
Abstract
The objective of this study was to determine the success of the natural crowns of endodontically treated canine teeth in pet dogs, instrumented and obturated using rotary driven non-taper nickel titanium files, through an occlusal access preparation, without the placement of a prosthetic cast metal crown. A search of medical records at a private veterinary dental referral practice was conducted to identify pet dogs having had endodontic treatment of one or more canine teeth over an eleven-year period (2007-2018). Follow up, performed by the same veterinary dental specialist, included a complete oral health assessment under general anesthesia and included intraoral radiography thereby allowing close visual examination of the crown and restoration as well as assessing endodontic success. Time to follow up was between two and nine years after treatment with a mean of 4.5 years. Analysis revealed that 29/29 (100%) of the treated crowns maintained their stability and did not require extraction. 5/29 (17.2%) of the treated teeth had an enamel fracture requiring additional treatment to the crown after the initial treatment; 1/29 (3.4%) had additional abrasion but did not require treatment and 23/29 (79.3%) were found to have sustained no additional damage. This study supports endodontic treatment without the placement of a prosthetic crown in canine teeth in pet dogs when an occlusal access site is used as described in this paper. Further study is required on the increased risk of fracture of the remaining unaltered canine teeth.
Keywords
Introduction
Endodontic therapy is a safe and effective treatment for fractured and/or nonvital teeth of sound periodontal health.1,2 Conventional wisdom states that one must achieve straight-ine access to the apex through a mesial access aperture in order to achieve success.3,4 The conventional recommendation regarding acceptable access for dog canine teeth does not seem to have changed, although instrumentation materials and methods have changed over the past several years. There is not an abundance of published material on the success of endodontic therapy in dogs. There are several references that discuss the superelasticity and shape memory properties of NiTi instruments, and their use in curved canals to produce apical preparation.5–8 Despite this, the recommended access site for dog canine teeth for endodontic treatment remains the same. Although not investigated in this study, one must accept the risk of torsion stress fracture of the NiTi files.
By using an occlusal access site, the authors believe that it simplifies the procedure while shortening procedure time by eliminating the time to access through a second aperture site and then the time to restore it. There are several factors that are known to influence the success of endodontic therapy, one important one of which is the mechanical closure and seal of the restoration to eliminate microleakage. 9 By having one restoration instead of two, it is the supposition of the authors that this may have been a contributing factor to treatment success.
The authors also suppose that a mesial access site just coronal to the alveolar crest creates a structural weakness to the natural crown, thereby increasing the risk of crown fracture through this mesial access site. By utilizing the occlusal access and avoiding the mesial access, the tooth will retain more of its natural strength and resistance to fracture. This would be an excellent subject for an in vitro study comparing load-to-failure in canine teeth with and without mesial access sites similar to the load-to-fracture study, 10 which showed there was no significant difference in the amount of force required for fracture between three different force direction groups. It would be interesting to know whether findings would differ in endodontically treated teeth and between teeth treated through an occlusal versus mesial access aperture (with the same H/D ratio).
The objectives of the current study was to: 1. determine if the crown had suffered any further trauma post-treatment that might have reasonably been avoided by using a mesial straight-line access site and/or the placement of a prosthetic crown, and 2. determine the long-term outcome of the natural crowns of endodontically treated canine teeth in pet dogs, instrumented and obturated through an occlusal access preparation, without the placement of a cast metal crown. To the authors’ knowledge, this approach has not been studied although, there has been one published case report detailing root canal treatment through an occlusal access after crown reduction for a malocclusion. 7
This study defined crown integrity as the ability of the crown to maintain form without significant crown or root fractures requiring extraction. Endodontic treatment in this study was considered successful if the periodontal ligament space around the root was normal at the most recent follow up assessment. Follow up was performed by the same veterinary dental specialist and included a complete oral health assessment under general anesthesia with intraoral radiographs at a subsequent procedure.
Materials and Methods
Endodontic Therapy Procedure
All procedures were performed by the same board-certified veterinary dentist. The technique involved instrumenting and obturating the canal through an occlusal access preparation as previously described. 11 A cast-metal prosthesis was not placed post treatment.
