eventually chose ACLR. This “worst-case scenario” represented an increased annual cost in the United States of $1.2 billion based on 200,000 annual ACLRs. The particular payer and the facility where the surgery is performed are also very sensitive and were addressed in Figure 3. With ASCs being reimbursed at 56% of hospital-based outpatient units, early ACLR saves $1977 per patient if the surgery is performed at an ASC while actually costing $965 more if performed at a hospital-based outpatient unit. The greatest cost saving for either strategy is $2417 saved per patient for early ACLR if ACLR is performed at an ASC at national average Medicare rates. Frobell et al 7 specifically mentioned in their article that rehabilitation techniques and results may be variable. We attempted to address this with a 2-way sensitivity analysis, as seen in Figure 4. If providers can achieve similar or better results to baseline values with fewer visits, rehabilitation is preferred for more patients. This graph also highlights that cost-effectiveness is influenced by both the success of rehabilitation and the number of visits, with a stronger effect from the former. This figure allows an economic analysis of future innovations in rehabilitation or specific provider or patient variations.
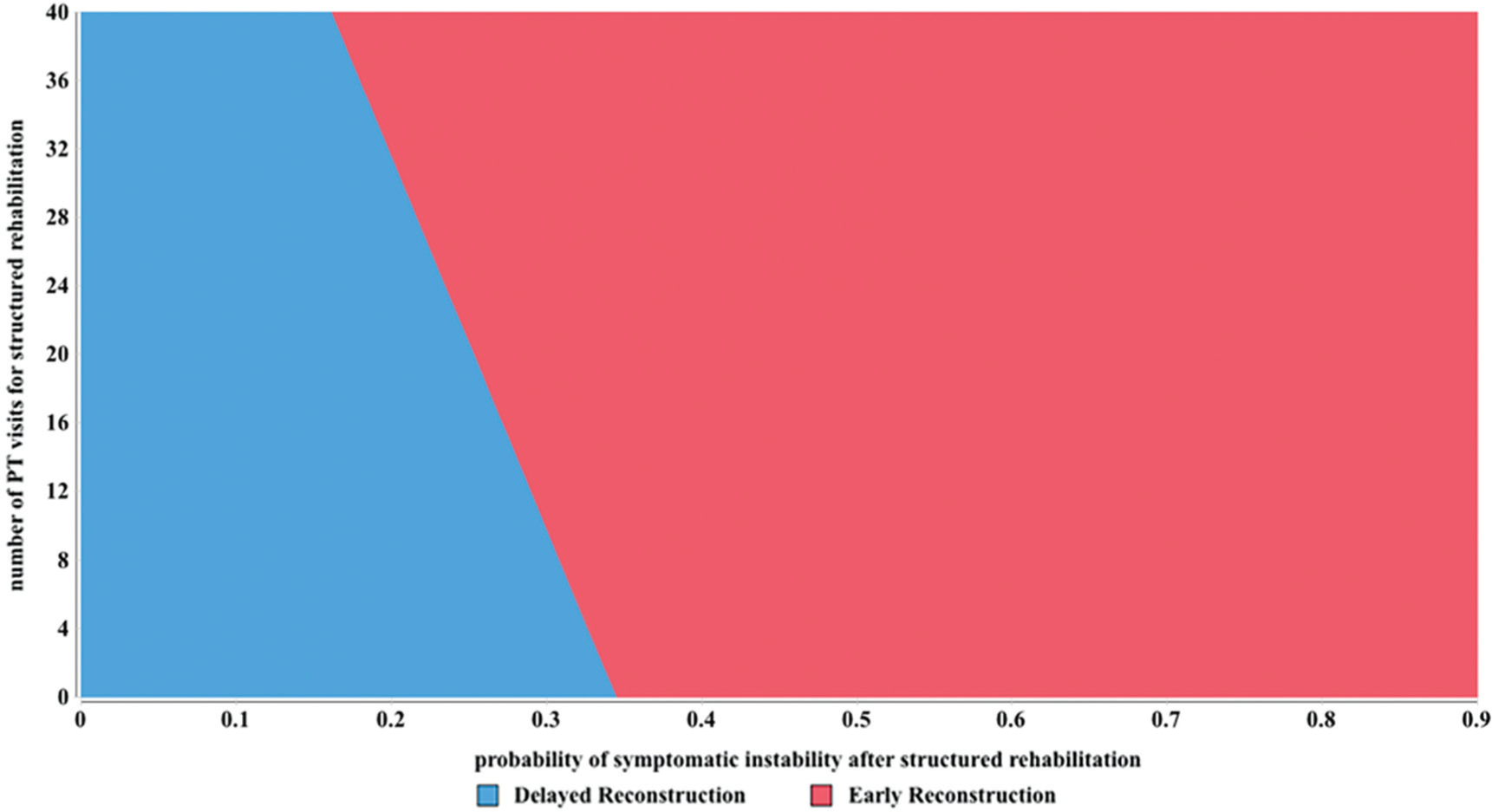
The effect of innovation and/or variability in the structure and success of rehabilitation of anterior cruciate ligament tears. The number of necessary physical therapy (PT) visits is on the y-axis, while the success of rehabilitation is on the x-axis.
