
Abstract
Background
Higher rates of postoperative complication following cleft lip or palate repair have been documented in low resource settings, but their causes remain unclear. This study sought to delineate patient, surgeon, and care environment factors in cleft complications in a low-income country.
Design
Prospective outcomes study.
Setting
Comprehensive Cleft Care Center.
Patients
Candidate patients presenting for cleft lip or palate repair or revision.
Interventions
Patient anthropometric, nutritional, environmental and peri- and post-operative care factors were collected. Post-operative evaluation occurred at standard 1-week and 2-month postoperative intervals.
Main Outcome Measures
Complication was defined as fistula, dehiscence and/or infection.
Results
Among 408 patients enrolled, 380 (93%) underwent surgery, of which 208 (55%) underwent lip repair (124) or revision (84), and 178 (47%) underwent palate repair (96) or revision (82). 322 (85%) were evaluated 1 week and 166 (44%) 2 months postoperatively. 50(16%) complications were identified, including: 25(8%) fistulas, 24(7%) dehiscences, 17(5%) infections. Mid-upper arm circumference (MUAC) ≤12.5 cm was associated with dehiscence after primary lip repair (OR = 28, p = 0.02). Leukocytosis ≥11,500 on pre-operative evaluation was associated with dehiscence (OR = 2.51, p = 0.04) or palate revision fistula (OR = 64, p < 0.001). Surgeons who performed fewer previous-year palate repairs had higher likelihood of palate complications, (OR = 3.03, p = 0.01) although there was no difference in complication rate with years of surgeon experience or duration of surgery.
Conclusions
Multiple patient, surgeon, and perioperative factors are associated with higher rates of complication in a low-resource setting, and are potentially modifiable to reduce complications following cleft surgery.
Background
An estimated five billion people lack access to safe, timely, and effective surgical care, the majority of whom reside in low-income countries (Meara and Greenberg, 2015). Orofacial clefts constitute a major portion of the burden of surgical disease, and treatment for clefts is highly cost-effective relative to other types of surgical and medical care (Debas et al., 2015; Meara and Greenberg, 2015). Nonetheless, gathering data on the effectiveness of such surgical care is challenging given the paucity of infrastructure, care continuity, and resource constraints in these environments (DeCamp, 2007; Furr et al., 2011; De Buys Roessingh et al., 2012; Maine et al., 2012; Sykes, 2014; Shrime et al., 2015). Several rigorous studies attempted to assess complication rates for cleft care in these settings, and unfortunately found strikingly high rates of poor outcome (25–57%) across multiple regions, settings and care delivery types.(Maine et al., 2012; Rossell-Perry et al., 2015; Daniels et al., 2018). Such complications are particularly devastating in low-resource settings, where they can severely affect growth and function, and secondary repair is often inaccessible and more challenging.
Potential drivers of such complications may include patient factors, such as poor nutrition or hygiene, surgeon factors, such as technique employed, meticulousness of tissue handling, or quality and quantity of their training, as well as health system factors influencing timeliness of access or follow-up, among others (Maine et al., 2012; Schönmeyr et al., 2016; Wes et al., 2018). Yet it remains unclear what key factors drive poorer cleft surgery outcomes in low-resource settings, and how these may differ from higher-resource contexts. The purpose of this study was to comprehensively investigate a combination of patient, healthcare system, environmental, and perioperative factors to identify deterministic and potentially modifiable drivers of poor outcomes in cleft lip and palate surgery.
Patients and Methods
Local Cleft Care Context and Patient Selection
The national children's Hospital Velez Paiz suffered an earthquake-related collapse several years ago. Since then, cleft care has been performed by multiple organizations, including various hospital partnerships with US plastic surgery programs and other international organizations. Operation Smile, through a primarily local team of clinicians, has been active for over 27 years in Nicaragua, and seven years ago entered into a formal joint cleft care partnership with the Ministry of Health (MOH). In 2016, Operation Smile established the Grace McGregor B. Comprehensive Cleft Care Center in Managua, providing multi-disciplinary surgical, dental, orthodontic, speech, psychology, and other care year-round, as well as orthognathic and craniofacial surgery programs in conjunction with the MOH. In addition to weekly comprehensive care there are two annual week-long high-volume surgical missions performed with an emphasis on patient outreach to the most rural and impoverished patients in the country. These are staffed predominantly by Nicaraguan clinicians and coordinators with supplementary international volunteers.
