
Abstract
Background:
Remplissage is used as an adjunct to arthroscopic Bankart repair (ABR) to reduce recurrent instability. Despite growing evidence supporting efficacy and broader application of the procedure, the absence of a specific procedural code limits knowledge of its utilization, and current surgical indications are not well defined.
Hypothesis:
It was hypothesized that remplissage utilization would increase over the study period and that indications would expand beyond traditionally defined off-track Hill-Sachs lesions.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
Patients undergoing arthroscopic anterior shoulder stabilization from 2012 to 2024 were retrospectively reviewed across multiple institutions. Patients were grouped by ABR alone (ABR) or with remplissage (REMP). Temporal trends were evaluated by comparing early (2012-2020) and late (2021-2024) cohorts. Preoperative magnetic resonance imaging was used to assess bipolar bone loss using established measurement techniques, including glenoid track (GT), glenoid bone loss (GBL), and distance to dislocation (DTD).
Results:
The cohort included 244 patients who underwent remplissage and 1100 patients who underwent ABR. The proportion of REMP increased 4.5-fold over the study period (7.7% in 2012 vs 34.7% in 2024). Later year of surgery was significantly associated with increased remplissage utilization (odds ratio [OR] per year, 1.21 [95% CI, 1.16-1.27]; P < .001). There were no differences in age (P = .53), sex (P = .10), or contact athletes (P = .35) between cohorts. The REMP cohort had more preoperative dislocations (3.1 ± 2 vs 1.5 ± 1.4; P < .001). Among patients with REMP, those in the late subgroup had fewer preoperative dislocations (2.7 ± 1.7 vs 3.9 ± 2.4; P = .01) and lower sports participation (58% vs 71%; P = .04). The late REMP subgroup also demonstrated greater GBL (7.3 ± 6.4% vs 5.6 ± 6.1%; P = .04) and shorter DTD (4.7 ± 4.6 vs 6.1 ± 4.8 mm; P = .03). GT classification did not differ between early and late REMP subgroups (P = .12), with approximately 75% of patients classified as near-track or on-track.
Conclusion:
The utilization of remplissage as an adjunct to ABR has increased 4.5-fold over the past decade. The majority of patients who underwent remplissage in this series had near-track or on-track lesions, suggesting a lower utilization threshold rather than greater pathology severity. This study defines trends in utilization and indications, while future work should determine whether these evolving practices translate into improved outcomes.
Anterior shoulder instability is common among young, active patients and is associated with a substantial risk of recurrent instability after initial dislocation.32,34,41 Bone loss involving the glenoid and humeral head is recognized as a critical contributor to recurrent instability and failure after isolated arthroscopic Bankart repair (ABR).7,10,37 In particular, the Hill-Sachs lesion (HSL) may engage the anterior glenoid rim during the functional range of motion (ROM), predisposing patients to repeat dislocation if not adequately addressed.13,15
The arthroscopic remplissage procedure is a capsulotenodesis of the posterior capsule and infraspinatus tendon into the HSL, preventing engagement with the anterior glenoid rim and creating a posterior tether that limits anterior humeral translation.12,19 The technique was introduced arthroscopically by Wolf and Pollack 46 in 2004 and further described by Purchase et al in 2008. Adoption of remplissage has occurred amid persistent concerns about high recurrence after isolated ABR, with reported long-term recurrence rates ranging from 18% to 57%.1,11,24,30,42,44 Early cadaveric and clinical studies raised concerns regarding loss of external rotation, residual posterior shoulder pain, and lower return to sport among throwing athletes, which contributed to initial hesitancy toward widespread use.12,16,19,31,33 However, more recent literature demonstrates no clinically significant loss of ROM. It supports favorable return-to-sport outcomes, with some studies reporting higher return-to-sport rates than Latarjet or ABR alone.2,8,40 Accordingly, remplissage has gained acceptance as an effective adjunct to ABR, and multiple studies have demonstrated lower rates of recurrent instability compared with ABR alone.2,3,23,27,28,40,47
Despite mentions of expanded indications and broader applications, the true incidence of remplissage remains unknown. 35 The procedure lacks a dedicated procedural code, resulting in heterogeneous coding and documentation practices that limit accurate assessment of utilization from large databases. Furthermore, current indications for remplissage are not well defined. While traditionally reserved for off-track HSLs with subcritical glenoid bone loss (GBL), emerging evidence suggests that remplissage also improves outcomes in high-risk individuals with less severe bone loss, such as young athletes with on-track HSLs.10,26,43 As evidence supporting remplissage continues to expand, an improved understanding of when and how often the procedure is being applied in surgical practice is warranted.
