
Abstract
Low-flow blood pumps rated under 1 L/min are emerging for new medical applications, such as hemofiltration in acute use. In those pumps, platelet adhesion and aggregation have to be carefully considered because of clogging risk in the filter part. To find an acceptable hemocompatibility that can be applied to low-flow centrifugal blood pump design, the platelet aggregation index, clogging on a micromesh filter, and the hemolysis index were investigated using a low-flow blood pump designed for hemofiltration use. We conducted circulation testing in vitro using fresh porcine blood and two centrifugal pumps with different impeller inlet shapes. The Negative Log Platelet Aggregation Threshold Index (NL-PATI), which reflects the ability of residual platelets to aggregate, and flow rate were measured during reflux for 60 min, and the Normalized Index of Hemolysis (NIH (g/20 min)) was calculated. In addition, blood cell clogging after reflux was observed on the micromesh filter by SEM, and the adhesion rate was calculated. Our results showed that the platelet clogging on the micromesh filter occurred when the average NL-PATI was greater than 0.28 and the average NIH (g/20 min) was greater than 0.01. In contrast, platelet clogging on the micromesh was suppressed when NL-PATI was less than 0.17 and the NIH (g/20 min) was less than 0.003. These values might be used as acceptable hemocompatibility of low-flow centrifugal blood pumps with suppressed platelet clogging for hemofiltration pumps.
Keywords
Introduction
Low-flow blood pumps rated under 1 L/min are emerging in new medical application fields, such as for acute hemofiltration of adults or for pediatric circulatory assist.1,2 In particular, a hemofiltration device in new fields, such as terminal or acute use, needs portability, and compactness.3,4 A centrifugal blood pump, which has better portability and good durability because it can be small and slow tube damage compared to a conventional roller pump, is expected to be applied to hemofiltration systems having venous access for emergency care. 1
The same as a conventional centrifugal blood pump for extracorporeal membranous oxygenation (ECMO) or ventricular assist devices, low-flow centrifugal blood pumps for hemofiltration use will require careful consideration of hemocompatibility, such as hemolysis and thrombogenesis, to reduce neurological complications, mortality, and pump trouble.5–8 Among the problems of hemocompatibility, we focused on platelet adhesion and platelet aggregation, which are important for suppressing clogging risk in the filter part. Platelet aggregation occurs due to platelet activation by shear stress in a blood pump. 9 Some studies have shown the relationship between platelet activation and shear stress based on computational fluid dynamics (CFD) analysis or experiments with a shear stressor,10–12 and these data can be used to design a pump with low platelet activation. However, Gross-Hardt et al. have shown by CFD results that the hydraulic efficiency dramatically decreases and the internal flow recirculation rate increases when existing high-flow rotary blood pumps, which are normally used at about 5 L/min, are operated at blood flow rates below 1 L/min. 13 They reported adverse effects on platelets due to multiple exposures to high shear stress. Flow generated in low-flow centrifugal blood pumps with small size has the possibility of different effects on platelet aggregation compared with high-flow centrifugal blood pumps, and the effects on platelets in actual pumps are unknown. In addition, while CFD analysis has the advantage of being able to predict the details of the flow in a pump, it also has the disadvantage that the solution differs depending on the choice of computational model, and it is difficult to incorporate a complex model of blood. It is an issue to develop the design from a hemocompatibility viewpoint for a low-flow centrifugal blood pump for hemofiltration with less clogging. It is important to find the acceptable quantitative hemocompatibility that could be applied to pump design by experiments using an actual pump even if the details of the flow in the pump are unknown. Thus, we investigated hemocompatibility, which depends on secondary flow, exposure time, and shear rate, in vitro using a low-flow centrifugal blood pump for hemofiltration use. As a basic study, different flows were investigated by using two pumps, one with a normal design and the other with an intentionally design to exert a higher destructive force on blood cells. The purpose of this study was in vitro assessment of platelet aggregation, filter clogging, and hemolysis using pumps that have different flow characteristics for developing a low-flow (<1 L/min) centrifugal blood pump with low platelet aggregation.
