
Abstract
Commercial sexual exploitation of children (CSEC) is a social problem in the United States that has recently received growing attention from policy makers, advocates, and researchers. Despite increasing awareness of this issue, information on the prevalence, demographic profile, and psychosocial needs of victims of CSEC is scarce. To better understand the scope of CSEC and to examine the feasibility of screening for CSEC in Child Advocacy Centers (CACs), a pilot study was initiated through Arkansas Building Effective Services for Trauma (ARBEST) to identify youth who may be at risk for commercial sexual exploitation. Data for this pilot study were collected from all of the state’s CACs (n = 14) over a 6-month period. Family advocates completed a screening questionnaire adapted from Greenbaum, Dodd, and McCracken with 918 youth aged 12 to 18 years old treated at CACs. Almost 20% of youth were identified as being at high risk for experiencing CSEC. Furthermore, youth classified as high-risk for commercial sexual exploitation reported significantly more avoidance symptoms on the UCLA (University of California at Los Angeles) PTSD (Posttraumatic Stress Disorder) Reaction Index than youth classified as low-risk. The results suggest that a significant portion of youth treated at CACs in Arkansas are at high risk for experiencing commercial sexual exploitation, which may be associated with a particular pattern of trauma symptoms. These findings also lend support for the feasibility and utilization of a screening questionnaire as part of routine care in CACs to potentially identify youth at risk for CSEC.
Commercial sexual exploitation of children (CSEC) is a significant problem in the United States (Saewyc, MacKay, Anderson, & Drozda, 2008), which involves the sexual abuse and exploitation of children for monetary or material gain (Albanese, 2007; Institute of Medicine [IOM] & National Research Council [NRC], 2013). CSEC can manifest in numerous forms, including forcing, coercing, or manipulating children to engage in activities such as prostitution or pornography (Estes & Weiner, 2002; Mitchell, Jones, Finkelhor, & Wolak, 2011). Youth who are exposed to CSEC often experience considerable psychological trauma that may significantly influence long-term functioning (Smith, Vardaman, & Snow, 2009). Furthermore, these youth are frequently involved with multiple systems that are difficult to navigate (e.g., juvenile justice, child welfare, medical teams, mental health, etc.). Child Advocacy Centers (CACs) have the valuable opportunity to identify and intervene with youth affected by CSEC by helping them navigate these systems and connect them with appropriate services.
Prevalence and Characteristics of CSEC
The “low visibility” and variation in definitions of CSEC make it difficult to determine the prevalence of CSEC in the United States (Salisbury, Dabney, & Russell, 2015). Moreover, estimates vary greatly due to the manner in which data are collected, as well as the identification of risk versus known exploitation. The most commonly cited estimate of CSEC indicates that as many as 244,000 children are at risk of CSEC each year (Estes & Weiner, 2002). However, a more recent study based on arrest rates for juvenile prostitution estimates approximately 1,450 youth experience CSEC annually (Mitchell, Finkelhor, & Wolak, 2010). Despite the lack of clarity around the prevalence of CSEC victimization, existing research has established its presence in the United States, and interest in examining CSEC more closely has increased over the recent years (Andretta, Woodland, Watkins, & Barnes, 2016).
Variations in risk may also be related to a youth’s exposure to CSEC. Qualitative research has identified three main pathways to sexual exploitation: (a) runaway children who are solicited or recruited for CSEC, (b) children who are kidnapped or lured into CSEC, and (c) children living at home who are exploited by family members or friends (Ashley, 2008; Priebe & Suhr, 2005; Smith et al., 2009). A significant portion of exploitation occurs when children are living at home (Estes & Weiner, 2002; Mitchell et al., 2010), with one study finding that 20% of all CSEC victims were living at home when they were first exploited (Saewyc et al., 2008). Furthermore, it is more common for children to be sexually exploited for monetary gain by family members and friends than by strangers (Albanese, 2007).
Risk Factors for CSEC
Efforts to screen and assess CSEC victims have centered on the identification of risk factors. A common risk factor among children who have been exploited is family dysfunction, including insecure attachments with primary caregivers (Estes & Weiner, 2002), family disruption (Clawson, Dutch, Solomon, & Grace, 2009), exposure to parental substance abuse and violence (Smith et al., 2009), family poverty (Logan, Walker, & Hunt, 2009), and family or community history of exploitation (Ashley, 2008). Often, the cycle of exploitation begins when an adult family member or friend sexually abuses a minor child in his or her care, and then escalates to photographing/videotaping the sexual abuse (Reid, 2011).
Exposure to early abuse is also a significant risk factor for CSEC. Researchers have found that many victims of CSEC experienced physical abuse (Ashley, 2008), psychological abuse (Office of Juvenile Justice and Delinquency Prevention, 2002), neglect (Boxill & Richardson, 2007), or sexual abuse (Clawson et al., 2009). In particular, childhood sexual abuse has consistently been identified as a robust risk factor for involvement in CSEC, with the prevalence of sexual abuse among female adolescents involved in CSEC ranging from 26% to 73.3% (Cole, Sprang, Lee, & Cohen, 2016; Tyler, Hoyt, & Whitbeck, 2000). A variety of theories explain the links between dysfunctional homes, child abuse, and increased risk for CSEC. One theory holds that children experiencing abuse at home may be more likely to engage in high-risk behaviors, thereby increasing the possibility they may come into contact with traffickers and other offenders (Walker-Rodriguez & Hill, 2011). Another theory posits that early histories of abuse increase the likelihood of children running away from home (Adelson, 2008; Brannigan & Van Brunschot, 1997), which again exposes them to potential exploitation or resorting to sexual activity in exchange for money to survive on the streets (Finkelhor & Ormrod, 2004). Children who run away from home and children who are homeless are disproportionately more likely to be sexually exploited, with estimates ranging from at least one in five to as many as one in three homeless runaway children trading sex for money, drugs, or shelter (Halcón & Lifson, 2004; Saewyc et al., 2008; Wilson & Widom, 2010). Another study of homeless runaway children found that 17.9% of girls and 14.6% of boys had recently been involved in sex work (Gwadz et al., 2009).
