
Abstract
Objective
To evaluate socioeconomic and geospatial factors at a cleft care center in the Southern United States and assess their impact on outcomes in patients with cleft lip and/or palate (CLP).
Design
Retrospective chart review of patients with CLP, with stratification by neighborhood disadvantage using the University of Wisconsin's Area Deprivation Index (ADI). Univariate analyses compared quartiles.
Setting
A cleft care center in the Southern United States.
Patients, Participants
Inclusion criteria included children with CLP born between 2011 and 2022 who received the entirety of their care at the institution. Exclusion criteria were patients without CLP, those born before 2011, or those who did not complete care at the institution.
Interventions
No interventions were introduced.
Main Outcome Measure(s)
Associations between ADI quartiles and sociodemographic factors, appointment adherence, clinic presentation, hypernasality, and speech surgery incidence.
Results
Significant associations were identified between the most disadvantaged quartile and others for ethnicity (P < .001), primary language (P = .013), insurance status (P = .001), and household income (P < .001). The most disadvantaged quartile had fewer cancellations (P = .002) and presented earlier (P = .050), but had higher rates of hypernasality (P = .005) and speech surgery (P = .046).
Conclusions
Patients in the most disadvantaged quartile demonstrated strong adherence despite socioeconomic and linguistic barriers but had worse speech outcomes. Findings highlight opportunities to address linguistic and cultural barriers to improve cleft care.
Keywords
Background
Care for CLP is complex and requires a multidisciplinary approach spanning from infancy through adolescence, including surgical interventions, speech therapy, orthodontics, and psychosocial support.1,2 The long-term nature of this care, coupled with the need for consistent follow-up, places significant demands on both patients and their families. For example, early interventions such as nasoalveolar molding (NAM) improve functional, aesthetic, and psychological outcomes for patients with CLP.3–9 However, NAM imposes a high burden of care due to the physical, financial, and psychological burden of distance traveled, treatment duration, and the number of appointments frequently requiring weekly or biweekly visits for up to 5 months.6,10 Figure 1 illustrates a sample timeline showing the various appointments involved in cleft lip and palate care. Therefore, these burdens of care for patients and caregivers could predispose patients to not receiving the highest standard of care, a problem particularly pertinent to the Southern United States due to the low proportion of patients living within a 1-h drive to a certified cleft lip care center. 11
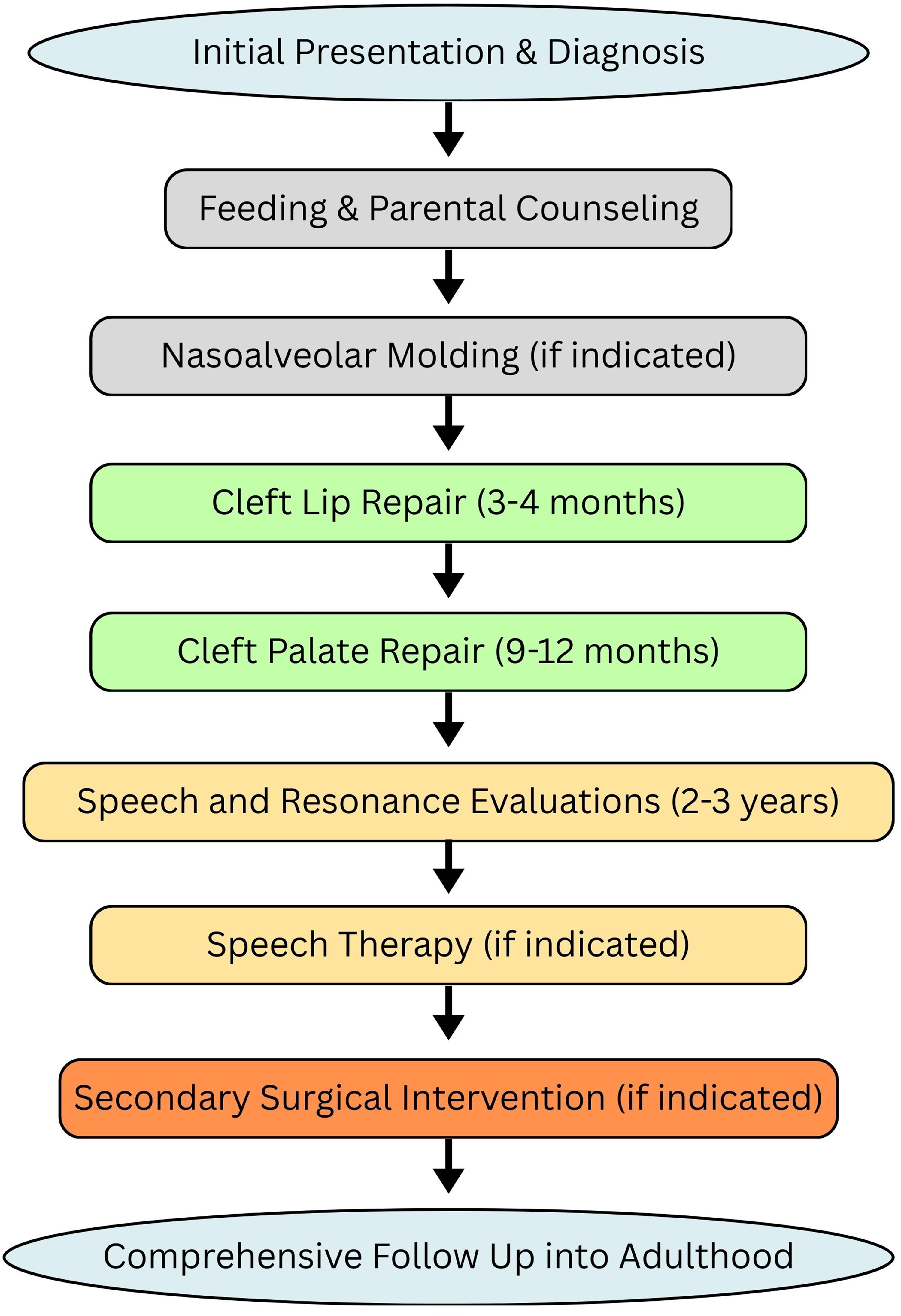
Timeline of surgical treatment of cleft lip and palate by age.
