
Abstract
Objective
Apert syndrome (AS) is a rare congenital craniofacial disorder that requires a multidisciplinary approach to treatment and multiple surgeries. Given that cleft palate (CP) is presented in some of these cases, this poses an additional risk of aggravating obstructed airways after closure. The timing and outcome of CP repair in these patients remains disputed and requires additional attention.
Design
This retrospective analysis included patients diagnosed with CP and AS, born between 1950 and 2020, and treated at our institution. Data were collected from medical records and evaluated using descriptive statistics.
Setting
Data analyses were conducted at Sahlgrenska University Hospital in Gothenburg, Sweden.
Patients/Participants
A registry of 83 patients with AS resulted in a cohort of 26 patients also presenting with CP.
Main Outcome Measures
Postoperative complications, requirement for intensive care, and reoperations following CP repair.
Results
CP incidence among all registered patients was 31%. Patients undergoing CP repair at low age (mean: 22.5 months) tended to experience more frequent postoperative complications and requirements for intensive care. Among the evaluated cohort with medical records describing CP repair (n = 14), 29% experienced postoperative complications, all of which involved aggravation of obstructed airways.
Conclusions
This study highlights the importance of airway assessment before and after CP repair in AS. The findings suggest that surgical outcomes might benefit from postponing CP repair, avoiding combined surgeries, and operating in two stages when indicated. However, additional and larger studies are required.
Keywords
Introduction
Apert syndrome (AS; also known as acrocephalosyndactyly) is a rare congenital disorder that occurs in approximately one in 100,000 births. 1 AS was first described in 1906 by the French pediatrician Eugene Apert and today is considered among the most severe forms of all craniosynostosis syndromes. Patients with AS display craniosynostosis (premature fusion of cranial sutures), midfacial hypoplasia, proptosis, and symmetric syndactyly of the hands and feet (fusion of phalanges). Patients can also present with varying degrees of intellectual disability, skeletal defects, respiratory difficulties, dermatological anomalies, and other visceral defects.2,3 Craniosynostosis in AS most frequently involves a premature fusion of the coronal sutures, leading to abnormal skull-base development that results in formation of a steep, wide, and flattened forehead. Children with AS commonly present an associated cleft palate (CP), although different studies report dissimilar frequencies (30–75%).2,4 In these cases, the most frequent presentation is a soft palate cleft. 5
AS-related malformations can also lead to secondary complications, such as obstructive sleep apnea (OSA) from tight airways, cornea damage from exophthalmos, recurrent ear infections and hearing loss from narrow auditory tubes, and feeding and speech problems from dental maldevelopment and possible CP. 1 Additionally, there are risks of developing increased intracranial pressure or hydrocephalus in AS, especially if the cranial deformity is left untreated. 6 Overall, these children require lifelong treatment to maintain the best possible physical and mental health and function.
Affected patients are referred to a craniofacial unit after birth, and treatments are symptom-specific and supportive. Patients receive a multidisciplinary approach to address the complexity of AS according to the results of individualized assessment. Breathing and nutrition are prioritized at birth. Some children may need a tonsillectomy; removal of adenoids; assessment of OSA; assisted breathing using continuous positive airway pressure (CPAP), nasopharyngeal airway (NPA), or oropharyngeal airway (OPA) methods; and in some cases tracheostomy.1,4 To promote growth development, patients may need specific feeders, feeding techniques, or percutaneous endoscopic gastrostomy (PEG). 7 Moreover, multiple surgeries are required for AS during childhood to prevent developmental delays and restore functions, as well as aesthetics. These include reconstructive surgery for craniosynostosis, fronto-facial surgery, Le Fort advancements, orthognathic surgery, and separation of syndactyly in the hands and feet. Furthermore, ventilation tubes may also be implanted in the ears to prevent hearing loss derived from recurrent middle ear infections.1,2,6 Although the appropriate timing of surgeries is disputed, studies agree on performing strategic surgical interventions to reduce the quantity of general anesthesia.2,8 A literature review from 2008 focus on the neurotoxic effects of general anesthesia in several animal models, suggesting that combining and coordinating operations may lower the risk of neurocognitive impairment in children. 9