Children in contact with certain state agencies are also at increased risk for CSEC, particularly children in the child welfare or juvenile justice systems. In a collaborative research study with 10 U.S. Department of Justice-funded trafficking task forces across the United States, Smith and colleagues (2009) found that many victims of CSEC had histories of Child Protective Services involvement. Relatedly, the National Center for Missing & Exploited Children (2017) reported that 86% of sexually exploited children were in the care of social services or foster care when they were reported missing. Moreover, victims of CSEC are more likely to be involved with the juvenile justice system when compared with nonvictims (Gragg, Petta, Bernstein, Eisen, & Quinn, 2007; Reid, 2010). In a study of CSEC victims in Massachusetts, Piening and Cross (2012) found that 10% of the CSEC victims had been arrested for prostitution, and over four in 10 had confirmed or suspected involvement in out-of-state trafficking. The authors noted that these children have historically been viewed as delinquents for the juvenile justice system to deal with, explaining that many victims of CSEC are processed within the juvenile justice system and not referred to agencies and services such as CACs. Fortunately, there is increasing recognition that these youth are manipulated by exploitive adults, and therefore victims of trauma (Reid, 2010). This changing paradigm has been associated with a recent push to better integrate juvenile justice and CAC services, though substantial work remains to be done.
Substance use is also associated with increased risk for CSEC. Certain studies have found that children reported using drugs prior to sexual exploitation (Erickson, Butters, McGillicuddy, & Hallgren, 2000; Tyler & Johnson, 2006), while other studies found that children reported starting to use substances as a consequence and coping strategy following sexual exploitation (Cusick, 2002; Hwang & Bedford, 2004). Brawn and Roe-Sepowitz (2008) determined that the longer youth are involved in CSEC, the more likely they are to abuse substances. Additional factors associated with CSEC include having an older boyfriend, having tattoos or brands, and possessing expensive materials, such as clothes or electronic devices (Salisbury et al., 2015).
Assessing Victims of Sexual Exploitation
Given their unique role in interviewing, triaging and providing multiple services within a single setting, CACs can play a critical role in assessing sexual exploitation and delivering victim-centered care (Edinburgh, Pape-Blabolil, Harpin, & Saewyc, 2015). These services can include forensic interviews, medical care, victim advocacy, mental health services, and connections to resources in local communities. Despite contact with a population at high risk for CSEC, CACs have faced barriers to providing services to these youth (National Children’s Alliance [NCA], 2017). Specifically, the NCA noted that a common barrier reported by CACs is the identification of youth involved in CSEC, with 31% of CACs indicating that they were unaware of how many CSEC cases were served at their center in 2016. The NCA (2017) provides a list of tools developed to identify trafficked youth. However, the majority of these tools are structured interviews that are lengthy and include questions that go beyond sexual exploitation. Given that youth already receive an in-depth forensic interview at the CAC, it is possible that youth may be hesitant to provide further information to advocates in a structured interview format. It is also possible that family advocates may lack sufficient time and training necessary to complete the more in-depth questionnaires.
Greenbaum, Dodd, and McCracken (2018) developed a brief screening tool consisting of six questions that were successful at identifying victims of CSEC among a broader sample of youth who experienced sexual abuse. They implemented the screening tool in three metropolitan pediatric emergency departments and one child protection clinic. The current pilot study sought to examine the feasibility of administering this screening tool in CACs statewide to more broadly estimate the prevalence of youth at risk for CSEC who present to these agencies. This study also sought to better understand associations between risk for CSEC and trauma symptoms, as well as mental health referrals. This study was conducted by the Arkansas Building Effective Services for Trauma (ARBEST) program, which was established in 2009 as a statewide initiative to enhance evidence-based care for children who have experienced trauma.
Method
Participants
Participants were 1,052 youth who received services at 14 CACs located throughout the state of Arkansas. Table 1 shows specific demographic information and comparisons between groups. In the 6-month time period in which data were collected, CAC family advocates completed the screening questionnaire for 918 (87%) of the eligible 1,052 youth. There were no significant differences between the screened and nonscreened groups with regard to gender, race, or ethnicity. However, there was a significant difference in age, as youth who were screened were slightly older compared with youth who were not screened.
Demographic Information and Group Comparisons.
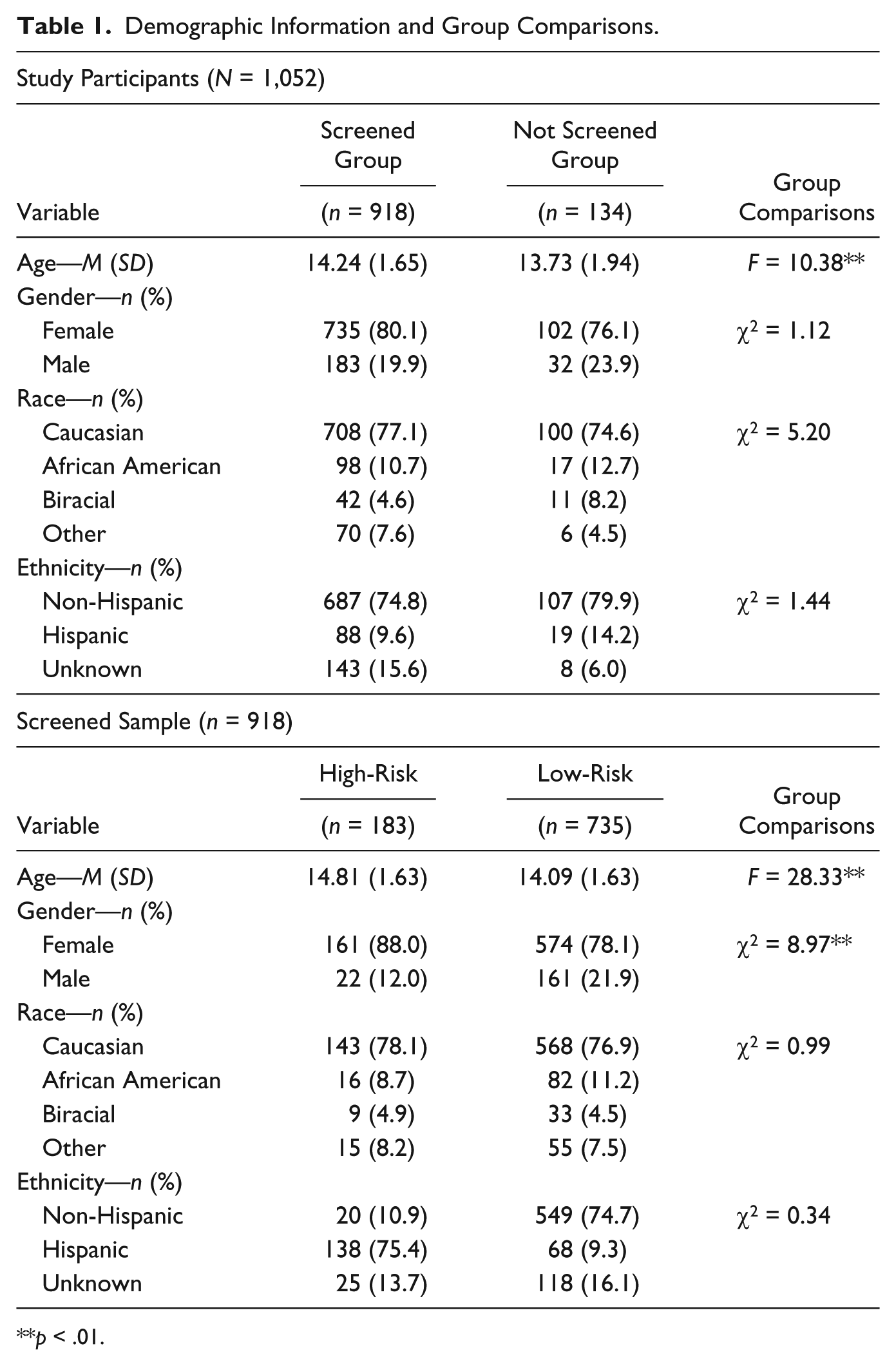
p < .01.