This study was implemented during the weeklong missions of 2016–17 in Managua and Esteli. Patients who completed a multi-disciplinary evaluation and were deemed prospective surgical candidates for cleft lip repair or revision, or cleft palate repair or revision, were included. During one of the missions, a two-day pilot pre-operative multi-disciplinary education workshop was implemented utilizing an interactive presentation/panel format combined with live clinical teaching cases (nasopharyngoscopy, surgical cases) that included review of techniques, challenges, and “pearls.”
The study was approved by the Nicaraguan MOH Ethics Board and Operation Smile's Institutional Review Board, and consent to study participation did not impact receiving treatment.
Data Collection
Patients meeting inclusion criteria were prospectively enrolled into an intent-to-treat cohort. Data was obtained via personal interviews by native Spanish speakers with the patient and his/her parent(s). Data points included measurements taken during screening day, laboratory test results, surgeon surveys, and intraoperative reports. Post-operative data was prospectively collected at standard 1-week and 2-month post-operative periods via physical evaluations by credentialed cleft surgeons. In cases where patients did not present, telephone contact was attempted and a standardized complication assessment performed and photos sent electronically. The complications of interest for this study were fistula, dehiscence or infection. Fistula was defined as an abnormal passage between the oral and nasal cavities, and classified as nasolabial, alveolar, hard palate and soft palate fistulas according to the Pittsburgh classification (Smith et al., 2007), including those as small as 1–2 mm. No “intentional” fistulas were excluded.
Patient and health system factors
In addition to patient demographics, temperature, weight, height, and mid-upper arm circumference (MUAC) were measured during screening day. The patient's medical and surgical history was obtained. Nutritional factors regarding infancy nourishment and current diet were documented. Laboratory tests including hemoglobin, hematocrit, leukocytes, albumin and total protein were recorded. Transportation details, access to medical care, socioeconomic and hygiene factors were documented.
Perioperative factors
Perioperative factors pertaining to the surgeon, procedure and patient were documented using operative reports. Each surgeon completed a questionnaire about their training, practice type, and both lifetime and prior year surgical volume in specific cleft cases.
Data Analysis
All data was analyzed using SAS JMP Pro (2018) with regression analyses for uni- and multivariate factors, Student t tests for comparison of continuous variables, and chi-squared or Fisher exact analyses for categorical variables. P-values <0.05 were considered statistically significant. All z-scores were obtained using the WHO Anthro software [2018]. Sensitivity analyses were performed comparing variance of hematologic and surgeon factors to complication rates.
Results
Overall Demographics
Four hundred and eight patients completed enrollment, among which 380 (93%) underwent surgical treatment. Patients ranged from 2 months to 41 years in age, with a mean of 5.8 and median of 3.2 years. Patients resided a median distance of 7.4 km (IQR 0.5-4) and 1.1 h (IQR 0.2-1.3) from the nearest medical help, which most commonly consisted of a health center (74%) staffed only by a general physician and nurse. The average time traveled to reach the surgical site was 8.7 h with a range of 5 min to 96 h of travel time, utilizing public bus (88%), car, boat, horse and walking. The most common political departments of origin were those farthest from the cleft center: the North Caribbean Coast Autonomous Region (RACCN) and the South Caribbean Coast Autonomous Region (RACCS).
The principal surgical procedure was identified as primary cleft lip repair in 124 (33%), cleft lip revision in 84 (22%), primary cleft palate repair in 96 (25%), and cleft palate revision in 82 (22%); 7 patients (2%) had multiple principal procedures. Follow-up assessment was performed in 322 (85%) who were assessed one week post-operatively (304 were physically examined and 18 underwent standardized complication assessment by mobile telephone), and 166 (44%) who were assessed two months post-operatively (99 physically, 67 telephonically). Patients most frequently lost to follow-up were those from the largest distance (RACCN, 29%; RACCS, 21%.)
A total of 50 subjects (16%) suffered one or more complications: 24 (7%) suffered a partial or full dehiscence (Figure 1), 25 (8%) developed a suspected fistula, and 17 (5%) had clinical evidence of postoperative infection (Table 1).