A pre-treatment radiograph was taken (Figure 1A). Access was achieved through the occlusal surface of the canine tooth, either through a fracture site or by removing a portion of the coronal crown to expose the pulp chamber. Crowns that were fractured were shaped to remove jagged edges and to eliminate unsupported enamel. Working length was established using standard tapered stainless-steel filesa,b and the canal was shaped using rotary driven non-tapered NiTi filesc and irrigated with 5% sodium hypochlorited (NaOCl). An apical negative pressure irrigation systeme was used to clean the apex. The NaOCl was rinsed well with sterile salinef and an irrigating solutiong was used as a final rinse and left in place for approximately 5 min before drying with absorbent paper pointsh,i. The canals were sealed with either a polymer epoxy resin sealerj or a silicone-based sealerk and obturated with a single gutta-percha master conel,m or by lateral compaction using two or more gutta-percha conesm. An intermediate layer was not used between the gutta percha/sealer cement and the restorative composite, since eugenol was not a component of the utilized materials. The coronal access point (approximately 4-5 mm) was restored adhering to standard techniques. The dentin was prepared by acid-etching utilizing 32% phosphoric acid geln. A light cured fifth generation adhesive agento,p was placed, followed by the placement of a light cured nano-hybrid resin compositeq. The restoration was smoothed with a 12-fluted trimming and finishing carbide burr. The acid-etchant was utilized and a final layer of the adhesive agent was placed (Figure 1B). Post op radiographs confirmed appropriate apical obturation (Figure 1C). Pain management for all patients included regional nerve block with bupivacaine HCl 0.5%s and post operative administration of a non-steroidal anti-inflammatoryt if not medically contra-indicated.
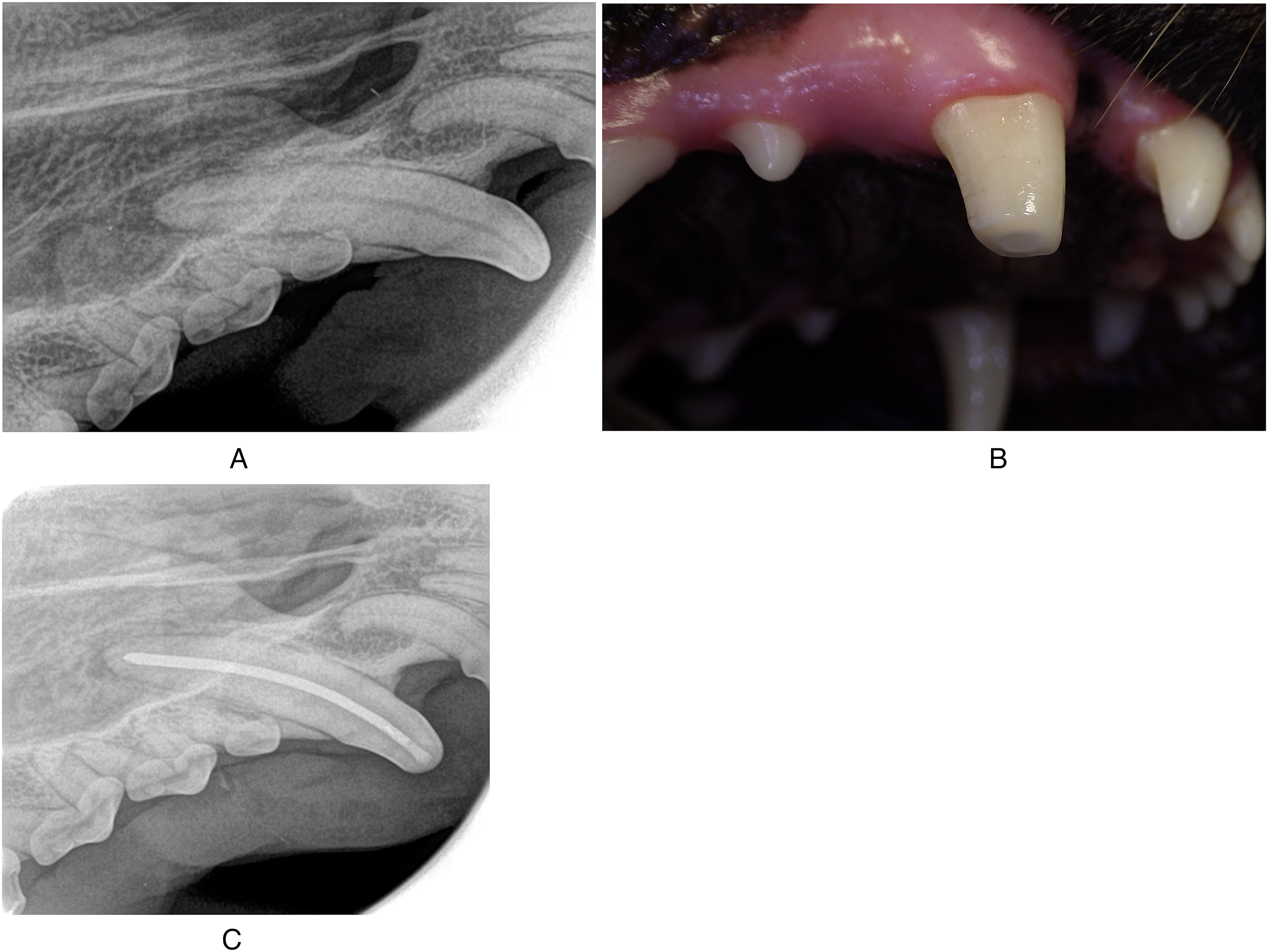
Tooth 104. A). Radiograph of non-vital tooth prior to treatment. B). Photograph of crown post treatment. C). Radiograph of the tooth post treatment.