Children presenting with CP often undergo CP repair within the first year of life. However, airway obstruction is common in AS, and CP repair can potentially aggravate this condition. A thorough assessment is critical to determine if the respiratory tract is at risk during CP repair and whether the procedure would be more appropriate at a later stage following accurate stabilization of respiratory functions.1,10 The ideal timing of CP repair is a topic of frequent discussion among physicians and requires individualized assessment and treatment that correspond with the extent and type of cleft, as well as patient-specific needs and the presence of breathing difficulties.11–13
In the United States, CP is recommended for repair before 18 months of age. This timing is based on the ratio between speech development and the effect of repair on midfacial growth, suggesting that early closure benefits speech outcomes, whereas late closure may instead lower the risk of maxillary surgery later in life. Because CP repair can potentially lead to an upper airway obstruction, this possibility must be assessed before surgery. 13 To promote positive outcomes in both speech and maxillary growth, a cleft of the hard and soft palate can be repaired in two stages (most frequently practiced in Europe). The first stage usually consists of soft palate repair, and the second stage involves hard palate repair. 10 At our institution (Sahlgrenska University Hospital), the soft and hard palates are generally operated at the ages of 6 months and ∼2 years, respectively. 12 The appropriateness of the two-staged repair is debated, and the timing of surgery varies between country, resulting in different study results. However, this method has reportedly proven beneficial to both speech outcomes and maxillary growth.10,14 Nevertheless, other secondary operations, such as surgery for a palate fistula, surgery due to velopharyngeal dysfunction, or correction of the maxilla, may still be needed. 12
The complexity and different degrees of severity in AS complicate treatment and management. Although several articles address the occurrence of CP in AS, none have discussed outcomes of CP repair in association with AS treatment. Considering the importance of treating CP to avoid feeding problems and developmental delays, 11 we retrospectively evaluated outcomes related to CP assessment and repair in the context of AS.
Materials and Methods
Data Collection Procedures
A retrospective study was conducted at Sahlgrenska University Hospital in Gothenburg, Sweden. At this hospital, the Department of Plastic Surgery administers a craniofacial registry of patients diagnosed with AS, born between 1950 and 2020, and having undergone treatment at this location. This registry includes 83 patients with AS. The study was based on a systematic examination of the medical records of patients with AS and also diagnosed with CP, resulting in a cohort of 26 patients (31% of AS patients in the registry). A research protocol was created and defined based on previous research of and clinical experience with these syndromes. Data collection was performed by following and completing the research protocol for all included patients. Information was gathered from the Swedish medical record system Melior. Medical records from other hospitals in Sweden were also requested, as necessary. This study was conducted under authorization of a previous approval by the Swedish Ethical Review Authority (registration number: 784-11). Patient consent was not required.
Variable Analyses
Of the 26 patients with AS and CP, 14 underwent initial CP repair and had complete medical records available. Variables for the analyses included the number and type of postoperative complications, amount of required postoperative intensive care (measured in days), and number of reoperations. These variables were also separately evaluated according to the age (in months) of the patient at the time of CP repair, whether CP repair was combined with other surgeries, and which operative technique was used (one- or two-stage) in regard to patients with a cleft of the hard and soft palate. Additional variables in these 14 patients were the use of CPAP/tracheostomy/PEG and whether respiratory support (eg, NPA or OPA) was necessary in relation to the process of CP repair.
Baseline variables were collected for all of the 26 included patients. These included gender, CP type, OSA, usage of CPAP/tracheostomy/PEG/respiratory support regardless of time for CP repair, recurrent upper airway infections and/or ear infections, hearing loss, hearing device, ventilation tubes in ears, intellectual disability, and other health conditions in addition to their syndrome.
Statistical Methods
For comparisons between two groups, we used Fisher's non-parametric permutation test for comparison between two means for continuous variables and Fisher's exact test for dichotomous variables. The main result of this study was the mean difference between two groups along with a 95% confidence interval (CI) and effect size [effect size = mean difference / pooled standard deviation (SD)]. The distribution of continuous variables is provided as the mean, SD, median, minimum, and maximum. The distribution of categorical variables is given as numbers and percentages. All significance tests were two-sided, with a p < 0.05 considered significant. Statistical analyses were performed using SAS software (v9.4; SAS Institute, Cary, NC, USA).