Procedure
All CAC directors within the state of Arkansas (n = 14) were invited and agreed to participate in the study. Directors completed a request for proposal and received funding through ARBEST to complete the study requirements. Participating CACs were instructed to conduct screenings for CSEC with a minimum of 80% of all youth ages 12 through 18 years old who presented to the CAC for services between November 1, 2016, and April 30, 2017. Screenings were completed in 64 (85.3%) of Arkansas’s 75 counties, and youth were identified as High-Risk in 34 (53.1%) of the 64 counties.
Screening for CSEC was conducted with the Screening Questionnaire for Commercial Sexual Exploitation of Youth in CACs. Following the family advocate’s initial visit with the youth at the CAC, the family advocate independently completed the questionnaire based on information obtained from this visit. The family advocate then entered the questionnaire items into the ARBEST online portal. At this time, family advocates provided additional information on the youth, including demographics, trauma history based upon the youth’s referral to the CAC, and referral status for additional mental health services. Finally, if a youth received services through a mental health professional affiliated with a CAC, that professional also provided data through the ARBEST online portal consisting of responses to the UCLA (University of California at Los Angeles) PTSD (Posttraumatic Stress Disorder) Reaction Index for Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV; American Psychiatric Association, 1994). Data were entered as part of the treatment process of 120 youth (13.1% of the original 918). There were no significant associations between gender and completion of the UCLA, χ2(1, n = 918) = 2.88, p = .09, or age and completion of the UCLA, F(1, n = 917) = 1.82, p = .18. However, there was a significant association between race and completion of the UCLA, with significantly more African American youth, χ2(3, n = 918) = 12.75, p < .01, and Hispanic youth completing the UCLA, χ2(1, n = 775) = 7.14, p < .01.
Measures
Screening Questionnaire for the Commercial Sexual Exploitation of Youth in CACs
The development of the Screening Questionnaire for the Commercial Sexual Exploitation of Youth in CACs followed a series of systematic steps. The first step consisted of an in-depth review of the relevant literature and identification of the pertinent risk factors. Next, the ARBEST team, which is an interdisciplinary group of clinical psychologists, social workers, and educational providers reviewed the items and refined the content and format of the questionnaire. Finally, the questionnaire was presented to CAC directors and family advocates in CACs, and adjustments were made based on feedback.
The final version of the questionnaire consisted of two parts. Part 1 was comprised of seven Yes or No items. Items 1 through 6 were drawn from a measure developed by Greenbaum and colleagues (2018) to identify youth at risk for CSEC. This research with youth who experienced sexual abuse revealed that if two or more of these six questions were answered “Yes,” then the chances of the youth having experienced CSEC was 22 times higher than the sample of sexually abused youth without a history of CSEC. Additional analyses of these six items found that a cutoff score of two positive answers had a sensitivity of 92%, specificity of 73%, positive predictive value of 51%, and negative predictive value of 97% (Greenbaum et al., 2018). In an effort to obtain information related to actual involvement in CSEC, the seventh item on the questionnaire was added for this pilot study, which explicitly asked the CAC family advocates completing the screening questionnaire to draw on their general knowledge of the case and determine whether they had knowledge of, or suspicion that, the youth experienced CSEC.
The results of Part 1 (Items 1-7) determined whether Part 2 of the questionnaire was completed by the advocate. Youth were classified as High-Risk if (a) two or more items were answered positively on Items 1 through 6 or (b) Item 7 was answered positively. All other youth were classified as Low-Risk. For youth classified as High-Risk, family advocates were instructed to complete Part 2 of the questionnaire. Part 2 consisted of 10 items aimed at gathering additional information about the High-Risk youth’s experiences and additional risk factors. These items were pulled from the broader literature on CSEC risk factors (IOM & NRC, 2013; Salisbury et al., 2015). Refer to Table 2 for a list of questionnaire items. The additional items were not completed for the Low-Risk group because the main purpose of the questionnaire was to serve as a brief screener, and if the youth screened as Low-Risk in Part 1, further information was deemed not necessary at this time.
Screening Questionnaire for the Commercial Sexual Exploitation of Youth in CACs.