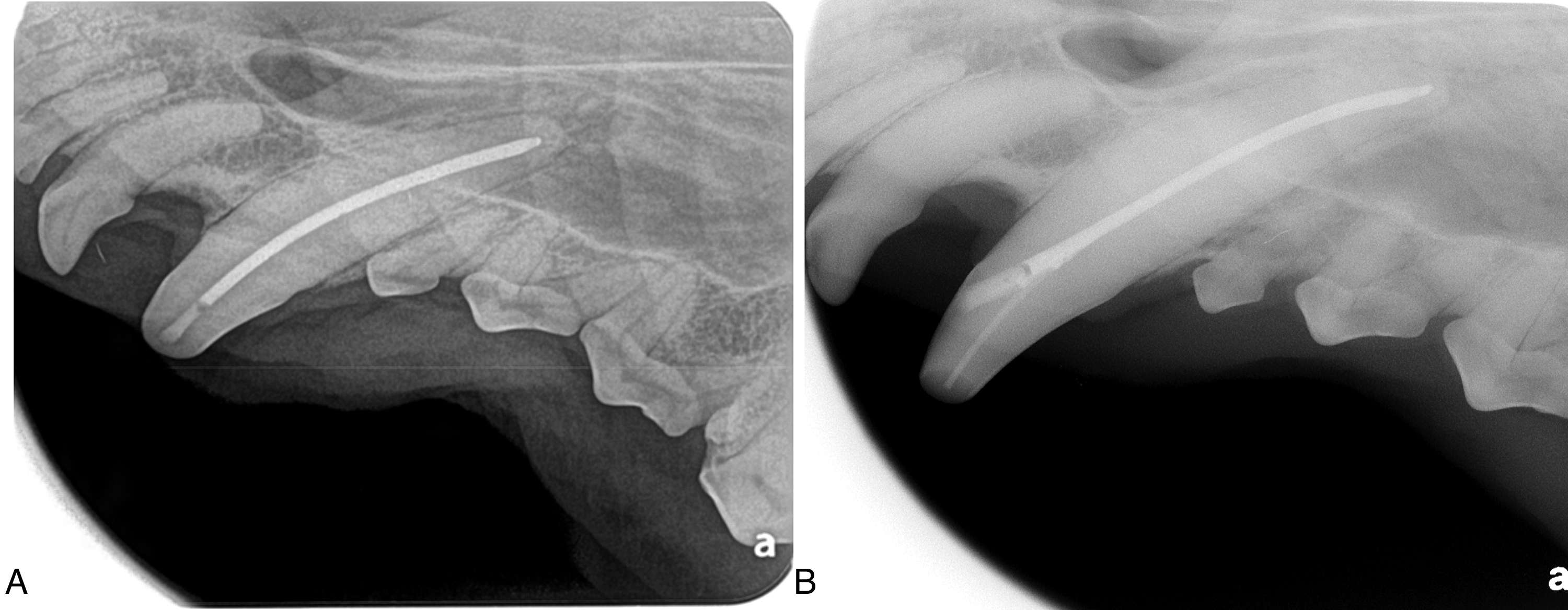
Radiographs showing access sites of endodontically treated teeth (204). A). Access via an occlusal non-straight-line access site. B). Access via a mesial straight-line access site.
Medical Record Review and Case Selection Criteria
A search of medical records at a veterinary dental specialty practice was conducted to identify dogs having had endodontic treatment of one or more canine teeth over an eleven-year period (2007-2018). The tooth had to have follow up at the same facility by the same veterinary dentist at least two years from the date of treatment for inclusion in the study.
