
Abstract
Despite its social importance, the care sector, particularly early childhood education and care (ECEC) and long-term care (LTC), faces a persistent ‘care trilemma’: balancing decent working conditions, public expenditure constraints, and broad service coverage. This paper examines strategies to address this trilemma in Hungary and Slovakia, where care provision follows a ‘low-road’ trajectory marked by underinvestment, poor job quality, and workforce shortages. The paper argues that institutional constraints, weak national coordination, and actor fragmentation limit systematic solutions. Instead, in the absence of cohesive national care policies, mitigation strategies emerge primarily at the local level. These initiatives often operate outside established bargaining structures and are driven by a fragmented actor landscape, including the emergence of new actors beyond formal industrial relations. These localised efforts provide important insights into potential pathways for reform. By highlighting the role of local actor interactions, the paper’s contribution lies in demonstrating how solutions may emerge in contexts where coordinated policies and bargaining failed to improve wages and working conditions in care.
Keywords
Introduction
Care work is an essential service in post-industrial societies, providing jobs for a significant share of the workforce and access to care services for vulnerable groups. Specific subsegments of the care sector, including early childhood education and care (ECEC) and long-term care (LTC) for those in need, resemble a social investment turn (Busemeyer and Garritzmann, 2019), where caring societies contribute to human capital accumulation, reducing social inequalities and higher labour market participation through relieving the burden of care provided by family members. For many socio-cultural professionals working in the care sector, for example, nurses, teachers, and professional carers, working in ECEC and LTC is a lifetime mission rather than just a job (Kitschelt and Rehm, 2014: 1700). Yet, as Szabó (2024) argued, even when seeing work as a mission, material politics remains relevant in the care sector just as in any other sectors (Kristal and Cohen, 2017).
Material politics refers to the responses of socio-cultural and public service actors to the material grievances arising from the pressures of professionalisation, proletarianisation, and welfare distribution in the post-industrial era (Szabó, 2024). From the perspective of users and providers of care services, material politics refers to securing access to care services while acknowledging budgetary constraints. From the care workers’ perspective, material politics refers to demands for decent working conditions including wages. The challenges emerging from material politics thus refer to a so-called care trilemma – securing decent working conditions and job quality, allocating public expenditure to address budget constraints in care services, and ensuring coverage of care services for those in need (Mori et al., 2026).
This paper examines the care trilemma in two Central and Eastern European (CEE) countries – Hungary and Slovakia. The aim is to explain how progress in addressing improvements in working conditions and access to quality care services can be reached in conditions of a so-called ‘low road’ of care services, where the trilemma refers to a lack of care provision and simultaneously a lack of improvements in working conditions and in tackling workforce shortage. The first step towards such an understanding is uncovering the working conditions in the care sector. The second step is analysing how the evolving interactions of industrial relations actors contribute to addressing the trilemma in specific institutional conditions at the national and local levels. In other words, the paper examines the actors who influence efforts to address the above challenges and how their interactions shape the material politics of resolving the care trilemma.
The paper argues that the above conditions can be explained by the existing dynamics of actors’ relations and institutional limitations. This state of the art fuels a lack of cooperation and an absence of a national care policy in both countries. Nevertheless, actor fragmentation and the lack of national policy produced relevant yet limited local solutions to address the trilemma. In the absence of national influence, trilemma solutions are facilitated through local, often informal, social dialogue structures (Pond, 2005). While Hungary relies on municipalities exercising patronage/paternalism over decisions regarding care services and thereby pre-empting social dialogue, Slovakia sees a more structured social dialogue to address the trilemma. At the same time, in Slovakia, vocal actors have been emerging beyond the established industrial relations structures, raising competition of interests at the local level with implications for sector-level bargaining and actor structures.
The paper is structured in five sections. The first develops a conceptual framework on the role of industrial relations actors in addressing the care trilemma in Hungary and Slovakia. The second outlines the methodology. The third examines evidence of the trilemma in ECEC and LTC sectors, focusing on employment, expenditure, and job quality. The fourth applies the framework to analyse actor dynamics and solutions based on case studies. The final section discusses the findings.
The care trilemma and industrial relations: A conceptual approach
Care services covering ECEC and LTC constitute two central pillars of welfare state provision and serve as key indicators of social investment and redistribution. Despite recurrent narratives of welfare state crisis, expenditure and institutional reform in social services have expanded in many countries since the 1990s (Kim, 2017). Yet, this expansion has been shaped by persistent structural trade-offs.
Trade-offs in care services can be understood through a sector-specific trilemma of three often competing priorities: budgetary expenditure, service coverage and job quality, particularly wages and working conditions (Esping-Andersen, 1999; Iversen and Wren, 1998; Pavolini et al., 2013). These dimensions reflect broader tensions in care services, where funding constraints often force compromises across key areas. Recent literature highlights a persistent trade-off between resource allocation and service quality. For instance, Pickard et al. (2018) longitudinal study shows that staffing and funding undermine both the availability and quality of care, placing additional pressure on caregivers who often combine professional and informal responsibilities (Pickard et al., 2018). Similarly, Cleary et al. (2013) demonstrate how resource constraints and bureaucratic inefficiencies weaken accountability and limit the quality of care provision.
These challenges are further compounded by systemic underfunding, which contributes to poor working conditions and high staff turnover (Nivorozhkin and Poeschel, 2021). The shift towards deinstitutionalisation and greater reliance on informal care also plays a role. Pickard (2012) cautions against substituting formal care with informal provision, as this increases unpaid, emphasising care burdens and may ultimately undermine formal care systems (Pickard, 2012).