Socioeconomic factors can profoundly influence health outcomes, particularly in chronic conditions requiring ongoing care. 12 Neighborhood disadvantage, defined by factors such as poverty, limited access to healthcare, lower educational attainment, and reduced social mobility, is associated with worse health outcomes. Belonging to a more vulnerable socioeconomic group was associated with language and speech concerns as well as developmental delay. 13 However, these disparities may also reflect factors outside of purely socioeconomic status, such as cultural and linguistic discordance. Differences between geographical regions, such as 1-h access to cleft lip care, were lowest in the Southern United States and highest in the Northeast. 11 In the Northeast, a shorter distance to a care center and a higher mean income predicted both incidence of NAM and prenatal plastic surgery evaluation. 14 Similarly, patients with lower socioeconomic status were shown to be more susceptible to disparities in weight gain from 4 to 8 weeks of life and failure to thrive. 15 Therefore, these previous studies have documented the effects of neighborhood disadvantage and socioeconomic status on CLP, influencing access to care, adherence to treatment plans, and ultimately clinical outcomes.
Geospatial analysis allows for precise measurement of neighborhood disadvantages using tools such as the University of Wisconsin's Area of Deprivation Index (ADI), 16 which assesses socioeconomic status based on a 9-digit ZIP code level. This level of granularity offers a unique opportunity to examine the relationship between neighborhood disadvantages and health outcomes in specific patient populations, such as those with CLP. Prior studies have examined neighborhood deprivation and speech outcomes in patients with cleft palate, but important gaps remain. 13 Varagur et al. evaluated ADI in the setting of a multi-institutional cohort and demonstrated associations with speech outcomes and secondary interventions. Our study, however, focuses on a single center in the Southern United States, the region of the United States with the least access to cleft care. 11
This study aimed to explore the relationship between neighborhood disadvantage, as measured by the ADI, and clinical outcomes in patients with CLP in the Southern United States. By analyzing socioeconomic and geospatial data alongside clinical interventions and outcomes, the authors sought to determine whether patients from more disadvantaged neighborhoods experience different care trajectories and health outcomes compared to their less disadvantaged peers. Understanding these relationships is crucial for identifying potential areas for intervention and ensuring equitable access to care for all patients with CLP.
Methods
Patients
We conducted a single-center retrospective study at a tertiary children's hospital that analyzed patients with CLP records. Inclusion criteria for patients included all patient records of children who received the entirety of their CLP care at the host institution, born between 2011 and 2022. Patients who began their care at a different facility and those who did not complete their care at the institution were excluded. This protocol was reviewed and approved by the institutional review board of the institution. No additional exclusions were applied for syndromic diagnoses or other medical comorbidities.
Neighborhood Disadvantage
Neighborhood disadvantage and socioeconomic disparity were measured using the University of Wisconsin's ADI scores. 16 Figure 2 presents a map of Texas categorized by national ADI quartiles. Each patient was scored based on their 9-digit zip code and subsequently received a number ranging from 1 to 100. Patients with a score of 1 would correspond to the lowest deprivation score and, therefore, the least disadvantaged population. Similarly, patients with a score of 100 would correspond to the highest deprivation score and, therefore, the most disadvantaged population. These scores were calculated based on the national percentiles of disadvantages (ADI). After patients were assigned a score of 1-100, they were further grouped into quartiles. Patients with national ADI scores of 1-25 were in the first quartile, 26-50 in the second quartile, 51-75 in the third quartile, and 76-100 in the last quartile. Neighborhood disadvantage was assigned using the most recent address documented in the patients’ electronic health record at the time of data extraction.