This study aimed to examine how the use of remplissage in conjunction with ABR has changed over time. Specifically, we sought to determine whether the frequency of remplissage has increased over time and whether the procedure has been increasingly applied to patients with less severe patterns of bipolar bone loss. We hypothesized that remplissage utilization has increased over the study period and that indications have expanded beyond traditionally defined engaging or off-track HSLs.
Methods
Patient Selection
A multicenter retrospective cohort study was conducted, including patients who underwent ABR for anterior shoulder instability between 2012 and 2024. Patients were identified via Current Procedural Terminology (CPT) code 29806 (arthroscopic labral repair with capsulorrhaphy) and subsequently confirmed to have undergone surgery for anterior shoulder instability. Procedures identified by CPT code 29806 underwent secondary manual review of operative reports by fellowship-trained surgeons to confirm the presence or absence of remplissage. All procedures were performed by 5 fellowship-trained orthopaedic surgeons (J.Y.B., R.C.R., A.L., T.D., P.J.D.) at high-volume shoulder surgery centers. Patients who underwent primary ABR were eligible for inclusion, regardless of whether a concomitant remplissage procedure was performed. The decision to perform remplissage was based on the surgeon's judgment at the time of surgery. Patients were excluded if they had a history of previous ipsilateral shoulder surgery or underwent concomitant procedures at the time of the index operation (rotator cuff repair, glenoid fracture repair, or bony augmentation). Patients with anterior labral tears extending into the posterior and/or superior labrum who were treated at the time of surgery were not excluded.
Demographic variables included age at the time of surgery, sex, body mass index (BMI), and athletic participation. Athletic status was categorized as either athlete or nonathlete and noncontact or contact. Contact athletes were defined as those who participate in sports that involve regular player-to-player physical contact, including football, rugby, hockey, martial arts, wrestling, boxing, soccer, and basketball.
Quantifying GBL, GL, and DTD
Preoperative magnetic resonance imaging (MRI) was used to assess GBL and HSL characteristics using previously reported measurement techniques. GBL was quantified on T1-weighted sagittal MRI sequences using the best-fit circle method. The percentage of GBL was calculated as the ratio of the maximum width of anterior bone loss to the diameter of the best-fit circle. The Hill-Sachs interval was defined as the maximum distance from the medial portion of the HSL to the insertion of the infraspinatus tendon. Glenoid track (GT) was calculated using the formula GT = 0.83D – d, as described in the literature, where D represents the diameter of the best-fit circle fit, and d represents the width of anterior bone loss. 48 distance to dislocation (DTD) was calculated as the difference between the GT and HSI (DTD = GT – HSI). 25 Lesions with DTD >8 mm were classified as on-track, lesions with DTD <0 mm were classified as off-track, and those between 0 and 8 mm were classified as near-track. 25
Statistical Analysis
Baseline demographic characteristics and radiographic variables were compared between cohorts using univariate analyses. Continuous variables were assessed for normality using the Shapiro-Wilk test. Normally distributed variables were analyzed using t tests, whereas non-normally distributed variables were compared using the Wilcoxon rank-sum test. Categorical variables were compared using χ2 test. To evaluate temporal trends, patients were stratified into early (2012-2020) and late (2021-2024) subgroups within each surgical cohort. The cutoff date was chosen based on emerging evidence demonstrating increased risk of failure with isolated ABR in patients with less severe HSLs. 25 Post-cutoff date was thought to represent a more contemporary period marked by the introduction of the “near-track” concept and increased evidence in support of remplissage to reduce recurrence risk for these patients. Subgroup analyses were performed to compare baseline characteristics and radiographic measurements between early and late time periods within each surgical cohort. Continuous variables were reported as the mean ± standard deviation, and categorical variables were reported as frequencies and percentages. All statistical analyses were 2-sided, with statistical significance defined as P < .05. Analyses were conducted using Stata/SE Version 17.0 (StataCorp).