This sectoral care trilemma mirrors the broader structural trilemma identified by Iversen and Wren (1998), in which governments in service-based welfare states face trade-offs among budgetary restraint, wage equality, and employment growth. However, welfare regimes differ in how they manage these tensions. Esping-Andersen’s (1990, 1999) typology provides an institutional lens: liberal regimes prioritise market solutions and cost containment, expanding low-paid service employment often at the expense of wage equality and job quality (Esping-Andersen, 1990, 1999). Corporatist regimes preserve status differentials through employment-based social insurance, with more limited service expansion and continued reliance on family-based care. Social democratic regimes emphasise universalism and decommodification, expanding public services while sustaining wage equality and accepting higher fiscal costs (Esping-Andersen, 1990; Pierson, 2001).
These regime strategies intersect with care policy trajectories, ranging from ‘familialism by default’ to ‘familisation’, shaping responses to rising care demands (Le Bihan and Martin, 2012; Verbakel et al., 2023). Familialistic systems tend to limit professionalisation and labour market stability, exposing workers to greater job insecurity (Marchetti and Scrinzi, 2014). In contrast, more de-familialised systems institutionalise care provision, reduce reliance on families and strengthen both worker rights and service quality (Le Bihan and Martin, 2012; Leitner, 2003).
The ongoing challenge of balancing expenditure, coverage, and quality in ECEC and LTC is intensified by demographic ageing and rising female labour force participation, which increase demand for care services. In response, policy frameworks have shifted towards a ‘Social Investment Turn’, aiming to boost employment and human capital through effective care provision (Eggers, 2022; Klenk and Reiter, 2023). While this elevates care as a strategic priority for economic performance and social equity, many countries face acute labour shortages in ECEC and LTC, exacerbated since the COVID-19 pandemic (Zacharenko, 2024). Despite their essential role, care sectors often operate with persistent staffing deficits, increasing workloads without improving employment conditions (Österle, 2010). These trends reinforce the ‘care penalty’, characterised by low pay, high work intensity, and limited career prospects (Bechter et al., 2012; Rummery, 2021).
At the same time, the organisation of care in ECEC and LTC sectors can be distinguished by the system’s integration and levels of organising care, including, for example, local, regional, and national levels (Pavolini, 2022). In terms of integration, care services can be integrated, split, or operate as separate systems (ibid.; European Commission, 2025). An integrated system refers to unitary care governance with a single key ministry in charge. In the case of ECEC, all the services for children from birth age up to the age of compulsory primary education are cared for and educated in a single, integrated structure, while for LTC, that means the integration of the health and social care services into one care provision system.
Hungary and Slovakia share a policy legacy of partial marketisation of care services combined with supported familiarism (c.f. Saraceno and Keck, 2010; Mori et al., 2026), where families remain central in providing care despite some state support. While policies include cash transfers to households, budget constraints and limited service availability restrict the professionalisation of care. Both countries also share institutional legacies of welfare states and industrial relations, classified as embedded neoliberal systems balancing market transformation with social cohesion (Bohle and Greskovits, 2012). However, persistent gaps remain, including limited care provision, low wages, and poor working conditions (Bohle and Greskovits, 2012; Bors and Kahancová, 2023; Holubová, 2023; Mori et al., 2026). This situation reflects a ‘low-road’ trajectory, characterised by insufficient service coverage, low public investment, and limited improvements in job quality, including wages, workload and labour shortages.
Industrial relations as drivers of change
Building on the low-road dynamics of the care trilemma, our framework examines how industrial relations actors contribute to addressing the identified tensions of material politics. Their primary focus within the trilemma lies on working conditions and wages, but this is also closely related to budgets and access to care. Staff shortages, often rooted in poor working conditions, can further constrain service provision. Accordingly, the analysis centres on how industrial relations actors influence wages and working conditions as key levers in addressing the care trilemma.
The capacity of industrial relations to improve care work depends on national institutional contexts (Bechter et al., 2012). Strong collective bargaining systems are generally associated with better working conditions, whereas liberal regimes tend toward precarisation and lower job quality (Bechter et al., 2012; Zacharenko, 2024). Labour regulation, central to our analysis, interacts closely with public funding, as governments face fiscal constraints that limit improvements in working conditions alongside service expansion (Borgermans et al., 2017). It is therefore crucial to assess the levels at which industrial relations actors can intervene through bargaining or policy influence.
Focus on local and regional actors within multi-level governance structures
To understand actor dynamics in the care sector, country-specific institutional conditions and levels of action can be conceptualised using the multi-level governance (MLG) framework in industrial relations (Marginson and Keune, 2015). While MLG typically focuses on transnational, national, sectoral and company levels of interactions, the regional and local levels are often overlooked despite their key role in adapting national policies to local socio-economic (Regalia, 1998: 157-158).
Recent debates highlight the growing importance of local actors in addressing labour market challenges, including employment, social protection, and access to services (cf. Leuprecht and Lazar, 2007). Within this framework, local actors operate between national directives and local needs, generating both innovation and tension. A key issue is whether they merely implement top-down policies or actively shape them through feedback and local initiatives. These interactions reflect power dynamics, as local actors may advocate improvements in care provision, but outcomes depend on governance structures and their capacity to influence policy decisions.
Applied to the care sector, the focus on actors’ interactions below the national level is justified for several reasons. Countries like Hungary and Slovakia are primarily characterised by decentralised governance systems, yet a legal and financial dependence on higher-level authorities – the central government. In Hungary, the 2011 Act on Local Governments re-centralised several competencies, underscoring the central government’s predominant role in local affairs (Committee of the Regions, 2019). Similarly, in Slovakia, despite constitutional provisions for municipal and regional self-governance, both levels are territorially and administratively independent yet heavily reliant on central financial allocations (Committee of the Regions, 2020). This dependency also impacts the effectiveness of local actors, making it more difficult for them to address region-specific issues and challenges. Following several waves of new public management reforms in both studied countries, care services are now extensively decentralised; however, the budgets available to local and regional authorities to secure care services are allocated at the central government level. In ECEC, it is the municipalities, rather than the central government, that operate educational facilities and manage their budgets. In LTC, while some care homes operate as private units in both Hungary and Slovakia, most facilities are operated by municipalities and higher territorial units.