There were 297 dogs logged by the specialty clinic between February 2007 and February 2018 having had endodontic treatment of one or more canine teeth during this period (totalling 374 teeth). Thirty-six dogs (50 teeth) were followed up by the veterinary dentist, however seventeen of these dogs (21/50 teeth) were excluded from the study because follow up was less than two years after the initial treatment. Nineteen dogs (29/50 teeth) met the inclusion criteria.
Follow up
Nineteen dogs (29 teeth) that had endodontic therapy performed had a subsequent complete oral health assessment under general anesthesia which included intraoral radiographs. The initial and the subsequent procedures were performed by the same veterinary dentist. The records were reviewed, and the following was recovered:
Diagnosis and treatment of the tooth. Procedure date and duration of time to re-examination. Further coronal damage to the treated tooth if present. Treatment required to repair the damaged crown of the treated tooth. Coronal damage to teeth other than the previously treated tooth. The success of the endodontic treatment. Endodontic treatment in this study was considered successful if the periodontal ligament space around the root was normal (consistent with the space surrounding the other areas of the tooth and symmetrical with the contralateral canine tooth if present) and there was no evidence of external apical root resorption at the most recent follow up assessment. Whether the treated tooth required extraction.
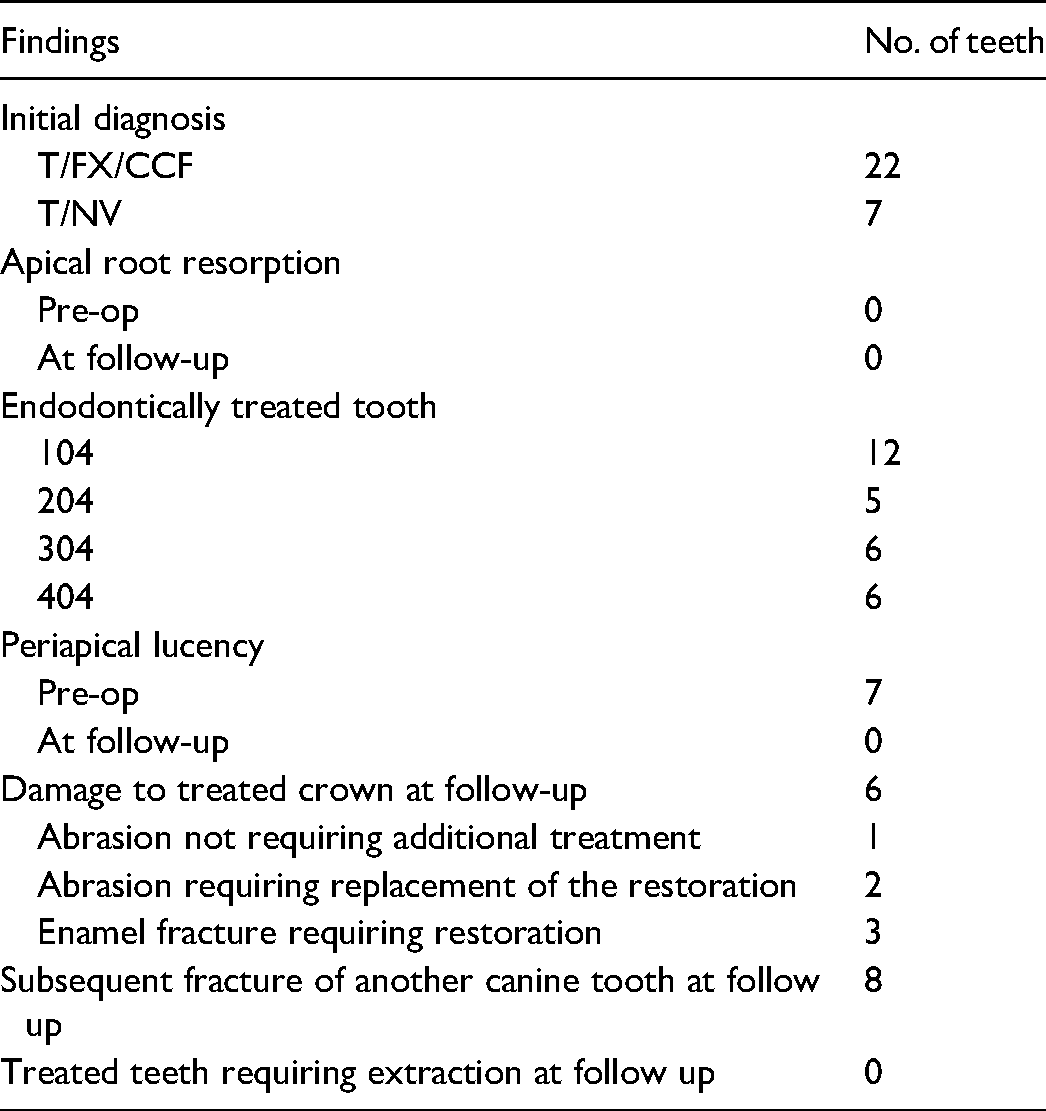
Follow up data included in the study was obtained on 29 canine teeth (19 dogs) that had endodontic therapy for treatment for pulp necrosis (7/29) and complicated crown fractures (22/29). Time to follow up was between two and nine years with a mean of 4.5 years. Of the 29 canine teeth, endodontic therapy was performed on 104 (12/29), 204 (5/29), 304 (6/29) and 404 (6/29). The dogs were of various breeds: Labrador Retriever (3); German Shepherd (2); Border Collie (1); Golden Retriever (2); Great Dane (1); Greyhound (1); Jack Russell Terrier (1); Mini Bull Terrier (1); Standard Poodle (1); Weimaraner (1) and cross breed (5). The age range of the dogs at the time of the initial endodontic treatment was 1.9 to 9 years, and the mean age was 5 years. The weight range was 13.5 kg to 69.5 kg and the mean weight was 30.3 kg. There were 7 female dogs (1 intact) and 12 male dogs (2 intact).
