
Abstract
Objective
To determine the efficacy of hyaluronic acid (HLA) lip filler to correct subtle cleft lip asymmetries in adults using a validated patient reported outcome measure (PROM).
Design
Prospective cross sectional.
Setting
UK National Health Service.
Patients, Participants
Over 18 years old with repaired cleft lip and dissatisfaction of their lip appearance.
Interventions
HLA lip filler injection.
Main Outcome Measures
A validated, cleft specific PROM, the lip module of CLEFT-Q™ prior to treatment and again after six weeks.
Results
24 patients included. A mean total CLEFT-Q™ score pre-procedure was 14.9 (Stand deviation (SD) = 4.91) and 24 (SD = 6.08) post-procedure. Difference in mean total score pre- and post-procedure were statically significant (P = .0001) in all domains on the CLEFT-Q™. No adverse outcomes.
Conclusion
HLA filler to correct subtle cleft lip asymmetries in adults is a simple low risk technique, which can significantly improve the patient's perception of lip appearance.
Conclusion
HLA lip filler to correct subtle cleft lip asymmetries in adults is a simple technique, low risk procedure which can significantly improve the patient's perception of lip appearance.
Introduction
Subtle cleft lip asymmetries can persist despite revision surgery and present a complex surgical challenge. In our experience, patients are often reluctant to undergo further surgical revisions and the uncertainties of repeat scarring. Increasing societal pressure and scrutiny placed on shared self-portrait photographs can be negatively associated with an individual's level of self-esteem and perceived minor lip defects can have a significant psychological impact on the patient and their wellbeing1–3.
The use of non-permanent fillers to enhance native lip architecture in line with current aesthetic trends is increasingly popular with a younger demographic, 2.6 million people in the USA having hyaluronic acid (HLA) filler during 2020. 4 Globally the market is worth an estimated $5.05 billon in 2021. 5 While this modality may offer a solution to a complex surgical problem with minimal down time, the use in cleft lip patients’ needs to be carefully evaluated to ensure that patients get a predictable outcome with minimal risks.
HLA is the most commonly used non-permanent fillers, 6 it is a glycosaminoglycan secreted by fibroblasts found in the dermis, synovial joints and hyaline cartilage. It plays an important role in dermal hydration, cellular proliferation and wound healing. 7 Exogenous HLA is inert and its viscoelastic and hydrating properties make it a good soft tissue filler. In its native form it is a liquid with a half-life of 1-2 days. 8 To prolong its half-life, HLA is crosslinked to impede enzymatic degradation. Higher degrees of crosslinking produce a cohesive viscous gel and increased longevity. Lower degrees of cross linking are easier to disperse once injected in the skin and are often preferred to correct small cutaneous defects. 7
To date the main use of HLA has been in soft tissue augmentation, filling rhytids and improving lip definition. There is good evidence on the safety of HLA filler but limited evidence in the literature of its use in patients with cleft lip9–12. In this study we describe our approach to using injectable HLA fillers to improve cleft lip asymmetry and aim to determine the impact of this treatment on patients using patient reported outcome measures.
Methods
Patients included were over 18 years of age with previous completed cleft lip repairs. Each attended the Welsh Centre for Cleft Lip & Palate with dissatisfaction of their lip appearance. All were keen to avoid any further surgery and wished to explore non-surgical therapeutic options to treat their lip asymmetries. Patients were assessed for their suitability for HLA filler, and were excluded on the basis of the following: allergy to Gram positive bacterial proteins, allergy to Lidocaine, pre-existing filler in lip areas to be treated, pregnant or breast feeding and on immunosuppressive therapy.
Suitable patients were counselled on the nature of the procedure and consented including the risks of skin necrosis, temporary or permanent impairment of vision, granuloma formation, hypersensitivity reaction and persistent asymmetry. Patients were counselled to refrain from strenuous exercise, alcohol, or excessive heat exposure as well as pressure on the lip for 48 h after treatment. All procedures were performed by a single consultant cleft surgeon.