Finally, by examining the dynamics of industrial relations actors and their interaction with regional and local authorities in care, we assess each actor’s capacity to drive improvements in working conditions. Drawing on an institutionalist perspective on capitalist actor constellations, we ask whether municipalities, social partners, and the state act as ‘policy makers’ shaping care provision across governance levels, or whether they adapt to existing system institutional care arrangements and remain ‘policy takers’ (Streeck, 2011).
Policy makers establish and adjust rules, in this case, the framework determining care workers’ working conditions, wage setting and wage levels (c.f., Streeck and Thelen, 2005: 13). Rulemaking often occurs amid conflict and competition, which the rule takers are expected to follow and live. In some rare instances, these roles may overlap. In a multi-country comparative analysis of responses to COVID-19, Stoney et al. (2023) found that local governments primarily acted as policy takers; however, in areas where they had discretion, they adapted policies to local needs, thereby becoming policy shapers or even policy makers. The degree of local autonomy in this case depended on the national governance structure, with federal systems providing more room for municipal initiative than unitary ones.
Building on the above framing of care services, the care trilemma, and its material politics, the remainder of this paper examines how industrial relations agency, particularly at regional and local levels, contribute to addressing the challenges of the care trilemma, and whether dynamics differ between ECEC and LTC in both countries. Given the MLG structure of care provision in Hungary and Slovakia, special attention is paid to the constellation of social partners, but also municipalities and regional governments as key actors in care provision.
Methodology
The empirical analysis employs a mixed-methods approach. Statistical data on care provision, public expenditure and care employment draw on Eurostat and national resources, while the structure and dynamics of industrial relations actors in ECEC and LTC are based on interviews. The authors conducted 18 interviews in Hungary (10 with national and sectoral social partners in ECEC and LTC, and 8 with regional and local actors) and 30 interviews in Slovakia (11 with national and sectoral social partners, care providers and other stakeholders, 19 with local and regional actors) in person or online in 2021–2022. All interviews were anonymised, transcribed and thematically analysed.
At the sector level, the analysis focuses on service provision structures, industrial relations actors, bargaining processes and collective agreements. At the local and regional levels, case studies captured actors’ responses to gaps in addressing the care trilemma. Interviews from both levels were analysed jointly to construct cases for cross-country and cross-sectoral comparisons, selected based on actors’ engagement across levels and efforts targeting one or more dimensions of the trilemma. These cases are summarised in the Section focusing on actor dynamics.
The comparative analysis focuses on ECEC and LTC, as well as a cross-country comparison. The sector-specific comparison is relevant for evaluating the actors’ ability to address the care trilemma in sectors facing similar challenges, despite some differences in actors’ structures and national institutional differences in how actors can affect wages and working conditions. The cross-country comparison of Hungary and Slovakia offers a chance to examine two Central and Eastern European countries that have been connected for many decades by a similar trajectory of industrial relations and social welfare development. Following the changes in political and economic regimes, their entry into the European Union, and the degree of centralisation, addressing the trilemma could take on its specificities.
Uncovering the care trilemma in Hungary and Slovakia
Hungary and Slovakia were selected for comparison based on several contextual similarities in the structure of care service funding, sectoral challenges, and the scope of social actors involved. The focus is exclusively on two types of social services – ECEC and LTC, since these are at the heart of social service provision for vulnerable groups in society. At the same time, social services resemble a stable workforce (despite shortages) and a decent union presence.
Operationalising the three poles of the care trilemma (expenditure, coverage, working conditions), this section introduces comparative data on employment in the care sector, public expenditure on LTC and ECEC (as a share of GDP), wages in the LTC and ECEC sectors compared to average wages in the economy, and the coverage rate of LTC and ECEC services. The LTC coverage rate is the share of people aged 65+ receiving home or residential care, and the ECEC coverage rate is the share of children aged 0–3 and 3–6 in education, as a share of the total number of children in these age groups.
In both countries, employment in both sectors accounts for less than 10% of total employment according to national statistics. Yet, employment in ECEC and LTC in Hungary and Slovakia illustrates a diverging trend. While in Slovakia, employment in education, including ECEC, has been steadily rising (reaching almost 8.5% of the overall employment in 2022), in Hungary, stagnation followed by a decline is noted since 2021 (ibid.). Employment trends in human health and social work (as a proxy for LTC in Eurostat) show long-term stability in both countries, with a slight increase in Hungary and a slight decline in Slovakia.
Both countries display gendered labour markets in ECEC and LTC, characterised by predominantly female workforce and challenges related to professional recognition and investment (Bors and Kahancová, 2023; Holubová, 2023). Evidence from national and European statistics confirms high female employment and a growing share of tertiary-educated workers (Eurofound, 2020, KSH, 2022). Both countries also face staffing shortages and rely significantly on informal care (ibid.).
In Hungary, local governments (46.7%) and the church-based institutions (33.1%) are the main employers in ECEC and LTC, while NGOs, business associations, and central government institutions play smaller roles (Gyarmati, 2022: 11). In Slovakia, services are provided mainly by public and non-profit providers. Although undeclared and non-standard work is less prevalent, Slovakia has one of the lowest ratios of LTC workers to the elderly population in the EU (1.5 per 100 individuals aged 65+), creating severe recruitment challenges, particularly in home-based care. Residential facilities face additional pressure to meet staffing and qualification requirements that are often unmet due to workforce shortages (European Commission, 2021).