Results of the Follow up Examination
Twenty-nine teeth (19 dogs) that had undergone endodontic treatment were examined under general anesthesia by the veterinary dentist. Full mouth intraoral radiographsu,v were obtained and evaluated at follow up. All hard and soft tissues in the oral cavity were examined, probing depths were measured, and abnormal depths were documented on the dental chart. The crowns were examined and explored for damage and recorded if abnormal. The occlusal restoration was evaluated, and findings were documented. Intraoral radiographs were used to evaluate endodontic treatment and considered successful if the periodontal ligament space around the root was normal and there was no evidence of external apical root resorption at the most recent follow up assessment.
Medical Record Review
Records indicated that of the dogs followed up at the referral clinic, 3/29 (10.3%) teeth developed enamel fractures which required minor restorative treatment. 2/29 (6.9%) had significant abrasion to the treated teeth and required replacement of the restorations. These were noted in the same dog which was recorded as having an obsessive-compulsive behavior of chewing rocks. 1/29 (3.4%) was found to have additional abrasion but did not require treatment and 23/29 (79.3%) were in good condition and had no further trauma (fractures, abrasion, etc) at the time of follow up by the dental specialist. All the treated teeth were found to be sound and did not require extraction.
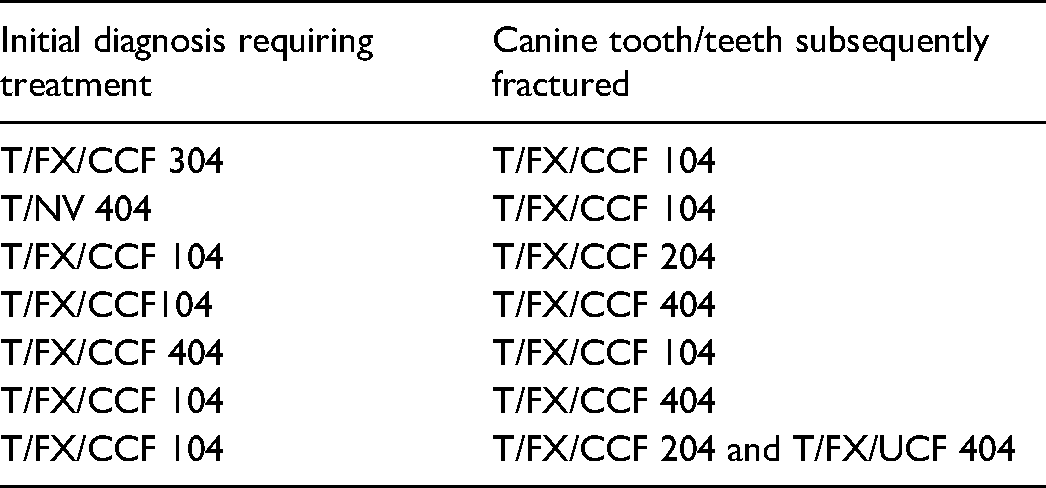
Record review also found ten out of nineteen dogs (52.6%) had trauma (abrasion, uncomplicated crown fractures, complicated crown fractures) to other teeth, indicating that these dogs continued to use their mouths for activities inclined to cause coronal damage. By nature of the technique described in this paper, the treated tooth was shorter than the remaining unaltered canine teeth. Eight previously untreated canine teeth were subsequently fractured during the time to follow up. The results are presented in Tables 1 and 2.