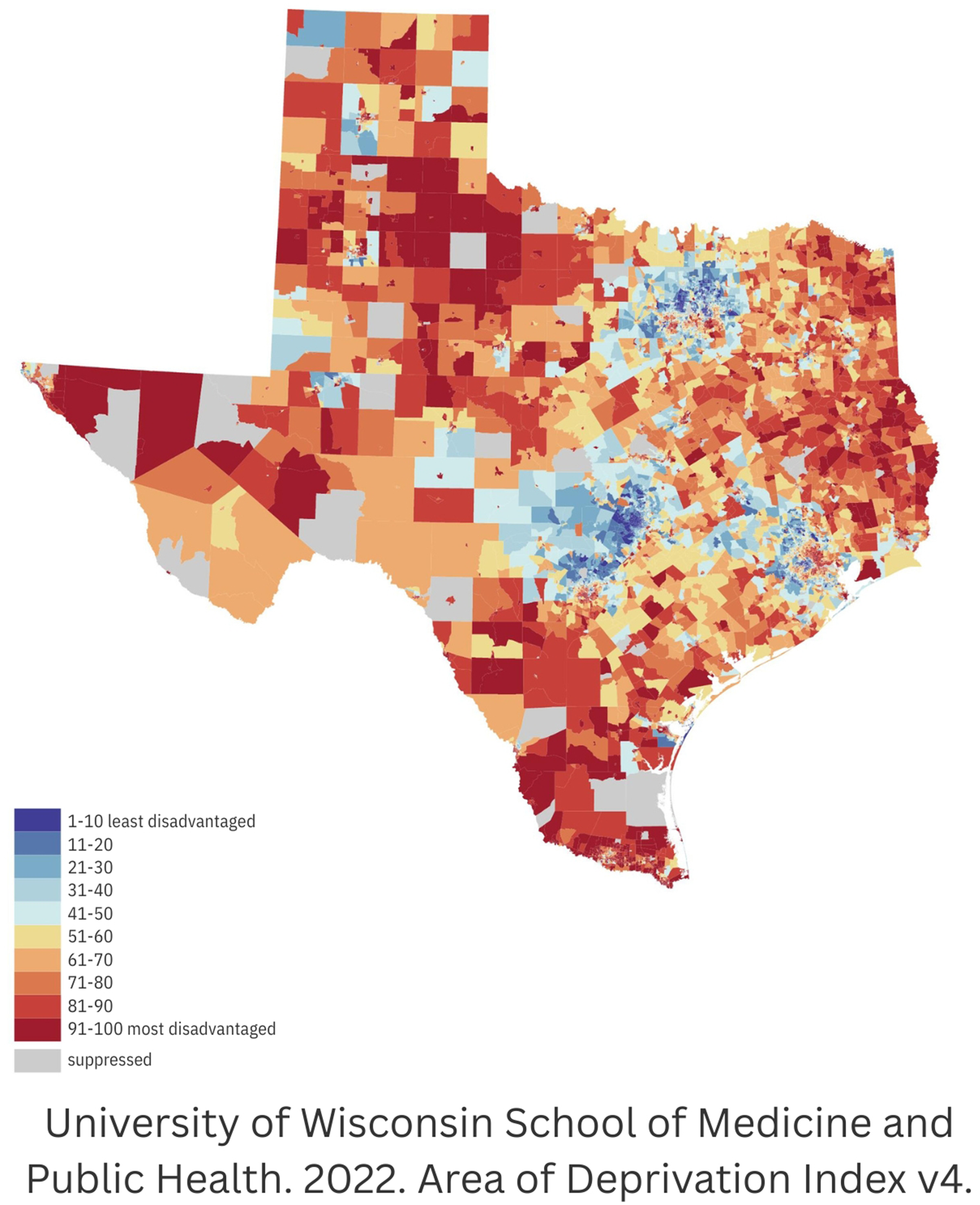
Texas ADI national rankings 2022.
Clinical Data:
Clinical data were obtained from patients’ electronic medical records (EMR) and stored in the Research Electronic Data Capture (RedCap) database. Data on patient birth history, CLP phenotype, and sociodemographic factors were collected for all the patients. Surgical records and follow-up data, including the presence of surgical complications, were recorded. The speech outcomes were also recorded. Hypernasality was measured using the Cleft Audit Protocol for Speech-Augmented-Americleft Modification (CAPS-A-AM) rating system based on a 5-point scale. In this system, 0 represented no degree of hypernasality or “normal,” while 1-4 indicated varying degrees of hypernasality. This system includes both a Spanish and English version. Inter-rater and intra-rater reliability were not formally assessed in this study. The CAPS-A-AM standardized data collection was used to mitigate potential measurement variability.
Statistical Analysis:
Data analysis was performed using Excel and the R-Studio software. Two-tailed unpaired t-tests were performed for continuous variables to determine the statistical significance of the observed findings. Categorical variables were analyzed using the chi-square test. The threshold for statistical significance was set at P < .05 for all analyses.
Results
The demographic data by ADI quartiles are shown in Table 1. A total of 406 patients met the inclusion criteria, with 24% in the most deprived quartile. The analysis revealed several statistically significant differences between the most deprived quartile and all other quartiles, particularly in terms of the primary language, insurance status, and mean household income.
Demographic Characteristics by Area Deprivation Index (ADI) Quartile.
