
Abstract
Palatal foreign bodies remain relatively rare, consequently, delays in diagnosis and misdiagnosis can occur leading to unnecessary anxiety and invasive investigations. We report three children with a reflective disc from inside a confetti balloon masquerading as a fistula of the hard palate. Awareness of this foreign body phenomenon enabled timely diagnosis in subsequent patients; hence the need to highlight such cases to the global cleft community. Crucially, while the foreign body remains in the oral cavity, there is an ongoing risk of airway aspiration which could be life threatening. Removal can be easily facilitated in the outpatient setting.
Introduction
Palatal foreign bodies remain relatively rare in comparison to ingested and nasal foreign bodies in children. For this reason, delays in diagnosis and misdiagnosis can occur leading to unnecessary anxiety for parents and invasive investigations for the child. The commonest misdiagnosis of a hard palate foreign body is a tumour of the palate. 1
There have only been three reports in the literature to date of a hard palate foreign body being misdiagnosed as a fistula but none of these have been due to reflective foreign bodies.2,3
We report on three paediatric patients referred to a regional cleft service with a retained reflective confetti disc from inside a party balloon masquerading as a fistula in the hard palate. The mirrored nature of the disc readily mimics a palatal fistula due to the reflection of the lingual mucosa appearing similar in nature to nasal mucosa. These discs are found inside confetti balloons, with some balloons containing multiple discs of varying sizes. (Figures 1 and 2) These balloons are becoming increasingly popular being commonly displayed in the home for birthdays and christenings, thus are readily accessible to young children. The nature of these discs and the potential risk for airway aspiration and obstruction is concerning.
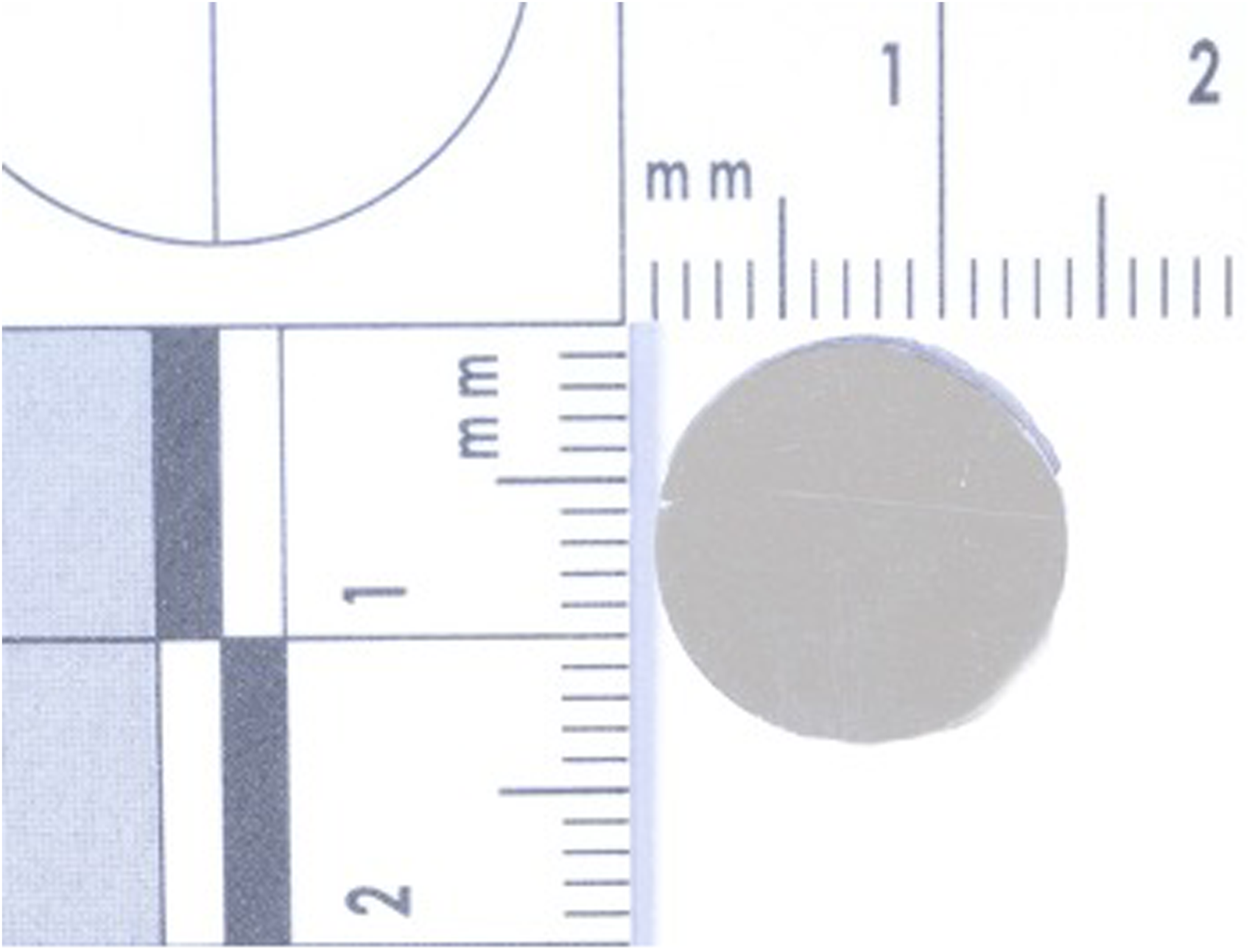
Image of the reflective disc removed from one of the patients in the series.