Technique
Bilateral infraorbital nerve blocks were administered with 2% Lidnocaine & 1: 80 000 adrenaline (Lignospan® Special 2%). Initial cutaneous puncture was undertaken using a 23G introducer needle. Scar subcision was then performed with a blunt-tip cannula (TSK 22G STERiGLIDE). HLA filler was then introduced to the body of the vermillion, superficial to the orbicularis muscle via the cannula. Further filler was placed more superficially via a needle where indicated. The precise type of the filler used (listed below) depended on the degree of subtlety of the issue reported.
Juvéderm Vobella® XC, Allegan Inc Juvéderm Volift ®XC, Allegan Inc.
Injections were performed in an outpatient treatment room on a relining dental chair. Hyaluronidase was accessible within the treatment room.
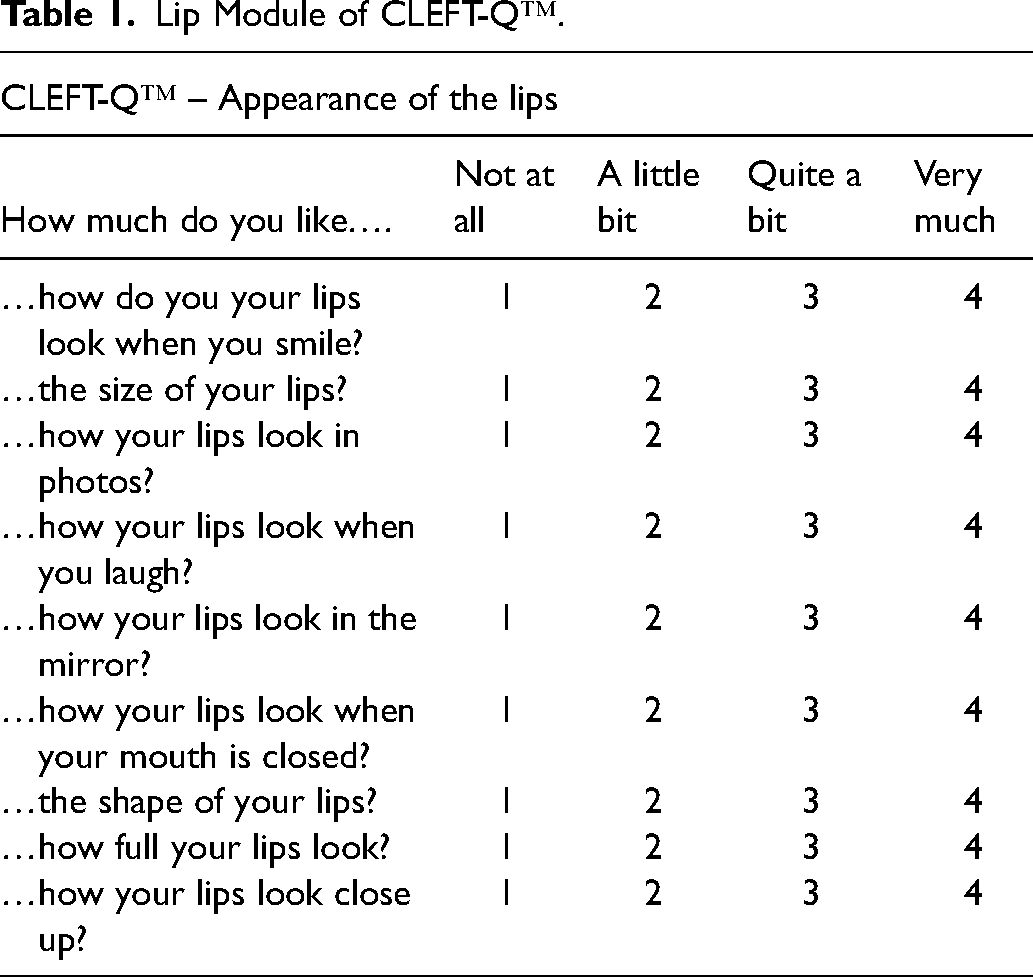
Assessment of treatment outcome was done using the lip module of CLEFT-Q™, a cleft specific and validated patient reported outcome instrument (Table 1). 13 Patients were asked to complete the lip module of CLEFT-Q™ prior to treatment and again six weeks later, by an independent investigator. A paired t-test was used, by a blinded statistician, to determine if there were any statistically significant differences in CLEFT-Q™ scores before and after the procedure.