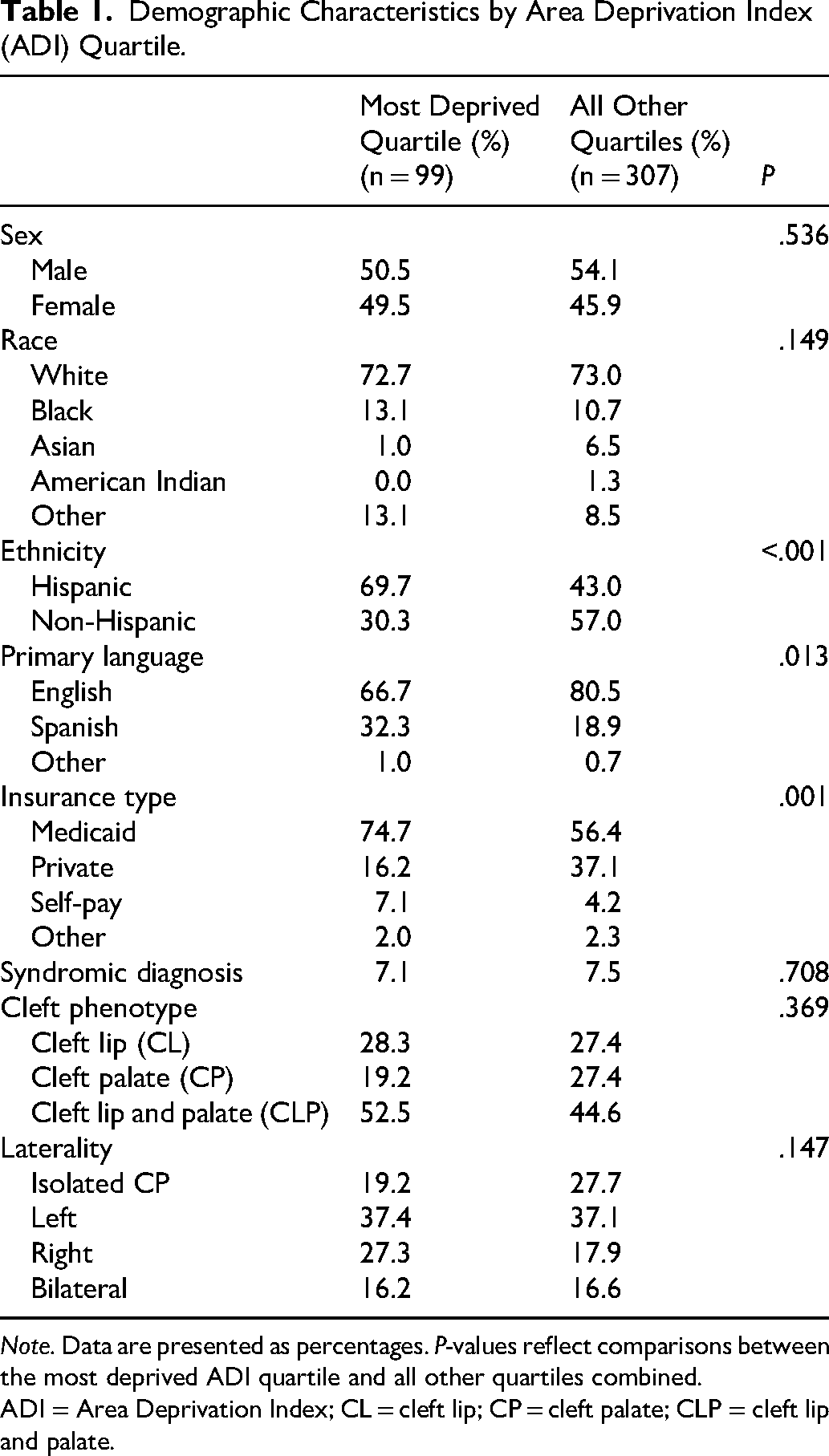
Note. Data are presented as percentages. P-values reflect comparisons between the most deprived ADI quartile and all other quartiles combined.
ADI = Area Deprivation Index; CL = cleft lip; CP = cleft palate; CLP = cleft lip and palate.
Primary language differed significantly by ADI quartile, as shown in Figure 3. In the most deprived quartile, 66.7% of patients primarily spoke English, compared with 80.5% in all other quartiles (P = .013). Conversely, Spanish was the primary language for 32.3% of the patients in the most deprived quartile versus 18.9% in all other quartiles.