Results Obtained Through Medical Record Review Recorded by Veterinary Dentist at Subsequent Visit.
Initial Diagnosis of the Canine Tooth Requiring Endodontic Treatment and the Diagnosis of the Subsequently Fractured Canine Teeth.
Radiographic Evaluation
The success of the endodontic treatment utilizing an occlusal access aperture was evaluated. Intraoral radiographs using the bisecting angle technique and/or an occlusal view were obtained, immediately prior to and after initial treatment and again during the follow-up examination. These radiographs were reviewed by a board-certified veterinary dentist and a third-year resident, who agreed in all cases. Seven teeth had a periapical lucency and twenty-two teeth did not have a widened periodontal ligament space at the time of initial treatment. All twenty-nine teeth were found to have a normal periodontal ligament space width on the follow up radiographs. There were no new lucencies visible on any of the teeth, and there was no evidence of external apical root resorption on any of the radiographs (neither initially, nor at follow up). It was determined that 100% of the treated teeth did not require extraction or further endodontic treatment and twenty-four teeth (82.8%) did not require any further restorative treatment at the time of follow-up.
Discussion
Endodontic therapy and extraction are treatment options for non-vital or pulp-exposed teeth. In animals with periodontally sound teeth, endodontic treatment is advantageous over exodontia since it is less traumatic to the tissues, and the animal is not burdened by a wound to heal. Endodontic therapy has been determined to be safe, effective, and adherent to the ethical principles in veterinary dentistry.1, 2, 11
This study supports the use of a slightly simplified method of endodontic treatment through an occlusal aperture using rotary non-tapered NiTi files, by showing it was effective and resulted in successful outcomes in 100% of the cases. All the treated teeth had a normal periodontal ligament space width and there was no evidence of external apical root resorption at the time of follow up. To the author's knowledge, there are no peer-reviewed studies on the use of an occlusal access site to debride, shape and obturate a dog's canine tooth. A much larger study, which evaluated the results of root canal treatment accessed as per previously published canine literature3, 12 in dogs showed an overall success rate of 69%. 2 The aforementioned study included incisors, canines, maxillary fourth premolars, a mandibular fourth premolar and first molar teeth. It had a shorter follow up time and some teeth classified as failures may have healed over a longer time period. 2 In addition, the root canal treatments performed in this previous study were performed by several different operators and it has been reported that the experience of the endodontist may influence outcome.13, 14
The present study also demonstrates that the natural canine crown can remain healthy without the protection of a prosthetic crown. Although veterinary studies have looked at the outcome of prosthetic crown placement and at the success rates of endodontic treatment, the authors did not find literature specific to the success of endodontically treated canine teeth in pet dogs without the placement of a prosthetic crown.
The purpose of an access site is to establish an unrestricted pathway through the pulp cavity to the apex of the tooth in order to instrument the canal to debride, shape and obturate completely.11, 15–17 In a dog's canine tooth, straight-line access is described as an access at the mesial aspect of the canine tooth, 2-3 mm coronal to the gingival margin directed towards the apex.11, 15, 18 Straight-line access is important when using stainless steel files due to their stiffness and tendency to straighten out in curved canals, increasing the chance of ledging, transportation, stripping or zipping.11, 15, 19 Tapered files result in the removal of more dentin (in comparison to the same ISO sized non taper file) to accommodate the taper. NiTi files are flexible due to their elasticity and memory. 11 It was due to the flexibility of the non-tapered NiTi files that the apex of the teeth could be instrumented effectively.
The long-term prognosis is an important factor when making treatment recommendations. A common cause for extraction of endodontically treated teeth in humans is subsequent tooth fracture.2, 20, 21 The authors chose to eliminate cases in which the follow up was less than two years, to evaluate a longer-term prognosis. Teeth included in this study were followed up within two to nine years, with a mean of 4.5 years, after endodontic treatment.