Image of a confetti balloon with multiple confetti discs inside.
Case Series
Case 1
A 10 month old female was referred to the paediatric team with a 20 mm circular lesion of the hard palate. This was initially noticed by her parents approximately four weeks prior to referral. The child regularly placed items into her mouth and the parents stated she had recently been inserting her fingers intraorally as if she was in discomfort. The paediatric team felt this was likely a congenital abnormality and a CT scan was performed that did not demonstrate a bony lesion nor a palatal defect. After review with another specialty she was discharged. Almost two years later the patient was seen by the cleft team in the outpatient clinic. The use of a light source both intra-orally and intra-nasally confirmed this was not a fistula and the plastic disc was dislodged pain free from the hard palate with ease using a Jobson Horne. The underlying palate was normal with no ulceration or other pathology evident clinically.
Case 2
A 10 month old female was referred to the regional cleft team with a two week history of a ‘large hole’ in her hard palate. There were no prior concerns regarding a palatal defect or any functional issues.
On examination there was the appearance of a large defect predominantly in the hard palate with a normal appearing soft palate. The ‘lesion’ was reflective and was removed uneventfully in the outpatient clinic with Adson forceps. The underlying mucosa was excoriated but there was no underlying soft tissue defect.
Case 3
A 12 month old female was referred urgently to the regional cleft team with a presumed missed diagnosis of a ‘cleft palate’ due to the finding of an approximately 20 mm palatal defect by her parents and their general practitioner. On review by the cleft team it was noted that a reflective disc was wedged within the vault of her hard palate with the remaining palate appearing normal. (Figure 3) This disc was easily removed in the outpatient clinic with a Jobson Horne without complication. There was no underlying ulceration nor infection but a small imprint of the disc remained in the hard palate. (Figure 4) It transpired the patient had a ‘Happy 1st Birthday’ balloon several weeks earlier that contained multiple silver confetti discs.

Image of the child with the reflective disc lodged in the hard palate.

Image of the hard palate following removal of the disc showing the imprint that remained.
Discussion
This case series introduces a novel foreign body that is becoming increasingly accessible to children. The nature of these reflective plastic discs is no doubt appealing to small children who, out of curiosity, will pick them up when the balloon bursts and place them in their mouth. The concern is not limited to the disc lodging against the hard palate, but also the potential risk of airway obstruction if the disc were aspirated.
The first case in this series had a delayed diagnosis of almost two years despite multiple specialty reviews and a CT scan. CT or MRI scans for palatal foreign bodies have been shown to give equivocal reports and potentially misleading diagnoses. 4 Heightened awareness of the ability of reflective disc foreign bodies to mimic palatal fistulae, as seen in the index case, enabled the timely diagnosis in subsequent patients; hence the need to highlight such cases to the global cleft community. Accurate diagnosis with a prompt referral to an appropriate speciality will ensure removal of the foreign body in a timely fashion and prevent prolonged retainment which could ultimately result in ulceration and potential fistulation of the hard palate. Crucially, while the foreign body remains in the oral cavity there is an ongoing risk of aspiration that could be life threatening.
A systematic review in 2019 examined all palatal foreign bodies reported in the literature since 1967. A total of 32 cases were recorded over a 52 year period, none of which involved foreign bodies with a reflective surface mimicking a palatal fistula or cleft palate. The majority of reported foreign bodies were circular plastic screw caps (63%) with other more unusual items including three artificial finger nails and nut shells. Similar to our series, this review article also highlighted the risks of misdiagnosis and invasive investigations in this paediatric population, with four patients having a CT scan to aid diagnosis and eight children being misdiagnosed as having a palatal tumour. In this review, over two-thirds of patients with palatal foreign bodies required a general anaesthesia to facilitate removal. The authors of this systematic review concluded by recommending that all palatal foreign bodies should be removed under general anaesthesia. 1
In our case series, all three palatal foreign bodies were easily removed painlessly in the outpatient setting by a specialist cleft surgeon without complication thereby avoiding an unnecessary hospital admission and general anaesthesia. Indeed, an article by Rocha and colleagues describes the issue of misdiagnosis in three patients with palatal foreign bodies and is in agreement with our view, stating that proper clinical evaluation with both palpation and appropriate lighting should be sufficient to determine the diagnosis and prevent the need for sedation or general anaesthetic. They discuss clinician reluctance to examine difficult children as one of the influencing factors for unnecessary general anaesthesia in this age group. 4
In conclusion, confetti balloons containing multiple reflective discs are becoming increasingly popular. Inevitably they are appealing to inquisitive young children. Each of these discs has the potential to become lodged in the oral cavity and pose an ongoing risk of airway obstruction while in situ. By highlighting this issue we aim to improve accurate diagnosis, with the aid of an adequate light source in the outpatient setting, ensuring prompt removal of the foreign body.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article