Results
A total of 1344 patients undergoing arthroscopic anterior shoulder stabilization were included in the study. The cohort included 244 patients who underwent remplissage and 1100 who underwent ABR alone. The mean age at the time of surgery was similar between cohorts (24.6 ± 7.9 for ABR vs 24.2 ± 7.4 for REMP; P = .53). There were no differences in BMI (25.5 ± 4.1 vs 25.6 ± 4.9; P = .67), and the majority of patients in both groups were men (75% vs 80%; P = .10). Rates of athletic participation were comparable, including overall athletic participation (69% vs 64%; P = .19) and contact sport participation (34% vs 30%; P = .35). The REMP cohort had significantly more preoperative dislocations before surgery compared with the ABR cohort (3.1 ± 2 vs 1.5 ± 1.4; P < .001) (Table 1).
Population Characteristics a
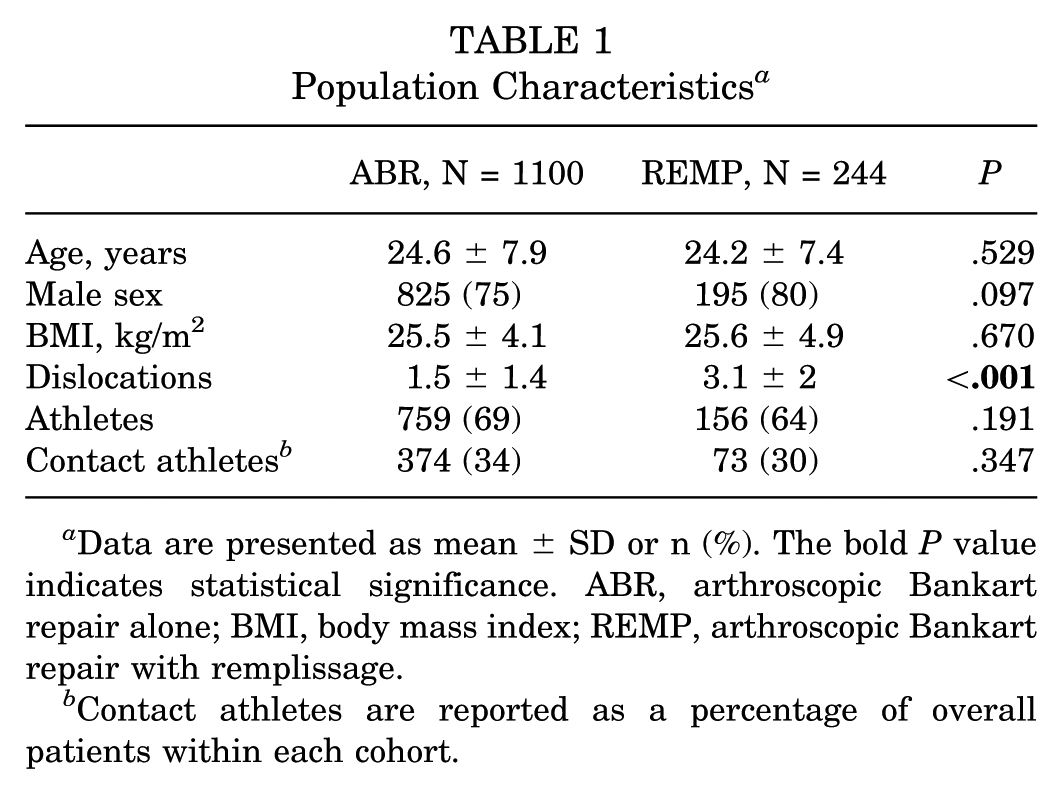
Data are presented as mean ± SD or n (%). The bold P value indicates statistical significance. ABR, arthroscopic Bankart repair alone; BMI, body mass index; REMP, arthroscopic Bankart repair with remplissage.