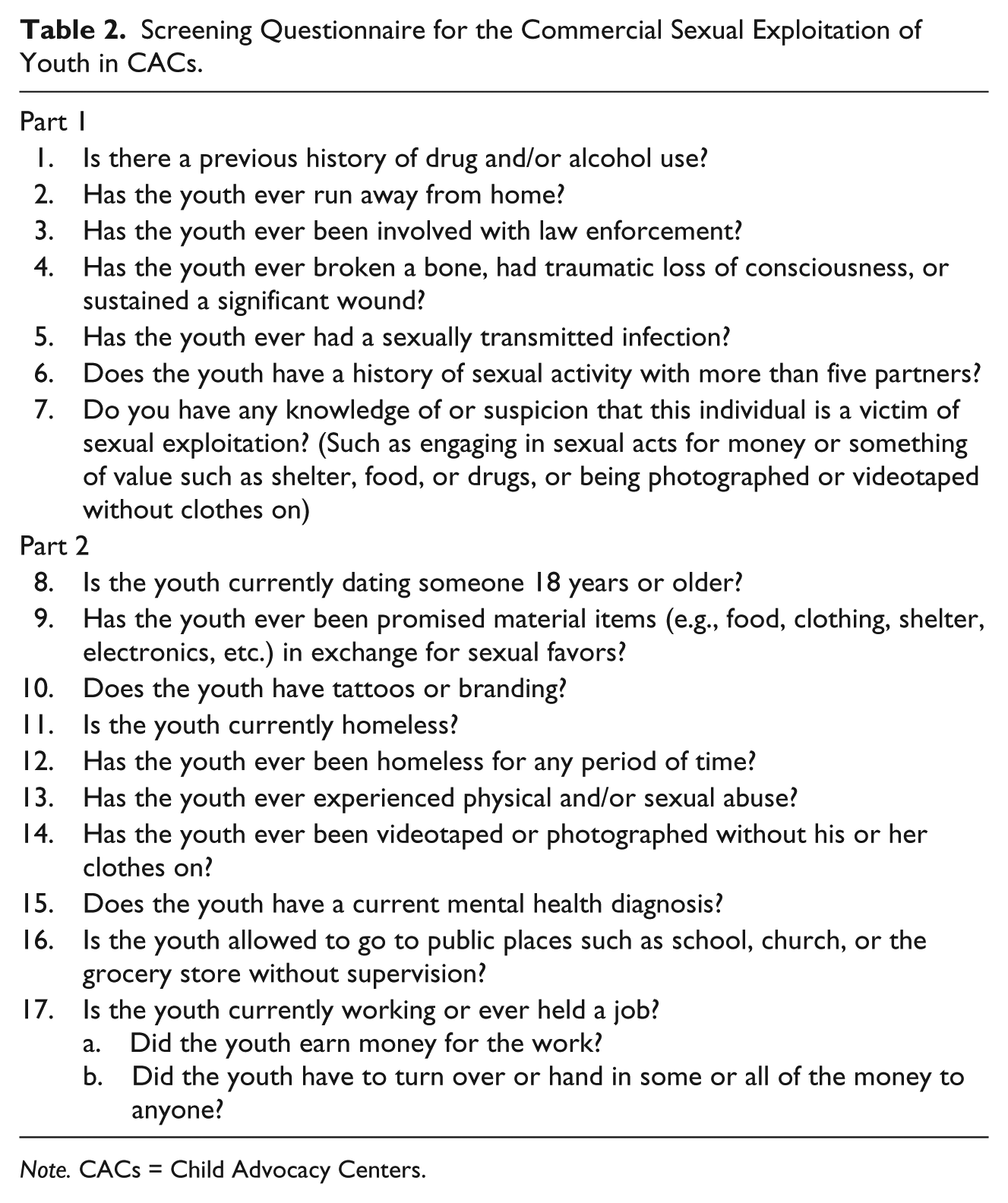
Note. CACs = Child Advocacy Centers.
UCLA PTSD Reaction Index for DSM-IV
The UCLA PTSD Reaction Index is a standardized self-report measure used to assess for traumatic events and related trauma symptoms in youth 7 to 17 years old (Pynoos, Rodriguez, Steinberg, Stuber, & Frederick, 1998; Steinberg et al., 2013). The UCLA consists of 12 Yes or No questions regarding specific traumatic events that a youth may have experienced. A 13th item asks whether the youth has experienced any other event that was scary or bothersome that was not noted in the first 12 items. Next, the youth is required to identify which event of those endorsed is the most bothersome to him or her, and the remaining questions refer to this specific event. The next 13 questions consist of Yes or No items that represent how the youth felt during, or right after, the event took place. Finally, the remaining 21 items are rated on a Likert-type scale (0 = none, never to 4 = most, almost every day) and assess for trauma symptoms (i.e., reexperiencing, avoidance, and arousal) that the youth experienced within the past month. A trauma symptom was judged to be present if it was rated as a 3 (much, 2-3 times a week) or 4 (most, almost every day). Three cluster scores are obtained for the domains of reexperiencing, avoidance, and arousal, as well as a total PTSD severity score (38 and above = severe symptoms, 33 to 37 = moderate symptoms, 27 to 32 = mild symptoms, and 26 or below = normative symptoms).
Results
Descriptive Data on the CSEC Screening Questionnaire for the Commercial Sexual Exploitation of Youth in CACs
For youth who were screened, 183 (19.9%) were classified as High-Risk for CSEC, while 735 (80.1%) were classified as Low-Risk for CSEC. Refer to Table 1 for demographic information and group comparisons. There were significantly more females than males in both groups and youth classified as High-Risk tended to be significantly older than youth classified as Low-Risk. There were no significant differences between the High-Risk group and the Low-Risk group regarding race or ethnicity.
Part 1: Classification of High-Risk and Low-Risk
Descriptive data regarding the classification of youth into the High-Risk group based on the first seven items on the questionnaire are presented in Figure 1. The majority of youth in the High-Risk group had a prior history with drug and/or alcohol use, ran away from home, and/or had previously been involved with law enforcement. The High-Risk group had an average of 2.20 (SD = 1.26) risk factors, and the Low-Risk group had an average of 0.56 (SD = 0.36) risk factors. As expected, there was a significant difference in the number of risk factors identified between the High-Risk and Low-Risk groups, F(1, 917) = 1,471.97, p < .01. Furthermore, family advocates endorsed Yes for Item 7 (suspected the youth was a victim of CSEC) for 65 youth, which comprised 35.5% of the 183 youth classified as High-Risk, and 7.1% of all 918 youth screened. Of note, 23 of the 65 youth were classified as High-Risk based solely on the family advocates’ response to Item 7 (i.e., less than two items were endorsed as Yes for Items 1-6 but Item 7 was endorsed as Yes). These youth comprised 12.6% of the High-Risk youth and 2.5% of all 918 youth screened.