Materials and methods
Prototype centrifugal blood pumps and experimental conditions
As shown in Figure 1, two centrifugal pump prototypes (pumps A and B) with different impeller inlet shapes were prepared to find the acceptable quantitative hemocompatibility that could be applied to pump design by experiments using an actual pump. Both pumps consisted of a casing, a drive motor, and a closed impeller with a double pivot bearing. Because hemocompatibility is affected by flow circulation and shear stress,9,13 the two pumps were designed to have distinctly different flow characteristics.
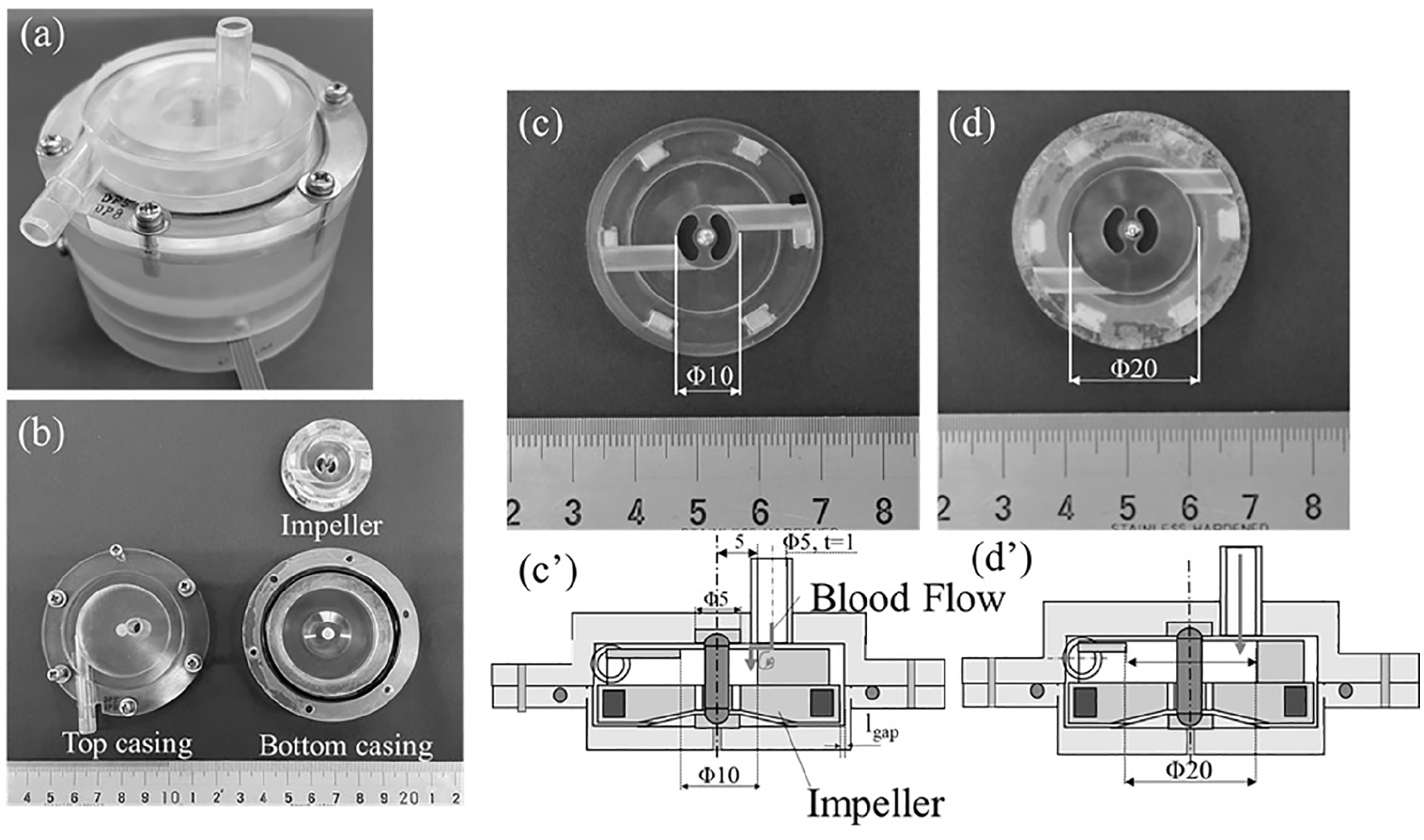
Two designs for a low-flow centrifugal blood pump. The impeller has a diameter of 38 mm, has a shaft at the center, and is supported by a double pivot bearing with a diameter of 5 mm made of ultra-high-molecular-weight polyethylene (UHMWPE) and pivot ball with a diameter of 3 mm made of stainless steel (SUS316). (a) Photograph of the assembled pump with motor. (b) Exploded view of the pump. The pump consists of a top casing, a bottom casing, and an impeller. Pumps A and B use the same casing, and only the impeller is different. (c) Impeller of centrifugal pump A; high destructive force on blood cell is expected with an inlet diameter of 10 mm. (c′) Schematic cross-sectional view of pump A. (d) Impeller of centrifugal pump B; low destructive force on blood cell is expected with an inlet diameter of 20 mm. (d′) Schematic cross-sectional view of pump B.