Public expenditure on care remains low in both countries. In Hungary, spending on pre-primary education declined from 0.96% of GDP in 2008 to 0.67% in 2020 (Eurostat, 2024). Funding comes from a multi-actor scheme combining national budget allocations and subsidised parental fees. Despite reforms in 2017 that expanded and restructured nursery provision, the sector still faces limited access to services and persistently low wages. In Slovakia, ECEC expenditures increased from 0.44% of GDP in 2013 to 0.66% in 2020, remaining below the EU average. Funding relies heavily on local government budgets linked to income tax revenues, making childcare provision sensitive to fiscal changes (Eurostat, 2024).
LTC spending is also low. Eurostat data distinguish between health LTC (medical and nursing care) and social LTC (assistance with daily activities). In Hungary, public expenditure fluctuates around 0.30% of GDP, with fragmented financing across health and social services, contributing to uneven quality and regional disparities (Bors and Kahancová, 2023; Eurostat, 2024: 22-23). In Slovakia, LTC spending is also low at 0.9% of GDP compared to the EU average of 1.6%, with increasing reliance on EU funds and client payments due to weak coordination and unsystematic investment.
Low wages remain a central indicator of the care trilemma. In Slovakia, residential care workers earned about EUR 766 gross per month in 2019 (less than EUR 5/hour), while home care assistants earned only EUR 562 (Bors and Kahancová, 2023; Holubová, 2023). In Hungary, the average gross monthly wage in health and social care was approximately EUR 780 in 2020, with entry-level pay for unqualified staff as low as EUR 430 (KSH, 2020; Meleg, 2021). Although nominal wages increased, they have not kept pace with inflation or rising care demand (Eurofound, 2020).
By contrast, pre-primary teachers’ wages have improved moderately. In Hungary, average gross monthly wages in education reached EUR 895 by 2020, with some local governments offering bonuses (Gyarmati, 2022). In Slovakia, kindergarten teachers earned 93.2% of the national average wage by 2021, reflecting gradual growth in salaries, staff numbers, and qualifications (Rehuš and Ostertágová, 2022).
Worker shortages remain severe. Slovakia has only 1.5 LTC worker per 100 persons aged 65+, less than half the EU average (European Commission, 2021; Holubová, 2023). Hungary faces similar staffing shortages due to growing demand and ageing workforce (Bors and Kahancová, 2023). Worker density in ECEC for children aged 0–2 is declining due to limited capacity expansion and recruitment challenges, particularly in nursery care. Services for children aged 3+ are somewhat more stable: Hungary has maintained relatively stable numbers of kindergarten teachers, while Slovakia has increased their numbers in the past decade, though regional disparities persist (Bors and Kahancová, 2023; Holubová, 2023; Eurostat, 2024).
The care trilemma in Hungary and Slovakia.
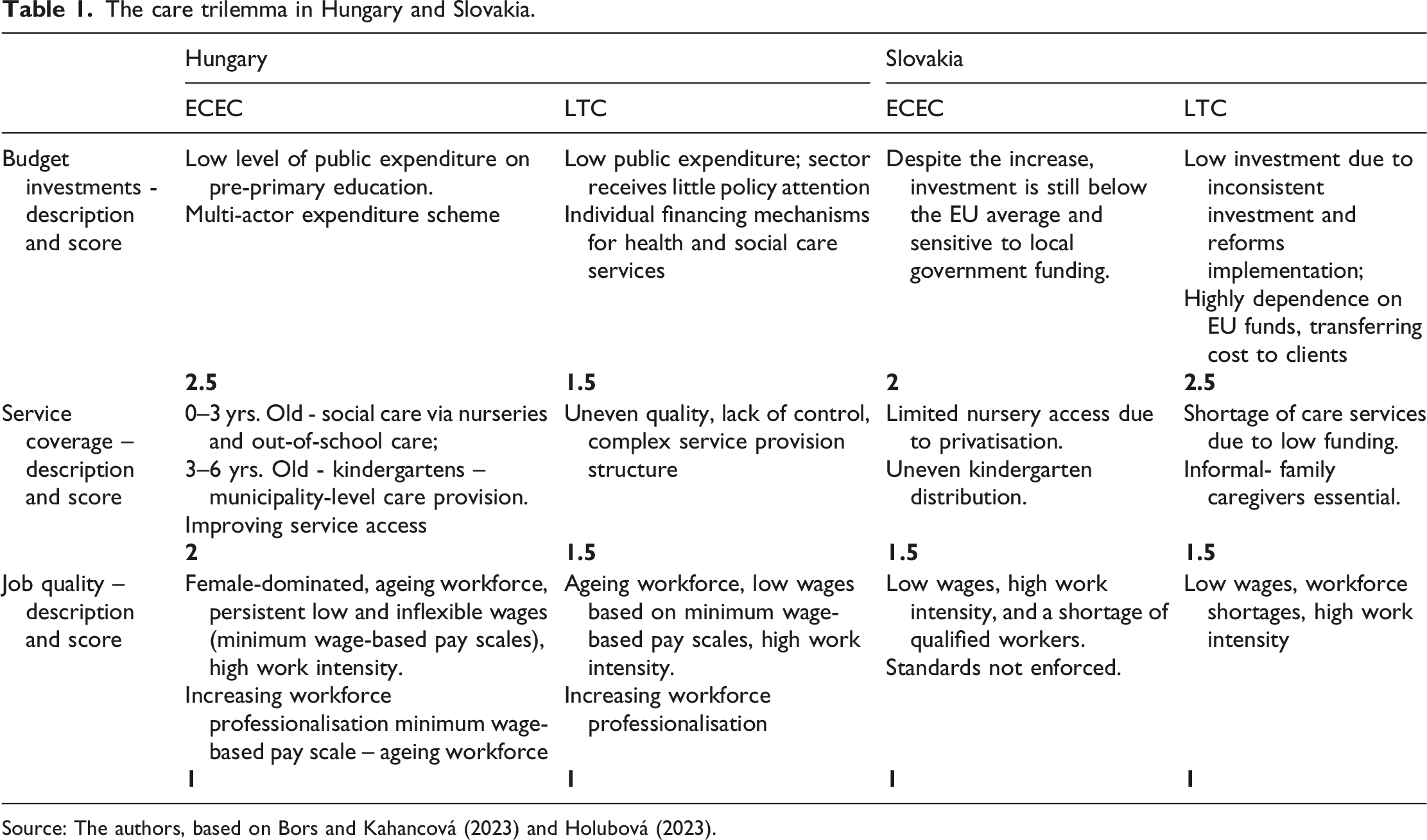
Source: The authors, based on Bors and Kahancová (2023) and Holubová (2023).