Contact athletes are reported as a percentage of overall patients within each cohort.
Over the entire study period, the percentage of REMP increased 4.5-fold, from 7.7% in 2012 to 34.7% in 2024 (Figure 1). Later year of surgery was significantly associated with increased remplissage utilization (odds ratio [OR] per year, 1.21 [95% CI, 1.16-1.27]; P < .001).
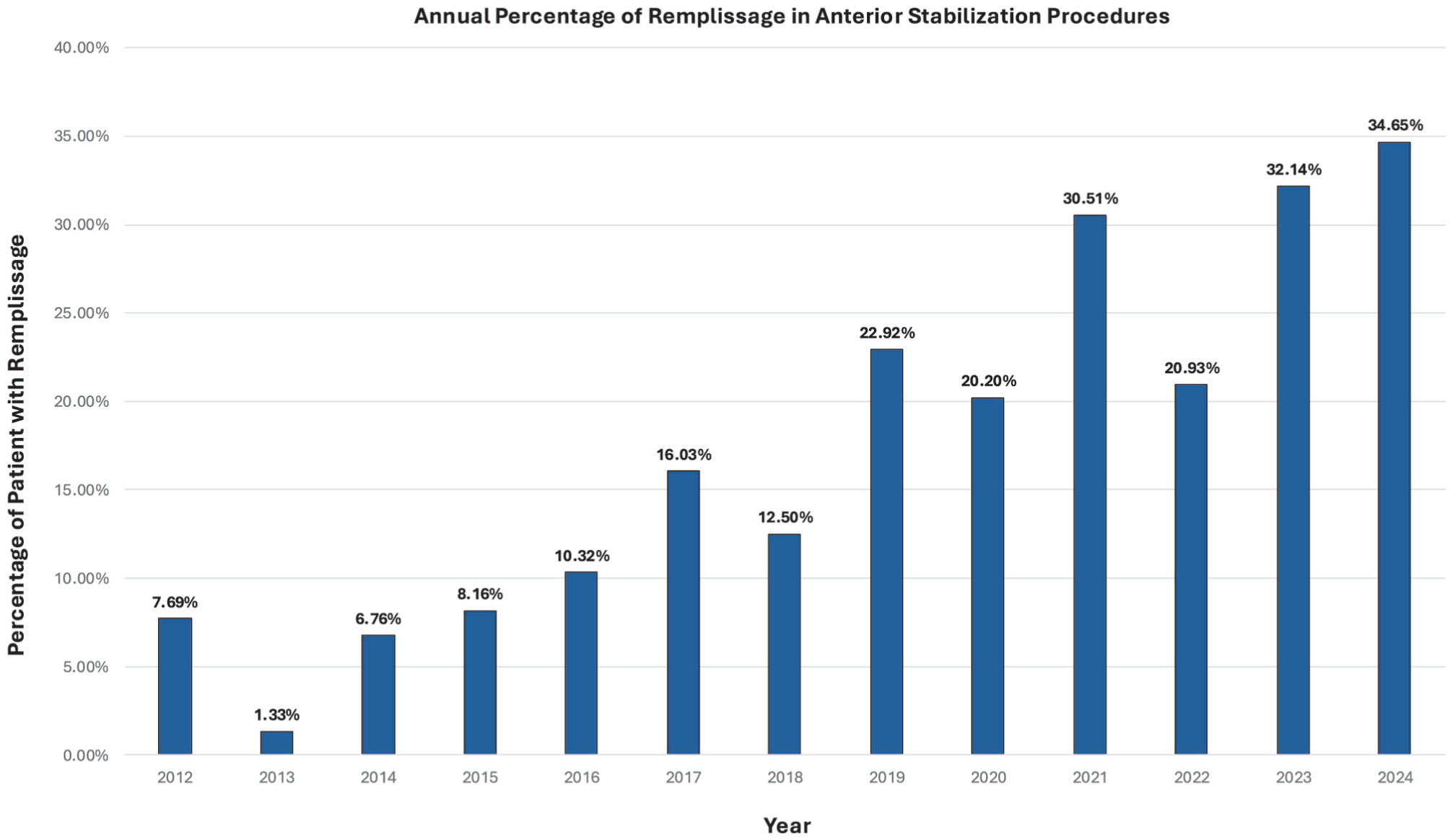
Annual rate of remplissage use as a proportion of total arthroscopic anterior stabilization procedures.