Pump A was prepared intentionally to exert a higher destructive force on blood cell. As shown by the blood flow path in Figure 1(c′), the flow from the inlet port of the pump hits the upper surface of the impeller. A turbulent flow may cause due to a small opening for the inlet diameter of the impeller that transfers blood flow between the upper surface of the impeller and the casing, and it is predicted to increase destructive force on platelet by repeated loading. On the other hand, pump B was designed for continuous 1-week animal experiments of the pump for blood purification use, and fluid dynamic performance of pump B meets clinical requirements. The impeller for pump B has a wide opening shape for the inlet diameter of the impeller, and pump B was expected to exert a lower destructive force on blood cell than that of pump A.
Because the same top and bottom casing are used in pumps A and B, the gap surrounding the inlet part between the impeller surface and the casing is the same for both pumps. The inlet port of both pumps is set at a position offset by 5 mm from the central axis to stabilize the pivot bearing by avoiding direct flow from the inlet port to the pivot bearing. The pump pressure head was 60 mmHg for both pumps when the pump speed was 2500 rpm and the flow rate was 500 mL/min.
As shown in Figure 2, the pump was connected by a closed circuit to a triangular soft reservoir, a 150-μm micromesh filter having a diameter of 25 mm, and a flow meter (FD-XS8; Keyence Co., Ltd., Japan) set downstream of the micromesh filter. The closed circuit was filled with prepared whole porcine blood at 37°C, and the flow rate was measured during operation of the centrifugal pump, which was driven at a constant rotational speed of 2500 rpm.
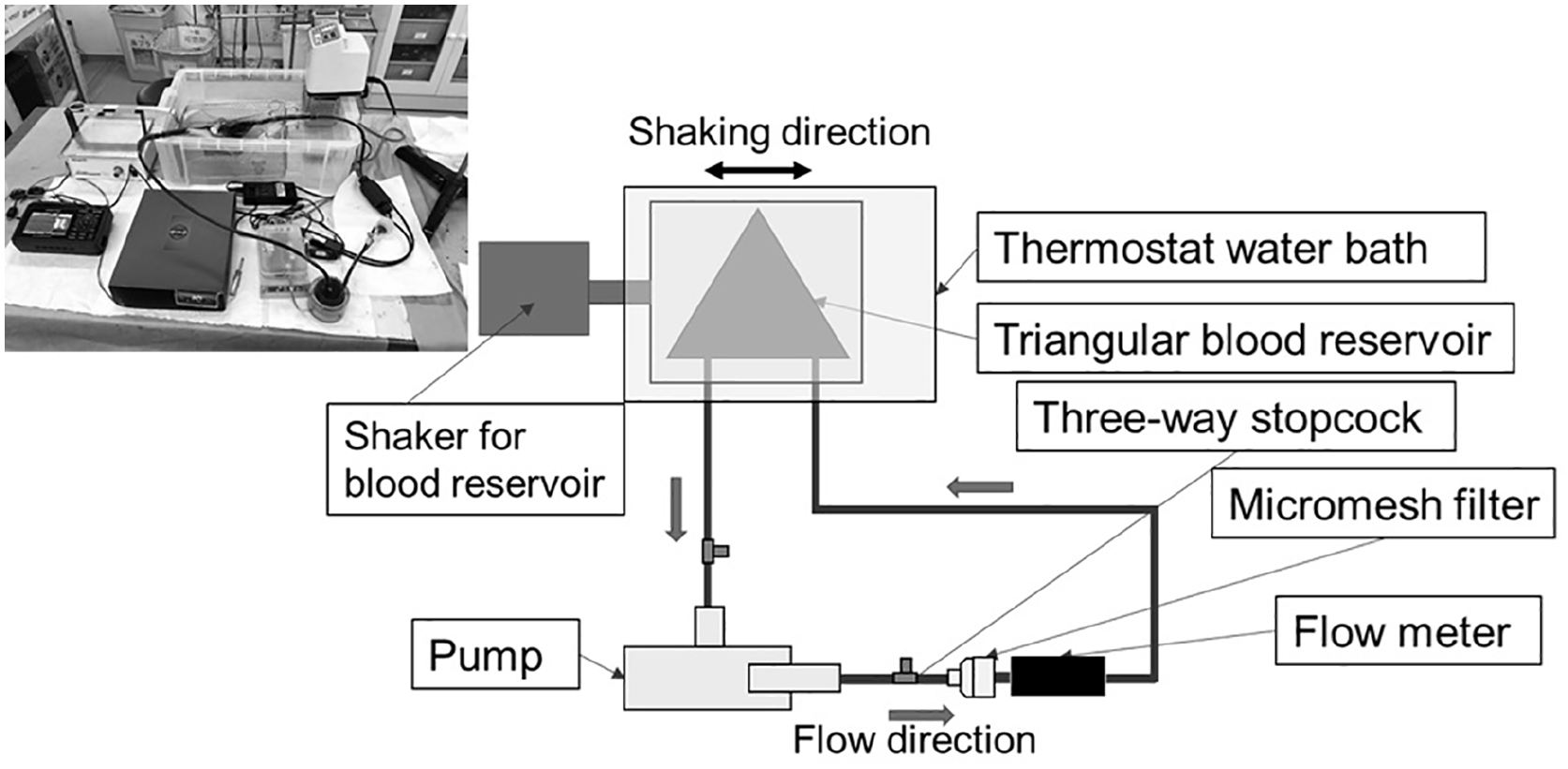
Blood circulation during in vitro test. The closed circuit consisted of the designed low-flow centrifugal blood pump, micromesh filter, flow meter, and triangular blood reservoir maintained at 37°C by a thermostat-controlled water bath.
Blood preparation