Incidence
For the 26 patients with AS and CP, the incidence of CP within this syndrome was calculated by dividing the number of these patients by the total number of patients with AS included from the registry (n = 83). The calculated incidence refers to all patients with AS who had received treatment at Sahlgrenska University Hospital. Given the rarity of the syndrome and the requirement for a multidisciplinary approach to treatment, it was reasonable to assume that all children with AS in Sweden had at some point received treatment at our institution.
Results
Among the 26 patients with AS and CP (14 male, 12 female), eight (31%) presented with soft CP, seven (27%) with soft and hard CP, three (12%) with submucosal CP, and eight (31%) with an unknown type of CP. One patient required 24-h breathing surveillance by family and assistants due to severe airway obstruction and chronic tracheostomy. One patient required OPA after CP repair until breathing was stabilized, and another patient required OPA during all of the surgeries to maintain an open airway. Additionally, one patient required use of an NPA for three years up until 1-year prior to CP repair. OSA was reported in 46% of patients within the cohort. Use of a CPAP was necessary at some point by seven patients (27%), a tracheostomy was required by eight patients (31%), and PEG by 10 patients (39%). Hearing impairment was reported in 10 patients (39%), although hearing devices were only reportedly used by five patients (19%). Problems with recurring ear infections were identified in 69% of patients, with implantation of ventilatory ear tubes required by 77%. Recurring upper respiratory tract infections were identified in 58% of patients, and there were reports of epilepsy in eight patients (31%), a heart murmur in four (15%), and hydrocephalus in three (12%). Intellectual disability was reported in 15 patients (58%).
Of the 14 patients with AS, CP, and available medical records describing CP repair, the mean age at repair was 22.5 months (median: 19 months). Postoperative complications were reported in four patients (29%) and all involved worsening obstructed airways. Patients with postoperative complications had either a soft CP (n = 2) or hard and soft CP (n = 2). Five patients (36%) required postoperative intensive care at an intensive care unit, with all only requiring intensive care for 1 day. Two patients (14%) required secondary palate surgery, with one patient undergoing two surgeries to reduce palate hyperplasia and another undergoing the same procedure in addition to surgery for a palatal fistula. CP repair was combined with other surgeries in 10 patients (71%), with the most common surgery being implantation of ventilation tubes in the ears in six patients. One patient required use of a CPAP, and three required PEG during the time of CP repair, whereas none required a tracheostomy. Among the six patients that had a cleft of the hard and soft palate, four completed CP repair in one stage and two in two stages.
Although statistical comparisons were limited by the small study population, the mean difference in age at CP repair was generally lower for patients experiencing postoperative complications or requiring postoperative intensive care (Tables 1 and 2). The mean difference in age at CP repair between patients with postoperative complications (n = 4) or without (n = 10) was 11.6 months [95% CI (−3.5, 41.5)], with those experiencing postoperative complications younger in age. The mean difference in age at CP repair between patients requiring postoperative intensive care (n = 5) or not (n = 9) was 9.8 months [95% CI (−6, 37)]. All the patients with postoperative complications or requiring postoperative intensive care underwent CP repair combined with secondary surgery. Of the four patients with postoperative complications, two completed CP repair using a one-stage palate procedure. Similarly, of the five patients requiring postoperative intensive care, two completed CP repair using a one-stage palate procedure.
Postoperative Complications After Cleft Palate Repair in Patients with Apert Syndrome.