Nine month old female with bilateral cleft lip and palate (preoperatively, a) who presented 5 days postoperatively (b) with acute infection, which went on to dehisce, shown two weeks (c), four weeks (d), two months (e), and six months (f) postoperatively.
Post-Operative Complication Summary.
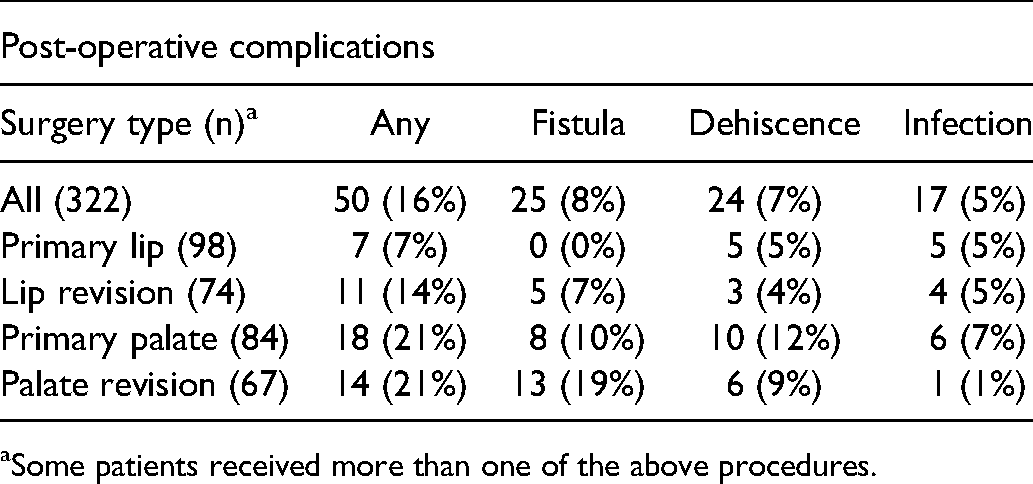
Some patients received more than one of the above procedures.
Patient Factors
Demographic elements
Among 322 patients with complete follow-up data, immunizations were up to date in all patients. Males experienced more frequent complications (31, 62%) than females (19, 38%; p = 0.032). Age at surgery was not associated with post-operative complications. Eight subjects (2%) were syndromic, a factor that was not independently associated with complication.
Anthropometric and nutritional elements
The mean body mass index (BMI) of patients whose surgery was cancelled due to suspected malnourishment following surgical screening was considerably lower (BMI-for-age z-score:−1.37 ± 2.38) compared to those who went on to receive surgery (BMI-for-age z-score: 0.42 ± 2.17, p < 0.001.) The mean BMI of patients with post-operative dehiscence after primary cleft lip repair (BMI-for-age z-score:−1.58 ± 3.93) trended toward being lower than those without dehiscence (BMI-for-age z-score: 0.31 ± 2.25; p = 0.08). BMI was not associated with complications for other surgical types. On a subset analysis of patients undergoing primary cleft lip repair, patients with a mean upper arm circumference ≤12.5 cm had a higher rate of dehiscence (50%) than those with MUAC within normal range >12.5 cm (4%, p = 0.018; Table 2). Participants’ diet consisted mostly of animal- and vegetable-based protein, and cereals. The overall cohort BMI showed a normal distribution. Duration of feeding with maternal milk was shorter (1.88 ± 4.23 months) among those with a complication compared to those without (3.94 ± 5.58, p = 0.031.) This finding was affirmed in a subset analysis of those who developed dehiscence, specifically.
Mid-Upper arm Circumference Relative to Complication Rates Among Patients Undergoing Primary Lip Repair.