Porcine blood was used in this study because bovine, goat, and porcine blood samples are usually employed in animal tests, and porcine blood is often used in commercial contract animal experiments for anti-thrombus tests. Porcine blood collected at a slaughterhouse was initially anticoagulated with 3.2% (w/v) sodium citrate (final concentration of 0.32% (w/v)), and the experiment was started within 2 h after collection. Four milliliters of heparin was added to 400 mL of whole blood to prevent fibrin thrombus formation immediately before the start of the experiment, and then the closed circuit was filled with prepared whole blood. The inlet and outlet of the soft reservoir were clamped before the pump was started, and about 20 mL of 2% (w/v) calcium chloride (Otsuka Calcium Chloride Injection 2% (w/v); Otsuka Pharmaceutical Co., Ltd.) was added and mixed into the reservoir to dissolve the citric acid anticoagulant and restart the platelet activation. The added amount of 2% (w/v) calcium chloride was calculated as the molecular weight ratio needed to cancel the chelating effect of the added sodium citrate, and the amount of calcium contained in the original blood was considered to remain there during the experiment. The activated clotting time (ACT) was measured in advance with an ACT measuring device (HEMOCHRON Response; Accriva Diagnostics Holdings, Inc., USA) when sodium citrate, heparin, and calcium chloride were added to the blood at the mixing ratio described above, the measured ACT was >1500 s. Three time tests were conducted using three different porcine blood batches prepared the same way, and the same batch of porcine blood was used in pumps A and B in each test.
Measurement of platelet aggregation
To quantitatively evaluate changes in platelets during blood circulation, the degree of platelet aggregation in whole blood and the platelet count were measured.
The pump was driven for 2 min after the addition of calcium chloride. Then, 2.5 mL of blood was collected at 2-min intervals after the addition of calcium chloride up to 10 min, and then at 10-min intervals from 10 to 60 min. Each 1.8-mL sample of collected blood was stored in a sodium citrate tube (Venoject II; Terumo Co., Ltd., Japan) for measuring platelet aggregation.