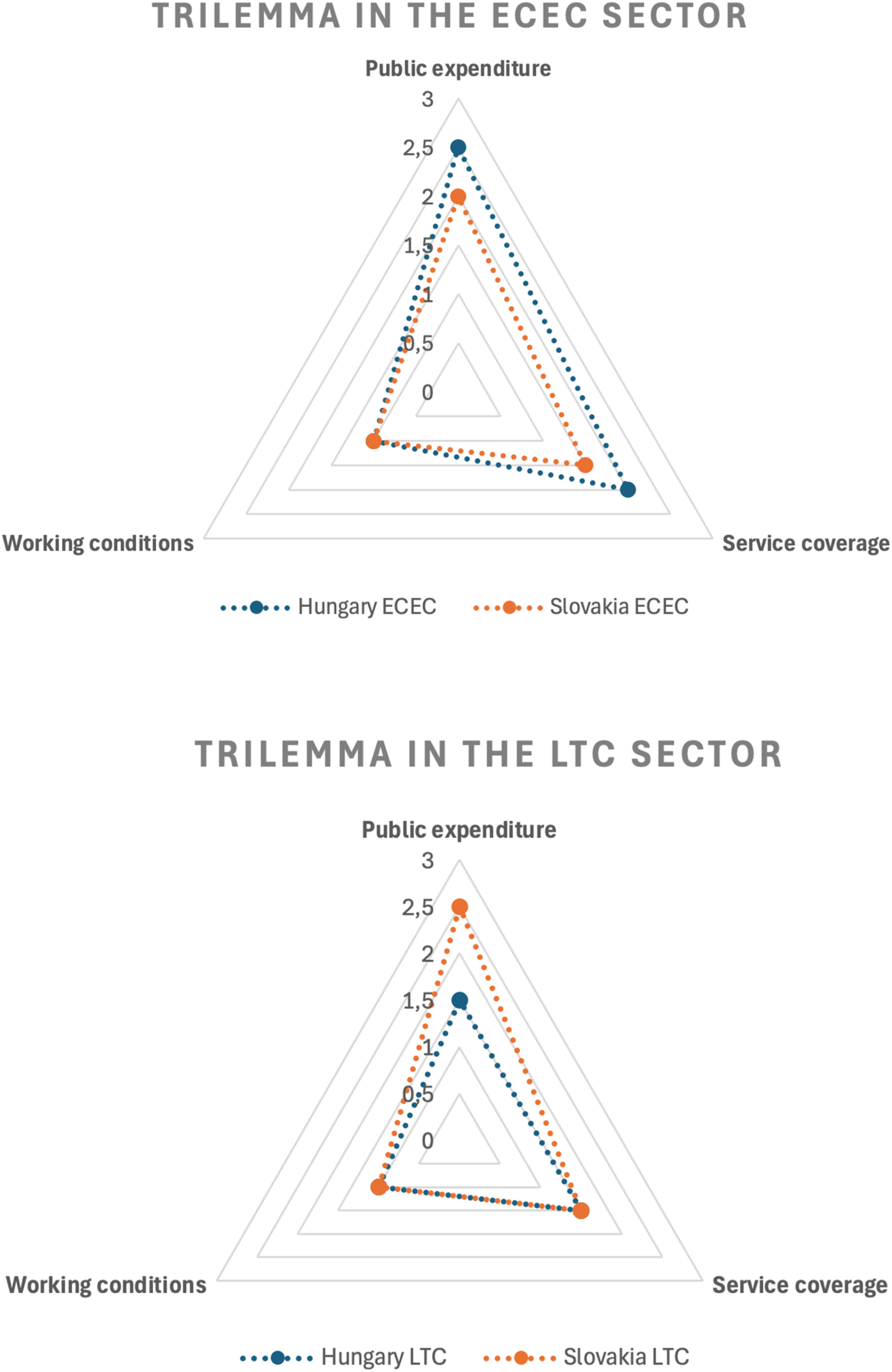
The care trilemma in the ECEC and LTC sectors in Hungary and Slovakia.