In the REMP cohort, 110 patients underwent surgery before 2021 (45%), compared with 134 who underwent surgery from 2021 to 2024 (55%). Patients in the late REMP subgroup had significantly fewer preoperative dislocations (2.7 ± 1.7 vs 3.9 ± 2.4; P = .01), but no difference in contact sports participation (31% vs 30%; P = .84). GBL was significantly higher in the late subgroup (7.3% ± 6.4% vs 5.6% ± 6.1%; P = .04). HSI was comparable between subgroups, while the late cohort had significantly shorter DTD (4.7 ± 4.6 vs 6.1 ± 4.8; P = .03) (Table 2). There was no difference in GT classification between the early and late subgroups of REMP (P = .12), with the majority of patients at both timepoints having near- or off-track lesions (Table 3).
Patient Characteristics and Radiographic Measures Stratified by Cohort and Time Period a
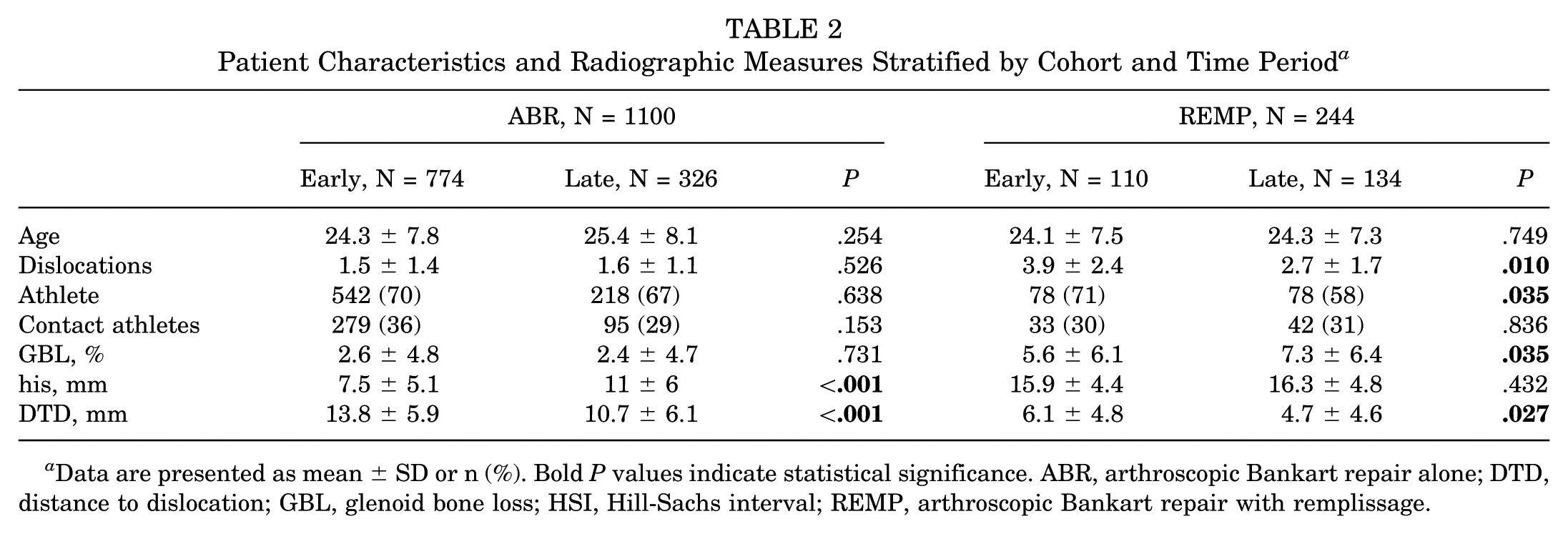
Data are presented as mean ± SD or n (%). Bold P values indicate statistical significance. ABR, arthroscopic Bankart repair alone; DTD, distance to dislocation; GBL, glenoid bone loss; HSI, Hill-Sachs interval; REMP, arthroscopic Bankart repair with remplissage.
Glenoid Track For the Remplissage Cohort Stratified by Time Period a
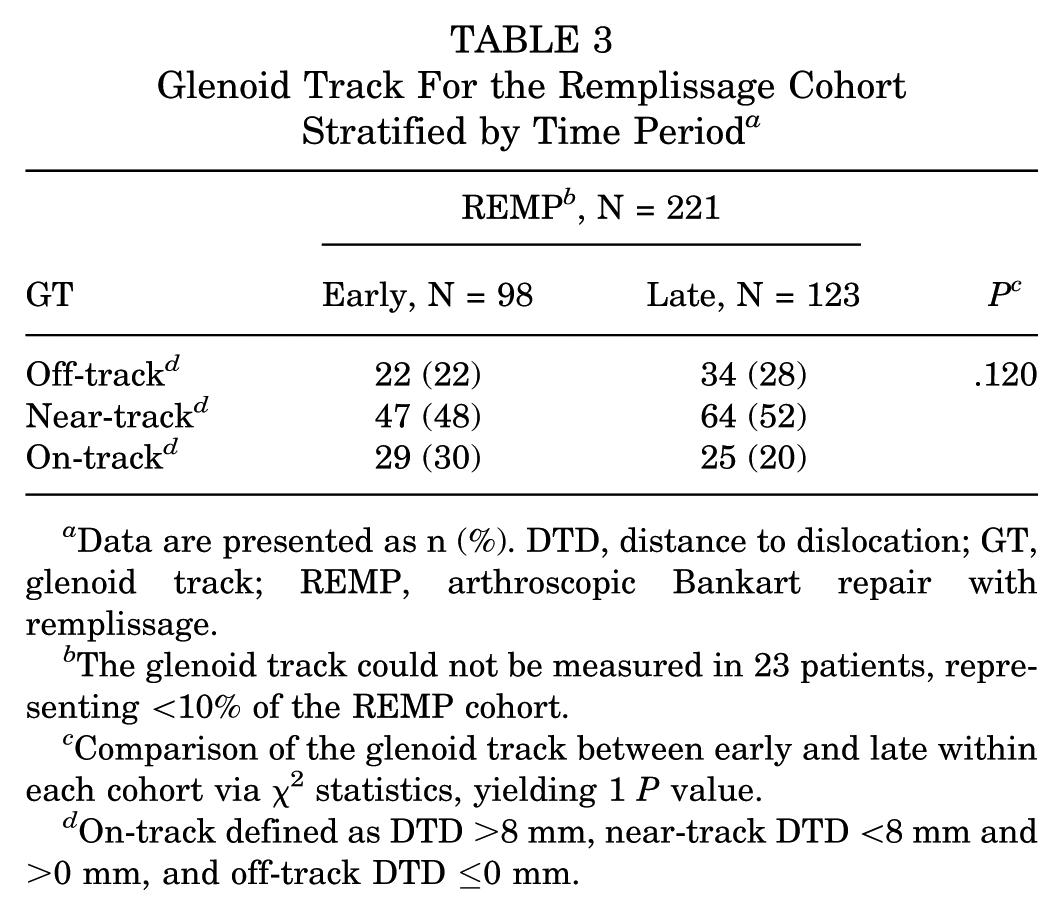
Data are presented as n (%). DTD, distance to dislocation; GT, glenoid track; REMP, arthroscopic Bankart repair with remplissage.