The degree of platelet aggregation in whole blood in a sodium citrate tube was assessed using a screen filtration pressure device (Hematracer ZEN; LMS Co., Ltd., Japan). 14 Platelet aggregation was recorded as a platelet aggregation threshold index (PATI) value. The PATI is the concentration of the agonist (collagen) at 50% of the pressure rate through a micromesh filter with platelet aggregation.
A small PATI represents high platelet aggregation and is calculated as a logarithm because blood with double-dilution agonist was suctioned; therefore, the negative log PATI was recalculated as NL-PATI, which demonstrates the ability of residual platelets to aggregate after shear loading. When the value of PATI ⩽ 0.4 (NL-PATI ⩾ 0.39) and is Class I or higher, it is clinically considered to indicate platelet hyperaggregation in the device.
Measurement of blood clogging on the micromesh filter
As a quantitative evaluation of clogging on the filter, the change in flow rate with time was measured. The flow rate was recorded every 0.1 s with a flow meter (FD-XS8; Keyence Co., Ltd., Japan) during reflux for 60 min.
As a quantitative evaluation, the micromesh filter was photographed after reflux for 60 min. The adhesion rate of blood cell in the photographed image was calculated with Image J analysis software (National Institutes of Health, USA). After being read as a 2016 × 1512 pixel TIF image, the micromesh part was cut out as a circle and used as the “whole area.” The color brightness threshold was set to 220 and converted to an 8-bit grayscale. The “non-adhered area” was calculated by binarizing the cropped image with a threshold of 244. After subtracting the “non-adhered area” from the “whole area” to calculate the “adhered area,” the adhesion rate with respect to the “whole area” was calculated.
Furthermore, to investigate the details of clogging on the micromesh filter, blood cells on the mesh fibers of the filter were observed using a scanning electron microscope (SEM) (TM1000; Hitachi High-Technologies Co., Ltd., Japan). After refluxing, the mesh filter was taken out, washed gently twice with 5 mL of saline, and photographed before drying. The blood cells on the micromesh filter were fixed in 2% glutaraldehyde in PBS solution for 2 h at 4°C, and dehydrated with 50%, 70%, 90%, and 99.5% ethanol for 10 min each. Blood cells were observed with a SEM after platinum deposition.
Measurement of hemolysis
As an index showing the effect of shear flow generated by each pump in blood, a hemolysis test was conducted. One milliliter of whole blood in a tube was centrifuged at 2000 × g for 10 min at 4°C (PMC-060, TOMY Co., Ltd., Tokyo, Japan), and the plasma was sampled to quantify plasma free hemoglobin after shear loading. Plasma free hemoglobin was measured using the 3,3′5,5′-tetramethylbenzidine (TMB) method with a commercial kit (527-A Plasma Hemoglobin; Sigma Diagnostics Inc., St. Louis, MO, USA), which employs TMB, a 90% (v/v) acetic acid solution, and a 0.3% (v/v) hydrogen peroxide solution. 15
The hemolysis level was calculated as the Normalized Index of Hemolysis (NIH (g/20 min)), which was obtained by multiplying the rate of change in total free hemoglobin in the circuit over 20 min:

where
The term
Equation (1) is a modification of the index defined in standard ASTM-F1841 to express the plasma free hemoglobin amount for the same sampling time of 20 min. This equates to a pumped blood volume of 100 L at a flow rate of 5 L/min, and it newly defines the index NIH (g/20 min). 16
Statistics
Platelet aggregation, blood cell count, and hemolysis results were statistically compared with the F-test followed by the t-test using an Excel spreadsheet (Microsoft Co., Ltd., USA).
Results
Results for platelet aggregation and hemolysis
Figure 3 shows the results for average NL-PATI and NIH. As shown in Figure 3(a), the average NL-PATI of pump A is higher than that of pump B. Pump A was predicted to have high shear stress at the inlet, and it had an average NL-PATI value of 0.28, 1.6 times higher than that of pump B (NL-PATI = 0.17), which was predicted to have low shear at the inlet. The NL-PATI value of pump A was lower than the value that is a clinically problematic platelet-activating state (NL-PATI ⩾ 0.39). In addition, the average NL-PATI of pump A may be considered as a reference value at which high clogging of blood cells occurs during perfusion in an in vitro circuit with porcine blood.