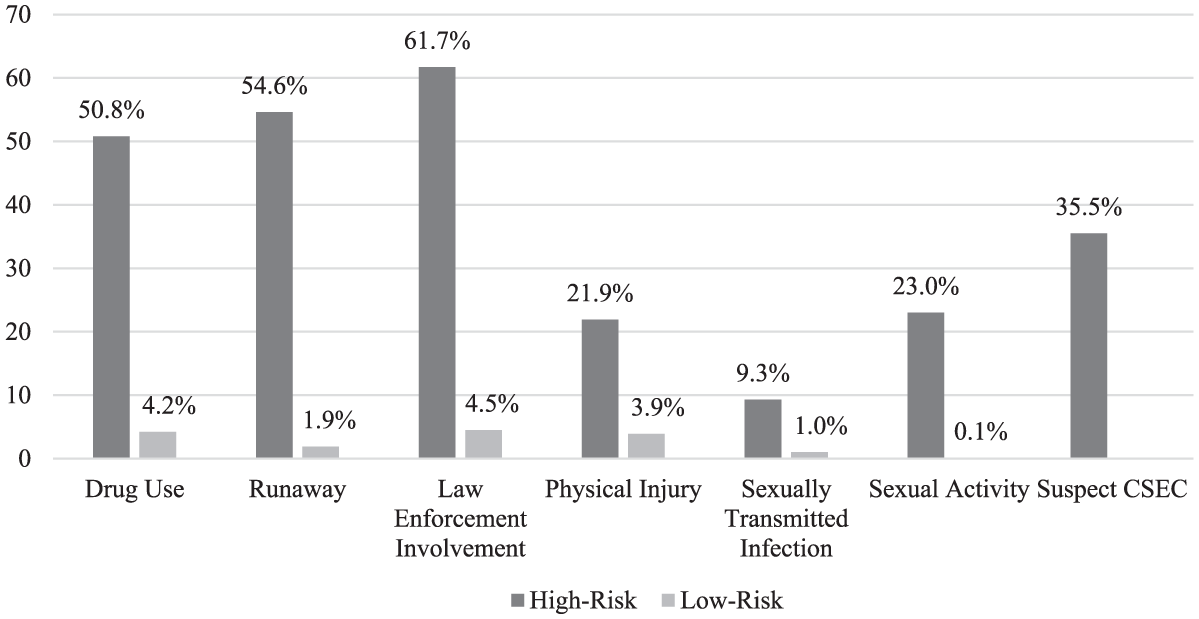
Screening Questionnaire for Items 1 to 7.
Part 2: Identification of additional risk factors
The remaining items of the screening questionnaire (Items 8-17b) were developed to identify other possible risk factors associated with CSEC. These items were completed by the family advocate if the youth was identified as High-Risk in Part 1. Figure 2 reflects the descriptive data regarding Items 8-17b. The majority of youth were identified as experiencing physical/sexual abuse and having a mental health diagnosis. The average number of risk factors endorsed for the total questionnaire (1-6, 8-17b) was 5.08 (SD = 1.50), and the average number of risk factors endorsed for the additional questions only (8-17b) was 2.92 (SD = 1.20).
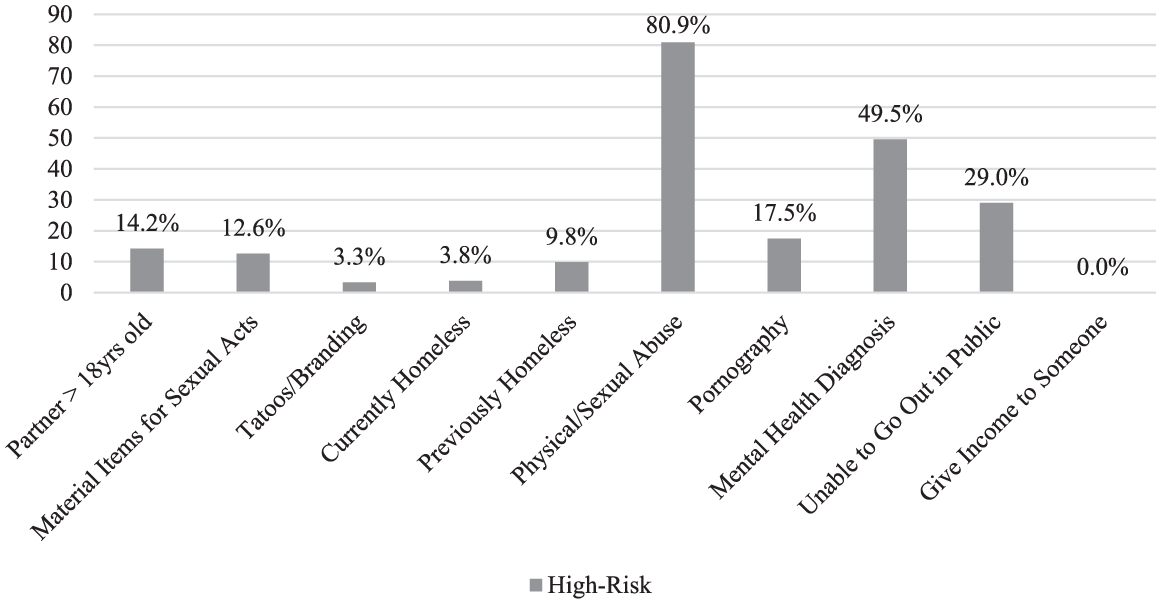
Screening Questionnaire for Items 8 to 17b.
Trauma and CSEC
Trauma exposure
Descriptive frequency analyses were conducted to better understand the population with regard to trauma-related variables (refer to Table 3 for a full summary of trauma-related descriptive data). Of note, there was a significant difference between the number of different types of trauma experienced by youth (as documented by family advocates) in the High-Risk group compared with youth in the Low-Risk group. In addition, there were significant associations between risk level and trauma experience with regard to drug endangerment and being removed from home, with youth in the High-Risk group experiencing these traumas more than youth in the Low-Risk group. There was not a significant association between risk level and other trauma experiences. Furthermore, there was a significant association between risk level and offender relationship, with the offender more likely being unknown to the youth in the Low-Risk group versus the High-Risk group. Moreover, there was a significant association between risk level and offender age, with the offender for both groups more likely being 18 years or older. Finally, there was a significant association between risk level and problematic sexual behaviors, with youth in the High-Risk group displaying more problematic sexual behaviors than youth in the Low-Risk group.
Trauma-Related Descriptive Statistics (n = 918).