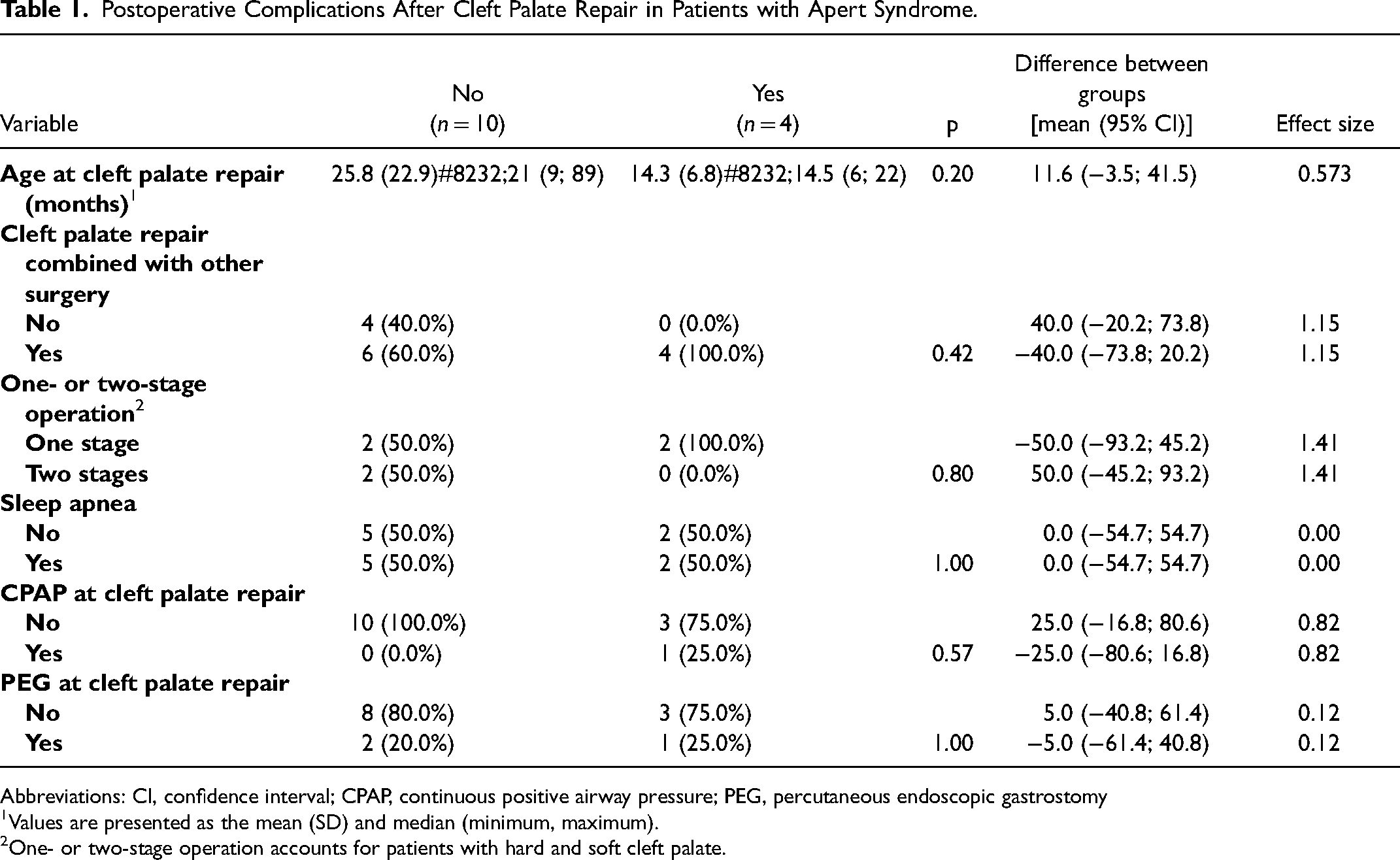
Abbreviations: CI, confidence interval; CPAP, continuous positive airway pressure; PEG, percutaneous endoscopic gastrostomy
Values are presented as the mean (SD) and median (minimum, maximum).
One- or two-stage operation accounts for patients with hard and soft cleft palate.
Patients with Apert Syndrome Requiring Intensive Care After Cleft Palate Repair.