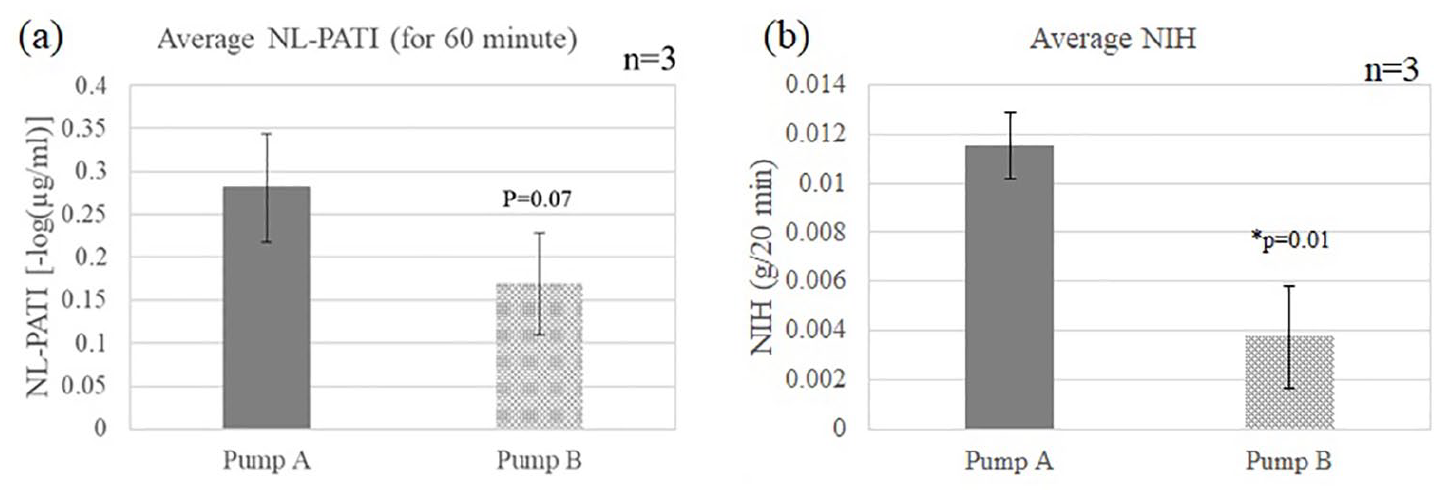
(a) Average NL-PATI (degree of platelet aggregation in whole blood) from three tests. A high number indicates high platelet aggregation. Error bars show standard deviation. Values for Pump A are higher than those for Pump B with a p-value of 0.07. (b) Average NIH (index of hemolysis per 20 min) from three tests. Error bars show standard deviation. Values for Pump A are significantly higher than those for pump B with a p-value of 0.01.
The NIH of Pump A was also significantly higher than that of pump B. The hemolysis index per 20 min was NIH = 0.0134 (g/20 min) for pump A and NIH = 0.0039 (g/20 min) for pump B in test 1, as shown in Figure 3(b). The results for test 2 were NIH = 0.0104 (g/20 min) for pump A and NIH = 0.0062 (g/20 min) for pump B, and the results for test 3 were NIH = 0.0107 for pump A and NIH = 0.0011 for pump B. The average NIH in the three tests of pump A was 0.01, and it was about three times higher than that of pump B (NIH = 0.003).
Results for flow rate and adhesion rate on the micromesh filter
Figure 4 shows the flow rate and platelet adhesion rate for pumps A and B in the three tests. Some fluctuation in the graph for flow rate reflects blood collection by a syringe through a three-way cock. In test 1, the flow rate of pump A increased slightly until about 35 min but decreased thereafter. In pump B, the flow rate repeatedly increased and decreased but finally increased. Regarding tests 2 and 3, the flow rate of pump A decreased greatly with time. The flow rate of pump B slightly increased in test 2 and decreased and then increased after about 20 min in test 3. In the 60-min reflux test, the flow rate of pump A finally decreased and that of pump B increased.