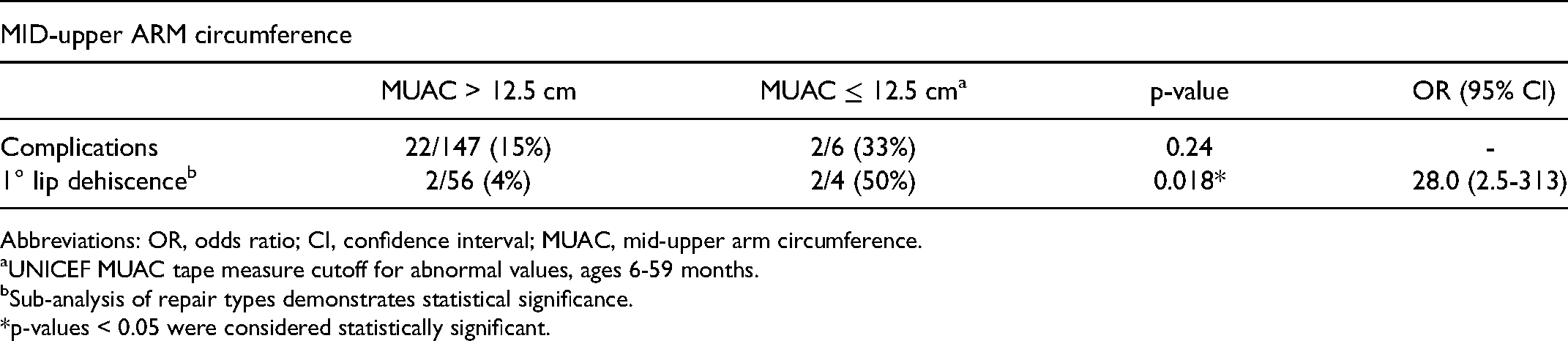
Abbreviations: OR, odds ratio; CI, confidence interval; MUAC, mid-upper arm circumference.
UNICEF MUAC tape measure cutoff for abnormal values, ages 6-59 months.
Sub-analysis of repair types demonstrates statistical significance.
*p-values < 0.05 were considered statistically significant.
Immunologic and hematologic elements
Mean pre-operative white blood cell (WBC) count, measured in 109 cells per liter, was greater among patients undergoing palatal revision with a post-operative complication (12.01 ± 3.23) than those without (8.42 ± 2.33; p = 0.0001; Table 3). This association held on subset analyses of patients undergoing lip or palatal revision who developed a suspected fistula, and all patients when evaluating those who suffered dehiscence. Sensitivity analyses were performed between WBC of 11.0 and 14.0 at intervals of 0.5; a threshold of 11.5 demonstrated greatest sensitivity to cohort differences. A leukocytosis of ≥11.5 was associated with increased incidence of any complication among all repair types, a finding that was demonstrated in subset analysis of dehiscences, and in palate revisions generally (Table 4).
Association of Pre-Preoperative Laboratory Indices and Post-Operative Complication.
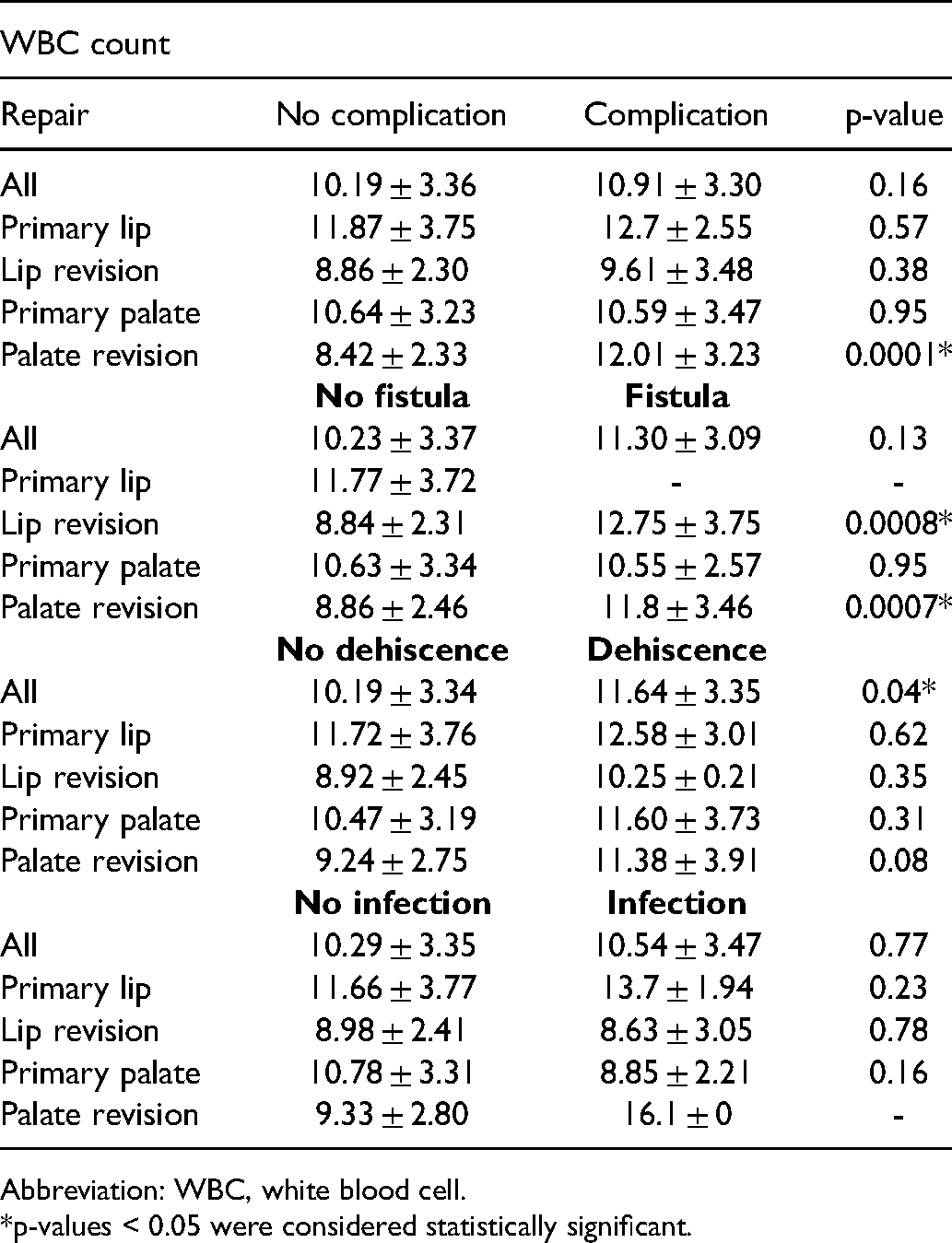
Abbreviation: WBC, white blood cell.
*p-values < 0.05 were considered statistically significant.
Association of Specific Leukocytosis Cutoff with Post-Operative Complication.
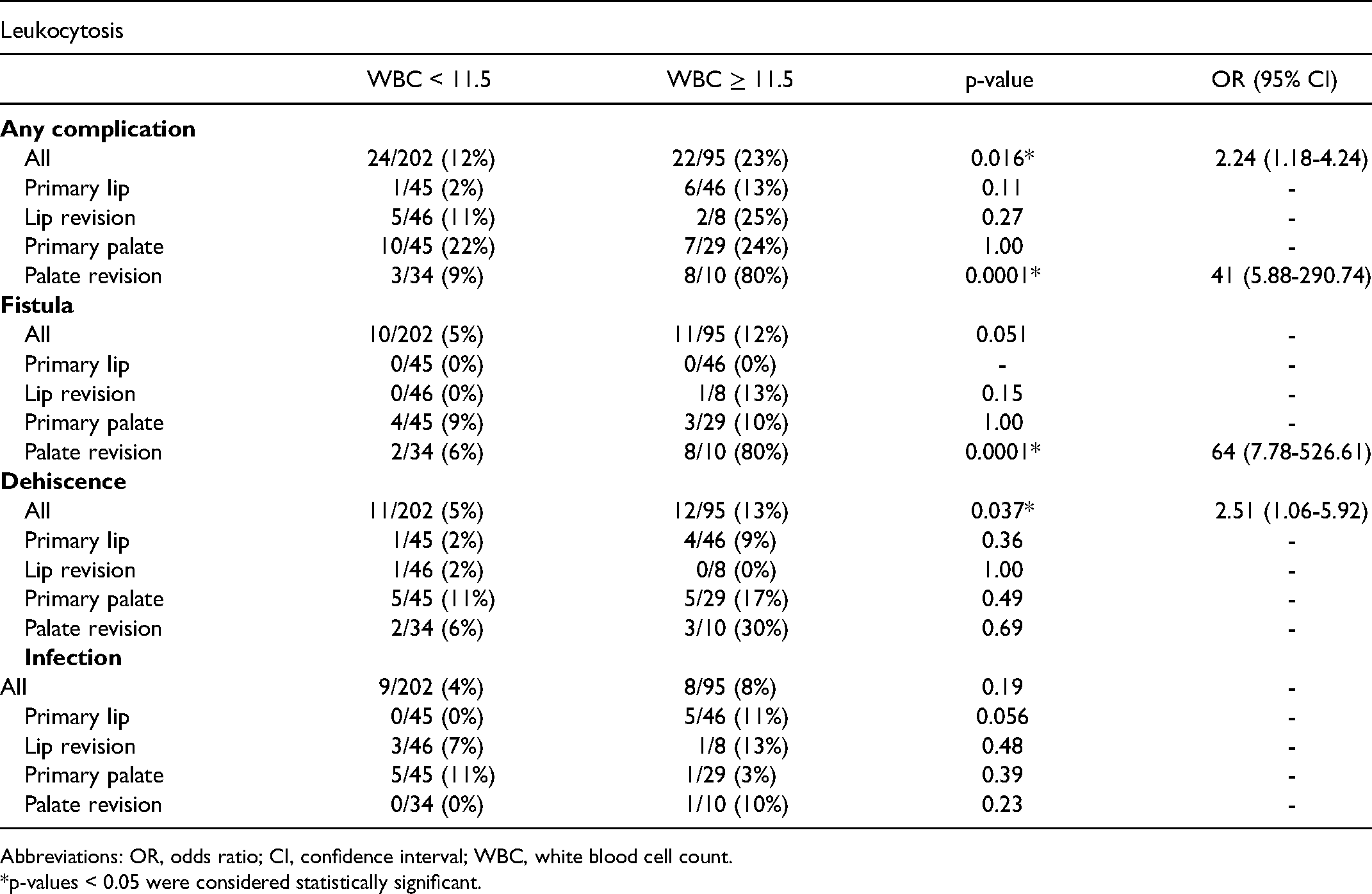
Abbreviations: OR, odds ratio; CI, confidence interval; WBC, white blood cell count.