Lip Module of CLEFT-Q™.
Standardised photographs were obtained both before and between 6-8 weeks after the filler procedure. Approval for this study was sort from the local audit and ethics committee and sperate written consent was obtained for the use of all photographs in this manuscript.
Results
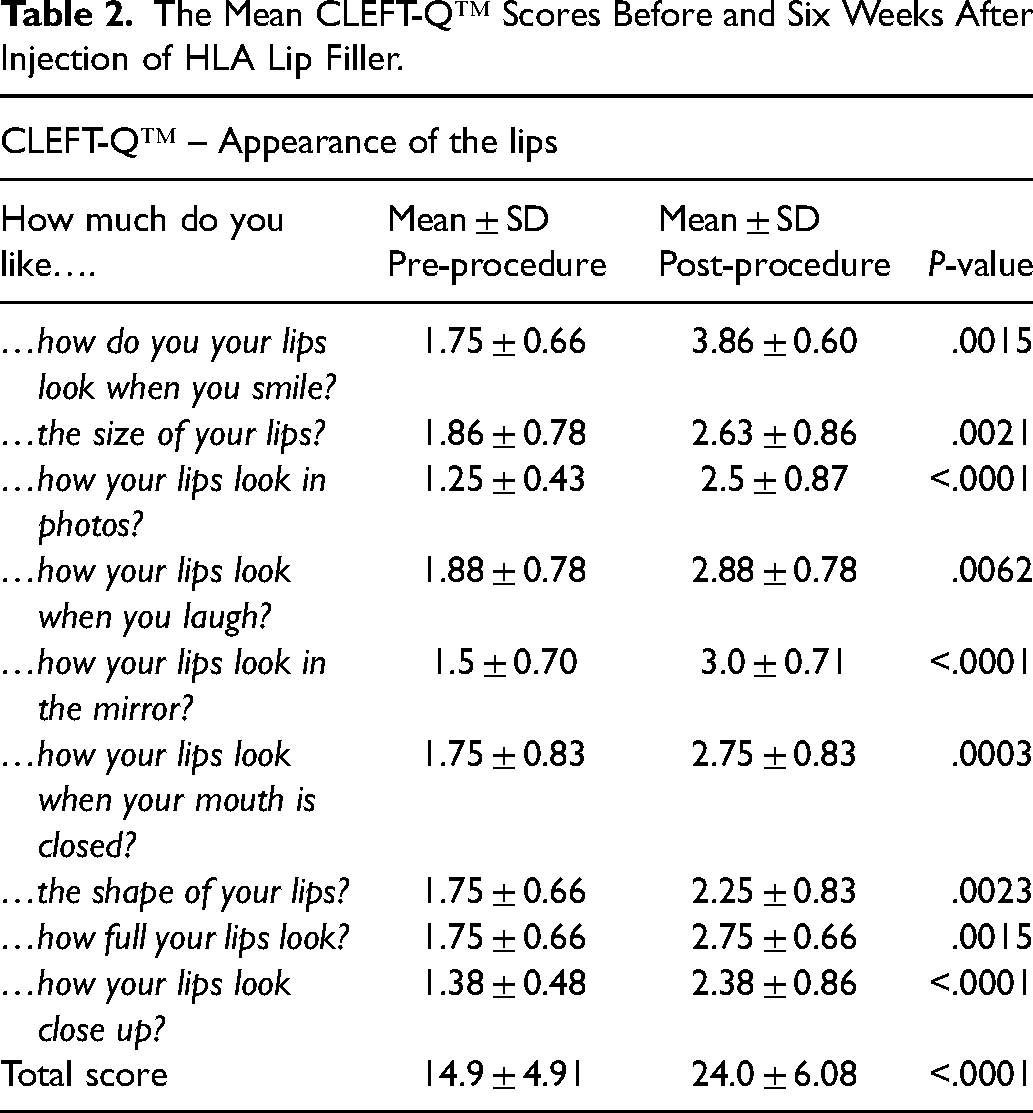
There were 24 patients who met the inclusion criteria (23 unilateral, 1 bilateral). Each patient completed the lip module of CLEFT-Q™ prior to the procedure and again six weeks later (Table 1). The mean total CLEFT-Q™ score before the procedure was 14.9 (Stand deviation (SD) = 4.91) and 24 (SD = 6.08) after the procedure. The lowest mean scores from the CLEFT-Q™ related to the appearance of the lips in photographs (1.25) and up close (1.38) before the procedure. In fact, all the domains pre-procedure had a mean score of less than two. The difference in mean total score pre- and post-procedure was statistically significant (P = <.0001) (Table 2) with all mean scores post-procedure being greater than 2. There were statistically significant differences in mean scores in all domains on the CLEFT-Q™ post-procedure. Improvements in photographs, in the mirror and closure up where the most significant (P = <.0001) (Table 2). The procedure was well tolerated, no patients had an adverse outcome and there were no complications. Pre and post procedure results are show for an adult patient with left unilateral cleft lip (Figure 1).