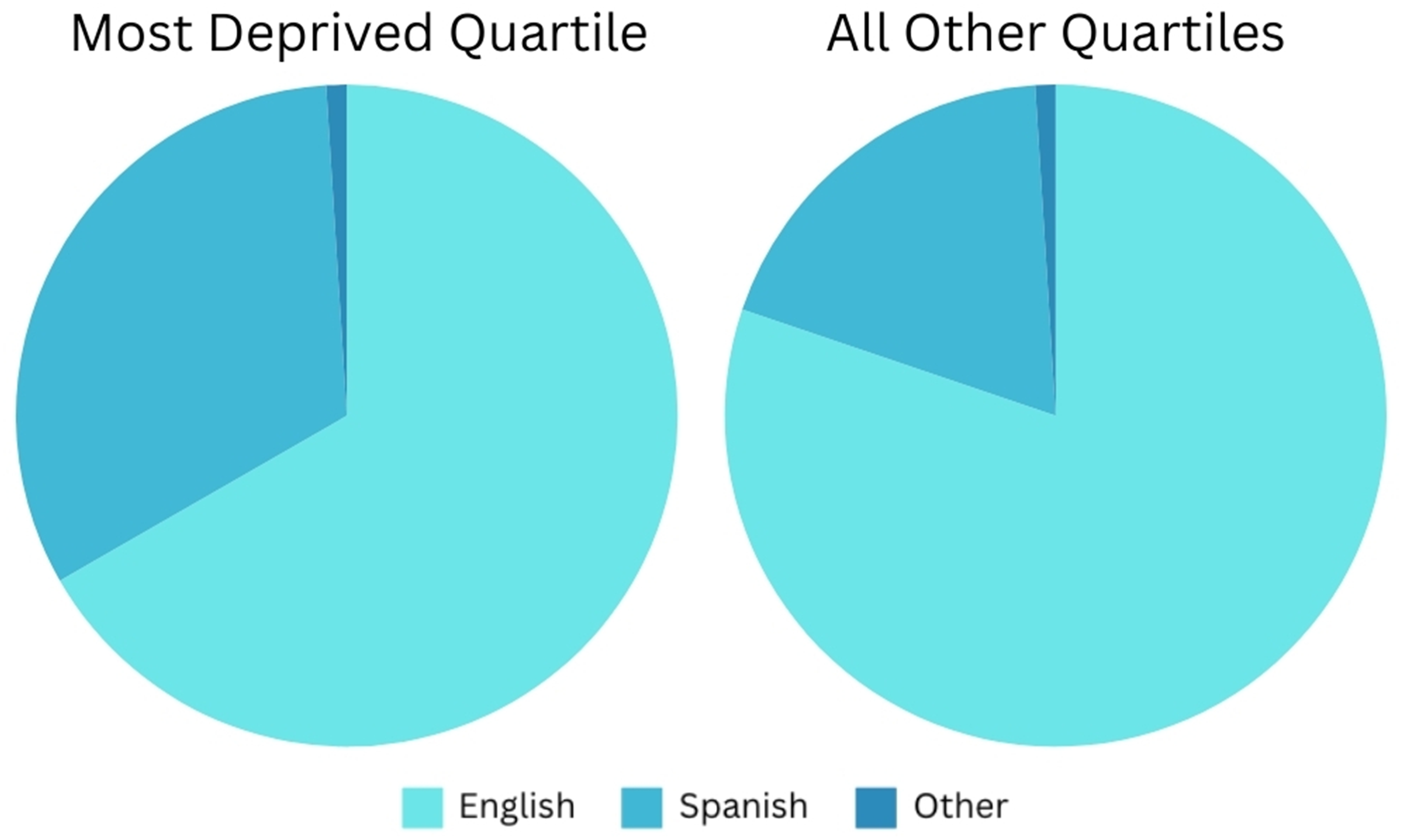
Primary language by ADI quartile.
The insurance status also differed significantly between the most deprived quartile and all other quartiles, as shown in Figure 4 (P = .001). In the most deprived quartile, the distribution was as follows: 74.7% Medicaid, 16.2% private insurance, 7.1% self-pay, and 2.0% others. For all other quartiles, the breakdown was 56.4% Medicaid, 37.1% private insurance, 4.2% self-pay, and 2.3% others.
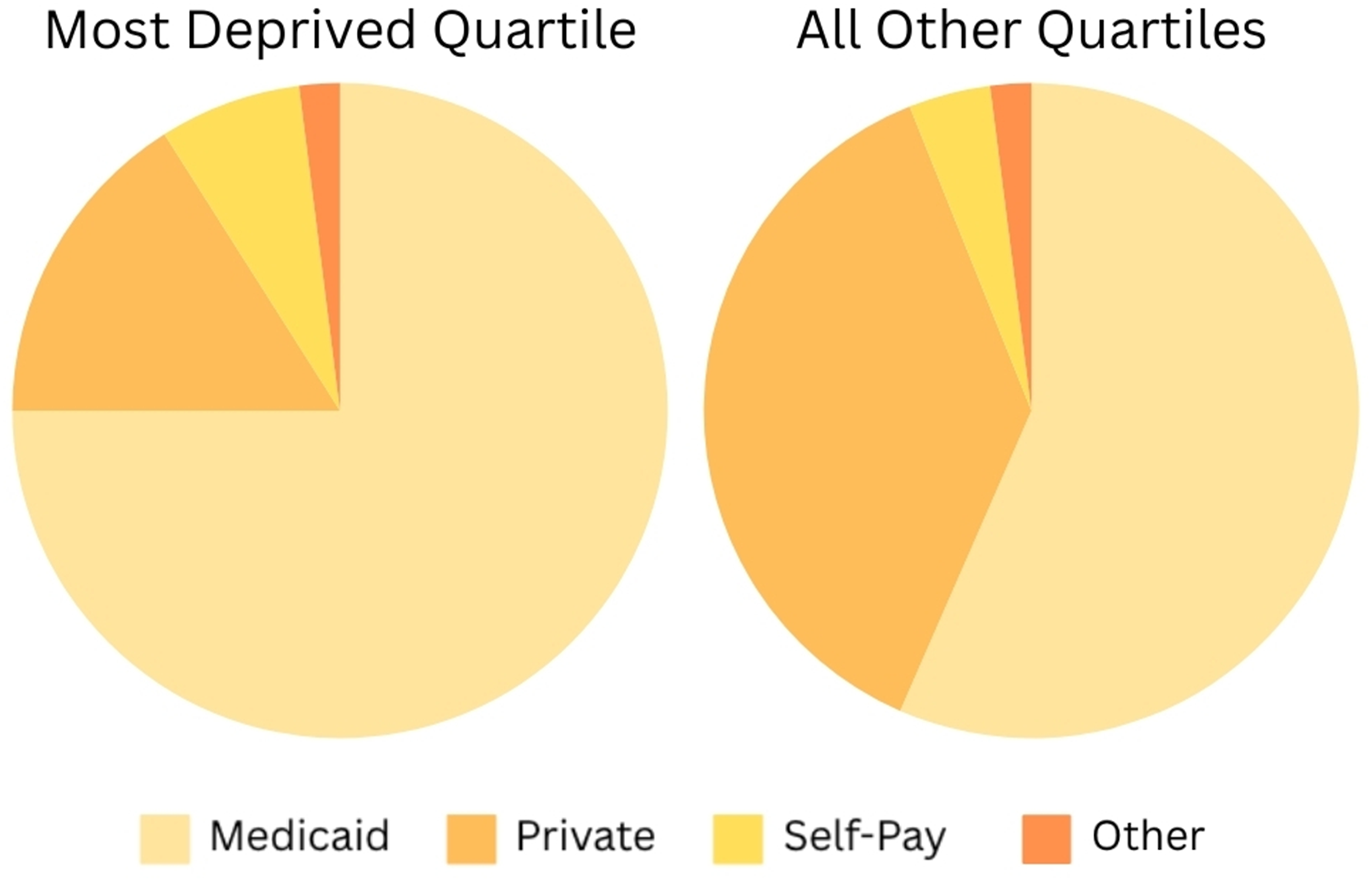
Insurance status by ADI quartile.