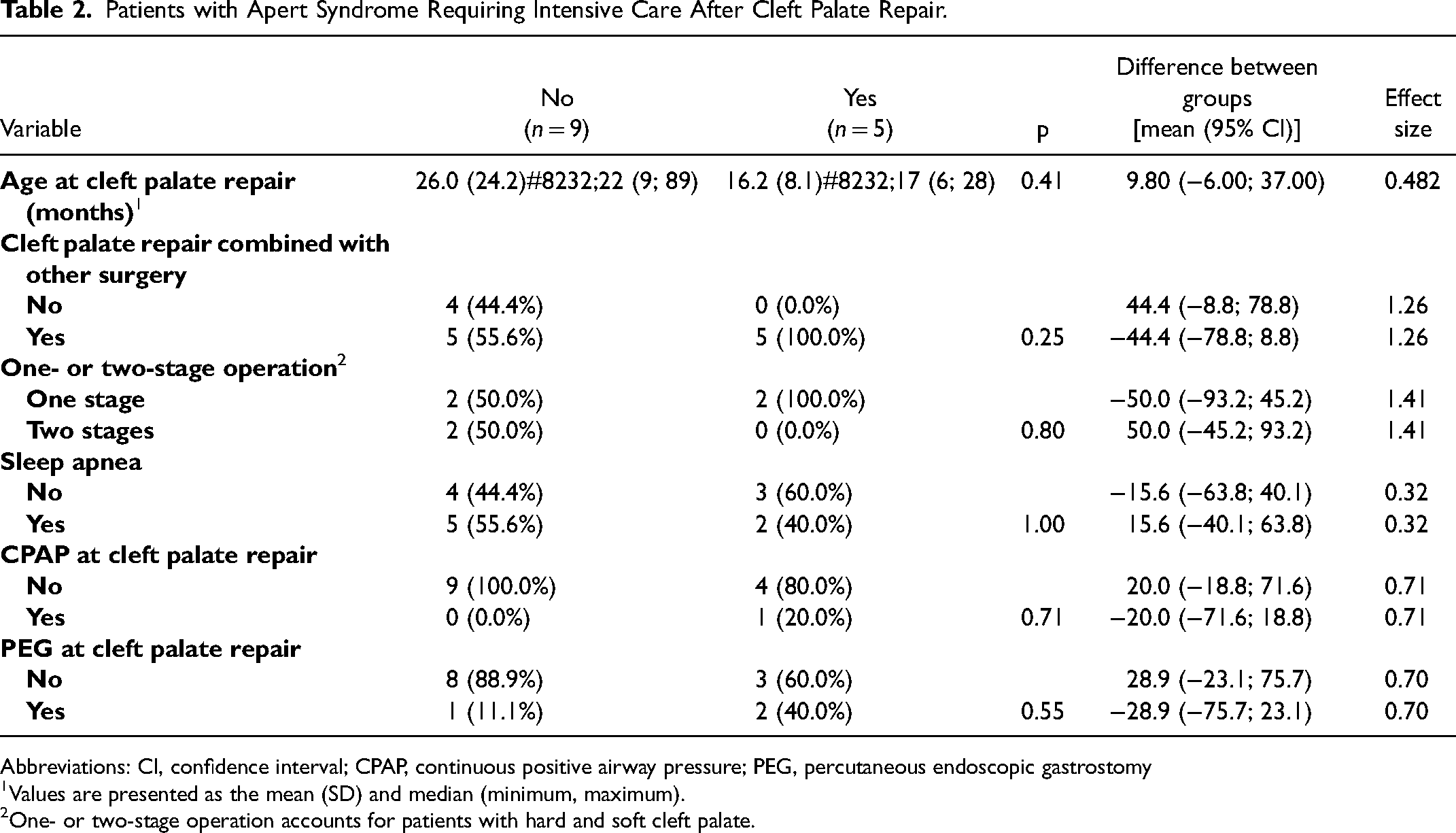
Abbreviations: CI, confidence interval; CPAP, continuous positive airway pressure; PEG, percutaneous endoscopic gastrostomy
Values are presented as the mean (SD) and median (minimum, maximum).
One- or two-stage operation accounts for patients with hard and soft cleft palate.
In the group of patients that underwent CP repair before the age of 20 months, three experienced postoperative complications, and four required postoperative intensive care. In the group of patients that underwent CP repair after the age of 20 months, one experienced postoperative complications, and one required postoperative intensive care. This provided a relative risk (RR) interval of 0.91 [95% CI (0.79, 1.06)] for postoperative complications and an RR interval of 0.96 [95% CI (0.86, 1.06)] for postoperative intensive care.
Discussion
This retrospective study presented follow-up data on a national population of patients with AS that underwent CP repair during a 60-year period. As a consequence of the small study population, we did not identify a significant difference between age at CP repair and postoperative complications, requirement for intensive care, or the need for reoperations. However, we found that patients who did experience postoperative complications or require intensive care also demonstrated a lower age at CP repair (<20 months). Furthermore, the available data were insufficient to draw conclusions regarding the reoperation rate; however, it is possible that age at CP repair might also affect this outcome. A recent study on the timing of CP repair and the impact of CP on upper airway obstruction in Pierre Robin sequence (a congenital disorder involving micrognathia and obstructed airways) revealed that presence of a CP decreased OSA severity. Furthermore, they identified common postoperative complications following CP repair as respiratory distress and palatal fistulas. The authors suggested that delaying CP repair might lower complication rates. 15 This supports the concept of age at CP repair possibly affecting postoperative complications in patients with obstructed upper airways, as in AS.