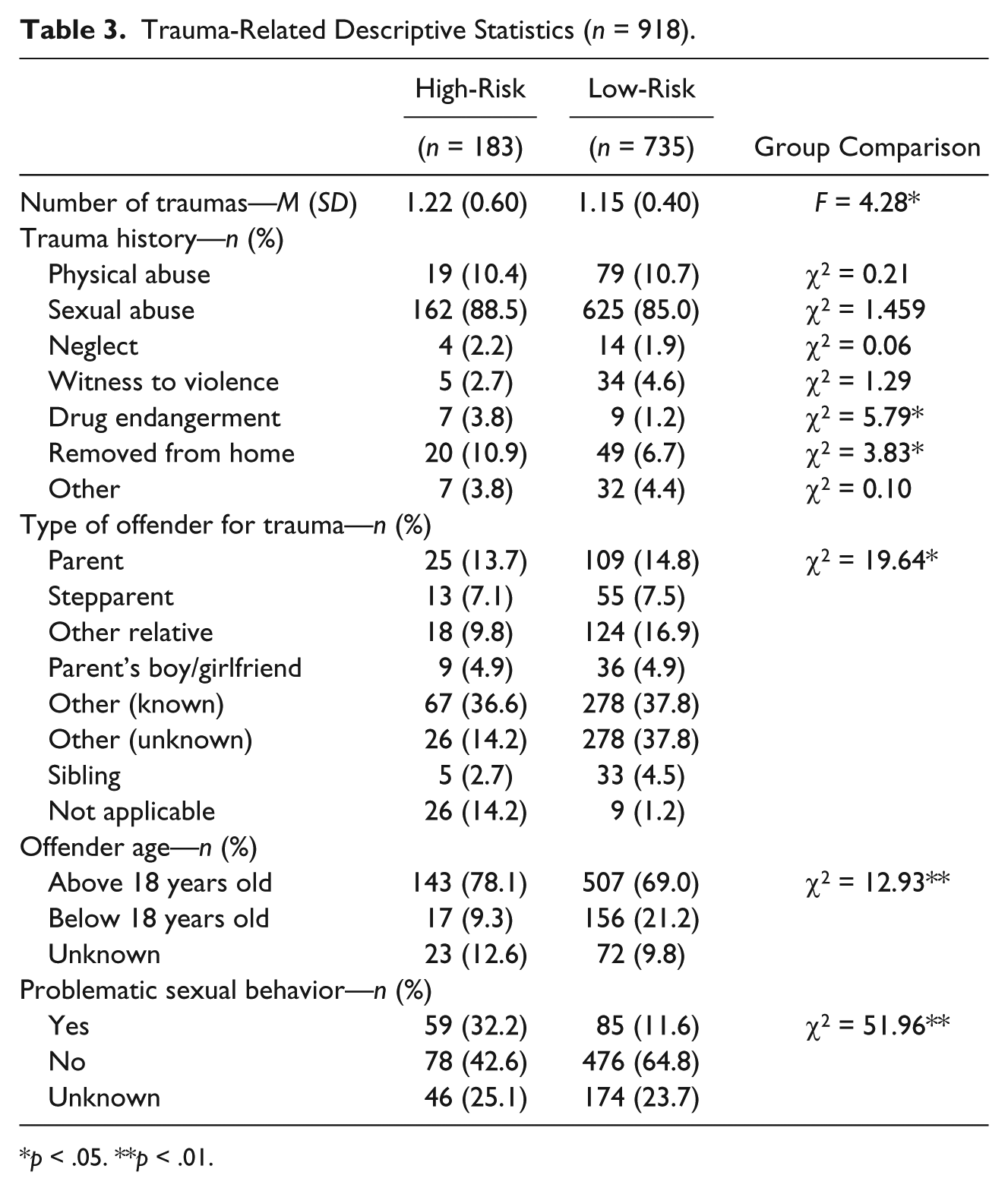
p < .05. **p < .01.
Trauma-related services
Of the sample that had screening measures completed, a total of 368 (40.1%) youth were referred for mental health services by family advocates, 322 (35.1%) were already in counseling, and 196 (21.4%) were not referred. Data regarding referrals were not available for 32 (3.5%) of the youth. There were significant associations between risk level and referral patterns, χ2(2, n = 886) = 18.48, p < .01, with more youth in the High-Risk group (46.9%) already in counseling, compared with youth in the Low-Risk group (33.7%). While a similar percentage of youth in both groups received referrals for counseling (High-Risk group: 41.8%, Low-Risk group: 41.5%), a significantly higher number of youth in the Low-Risk group (24.8%) were not referred for counseling, compared with the High-Risk group (11.3%).
Regarding referral services, data were available for 370 (40.3%) of the youth who were screened. Of these youth, 185 (50.0%) were referred to a CAC mental health clinician, 140 (37.8%) were referred to a community mental health center, and 45 (12.2%) were referred to other community services. There was a significant association between risk level and referral services, χ2(2, n = 370) = 7.84, p = .02, with more High-Risk youth referred to CAC mental health clinicians (High-Risk group: 56.0%, Low-Risk group: 48.5%) and other community services (High-Risk group: 18.7%, Low-Risk group: 10.5%), and more Low-Risk youth referred to a community mental health center (High-Risk group: 25.3%, Low-Risk group: 41.0%).
Trauma-related symptoms
Data regarding trauma symptoms, as assessed with the UCLA PTSD Reaction Index for DSM-IV, were collected from 120 youth referred for services to CAC mental health professionals. Differences in the number of types of traumas experienced, the number of trauma symptoms reported, and severity of these symptoms between the High-Risk group and the Low-Risk group were examined using analysis of variance (see Table 4). There was a marginally significant difference between the High-Risk and Low-Risk groups with regard to the number of different types of traumas experienced, with the High-Risk youth experiencing more types of trauma than the Low-Risk group. Examination of the PTSD symptom clusters showed that youth in the High-Risk group reported significantly more symptoms of avoidance, compared with the Low-Risk group. Severity scores on the avoidance cluster were also significantly higher for the High-Risk group compared with the Low-Risk group. For the arousal cluster, youth in the High-Risk group reported more arousal symptoms than youth in the Low-Risk group at a level that approached significance. Finally, the youth in the High-Risk group reported more overall PTSD symptoms than youth in the Low-Risk group at a level that approached significance.
Trauma Exposure and Symptoms as Measured by UCLA PTSD Index for DSM-IV (N = 120).