*p-values < 0.05 were considered statistically significant.
Albumin levels were lower in patients who underwent palate revision and suffered dehiscence (3.89 ± 0.13) compared to those who did not (4.18 ± 0.30, p = 0.023). Albumin levels did not differ between those with and without complications among primary lip and palate repairs. No differences in pre-operative hemoglobin or hematocrit levels were found between those with complications and those without (data not shown).
Social and Health System Factors
Almost half (183, 48%) of patients reported daily home smoke exposure, and 46 (12%) reported a cigarette smoker at home. No association was found between the department of origin of patients, transportation means, people in household, tobacco use at home, exposure to kitchen smoke at home or teethbrushing and complication rates.
Surgeon Factors
Duration of operative time did not differ in cases with complication and those without. Sensitivity analysis revealed that a surgeon's annual volume of palate repair cases (including both primary and secondary) best correlated with risk of complication. Further, this analysis showed that 25 palate repair cases per year was the threshold that best distinguished risk of complication. Individual surgeon prior year palate repair volume of ≤25 cases had a higher rate of overall complications (17% vs 8%, p = 0.013; OR 2.25 [1.20-4.21]), as well as palate repair complications, specifically (34% vs 14%, p = 0.006, OR 3.03 [1.36-6.73]) as compared to surgeons who performed >25 