Based on Figure 1, the comparison of the care trilemma reveals several patterns. First, public funding for ECEC remains low in both countries, significantly below international averages. Hungary relies on a multi-actor financing scheme, while in Slovakia ECEC funding depends heavily on local government budgets. Slovakia’s ECEC expenditure per child aged 3–5 rose to 0.55% of GDP by 2016, below the OECD average of 0.6%, while Hungary’s decreased to about 0.71% in 2018. In LTC, EU funding plays a role in Slovakia, but in both countries, part of the costs is transferred to clients and their families. Public spending on LTC is critically low in Hungary (0.25% of GDP), compared to approximately 0.9% of GDP in Slovakia, both below the EU average of 1.6%. Second, service coverage in ECEC is higher in Hungary. With about 50,000 nursery places under age of three, this may increase pressure on job quality and service standards. In Slovakia, participation is just 5%, well below the 26% OECD average, and provision remains uneven and limited. While kindergarten access has improved due to compulsory attendance from age five, regional disparities persist. In 2020, over 18,000 applications were unmet. In LTC, provision is fragmented in both countries, with uneven quality and strong reliance on informal care. In Slovakia, waiting lists for residential care increased by 40% between 2016 and 2019. Third, job quality remains low across both sectors and countries, characterised by feminisation, ageing workforces, low wages, and high work intensity. In Hungary, care wages are among the lowest, with 85% of public service salary scales covered by the statutory minimum wage in 2021. Slovak LTC wages reached 78% of the average wage in 2018, while ECEC kindergarten teachers earned 93.2% of the average in 2021. Both countries face severe labour shortages, although Hungary shows some signs of increasing professionalisation. Overall, the analysis points to a ‘low-road’ trajectory in both countries and sectors, where job quality is often sacrificed to accommodate budgetary constraints and service expansion.
Actor dynamics in local responses to the care trilemma
Against the structural background of the care trilemma, this section examines specific initiatives and actor dynamics aimed at improving working conditions in both countries and subsectors. Besides social partners, municipalities play a central role as budget holders, giving local actors significant influence. Building on the multi-level governance framework, we examine whether local actors in the care sector primarily act as policy takers, implementing nationally defined rules, or as policy makers who adapt and supplement these frameworks in response to local constraints.
ECEC – Sector-wide challenges addressed by local actors’ dynamics
The Hungarian ECEC sector operates under a decentralised management system, with nurseries and kindergartens falling under different ministerial competencies. This fragmentation creates wage, qualification, and working-condition disparities. As an illustrative case, we examine the town of Veszprém in Western Hungary. While not representative of the national situation, this case is notable for maintaining a younger nursery workforce despite national staff shortages and low wages, making it useful for understanding the local response to the care trilemma.
Cooperation between the municipality of Veszprém and the local branch of the nursery trade union (BDDSZ) plays a key role in addressing everyday ECEC challenges. Their collaboration was particularly visible during the COVID-19 pandemic, when ECEC providers, the municipality, and BDDSZ representatives adapted services to lockdown conditions. Nurseries remained operational via online platforms, offering seminars for children and parents and assigning home-based educational tasks.
Interview respondents from the trade union and a local service provider noted that, in absence of coordinated national or sectoral solutions, local actors focused on stabilising employment and wages. To prevent workforce loss during the pandemic, the municipality supplemented the nationally set (low) wages with bonuses, reflecting a paternalistic approach to workforce support. Cooperation between social partners was crucial in implementing these measures and maintaining service provision.
This case illustrates how local cooperation between municipalities and trade unions can address elements of the care trilemma. Veszprém’s financial contributions, including wage bonuses and supplementary payments, helped stabilise the ECEC sector despite structurally low national wages. The local BDDSZ representation actively negotiated wage supplements, supported workers during disputes, and used these gains to recruit new members. The effectiveness of these initiatives thus depended on both the financial capacity and political responsiveness of the municipality and the strategic engagement of the trade union, offering an example of responsive decentralised labour relations within constrained national frameworks.
In Slovakia, ECEC faces similar challenges, particularly insufficient kindergarten capacity in some districts and quality concerns, reflected in large size classes, inadequate working conditions, and declining teacher qualification standards. Interview data indicate that local authorities (municipalities) prioritised expanding kindergarten capacities, renovating existing facilities and creating new places, rather than improving working conditions. Simultaneously, professional associations advocated higher quality standards through policy engagement and dialogue with local, sectoral and national authorities. While cooperation with established social partners exists, the interaction involves a broader range of actors beyond traditional social partners.
Local examples illustrate these dynamics. The Bratislava district of Petržalka used EU funds through the Ministry of Education to renovate and expand ECEC facilities, introduce recruitment incentives, and involve social associations in participatory decision-making. At regional and national levels, professional associations such as the Council for Kindergarten Development and the Society for Pre-primary Education contributed through informal regional dialogues, national working groups, media campaigns, and advocacy, despite lacking formal roles in national social dialogue. These multi-level initiatives occasionally revealed trade-offs between expanding service coverage and improving quality.
In sum, responses to the care trilemma in ECEC combined elements of paternalism and autonomy. The paternalistic dimension is visible in municipalities actively intervening in capacity management, wages, and service delivery, supported by national funding, which provides a top-down framework for actor interaction. In this respect, municipalities partly act as rule takers, implementing nationally defined frameworks, but also increasingly as rule shapers by exercising local discretion in how these rules are applied.
At the same time, an autonomous dimension emerged through the activities of trade unions in Hungary and professional associations in Slovakia, which advocated higher quality standards, improved teacher qualifications, and more participatory decision-making. Their influence largely occurred outside formal industrial relations structures, relying on mobilisation and dialogue rather than on institutionalised bargaining. In this sense, these actors function mainly as rule shapers, shaping local outcomes and policy interpretations despite limited formal power within national industrial relations systems.
LTC: A paternalistic approach meets actor cooperation
The LTC sector faces challenges like those in ECEC, including low wages, poor working conditions, an ageing workforce, and labour shortages. Coordination is further complicated by the sector’s division between healthcare and social care, which are managed separately at the national level.
Interview-based analysis highlights a local response in Veszprém, Hungary, where a Local Multipurpose Partnership was established in 2016 to mitigate sector-wide challenges. The partnership brings together 19 municipalities, jointly operating seven LTC institutions that provide a range of social care services.