The disparity in the mean household income was also statistically significant (P < .001). Patients in the most deprived quartile had a mean household income of $38,615.5 ± $11,139.1, compared with $62,778.1 ± $23,720.1, for all other quartiles.
Table 2 depicts the clinical information and outcomes according to the ADI quartile. There were no statistically significant differences between the groups in several key areas, including follow-up to age 5 years, quantity of no-shows, distance to care center, age at primary repair, age at speech surgery, or age at initial clinical presentation. The most deprived quartile had statistically significantly fewer cancellations (P = .002) and presented to the clinic earlier (23.5 ± 28.9 days) compared to all other quartiles (30.1 ± 48.6 days, P = .050). Despite these seemingly favorable factors, the most deprived quartile still experienced a greater percentage of hypernasality (P = .005) and a higher incidence of speech surgery (P = .046).
Clinical Characteristics by Area Deprivation Index (ADI) Quartile.
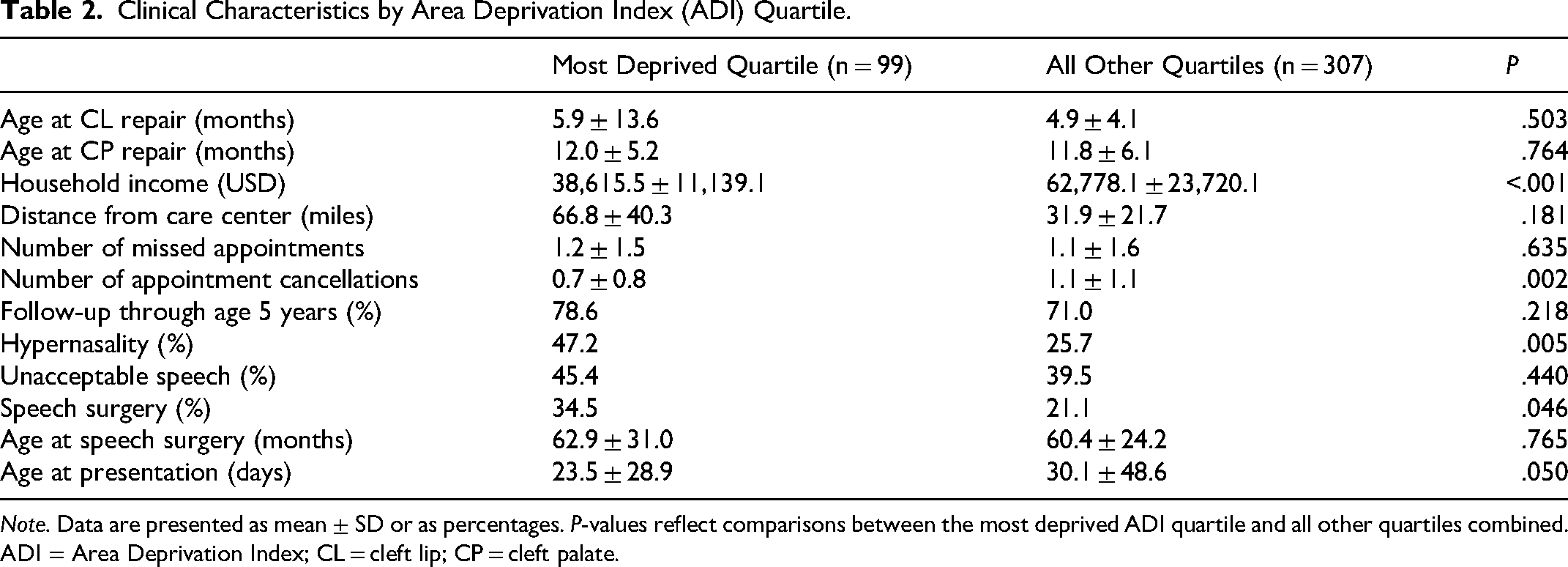
Note. Data are presented as mean ± SD or as percentages. P-values reflect comparisons between the most deprived ADI quartile and all other quartiles combined.
ADI = Area Deprivation Index; CL = cleft lip; CP = cleft palate.