palate repairs in the prior year (Table 5). One of the missions included an intensive 2-day pre-operative surgical education program, and surgeons who attended this program had significantly fewer dehiscence rates of 0% (0/73) compared to those who did not 7% (3/43, p = 0.049). The number of years that a cleft surgeon had been in practice or completion of formal fellowship training did not influence rate of complication (data not shown.)
Surgeon Previous Year Palate Repair Case Load and Complications.

Abbreviations: OR, odds ratio; CI, confidence interval.
Case-Specific Factors
Among lip repairs, bilateral primary lip repairs had higher rates of complication (20% vs 1%, p = 0.0031; OR 16.75), including dehiscence and infection, compared to unilateral repairs. The technique of repair did not influence complication rates. Among primary palate repairs, the rate of complication did not vary by Veau classification. There was a higher rate of infection (4/18, 22%) in subjects who underwent a two-flap pushback repair versus those that did not (2/56, 4%; p = 0.028, OR 7.7). Complication rates did not otherwise vary among hard palate repair types (eg Von Langenbeck, two flaps without pushback, limited incision) or soft palate repair types (eg intravelar veloplasty, Furlow z-plasty, lateral relaxing incision). Among palate revisions, when a fistula was present pre-operatively, neither its presence nor its location—most commonly anterior palate/incisive foramen (50%), followed by central hard palate (24%)—affected the rate of post-operative complication.