Through this partnership, the municipality of Veszprém and surrounding municipalities play a leading role in supporting the LTC sector, aiming to maintain service standards and address workforce shortages. The municipality provides wage bonuses and other financial support to retain employees and safeguard care quality.
The partnership introduced several concrete measures. During the COVID-19 pandemic, it implemented a quarantine system and strengthened its IT infrastructure to maintain services and limit virus transmission. In addition, the municipality introduced a Performance Contract to attract doctors to LTC, offering incentives such as free medical office space.
This paternalistic municipal approach proved effective in addressing local LTC challenges. Cooperation among municipalities allowed resource pooling and coordinated action to improve working conditions and staff retention, demonstrating how local initiatives can partly compensate for limitations of the national industrial relations framework. However, trade union involvement remained limited. This reflects both the fragmented structure of unions in Hungary and the dominant paternalistic role of the municipality, which – together with limited local union capacity – prevented the development of cooperation like that observed in the ECEC case in the same municipality.
In Slovakia, trade union presence in LTC, particularly organisations affiliated with the Slovak Trade Union of Healthcare and Social Services (SOZZaSS), is well established in public care homes. Nevertheless, service provision remains fragmented, marked by weak coordination, geographical isolation, insufficient capacity, poor working conditions, and low wages. As regular collective bargaining delivered limited improvements, additional actor organisations have emerged outside the structures of established social partners, including associations of carers and associations of care providers.
At the local level, interview evidence highlights initiatives such as those in a marginalised district of Banská Bystrica, where Integrated Community-Based Social Service Centers (CSSCs) were created to overcome fragmentation. These centres improved coordination between municipalities and LTC providers by linking local, regional, and national service levels. In parallel, social partners pursued improvements in employment conditions, workplace safety, and wages through localised collective bargaining advocacy.
These processes involved both regional and local levels of governance. The pilot CSSCs, financed by the Regional Cohesion Fund, supported horizontal integration among municipalities and vertical coordination with regional and national authorities, strengthening the sustainability of LTC services. At the same time, SOZZaSS supported these initiatives through regional informal dialogue, preventive labour inspections, negotiation support, and legal counselling, contributing to collective agreements that secured wage increases of 10–20% and improved working conditions.
Actor dynamics in improving working conditions in care in Hungary and Slovakia.
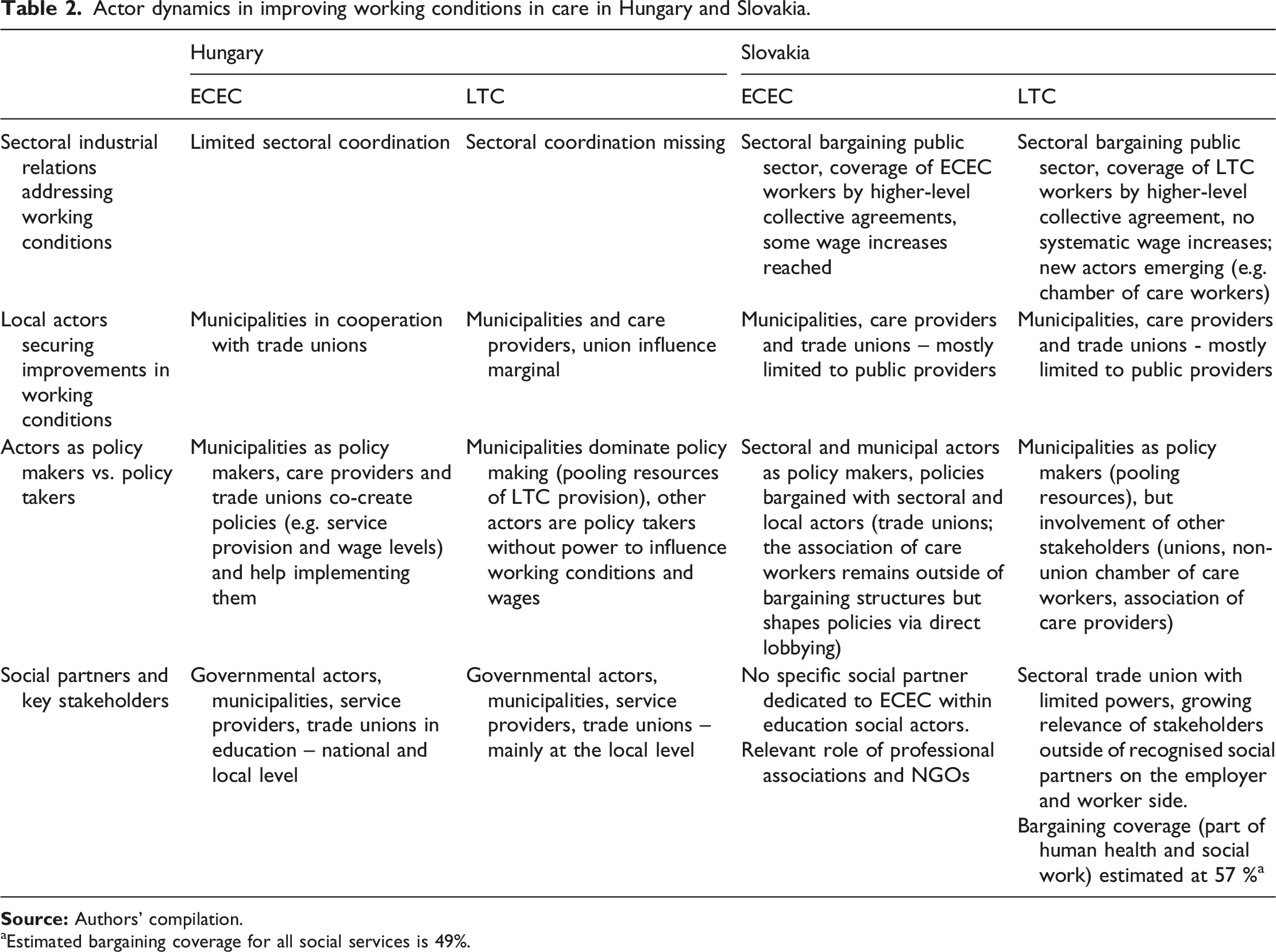
aEstimated bargaining coverage for all social services is 49%.