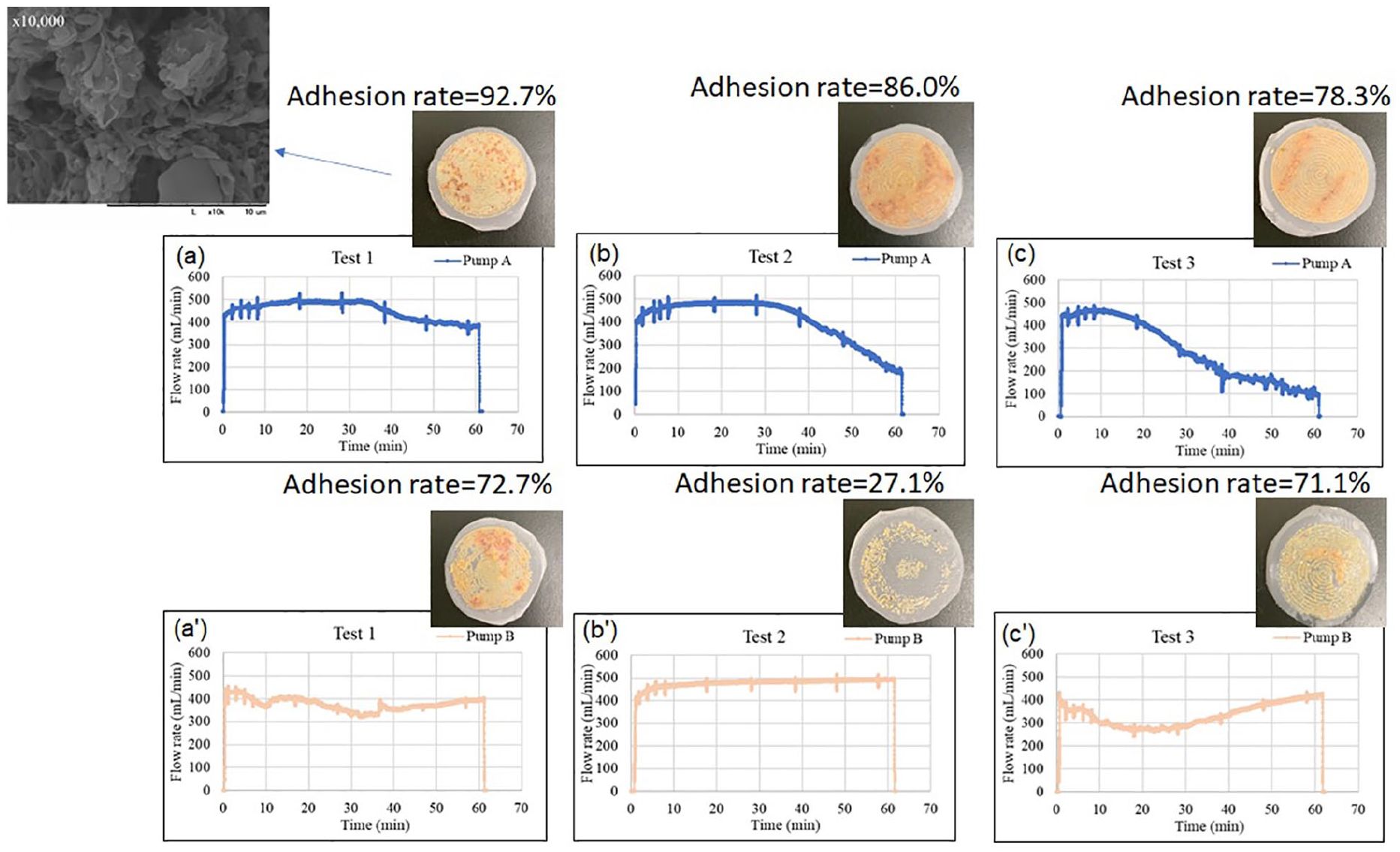
Flow rate and pictures of micromesh filters with corresponding adhesion rates. (a–c) Flow rate of pump A in tests 1, 2, and 3, respectively. (a′–c′) Flow rate of pump B in tests 1, 2, and 3, respectively. Each picture of platelet adhesion indicates the final adhesion condition after attachment and peeling for each 60-min test, and the adhesion rate is shown as percentage of blood cell adhesion on the micromesh filter.