Postoperative Case Detection
Among 95 patients who underwent physical examination at both 1 week and 2 months postoperatively, only 7 (54%) of 13 subjects with verified complication at 2 months had suspected complication at 1 week. Evaluation at 1 week postoperatively had 54% sensitivity and 95% specificity; yielding a positive predictive value of 64% and a negative predictive value of 93% in our sample.
Discussion
Occurrence and risks of major perioperative complications such as airway compromise, intra-operative hemorrhage, and mortality have well-established in cleft surgery literature (Desalu et al., 2010; Kulkarni et al., 2013; Zhang et al., 2014). Attention to such complications is critical, particularly in low-resource settings. Fortunately, life-threatening complications are rare and decreasing (Conway et al., 1966), in large part due to the establishment of safety guidelines (Politis et al., 2011; Schneider et al., 2011). However, far less data focus on complications such as velopharyngeal insufficiency, growth problems, dehiscence, fistulas, and infection, that while not acutely perioperative, often lead to intractable oral and speech dysfunction, invoke considerable patient suffering, and whose resolution often exceeds the resources and ability of many surgical teams. Retrospectively assessing complications is challenging in low-resource settings given the paucity of records and patient follow-up, likely underestimating complication incidence and limiting insight into potentially modifiable risk factors (Bruny et al., 2013; ACS NSQIP 2018; Ellis et al., 2018).
This study prospectively identified that 16% of cleft cases were complicated by fistula formation, dehiscence and/or infection in this low-resource setting that represented a hybrid of center-based and mission-based care. The overall fistula rate was 8%; and for palatal repairs or revisions was 14%. This is lower than other reported mission-based rates of up to 33% (Morioka et al., 2007; Abdurrazaq et al., 2013; Rossell-Perry et al., 2015; Adesina et al., 2016), perhaps due to the hybrid mission-cleft care center model in Nicaragua. Mounting evidence suggests better outcomes in center-based programs, which emphasize strengthening local resources (Lambadusuriya et al., 1988; Maine et al., 2012; Schönmeyr et al., 2016; Daniels et al., 2018). Nonetheless, this complication rate is a magnitude greater than those in high-income countries, and represents considerable ongoing burden of disease and opportunity for improvement.
Patient Factors
Neither older age, nor syndromic status, were associated with increased risk of post-operative complication, consistent with other studies (Emory et al., 1997; Landheer et al., 2010; Reddy et al., 2018). Interestingly, more males than females encountered complications, for unclear reasons. Other studies have found that male cleft patients preferentially surmount barriers to care in low-resource settings (Swanson et al., 2017). Thus, this cohort could present for post-operative assessment at a lower threshold of parent concern, as a form of observation bias. Vaccination programs have been very successful in many low-resource countries (Tungotyo et al., 2017) all patient immunizations were up to date in our cohort (PAHO, 2018).
The anthropometric data obtained showed a lower mean BMI-for-age z-score in those whose surgery was cancelled due to suspected malnourishment, indicating a proper filtering of severely malnourished patients during surgical screening. Of those who underwent surgery, specifically primary lip repair, lower trending mean BMI-for-age z-scores were found in cases complicated by dehiscence. MUAC in the malnourishment range (≤12.5 cm), was associated with increased risk of dehiscence after primary cleft lip repair. Shorter duration of maternal milk intake in infancy was also associated with complication, especially dehiscence. These findings demonstrate that although current screening mechanisms are appropriately filtering severely malnourished patients, some borderline-malnourished patients constitute a significant portion of lip dehiscence patients. Adding MUAC measurement during surgical screening and more stringent guidelines based on BMI-for-age could potentially decrease lip dehiscence rates.