Discussion
The findings of the study corroborate existing evidence regarding the increased incidence of adverse speech-related outcomes in the most socioeconomically deprived population, while observing no significant difference in follow-up rates across ADI quartiles. 13 Our specific outcome disparities are the higher prevalence of hypernasality and increased rates of secondary speech surgery observed in the most deprived ADI quartile, despite similar treatment adherence. The timely initiation of CLP care is crucial, encompassing various tests, potential NAM device treatment, and optimal surgical planning. Interestingly, despite earlier clinical presentation, fewer cancellations, and equivalent follow-up visit rates, patients in the most deprived ADI quartile still experienced a higher incidence of speech surgery and significantly greater hypernasality, suggesting that earlier presentation, fewer cancellations, and adequate follow-up may not be sufficient to prevent adverse outcomes. This apparent disconnect between adherence to care and outcomes suggests that care access alone may not fully account for disparities, but instead, other mediators, including socioeconomic factors and linguistic discordance, that may underlie the disparity.
Despite socioeconomic and linguistic barriers, patients from the most disadvantaged quartile demonstrated comparable adherence to care. They also experienced worse speech outcomes and a higher incidence of secondary speech surgery. This suggests that the multidisciplinary approach at our specific institution may limit traditional access-related disparities. This highlights the importance of socioeconomic barriers unrelated to access to care alone that may affect outcomes. These other factors could include speech therapy intensity, continuity of care outside of our institution, and constraints on the caregivers of patients. Our findings suggest that addressing disparities in cleft care requires not only improving access to multidisciplinary services but also targeting other areas of socioeconomic disparity. Transportation to appointments and adhering to care alone may be insufficient to equalize speech outcomes across socioeconomic backgrounds.
These patients were also more likely to speak Spanish as their primary language and were enrolled in Medicaid insurance. The study further confirmed significant disparities in the mean household income among the most deprived quartiles. Lower household income in the most deprived quartile can exacerbate the challenges faced by families of patients with CLP. The management of CLP often requires numerous appointments, surgeries, and follow-ups over several years, which can be particularly burdensome for those of lower socioeconomic status. Higher hypernasality rates were observed in the most deprived quartiles. Other studies have confirmed these findings regarding worse language outcomes in patients with greater socioeconomic burden, which has also been associated with worse speech outcomes and a greater incidence of developmental delay.13,17 The significantly lower proportion of English as a primary language in the most deprived quartile may be a contributing factor to poor patient outcomes. A systematic review highlighted that language barriers in healthcare lead to higher rates of miscommunication between providers and patients, decreasing satisfaction, quality of care, and patient safety. 18 Studies consistently demonstrate that professional interpreters improve communication, patient satisfaction, and understanding. For Hispanic Spanish-speaking patients, communicating with the care team in their primary language was found to be more important than for English-speaking patients. 19 Consequently, patients in the most deprived quartiles facing language barriers are at greater risk of misunderstanding care instructions, potentially resulting in poorer adherence to prescribed care and worse patient outcomes. Current and future immigration policies may intensify the current disparities by limiting healthcare access for non-English speaking or undocumented patients, especially in the Southern United States.
Because our study found a greater percentage of Spanish-speaking patients in the most deprived quartile compared to all other quartiles, it is possible that the outcome disparities related to speech may reflect a linguistic mismatch between patients and therapy protocols. Importantly, the phonemics and pronunciation between English and Spanish could potentially complicate standardized speech assessments, leading to an overestimation of speech impairment in Spanish-speaking patients, even in the setting of both bilingual rating systems. Previous studies have demonstrated that listener language and dialect influence the perceptive rating of hypernasality.20,21 In this retrospective study, the dominant language of the speech language pathologists was not consistently available, but the institution uses speech language pathologists who speak the patient's native language. However, the hypernasality alone may not fully capture the complexity of a speech evaluation, especially in a Spanish-speaking population.
Medicaid reliance is another variable that likely affects patient outcomes. Research has shown that children in hospitals with higher Medicaid reimbursement reliance are more likely to experience adverse outcomes compared to children in other hospitals. 22 Moreover, Medicaid pediatric inpatients experience adverse effects more frequently than their privately insured counterparts. Medicaid patients also face a 3.3 times lower likelihood of successfully scheduling specialty appointments than privately insured individuals. 23 This barrier to care disproportionately affects the most deprived quartile and may additionally reduce access to specialized services even among those patients with high adherence to care.
Ancillary cleft care services, such as infant orthopedics and NAM, are important components of cleft care that are likely affected by socioeconomic factors. NAM requires a significant amount of both time and appointments for families, which may disproportionately burden those with pre-existing socioeconomic hardship. Our study focused primarily on speech outcomes in cleft care stratified across socioeconomic quartiles, but we recognize the importance of completion and access to presurgical treatments as well, and their potential impact on speech development. We recommend future investigations into NAM implementation and completion across socioeconomic backgrounds to provide a more comprehensive understanding of when we can target these disparities earliest.