The canine tooth is designed to pierce, tear and hold a victim and to be used as a weapon when fighting. 22 The authors believe these actions are not required of a pet, and these behaviors should be discouraged for many reasons, one of which is to prevent further damage to the remaining crown after endodontic therapy and to all other teeth. Prosthetic crowns have been recommended in both working dogs and pet dogs after root canal therapy to protect the remaining crown from further damage.20, 23 With patients that are aggressive chewers or with “cage biters”, prosthodontic crowns do not eliminate the risk of prosthetic crown damage or tooth fracture. 20 The results of the present study document that the natural canine crown can do well without additional protection of a cast metal crown. In working dogs, the canine teeth may be required to perform as designed and the stresses imposed on them are inherently higher than what is expected in a pet. This study looked specifically at the crowns of endodontically treated dog canine teeth in pet animals; none of the dogs were doing bite work.
The law of tooth conservation is noted to be important when performing endodontic and/or restorative procedures to preserve the strength of the tooth structure.5, 11, 15, 18 In dogs, it is common to instrument and obturate through the fracture site for incisor teeth, as is common in feline patients with fractured canine teeth. This practice follows the law of tooth conservation to prevent the weakening the tooth from an additional access site.18, 24 The authors propose that this can be applied to dog canine teeth and are suggesting that an additional (mesial) access site could weaken the tooth at the fulcrum and increase the risk of further fracture (Figures 2A and B). In the present study, several of the treated teeth were reduced in height, therefore sacrificing some of the crown structure (others were reduced in height by the fracture itself). Despite the law of tooth conservation, it has been established that the length of the crown does not add strength to the canine tooth.25, 26 In fact, one study concluded that reducing the height to diameter (H/D) ratio of a dog's canine tooth increases the fracture resistance of that tooth. 25 They determined that reducing the canine H/D ratio by 10% and 20% resulted in a decreased probability of fracture by 24.1% and 60.4%, respectively, compared to the unaltered canine teeth. 25 As mentioned in the introduction, further studies on force to fracture the crowns of canine teeth of dogs, first having endodontic shaping and obturation may be warranted.
Twenty-two teeth in this study had reduced crown height due to the fracture itself. Seven of the teeth were non-vital teeth with intact crowns. Since measurements of the crowns were not obtained at the time of the procedure, the exact reduction in crown height was not documented. However, subjective assessment using photographs showed 5/7 of the non-vital teeth had been reduced in height by 50%; 1/7 appeared reduced by 33% and 1/7 could not be determined based on available records. Of the 22 fractured teeth, only 17/22 could subjectively be assessed for the percentage of crown height reduction. Of these, the fracture reduced 7/17 crowns by ∼75–80%; 1/17 by ∼66%; 4/17 by ∼50%; and 5/17 by ∼20–25%. Teeth missing 50% or more of the crown were not reduced further, other than to smooth and shape the occlusal surface so that it did not come to a sharp point, have rough edges, and did not have overhang of enamel. Teeth wherein the fracture had caused a 20–25% reduction in crown height were assessed as having 50% reduction of the original height after the procedure was complete.
Along with altering the appearance of the non-vital crown, another concern with shortening the crown to facilitate treatment is the risk of fracture of the remaining normal canine teeth.23, 27 In the above mentioned study investigating the influence of crown height to diameter ratio on fracture force, it was predicted that the reduction of the H/D of one canine tooth may increase the risk of fracture for the remaining unaltered canine teeth. 25 It was predicted that there would be a 54.4% increase in probability of fracture of the unaltered contralateral canine tooth. 25 Although not the focus of the study, it was noted that of the 19 dogs included in the study that returned to the hospital for subsequent treatment, seven of the dogs had fractured another canine tooth (one dog fractured two canine teeth, totalling eight subsequently fractured canine teeth). It may be worth noting that these subsequent fractures were not all of the contralateral canine tooth. In fact, only two out of eight subsequent fractures involved the contralateral tooth. It is not possible to conclude that these subsequent fractures were a result of the shortening of the canine tooth, since continued inappropriate oral activity would be a significant factor. Further investigation is required to assess whether a shortened crown poses a significant increase in risk of fracture of the other normal canine teeth. One may infer that if shortening a crown increases the risk of fracture to other canines, so may extraction of a canine tooth, and also the common practice of crown reduction procedures performed as treatment for malocclusions. As with all medical treatments, risk and benefit must be considered.