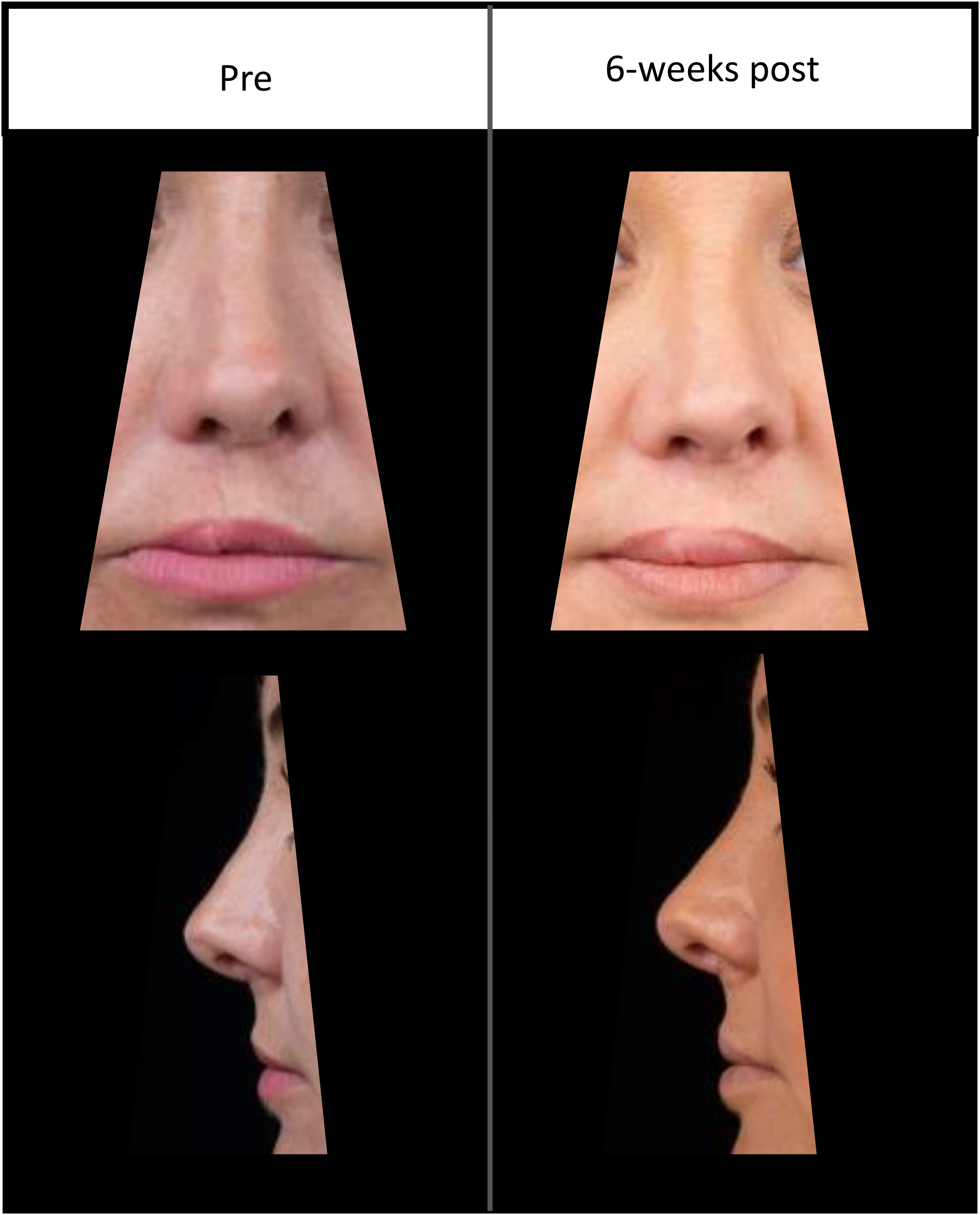
Photographs of an adult patient with right unilateral cleft lip appearance before and six weeks after HLA lip filler.