We recently published another economic analysis that found a substantial societal burden of ACL tears ranging from $10 to $18 billion annually in the United States. 16 In that study, we found that ACLR was cost saving. There are clear fundamental differences between that study and this one. First, this study is a specific economic analysis of a randomized controlled trial. The KANON trial was a powerful study with policy implications, but it lacked an economic analysis. Second, this study only examined direct costs, not indirect costs as our previous study included. Third, this study examines only the 6 years after injury, while our previous study had a lifetime perspective. Last and possibly most important, the previous study modeled the counterfactual, as the rehabilitation arm in that study could not cross over to ACLR. 16 The current study models a more realistic clinical scenario, assuming the crossover rate in the KANON trial. Modeling the actual clinical pathway is critical to applying an economic analysis to policy and practice. Each study is distinct and addresses specific aspects of an economic analysis.
One of the strengths of a decision analysis is its ability to focus future research. By identifying variables with the greatest effect on cost and effectiveness, we can streamline potentially time-consuming and expensive clinical research to clarify specific critical factors affecting outcomes. Both of these treatment strategies are likely to yield high-quality, low-cost care when performed for the appropriate patient. This is evidenced by 78% of patients achieving better outcomes with early ACLR and 22% of patients doing better with rehabilitation plus optional delayed ACLR in the microsimulation. Opportunities for improvement in decision making for ACL tear treatment, therefore, lie in better understanding patient preferences and patient-centered care. For example, a patient who is at risk of low utility with an unstable knee might be better treated with early ACLR, whereas a low-demand patient who has a lower than average risk of symptomatic instability could undergo rehabilitation first.
There are several limitations to this study. First, we did not model long-term outcomes including meniscus status. Clearly, the effects of ACL tears extend beyond 6 years; however, the understanding of those effects is less certain. We chose to err on the side of using high-level inputs, which resulted in a stronger conclusion in the base case. Second, we did not account for differences in patient or provider variability. The inputs in this model came from a controlled study and a cohort of experienced fellowship-trained sports surgeons. These values may not be representative of the larger population. Next, the MOON’s ACLR cohort did not have a nonoperative counterpart for comparison. To combine data from the MOON and KANON studies, we assumed that the utility for patients with unstable knees was equal to the preoperative utility of patients with chronic ACL deficiency from the MOON cohort. That is, we did not use the preoperative utility for anyone undergoing ACLR within 10 weeks of the initial injury. All utility values were from patients living with symptomatic ACL deficiency. Lastly, while we attempted to estimate costs based on all payer populations, limited data exist to precisely estimate the actual reimbursement as a percentage of the Medicare reimbursement. Furthermore, while using reimbursement as a measure of cost is widely accepted as the preferred technique to estimate costs in an economic analysis, it has its limitations. Reimbursement is a surrogate for costs and does not reflect actual costs. However, obtaining actual costs is currently not possible for any procedure or disease at a state or national level. Actual costs can only be measured at the health system or institutional level. This methodology has substantial limitations in that it may not be generalizable. We recognize the limitations of our approach but do believe that we have executed the best available method of cost estimation.
An economic evaluation is integral to clinical trials; however, the KANON trial lacked a comprehensive economic evaluation despite a conclusion that could substantially affect access to care for ACL tears. We provided an economic analysis using evidence level 1 data from 2 major respected sources. At an average, early ACLR is slightly less costly and substantially more cost-effective for the patient. Greater study in patient-centered care is necessary to determine the optimal treatment strategy for individual patients and providers, but this study demonstrates that early ACLR is a viable treatment strategy when optimal societal health care is the outcome.
Footnotes
One or more of the authors has declared the following potential conflict of interest or source of funding: L.K. has received payment to write or review a paper by the AAOS, funds for research from the AAOS, funds as an employee by the AAOS, and royalties or fees for consulting from the AAOS. Vanderbilt Sports Medicine (K.P.S.) has received research funds from Smith & Nephew. This study was partially supported by National Institutes of Health/National Institute of Arthritis and Musculoskeletal and Skin Diseases grant No. 5R01 AR053684. R.C.M. has a KM1 award for general research support.