Mean white blood cell (WBC) count was significantly higher in those who suffered a complication after palatal revision, irrespective of normal physical examination. A detailed sensitivity analysis showed that an asymptomatic leukocytosis ≥11.5 × 109/L was associated with complication in all repair types (OR = 2.24) and more strongly after palate revision (OR = 41), specifically fistula (Table 4). Other studies corroborate an association between asymptomatic pre-operative leukocytosis >11 as defined by SIRS criteria (Lindner et al., 2016) and complication (Moghadamyeghaneh et al., 2015; Mahmood et al., 2017). Additionally, albumin levels were lower in those who suffered dehiscence after palate revision than those who did not (p = 0.02). Protein deficiency and active throat infections have been shown to adversely affect healing of tissues in the literature (Murthy, 2014). Although leukocyte concentrations of up to 14 × 109/L can be normal in pediatric patients, these findings suggest the utility of 11.5 × 109/L as a threshold for considering deferment of surgery in all patients, regardless of age, as well as those with hypoalbuminemia.
Surgeon Factors
Multiple studies have shown the surgeon as a contributing factor to complications (Emory et al., 1997; Landheer et al., 2010; Russell et al., 2011; Reddy et al., 2018), but few parse out attributable surgeon characteristics. In this study, prior-year palate repair surgical volume ≤25 cases was associated with complication when compared to a greater prior-year palate repair surgical volume (OR = 2.25), regardless of fellowship status or years of practice. This highlights the importance of ensuring a certain level of continual practice in cleft surgery, which may be particularly applicable in low-resource settings given the higher apparent overall complication risks. Pairing higher cleft palate-volume surgeons with lower volume surgeons in cases, as well as graduated-autonomy training methods may be useful in such settings to increase safety, mitigate complications and facilitate eventual autonomy (Yao et al., 2016).
Surgeons who attended a 2-day pilot pre-operative surgical education program that utilized simulators and focused on technique review, had fewer dehiscence rates than those who did not attend. Regardless of workshop availability, recent innovations such as cleft palate simulators may enable surgeons to maintain a certain level of cleft palate repair technical proficiency even in the absence of fewer recent cases, or serve as a primer (Vadodaria et al., 2007; Nagy and Mommaerts, 2009; Cheng et al., 2018).
Case-Specific Factors
Consistent with the literature (Murthy, 2014), bilateral cleft lip repairs had higher complication rates than unilateral lip repairs, specifically dehiscence and infection (p = 0.003). Four of the five patients who suffered an infection in bilateral cleft lip repairs did not receive post-operative antibiotics, suggesting the potential benefit of a post-operative antibiotic regimen after bilateral lip repair. Our findings did not demonstrate a difference between Veau cleft classification or surgical repair technique regarding complications, which is corroborated by other studies (Emory et al., 1997; Landheer et al., 2010; Murthy, 2014; Reddy et al., 2018). Wider clefts have been shown to be associated with higher fistula rates (Landheer et al., 2010), which we could not confirm in our study due to lack of cleft width data.
Limitations
The generalizability of these findings to either center-based or mission-based cleft care may be limited given the surgical mission–cleft care center hybrid model on which this data is based. In-person follow-up attendance at the cleft center was 80% at one week, but decreased to 26% at two months, reflecting the many barriers patients face in follow-up care. The use of a standardized complication assessment by mobile telephone has been shown to be useful in rural settings (Wes et al., 2018), and increased our follow-up volume considerably although potentially with reduction in assessment precision. Thus, the study may underestimate overall complications. Interestingly, some suspected complications at 1 week postoperatively may have self-resolved, such as infection. Likewise, some fistulas and dehiscence are not yet apparent at 1 week that become visible at 2 months, as affirmed by the modest sensitivity shown by the 1 week post-op assessment. Despite these limitations, we would not expect them to influence the factors, which the study identified as associated with developing complications. Finally, we acknowledge that other important long term complications, including velopharyngeal insufficiency or restricted maxillary growth, were not included in this study.
Conclusion
Multiple perioperative factors seem to predict subacute complication in cleft surgery in this setting, including a MUAC <12.5 cm, an elevated WBC count of ≥11.5, hypoalbuminemia, as well as a surgeon with low prior-year cleft palate repair surgical volume. Complications such as fistula and dehiscence are likely to be reduced by incorporating these criteria into patient assessment, as well as distributing cleft cases among surgeons with high volume cleft practice or pursuing adjuncts such as refresher workshops or simulator use.