In Slovakia, by contrast, trade unions (especially SOZZaSS) partly transcend a rule-taking role through autonomous activities such as regional dialogue, legal counselling, and support for local collective bargaining. These initiatives contributed to wage increases of 10–20% and improvements in working conditions, demonstrating a stronger bottom-up dynamic that complements municipal and regional coordination efforts. Thus, Slovak unions act at least partly as rule shapers, influencing local outcomes despite the limited effectiveness of sector-level bargaining.
Comparing these findings within the MLG framework shows that sectoral and local coordination among actors is largely absent in the Hungarian LTC sector, although some cooperation exists in ECEC (see Table 2). In Slovakia, a higher-level collective agreement for public services formally ensures bargaining coverage for most care providers. However, this framework has delivered limited improvements in wages and working conditions, prompting the emergence of local initiatives outside formal bargaining structures.
In Hungary, the decentralised structure of social partners further reinforces the importance of local dynamics. In Slovakia, although the sector is formally covered by higher-level collective agreements, social partners have struggled to substantially improve working conditions or resolve the care trilemma.
Overall, local actors shift from rule takers to rule shapers where discretionary space and resources allow, but this transformation remains uneven and sector specific. Local policymaking can mitigate immediate pressures of the care trilemma, yet it rarely substitutes for missing national coordination. As shown in Table 2, some innovative solutions emerged through cooperation among multiple stakeholders, while in other cases, municipalities dominated decision-making on care provision and working conditions, leaving trade unions and care providers with limited influence.
Conclusions
Care work reflects a social investment approach that supports human capital and reduces inequalities, yet it faces tensions captured by the care trilemma: balancing job quality, budget constraints, and service coverage. This paper examines the role of industrial relations actors, arguing that persistent gaps in provision, working conditions and workforce shortages stem from actor configurations, interaction dynamics, and institutional constraints. In the absence of effective national cooperation and comprehensive care policies, it focuses on local-level dynamics, using a MLG framework to assess whether locally embedded initiatives can address these challenges.
The analysis unfolded in two steps: first, it assessed working conditions in the care sector in the studied countries; and second, it examined how industrial relations actors and local governments interact within institutional contexts to address these challenges and shape the material politics of care provision. Conceptually, the analysis distinguishes between actors who act as rule shapers and those remaining rule takers.
The findings show that actors move between these roles depending on sectoral conditions and institutional capacity. Municipalities frequently emerge as de facto policy makers, exercising discretion over service provision and resource allocation, while trade unions and professional actors alternate between policy-shaping and policy-taking roles when attempting to influence working conditions and address the care trilemma.
The analysis confirms that both Hungary and Slovakia prioritise service coverage and fiscal restraint over improvements in working conditions, reinforcing a persistent ‘low-road’ trajectory. This prioritisation is evident in the systematic underfunding of the sectors. To manage these fiscal limits while expanding coverage, job quality is the primary sacrifice. Policies expanding access, such as Hungary’s expansion of nursery capacity or Slovakia’s mandatory kindergarten attendance, therefore rely on maintaining low labour costs, resulting in wages that remain among the lowest in the economy. Furthermore, more stable union structures and higher bargaining coverage in Slovakia have no visible effect on the care trilemma compared to Hungary. This suggests a significant gap between formal industrial relations structures and actual agency, as unions often pivot away from failed sectoral bargaining toward political lobbying or local mobilisation.
It has been expected that reliance on family-based care reduces pressure to expand services and limits the influence of industrial relations actors in the sector. Contrary to this expectation, the paper shows that resolving the care trilemma in resource-constrained contexts depends on shifts in multi-level governance. In the absence of cohesive national policies, improvements emerge through different local dynamics. In Hungary, municipal paternalism plays a central role, with local authorities acting as ‘patrons’ who pool resources and provide wage bonuses or performance contracts to stabilise the workforce. However, this often bypasses established industrial relations actors and governance mechanisms, relying instead on top-down resource allocation. In contrast, in Slovakia, advocating for improvements in job quality and service coverage is driven by the more autonomous mobilisation of new actors, such as professional associations and unions, operating beyond traditional industrial relations structures and local government authorities.
Despite the ongoing ‘low-road’ trajectory of care regimes in Hungary and Slovakia, marked by limited public funding and poor job quality, local efforts have partially alleviated the care trilemma pressures. Municipalities, service providers, and local trade unions have introduced initiatives that temporarily fill gaps left by national policies. Addressing issues of job quality, service coverage, and budgetary constraints, these interventions demonstrate the potential of subnational governance and locally embedded social dialogue to deliver flexible solutions, such as tailored collective agreements or municipal wage supplements, particularly in response to labour shortages. However, these efforts remain fragmented and geographically limited. In the absence of coordinated national care strategies, they function mainly as local coping mechanisms rather than addressing systemic challenges in the care sector.
Footnotes
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Findings of this paper are drawn from the project funded by the EU Commission - DG Employment, Social Affairs and Inclusion ‘SOWELL – Social dialogue in welfare services. Employment relations, labour market and social actors in the care services’ (GA VS/2020/0242).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.