After the three tests, the final platelet adhesion on the micromesh filter after 60 min had almost same shape as a circle, especially for pump A. Further, the adhesion rate of pump A was higher than that of pump B in all tests, as shown in Figure 4. SEM observations showed that the clogging of the filter generated by flow in the low-flow-rate centrifugal pump was caused not by protein but by platelets.
The degree of platelet clogging on the filter correlates with the flow rate change. Platelets in the circuit were repeatedly attached to and detached from the filter, but some became physically trapped because the filter acted like a net. In addition, as platelet adhesion progressed and the platelet accumulation on the filter thickened, the filter became almost completely clogged and layers of red blood cells accumulated. This phenomenon caused a significant decrease of the flow rate in pump A.
Figure 5 shows the average adhesion rate in the three tests. There was no significant difference between the adhesion rates of pumps A and B, but the average value was higher for pump A.

Comparison of average adhesion rates from three tests. Error bars show the standard deviation.
Discussion
Acceptable hemocompatibility for design of a low-flow centrifugal blood pump
The shear rate applied to the inside of the pumps was calculated for both pumps A and B. At 2500 rpm, the shear rate γu (per second) loaded on the outer circumference of the impeller (position at radius r = 17 mm) was determined as

where
Therefore, the shear rate of both pumps applied to the outer circumference of the impeller is 15,000/s in a simple calculation (shear stress is about 45 Pa). The two pumps created a shear load on the order of about 10,000/s at the outer impeller tip at 2500 rpm. Because it is considered that platelet activation occurs at a shear rate of about 150 Pa for 0.5 s, 11 it is possible that platelets are activated at the outer tip. When the two pumps are compared, it is considered that pump A, which has a smaller impeller inlet diameter, has a secondary flow at the upper part of the impeller because the blood flow from the inlet port collides with the upper surface of the impeller. Due to the combined load of shear rate and exposure time in the pump, pump A seems to have a higher platelet aggregation and hemolysis index than pump B.
The obtained aggregation and hemolysis values might provide a design reference index from the aspect of hemocompatibility for designing a low-flow centrifugal blood pump for hemofiltration that suppresses blood cell clogging. It will be possible to overcome the poor hemocompatibility that is a problem of centrifugal blood pumps by using these values for hemocompatibility design, and develop a compact and durable low-flow centrifugal blood pump for hemofiltration in acute use. In addition, low-flow blood pumps rated under 1 L/min are required for ECMO for infants; however, there is also a problem of hemocompatibility. 6 It is expected that the index of hemocompatibility to suppress platelet aggregation gained from our results can be used in blood pump design for ECMO for infants.
Limitations of the study
In this study, porcine blood collected at a slaughterhouse was refluxed for only 60 min to assess platelet aggregation, clogging on the micromesh filter, and hemolysis. A longer experimental time should be considered as the next step. In addition, the result is for a micromesh filter of 150 μm. Different micromesh filter sizes and materials are expected to have different platelet adhesion performance and may show different clogging results. Using blood from different species is also considered as the next step.
In this study, the results were obtained based on the experimental results of each pump with two sizes of impeller inlet diameter. Investigation of platelet clogging with more impeller configurations may yield better design specifications for a low-flow centrifugal blood pump.
Conclusion
We investigated the acceptable hemocompatibility that could be applied to a low-flow centrifugal blood pump with less clogging on a micromesh filter using two types of blood pump having different impeller inlet sizes. The platelet clogging on a micromesh filter occurred when the average NL-PATI was greater than 0.28 and the average NIH (g/20 min) was greater than 0.01. In contrast, the platelet clogging on a micromesh was suppressed when the average NL-PATI was less than 0.17 and the average NIH (g/20 min) was less than 0.003. These values might be used as acceptable hemocompatibility measures for low-flow centrifugal blood pumps with suppressed platelet clogging for hemofiltration pumps instead of a roller blood pump.
Footnotes
Acknowledgements
We would like to thank the Ibaraki Prefecture Central Meat Center for providing porcine blood.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Grants-in-Aid for Scientific Research from the Japan Society for the Promotion of Science, grant numbers 18K12130 and 18J40257.