The Mean CLEFT-Q™ Scores Before and Six Weeks After Injection of HLA Lip Filler.
Discussion
This study describes a technique for HLA lip filler in adult cleft lip patients and highlights patient perceptions of their lips after cleft repair and following the administration of filler to improve asymmetry using a validate patient reported outcome measure: the CLEFT-Q™. In particular, this study demonstrates that a significant improvement in how patients perceive the appearance of their lips can occur following the simple administration of lip filler. This is specifically the case in photographs, in the mirror and on close up appearance. HLA filler was associated with minimal bruising or swelling and was well tolerated by all patients, matching experience of other authors.11,12 It was of interest to note that our patients indicated the lowest scoring component of the CLEFT-Q™ was the appearance of their lips in photographs, perhaps pertaining to the increasing aesthetic pressures and expectations, mirroring trends in non-cleft peers. 14 This was also the domain of the CLEFT-Q™ that demonstrated the highest rise in mean score after the procedure, indicating not only the weighting patients place on this component of their appearance, but moreover reveals the reversibility of this negative self-perception which can be greatly augmented through a relatively simple procedure such as the use of injectable fillers.
HLA has proved versatile and safe in a metanalysis of use in correction of nasolabial folds, the Juvéderm™ produce range achieving the best efficiency in a subgroup analysis. 15 If performed correctly, HLA filler offers patients a lower risk and quicker recovery compared to surgery. However there are well documented reports of serious potential complications including the occlusion of central retinal artery and resulting visual loss. 16 Most frequently this has been associated with injections to the nose. 17 Furthermore, the injection of too much filler, especially if injected into the muscle, can lead to distortions of normal lip architecture and uneven distribution. Infections are uncommon, though patients with a history of oral herpes simplex should be considered for pre-treatment acyclovir. 7 Granulomatous inflammation after injection is estimated at 0.1%-0.01% and can be challenging to treat. 16 Hyaluronidase can reduce the effects of unwanted deposits and vascular complications of HLA injection. 18
A department of health review of the regulations of cosmetic intervention in 2013 identified dermal fillers as a particular cause for concern. 19 In the UK there is currently no requirement for training or previous experience to inject dermal fillers and patients seeking treatment in the private sector risk treatment by unscrupulous practitioners. A recent survey of cleft lip patients over 16 years old by CLAPA (cleft lip and palate association) suggested that 45% of patients surveyed wish to have access to lip fillers as part of their cleft treatment. 20 We acknowledge that this is a small single centre study with a short follow up period, however we show that HLA filler can have a role in improving perception of appearance in adult patients with subtle lip defects who wish to avoid surgery and could be considered as a tool to predict satisfaction prior to future surgical lip augmentation with autologous (fat, dermis, fascia) or alloplastic material (PermaLip™ silicone lip implant). 21 This treatment was provided with no cost to the patient on the National Health Service (NHS). We appreciate that in other health systems the cost of a non-permanent solution may represent a limiting factor for patients. There is need for a larger multicentre study, with longer term follow-up to determine the costs and benefits of providing on going HLA filler as part of treatment for cleft lip.
Conclusion
HLA lip filler to correct subtle cleft lip asymmetries is a simple technique, low risk procedure which can significantly improve the patient's perception of lip appearance. It is quick and suitable in an outpatient setting.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Not required.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.