Previous studies reported associations between neighborhood deprivation and disparities in speech outcomes and interventions in other geographical areas. 12 Our study's findings are consistent with this finding, but offer a different perspective, being in the Southern United States serving a high population of Spanish-speaking families. The large population of Spanish-speaking patients in the most deprived ADI quartile might warrant different approaches to patient care with community-based support tailored to their specific needs. Given that the most deprived quartile was largely comprised of Spanish-speaking patients on Medicaid with speech and language concerns, targeted initiatives to mitigate these barriers could include telehealth appointments for speech therapy with Spanish-speaking providers, including Spanish-speaking speech-language specialists. It is possible that language factors contributed to the observed differences in speech outcomes. However, because language and neighborhood deprivation were closely related in this study, we believe this reflects structural inequities. Therefore, our study exemplifies that both language discordance and socioeconomic disadvantage act together to affect outcome disparities. Additionally, recognizing the impact of not only socioeconomic factors but also language barriers in cleft lip and palate outcomes is crucial. Enhanced Medicaid reimbursement policies are also recommended to help bridge the gap in outcomes across quartiles so that patients have access to specialized care. Similarly, because the Southern United States historically has the least access to cleft lip care, transportation assistance might be beneficial for low-income families, especially in the southern states. Community outreach programs may also benefit patients by providing opportunities to learn about cleft lip and palate alongside their peers and connecting with other community members experiencing similar circumstances. Previous research has identified the Southern United States as the geographic area with the least access to cleft care within a 1-h radius. 11 Therefore, studies such as these are crucial in determining factors influencing care and outcomes, specifically in this region. The data provide insight into the demographics and challenges faced by those seeking care for cleft lip and palate in the Southern United States. In summary, our findings highlight several modifiable factors such as expansion of telehealth appointments, increased investment in Spanish-speaker providers and speech language pathologists, and increased Medicaid pediatric specialty coverage to reduce disparity in cleft lip and palate care in the Southern United States. Further, our study highlights the importance of considering regional differences when interpreting socioeconomic effects on cleft outcomes.
Many of the demographic and socioeconomic factors in our results, such as household income, are components of the ADI, and therefore, we expected these to differ across quartiles. We included these variables to emphasize specific components represented by the ADI. Coordinating care clinical visits and integrating social work may have contributed to reducing disparities in access and adherence to care. Importantly, despite these differences in socioeconomic variables, many of the care trajectories, including timing to presentation and clinical adherence, were similar across quartiles. Therefore, while access to surgical and clinic care may be equitable, disparities may still emerge, as shown in our speech outcomes. These findings highlight the strengths and limitations of multidisciplinary cleft care models and the necessity to further investigate factors other than simply access to care when addressing differences in socioeconomic outcomes.
The increase we observed in unsatisfactory speech outcomes and speech surgery in the most deprived quartile is likely multifactorial and cannot be attributed to language barriers alone. While language discordance certainly can complicate speech assessment and therapy, it is unlikely to be the only factor determining speech outcomes. Other factors, such as greater cleft severity, variability in cleft phenotype, and presence of comorbid conditions or syndromic conditions, likely contribute to the observed outcomes. It is also possible that continuity and availability of speech services outside of our multidisciplinary care team may further compound undesired speech outcomes in the most deprived quartile, despite comparable engagement with surgical care. Therefore, our findings suggest that neighborhood deprivation may exert a greater influence through cumulative effects of disease severity, co-morbidity burden, and longitudinal speech therapy rather than through initial presentation and surgery follow-up.
While regional and local initiatives are important, national cleft care societies and organizations have a critical role to play as well. Their function serves to convert relevant research findings into system-wide improvements by offering guidelines for practice. This could potentially include expectations for language access and speech outcome reporting. Further, national societies can support multicenter registries and databases that allow outcomes to be compared across regions to best identify gaps in care. These organizations also play a crucial role in advocacy for policy and reimbursement reform to further lessen any potential burdens on patients in need of this care. This includes access to high-quality speech therapy, telehealth services, and ancillary cleft care. Confronting these disparities at a national level would help ensure cleft care services are consistent across the United States.
The strengths of the study include the consistency of single-center data collection, high granularity of ADI scores, large patient cohort, and comprehensive capture of socioeconomic and clinical data. However, the single-center nature of the study, while aiding in consistency, limits the generalizability of the findings to other CLP centers. Additionally, the retrospective nature of this study might not have fully captured potential confounding factors not listed in the EMRs, such as educational attainment and cultural practices. Quantitative measures of cleft severity, hearing status, and speech therapy intensity were not available for all patients and, therefore, could not be incorporated into adjusted analyses. This study did not exclude patients with syndromic diagnosis, other medical comorbidities, or stratify by cleft phenotype or severity. However, syndromic diagnoses were similarly distributed across ADI quartiles. Another limitation of this study is that we were unable to account for residential mobility over the time span of this study and instead used the most recent address listed in the patients’ electronic health records to calculate ADI scores.
Future studies could benefit from exploring more longitudinal outcomes across ADI quartiles in CLP care. It would also be beneficial to investigate other measures of speech evaluation in addition to hypernasality. Future studies could analyze measures of quality of life as the objective measures in our study may not reflect the reasons individuals and families pursue a secondary speech surgery. Additionally, expanding similar studies to include multiple centers or national cohorts would allow for a broader understanding of regional disparities.
Footnotes
Ethical Statement
This study received initial ethical approval from the University of Texas Southwestern Medical Center IRB (UTSW-IRB-Form Y1) on 08/03/2023.
Author Contributions
Lauren Reese: Data analysis and interpretation; drafting of the manuscript.
Alexander Velazquez: Data acquisition; drafting of the manuscript.
Kayla Prezelski: Data acquisition; drafting of the manuscript.
Alex Kane: Critical revision of the manuscript; final approval of the version to be published.
Paymon Sanati-Mehrizy: Study conception and design; data acquisition; analysis and interpretation of data; final approval of the version to be published.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.