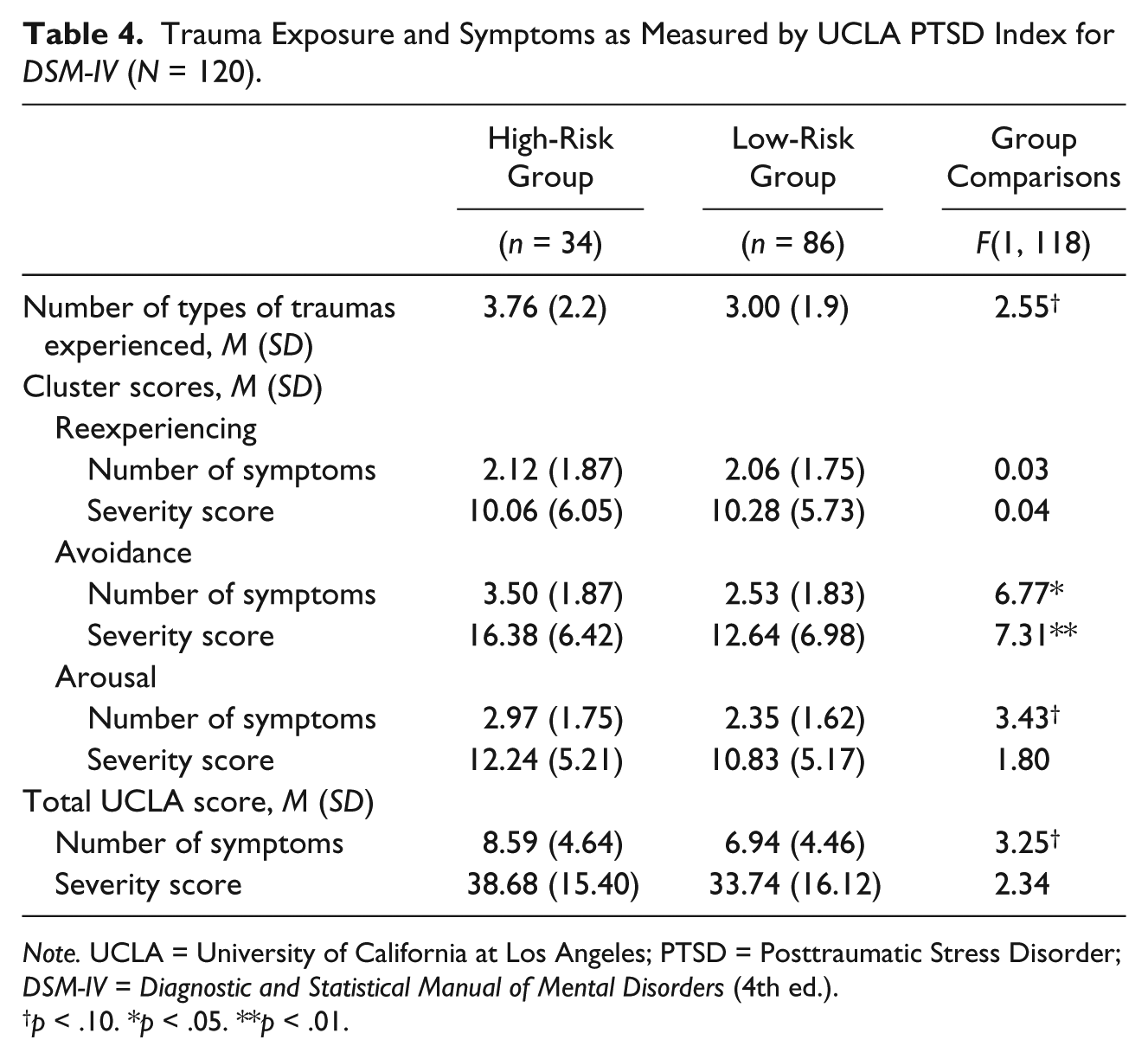
Note. UCLA = University of California at Los Angeles; PTSD = Posttraumatic Stress Disorder; DSM-IV = Diagnostic and Statistical Manual of Mental Disorders (4th ed.).
p < .10. *p < .05. **p < .01.
Discussion
CSEC is a complex social issue that must be addressed through the multiple systems that these youth encounter, including legal systems (i.e., juvenile justice, court appointed special advocates, attorneys ad litem, etc.), child welfare, mental health services, and medical providers. One critical step in addressing this issue is the identification of youth at risk of CSEC who encounter these systems of care. This study sought to investigate the feasibility of administering a brief screening measure for CSEC in CACs, as well as to explore the prevalence of risk factors for CSEC and associated trauma symptoms in this population.
Indeed this study demonstrated the feasibility of implementing a brief screening instrument for CSEC in CACs within the state of Arkansas. The screening instrument was completed with 918 (87.3%) youth out of a possible 1,052, showing that family advocates in CACs were willing and able to collect and enter these data for the majority of clients who presented to their center in a 6-month time period. Of the 918 youth screened for CSEC, a total of 183 (19.9%) were classified as being at high risk for CSEC. This rate is similar to that of the original sample (23.1%) used to develop the CSEC screening measure (Greenbaum et al., 2018).
Overall, the risk factors found to be associated with High-Risk status are consistent with existing literature on characteristics of CSEC victims. For example, results indicated that youth in the High-Risk group were more likely to be older adolescent females with a history of running away from home or being removed from their home. This further supports previous research identifying the solicitation of runaway and homeless females as a potential pathway to CSEC (Priebe & Suhr, 2005; Smith et al., 2009). Furthermore, youth in the High-Risk group were more likely to be involved with law enforcement. This is not surprising given that delinquent behaviors such as running away and substance use increase the likelihood of involvement in multiple systems, including juvenile justice (Gragg et al., 2007; Reid, 2010).
Results also showed that a majority of youth in the High-Risk group had experienced physical and/or sexual abuse, and that these youth were significantly more likely than youth in the Low-Risk group to have experienced more types of traumatic events. Furthermore, youth classified as High-Risk reported significantly more avoidance symptoms on the UCLA PTSD Reaction Index than youth classified as Low-Risk for CSEC. Symptoms of avoidance may be adaptive for runaway youth who resort to exploitation to survive (Finkelhor & Ormrod, 2004). In addition, elevated avoidance symptoms have been associated with alcohol use disorders (Dworkin, Wanklyn, Stasiewicz, & Coffey, 2018), which are common among CSEC youth. It is possible that the risk factors associated with CSEC in combination with trauma exposure, both before and during exploitation, contribute to observed PTSD symptoms. Indeed, one study highlighted that approximately 80% of sexually exploited adolescent and adult women developed PTSD symptoms, as well as anxiety and depression (Hossain, Zimmerman, Abas, Light, & Watts, 2010). Similarly, the current study revealed the majority of youth in the High-Risk group were noted as having a current mental health diagnosis and endorsed clinically severe symptoms of PTSD. These findings are consistent with a significant body of research suggesting that youth with more trauma exposure, specifically sexual trauma, are at greater risk for developing PTSD (e.g., Salazar, Keller, Gowen, & Courtney, 2015).
Fortunately, researchers have demonstrated that youth with greater trauma exposure are more likely to engage in mental health services (McChesney, Adamson, & Shevlin, 2015). Consistent with this, the current study revealed that youth in the High-Risk group were more likely to already be in counseling, compared with youth in the Low-Risk group, although there was some variation with regard to race. Caucasians were more likely to be receiving mental health services prior to presenting at the CAC. This may account for the fact that more African American children completed the UCLA PTSD scale in this study, as this was only requested of new clients referred for mental health services. Potential disparities in mental health service access and/or utilization is a critical issue for this population and should be further investigated given that African American youth are less likely to be engaged in mental health services (Thompson, 2005) despite the need for services being recognized (Thompson & May, 2006). Differences among racial and ethnic minority status within the CSEC population are also sparse in the current literature and warrants further investigation. Additional differences were difficult to examine in the current study given that the study consisted mostly of Caucasian youth.