The glenoid track could not be measured in 23 patients, representing <10% of the REMP cohort.
Comparison of the glenoid track between early and late within each cohort via χ2 statistics, yielding 1 P value.
On-track defined as DTD >8 mm, near-track DTD <8 mm and >0 mm, and off-track DTD ≤0 mm.
In the ABR cohort, 774 patients underwent surgery before 2021 (70%), compared with 326 who underwent surgery from 2021 to 2024 (30%). There were no differences in age (24.3 ± 7.8 vs 25.4 ± 8.1; P = .25), number of preoperative dislocations (1.5 ± 1.4 vs 1.6 ± 1.1; P = .53), or contact athletes (36% vs. 29%; P = .15) between early and late cohorts undergoing ABR. Patients in the early subgroup with ABR had similar amounts of GBL compared with those in the late subgroup (2.6% ± 4.8% vs 2.4% ± 4.7%; P = .73). Patients in the late subgroup had significantly larger HSI (11 ± 6 vs 7.5 ± 5.1; P < .001) and shorter DTD (10.7 ± 6.1 vs 13.8 ± 5.9; P < .001) (Table 2).
Discussion
The principal finding of this study is that the use of remplissage in conjunction with ABR has increased substantially over the past decade in our multicenter cohort. Remplissage utilization, as a proportion of all primary ABR, rose from <10% between 2012 and 2015 to 34% of procedures in 2024. Increased utilization has occurred alongside subtle changes in patient selection. The significant increase in utilization suggests a meaningful shift in surgical practice. It helps characterize the use of remplissage, which has not yet been quantified due to the lack of a dedicated procedural code.
Due to the lack of specific coding for the remplissage procedure, our study is the first to quantify the utilization of remplissage as an adjunct to ABR in a large, multicenter setting. We observed an increase in remplissage utilization over the study period, with more than one-third of anterior stabilization procedures incorporating remplissage in 2024. Several factors may explain this increased utilization. Early cadaveric studies raised concern for decreased ROM and increased shoulder stiffness with remplissage, specifically in external rotation, which created hesitation to widespread adoption of the procedure.12,19 While few clinical studies reported similar loss of ROM at short-term follow-up,14,29 numerous studies have shown no restriction in ROM after remplissage compared with isolated Bankart repair at final follow-up.17,40 Furthermore, recent literature suggests lowering the threshold for adding remplissage, as it has proven effective in reducing recurrence rates in patients with on-track HSLs.20,26 Several studies have also shown that ABR with remplissage has significantly lower complication rates and similar recurrence rates compared with open Latarjet in patients with a wide range of GBL and engaging or off-track HSLs.18,21,22 Lastly, mid- to long-term outcome studies have shown maintenance of shoulder function and lower rates of recurrent instability compared with ABR alone.4,6,47 Along with increased familiarity and improvements in surgical technique, we believe these factors have collectively led to increased utilization of remplissage to augment ABR.