In this study, the structural integrity of the crowns of treated teeth was found to be sound. 23/29 teeth (79.3%) of the crowns were recorded as having had no additional damage. 6/29 teeth (20.7%) were recorded to have had damage to the remaining restored crown, none of which resulted in exodontia. Three of these six teeth were found to have an enamel fracture at the level of the gingival margin and required minor restoration (two of these required minor type I crown lengthening procedures to facilitate the restoration). Two crowns with damage, requiring subsequent treatment, were in one dog, known to be a compulsive rock-chewer who had worn the crowns down and required replacement of the restoration in both teeth.
Subsequent fracture of the crown after treatment proved not to be a high risk. In this study, resulting enamel fractures (in 3/29 teeth) did not necessitate extraction. It was once thought that dentin of endodontically treated teeth was more brittle due to water loss and the loss of collagen cross-linking, however further studies concluded that endodontic treatment and the loss of water did not decrease the compressive and tensile strength values.28, 29 Non-vital dentin is 3.5% more brittle than vital dentin, which is likely not significant to the structural integrity of the crown. 30 To restore the access site, a nano-filled composite resin was chosen for its properties of mechanical strength and polishability.
One study reported an incidence of subsequent fracture following endodontic treatment and restoration to be 3.7% in dog teeth. 2 Whereas, in another study, the incidence of fracture of a prosthodontically treated tooth was found to be 10.3%. 20 In contrast to the present study, six out of seven fractured teeth were in working dogs; one of these six teeth did not have endodontic treatment performed; and one was an upper fourth premolar tooth. 20 In another study looking at the convergence angle and clinical outcome of full veneer crowns, 9.67% of the crowns studied were lost because of a tooth fracture. This was similar to the findings of a study exclusively evaluating performance of prosthetic crowns placed on damaged canine teeth of working dogs, which demonstrated a fracture rate of 9.8%.23, 31 The present study does not investigate whether the resulting crown structure could withstand the performance of a working dog required to do bite work.
To meet the expectations of the clients, it is important to discuss the goals of therapy, the technique, and the physical characteristics of the resulting tooth appearance prior to proceeding with endodontic treatment. Using photographs of other cases can set the client up for realistic expectations, particularly when treating non-vital teeth with this technique.
The placement of a crown is accompanied by additional cost and risks associated with the additional prep time, materials, fabricating costs, and a second anesthetic procedure for the pet. This may be of importance for patients with concurrent disease compromising their health. The crowns included in this study remained structurally sound, concluding that the additional protection of a cast metal crown would have been unnecessary in these cases. In total, it was determined that 29/29 (100%) of the endodontically treated teeth in this study remained structurally sound throughout the study period.
As with all retrospective studies, there are several limitations in this study. The population size was limited. Follow ups were not standardized or blinded and repeat photographs were not obtained for all dogs. In addition, several potential cases were excluded due to being lost to follow up.
Materials
K-reamer, Shipps Dental & Specialty Products, Marana, AZ K-file, Brassler Canada, Quebec, QC Canada LightSpeed LSX Files, Kerr Corporation, Orange, CA No Name, Loblaws, Toronto, ON Canada EndoVac System, Discus Dental, Culver City, CA 0.9% Sodium Chloride, Braun Medical, Bethlehem, PA Q-Mix, Dentsply Tulsa Dental Specialties, Johnson City, TN Absorbent Paper Points, DiaDent, DiaDent Group International Inc, Burnaby, BC Canada Parallax Absorbent Paper points (60 mm), Shipps Dental & Specialty Products, Marana, AZ AH Plus, Dentsply Maillefer, Tulsa, OK GuttaFlow 2, Coltene/Whaledent Inc, Cuyahoga Falls, OH Gutta Percha Points, DiaDent, DiaDent Group International Inc, Burnaby, BC Canada Parallax Gutta Percha Points (60 mm), Shipps Dental & Specialty Products, Marana, AZ Uni-Etch with BAC, Bisco Inc, Schauburg, IL MPa Max, Clinician's Choice Dental Products Inc, London, ON Canada MPa, Clinician's Choice Dental Products Inc, London, ON Canada GrandiO Caps, VOCO GmbH, Cuxhaven, Germany Neoburr, Denteq Medical Technologies, Eggenstein-Leopoldshafen, Germany Vivacaine, Novocol Pharmaceutical of Canada Inc, Cambridge, ON Canada Metacam Solution for injection, Boehringer Ingelheim, Duluth, CA Metron Imaging software, Creston, CA Scan X, Air Techniques, Melville, NY
Footnotes
Author's Note
Fraser A. Hale is also affiliated with Hale Veterinary Clinic, 159 Fife Rd. Guelph, Ontario N1H 7N8, Canada.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.