Researchers have noted that mental health professionals face a number of barriers when attempting to provide trauma-informed care specifically for CSEC youth, including building rapport with youth who do not view their experiences as traumatic; addressing problematic behavior such as risky sexual behavior, substance use, and running away; and engaging overwhelmed caregivers (West Coast Children’s Clinic, 2012). In the current study, about one fifth of the total sample was not referred for treatment, including 11.3% of the High-Risk group. Data indicate that children were not referred for a number of reasons, including the parent/caregiver refused counseling (26%); the child was not reporting mental health needs (17%); there was no evidence presented of abuse (25%); and other reasons, such as no caregiver was present at the time of the investigation, the child presented from a different service area from the CAC, or child welfare agreed to handle the referral (32%). Problems coordinating care for these youth continue to be complicated, particularly given the fact that families may not recognize the extent of the problem or may actually be responsible for exploiting the child. As such, there is a need for specialized, trauma-informed services to address the unique clinical presentation of these youth. Ongoing research has highlighted the utility of providing treatment services to CSEC youth who are informed by a complex trauma perspective (Cohen, Mannarino, & Kinnish, 2015), but caregiver engagement must be an integral component of such approaches.
Study Limitations
Screening for CSEC youth is a complex issue, and this study was only able to examine the identification of youth who may be at risk for CSEC, rather than confirmed experience of CSEC. In an effort to obtain information related to actual involvement in CSEC, an item was included on the screening questionnaire to assess the family advocate’s suspicion or knowledge that a youth was involved in CSEC. However, this item did not distinguish the advocate’s suspicion from the advocate’s knowledge regarding CSEC involvement. It would be beneficial to assess both suspicion and direct knowledge (e.g., disclosure, legal records) of engagement in CSEC in future iterations of this questionnaire. Similarly, the family advocates completed the questionnaire based on information gathered during the initial visit with the youth. While this was intended to reduce the likelihood that youth would minimize symptoms, it is important to acknowledge the limitations associated with this type of secondary data collection, including influence of individual advocates and potential for not gathering information relevant to all questionnaire items. In addition, although the CACs were required to screen at least 80% of 12- to 18-year-old clients, it may be that some advocates decided not to screen younger children, either because they did not think they were at high risk for CSEC or for some other unknown bias. Furthermore, data regarding trauma symptoms were only available for a small subgroup (13.1%) of the youth screened for CSEC. It is unknown how many youth were able to link to trauma-informed mental health services, particularly providers who are not affiliated with CACs and therefore do not participate in the online data entry. Finally, participation in this study was voluntary, and CACs were provided with funding through ARBEST to complete the screenings. Therefore, the study likely attracted CAC leaders and family advocates more willing to implement new processes. Universal implementation of a screening system may face more barriers within other agencies.
Future Directions
These results reveal the significant number of youth in Arkansas who are at risk for CSEC. Based on data, it is estimated that in 1 year, there could be as many as 400 youth, or as many as 20% of youth at CACs, who are at high risk for CSEC. However, this may be an underestimate as these numbers do not include other high-risk populations (e.g., child welfare, juvenile justice). The extent to which these groups overlap is deserving of future studies but requires data sharing across multiple stakeholders.
Nonetheless, identification of youth who are at risk or have experienced CSEC is only one step in the larger process of ensuring these youth receive evidence-based trauma-informed services that are integrated across the many systems they encounter. CACs have the valuable opportunity to identify and intervene with youth affected by CSEC and are often able to provide a number of services within one agency. Future research efforts should focus on developing reliable and efficient methods to identify youth at risk for CSEC, which may help in implementing preventive strategies. Trauma-informed mental health services utilized with youth with known trauma histories who also present with risk factors associated with CSEC could incorporate CSEC-specific psychoeducation and safety planning as preventive efforts.
Furthermore, once youth are identified by the brief screening questionnaire as being high risk for CSEC, a logical next step is to implement more extensive, validated measures of trafficking such as those noted by the NCA’s (2017) issue brief. In addition, it will be important to provide consultation and support for CAC mental health professionals working with youth who have experienced CSEC and encourage use of evidence-based, trauma-informed treatments such as Trauma-Focused Cognitive-Behavioral Therapy (Cohen et al., 2015). With the wide implementation of such assessment and treatment strategies, the problems of CSEC can begin to be addressed.
Although CACs are an ideal setting for identification of CSEC, the potential for commercially sexually exploited youth to present to varying levels of care outside of the CAC is inevitable. As such, it is critical that states develop systematic methods of data collection and programs to address the needs of this group beyond what can be found in a CAC. For example, three laws concerning human trafficking were recently passed in Arkansas: (a) Act 209, which expanded the definition of child maltreatment to include human trafficking; (b) Act 765, which established the Human Trafficking Victim Support Fund to support nonprofit, religious, and other third-party organizations that provide services and treatment for victims of human trafficking; and (c) Act 922, which requires all Class A commercial driver license holders to complete an online human trafficking prevention course. In addition, organizations nationwide are beginning to establish prevention guidelines to help address the needs of children who are at high risk (i.e., Georgia Statewide Human Trafficking Task Force). Furthermore, NCA has recently released an online learning portal (www.CSEC-response.org) for CAC staff to improve services for this population. Finally, programs such as ARBEST that are focused on enhancing trauma-informed services can also play a critical role in connecting the varying systems of care to appropriate resources and supporting the implementation of evidence-based methods of assessment and treatment.
Footnotes
Acknowledgements
The authors would like to thank the Child Advocacy Centers of Arkansas for supporting this project. A special thank you also goes to Emily Robbins, LCSW, care manager for ARBEST (Arkansas Building Effective Services for Trauma) and social worker for the UAMS Child Study Center, for her contributions to the study, her continued dedication to provide trauma-informed services to children who are commercially sexually exploited, and her commitment to improving services statewide. Finally, a special thank you goes to Kelly Kinnish, director of Project Intersect in Georgia and leader in the field of addressing commercial sexual exploitation of children (CSEC), who gave invaluable input for the study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Arkansas Building Effective Services for Trauma (ARBEST) is supported through Act 512 of the Regular Session of the State of Arkansas 91st General Assembly in 2017. ARBEST is a program operated by the University of Arkansas for Medical Sciences, College of Medicine, Psychiatric Research Institute.