In addition to quantifying increased utilization, our findings provide insight into the patient characteristics and radiographic measurements associated with remplissage across the study period. Di Giacomo et al 10 published their recommendations for the management of anterior shoulder instability based on the GT concept. With their treatment paradigm, remplissage was indicated for patients with subcritical GBL (<25%) and off-track HSLs. However, the GT concept does not account for nonanatomic risk factors associated with recurrent instability, such as young age and sports participation, and accumulating evidence suggests5,9,38,39,45 that isolated Bankart repair may fail at GBL thresholds below the traditionally cited 20% to 25%. Hence, current indications for remplissage have expanded and become more nuanced.
We found a decrease in preoperative dislocations and sports participation among patients undergoing ABR with remplissage in recent years, which may reflect a lower threshold for adding remplissage. Similarly, recent literature supports the use of remplissage for patients with less severe pathology, with Lin et al 26 reporting significantly decreased rates of recurrent instability among contact athletes with on-track HSLs. We also found increased GBL and shorter DTD among patients undergoing remplissage in the later subgroup, suggesting a trend toward treating lesions with more severe bipolar bone loss. Notably, these differences were not accompanied by changes in GT classification, as approximately 80% of remplissage procedures in both early and late cohorts were performed in shoulders classified as near-track or off-track. Taken together, this suggests that surgeons may also be increasingly using remplissage to address more borderline or higher-risk lesions within established radiographic categories rather than expanding use to fundamentally different patterns of bipolar bone loss. These findings align with recent literature supporting the use of remplissage as an alternative to Latarjet in patients with greater GBL. 22 Specifically, Horinek et al 21 found no differences in recurrent dislocation, return to sport, or patient-reported outcomes between remplissage and open Latarjet in patients with a mean GBL >25%. Our results support the hypothesis that indications for remplissage have expanded beyond those traditionally referenced, with the procedure increasingly applied across a broader spectrum of bipolar bone loss.
This study has several limitations. Although the multicenter approach improves generalizability, variability in documentation limits the precise assessment of remplissage utilization. To address this, all procedures identified by CPT 29806 underwent secondary manual review by fellowship-trained surgeons to confirm the presence or absence of remplissage. Radiographic measurements, while performed using validated techniques, are subject to inherent variability, and our analysis was limited to preoperative imaging and did not correlate with postoperative clinical outcomes. Importantly, this study was not designed to evaluate recurrence, functional outcomes, or complications associated with remplissage, as its primary aim was to characterize the incidence and evolving indications rather than its effectiveness. Future studies should build on these findings by prospectively evaluating clinical outcomes associated with changing indications, including recurrence rates, return to sport, and patient-reported outcomes, to better define the optimal role of remplissage within contemporary anterior shoulder instability treatment algorithms. Furthermore, future studies would benefit from a dedicated procedural code to better understand incidence and indications.
Conclusion
The use of remplissage as an adjunct to arthroscopic Bankart repair has increased 4.5-fold over the past decade at high-volume centers. Indications have evolved, with the majority of patients undergoing remplissage in this series having near-track or on-track lesions, suggesting a lower threshold for utilization rather than increased pathology severity. This study highlights utilization and indication trends across multiple institutions, while future work should determine whether these evolving practices translate into improved outcomes.
Supplemental Material
sj-docx-1-ajs-10.1177_03635465261456225 – Supplemental material for Changes in Rate and Indications for Remplissage When Performing Arthroscopic Bankart Repair for Anterior Shoulder Instability
Supplemental material, sj-docx-1-ajs-10.1177_03635465261456225 for Changes in Rate and Indications for Remplissage When Performing Arthroscopic Bankart Repair for Anterior Shoulder Instability by Benjamin L. Brej, Ryan C. Rauck, Kyle S. Huntley, Tal David, Patrick J. Denard, Albert Lin and Julie Y. Bishop in The American Journal of Sports Medicine
Footnotes
Submitted February 1, 2026; accepted April 19, 2026.
The authors have declared that there are no conflicts of interest in the authorship and publication of this contribution.
Ethical approval for this study was obtained from The Ohio State University Office of Responsible Research Practices (Approval Number: 2024H0084).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.