In this study, all postoperative complications following CP repair comprised aggravation of obstructed airways, with OSA reported in 46% of patients with AS and CP. A retrospective study from 1998 examining airway management in 251 children with major craniofacial anomalies, including AS, found that patients with CP showed a reduced probability of receiving a tracheostomy, given that an open CP provides an additional nasal airway. 16 These results agree with CP repair potentially worsening obstructed airways. Additionally, that study indicated the utility of surgical treatment for OSA (eg, tonsillectomy, adenoidectomy, tongue reduction, or midface advancement) in patients with craniofacial syndromes, with the specific clinical features of patients also suggesting positive outcomes following tongue reduction and midface advancements. These findings were supported by a 2016 study suggesting that upper airway endoscopy could optimize the treatment of AS-related OSA. 17 Moreover, another study established the negative effect on the quality of life of OSA in children with syndromic craniosynostosis. 18 These results highlight the critical need for breathing assessment, treatment, and stability before CP repair is performed in relation to AS.
Among the six patients with a cleft of the hard and soft palate, four underwent CP surgery with one-stage palate repair. Two of these four patients experienced postoperative complications with aggravated airway obstruction, which differed from the other two patients who underwent two-stages CP repair without any postoperative complications. We observed a similar outcome for patients requiring postoperative intensive care (2 of 4 patients undergoing one-stage surgery required intensive care). Interestingly, all patients that experienced postoperative complications or required intensive care also underwent CP repair combined with secondary surgeries. These findings could suggest that less surgical stress could benefit postoperative outcomes in these patients. This includes performing CP repair divided into two stages and to avoid combined surgeries.
Notably, 31% of the patients in the AS and CP cohort also had a record of epilepsy. There are few reports in the literature of epilepsy in patients with AS. A previous report from an investigation at the same hospital as the present study found that 17% of patients with AS also had epilepsy. 19 A more in-depth investigation is required to determine whether this qualifies as a separate phenotype of AS or if it is a possible secondary effect of a shunt inserted to address excess cerebrospinal fluid related to hydrocephalus (as observed in some patients). Nevertheless, reports of epilepsy in the present study were higher than those of hydrocephalus, suggesting the possibility of epilepsy as an AS phenotype.
This study has numerous strengths and limitations. First, the assessment involved an extended time period and multiple patients registered at the craniofacial center at Sahlgrenska University Hospital. Given the rarity of AS and the corresponding prevalence of CP, this offered a relatively large dataset for evaluation. However, a major limitation remains the relatively small cohort, which was as a consequence of the retrospective nature of the study and the absence of specific information in many of the older medical records. Therefore, this limited the performance of more complex analyses and relegated the statistical results to those that were mainly descriptive. Future studies should consider collaborations that allow multi-center studies in order to expand sample sizes and thereby provide more reliable results.
Additionally, given that maintaining open airways is a common challenge in patients with AS, there were potential problems that we did not specifically address in this study. For example, we did not directly assess the impact of CP repair on OSA or whether proper preoperative breathing assessment and treatment were performed prior to CP repair. Future studies should investigate these areas, if possible. Furthermore, it is reasonable to suggest that postponing CP repair might reduce the risk of aggravating obstructed airways in patients with AS, despite the importance of CP repair for avoiding other developmental delays. Therefore, future studies should also investigate how long CP repair can be postponed before other issues predominate the risk of aggravated airway obstruction.
Conclusion
In this study, we found that patients with AS and CP and who underwent CP repair earlier (aged <20 months) tended to experience more postoperative complications and were more likely to require intensive care. Notably, this was also observed in patients that underwent CP repair combined with secondary surgeries. Additionally, we found that in patients with a cleft of the hard and soft palate, performing CP repair in two stages might benefit surgical outcomes. Moreover, all postoperative complications identified in this study involved aggravated airway obstruction, highlighting the importance of airway assessment before and after CP repair. These findings emphasize the importance of mandatory and strategic airway assessment and treatment to help prevent future breathing complications in children with AS and undergoing surgery to address secondary conditions.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.