
Abstract
Objective
Characterize the interventions and assistance employed by a cleft nurse navigator (CNN) which have mediated improvement in care equity at our institution.
Design
Retrospective study.
Setting
Academic tertiary care center.
Patients, Participants
Patients presenting with cleft lip and/or cleft palate presenting between August 2020 and August 2021 with exclusions for syndromic diagnosis, Pierre-Robin sequence, late (> 6 months) presentation, and prior cleft surgery at outside institutions.
Interventions
Multidisciplinary cleft nurse navigator program
Main Outcome Measure(s)
Family interactions with the CNN by phone, text, and email across the first year of life including feeding support, nasoalveolar molding (NAM) assistance, appointment scheduling, financial assistance, addressing perioperative concerns, and facilitating physician consults. Patient weight and surgical timing were also recorded.
Results
Sixty-nine patients were included with a total of 639 interactions between the CNN and families. Scheduling support (30%), addressing perioperative concerns (22%), and feeding support (20%) were the most common interactions. Feeding support and NAM assistance were heavily distributed in the first 3 months of life compared to after 3 months (P < .001). Median age at first contact was 1 week (range: 22 weeks gestation-14 weeks). There was no difference in the proportion of families receiving feeding support, NAM assistance, or scheduling assistance based on insurance status or race (P > .05 for all).
Conclusions
Scheduling assistance, addressing perioperative concerns, and feeding support are the predominant methods by which the CNN interacts with and assists families of patients with cleft conditions. CNN service distribution is largely equitable between demographic groups.
Introduction
Cleft lip and palate are the most common congenital anomalies impacting the head and neck region.1–3 The presence of a cleft condition presents both functional and esthetic challenges for patients. In early life, infants with clefts experience problems with feeding, susceptibility to ear infections, and abnormalities in dental development.4–7 Later in life, facial appearance and difficulties with speech production increase risk for poor psychosocial outcomes in these patients, including anxiety and depression.8–12 As a result of these challenges, patients with orofacial clefts benefit from care delivered by a multidisciplinary cleft team.13–15
Unfortunately, the complexities of coordinated cleft care have led to inequities for underserved patient populations. Analyses of national databases have shown that nonwhite and publicly insured patients have delayed lip and palate surgery compared to white and privately insured counterparts, and that white patients experience fewer postoperative complications, shorter hospital stays, and lower hospital charges.16–20 Additionally, minority patients are more likely to miss appointments and are less likely to pursue nasoalveolar molding (NAM).21,22 These inequities in early care continue later in life, as minority populations show delays in alveolar bone grafting and lower utilization of cleft rhinoplasty and secondary speech surgery.23–28 Disparities in the timing and utilization of cleft care services are of major importance, as delayed palatal surgery can increase the incidence of velopharyngeal insufficiency and poor speech outcomes.29–31 Moreover, indicators of lower socioeconomic status such as decreased educational attainment and lack of prenatal care have been linked to higher incidences of cleft lip and palate among newborns. 32 Thus, disadvantaged groups are not only more likely to be impacted by cleft lip and palate, but are also at higher risk from poorer outcomes as a result of their condition.
However, while literature describing the unjust distribution of cleft care services has broadened, there have been few reported interventions combating these injustices. An approach which holds potential for patients with cleft lip and palate is patient navigation, which has been shown to reduce spending and improve outcomes in multiple healthcare settings.33–36 Similarly, our group instituted a cleft nurse navigator (CNN), a registered nurse within our department who serves as the primary contact point between parents and the cleft team, with the hypothesis that close communication and clinical follow up with patient families would decrease the likelihood for delayed care. A previous investigation of this program demonstrated that the CNN reduced disparities in the timing cleft lip and palate surgery and improved weight gain in early life, particularly for minority patients. 37 While the benefits of this program have been elucidated, an in-depth description of how the CNN has improved care equity is indicated to promote the development of other CNN programs. Therefore, the purposes of the present study were to 1) Describe the interventions and interactions between the nurse navigator and families that have mediated improvements in care, and 2) assess equity in the distribution of CNN care services to advantaged and disadvantaged groups.
Methods
Patients
This study was approved by the Institutional Review Board. Patients presenting with cleft lip and/or cleft palate between August 2020 and August 2021 were considered for review. Patients were excluded if they had a syndromic diagnosis, Pierre-Robin sequence, Tessier facial clefts, submucous cleft palate, late (>6 months) presentation, or if they did not undergo surgery at our institution. Demographic information was collected for each patient and included race, ethnicity, and insurance coverage, which was recorded as private or public (Medicaid). Each patient was followed until 1 year of age and at least 30 days postoperatively from their last cleft surgery.
Nurse Navigator Interactions
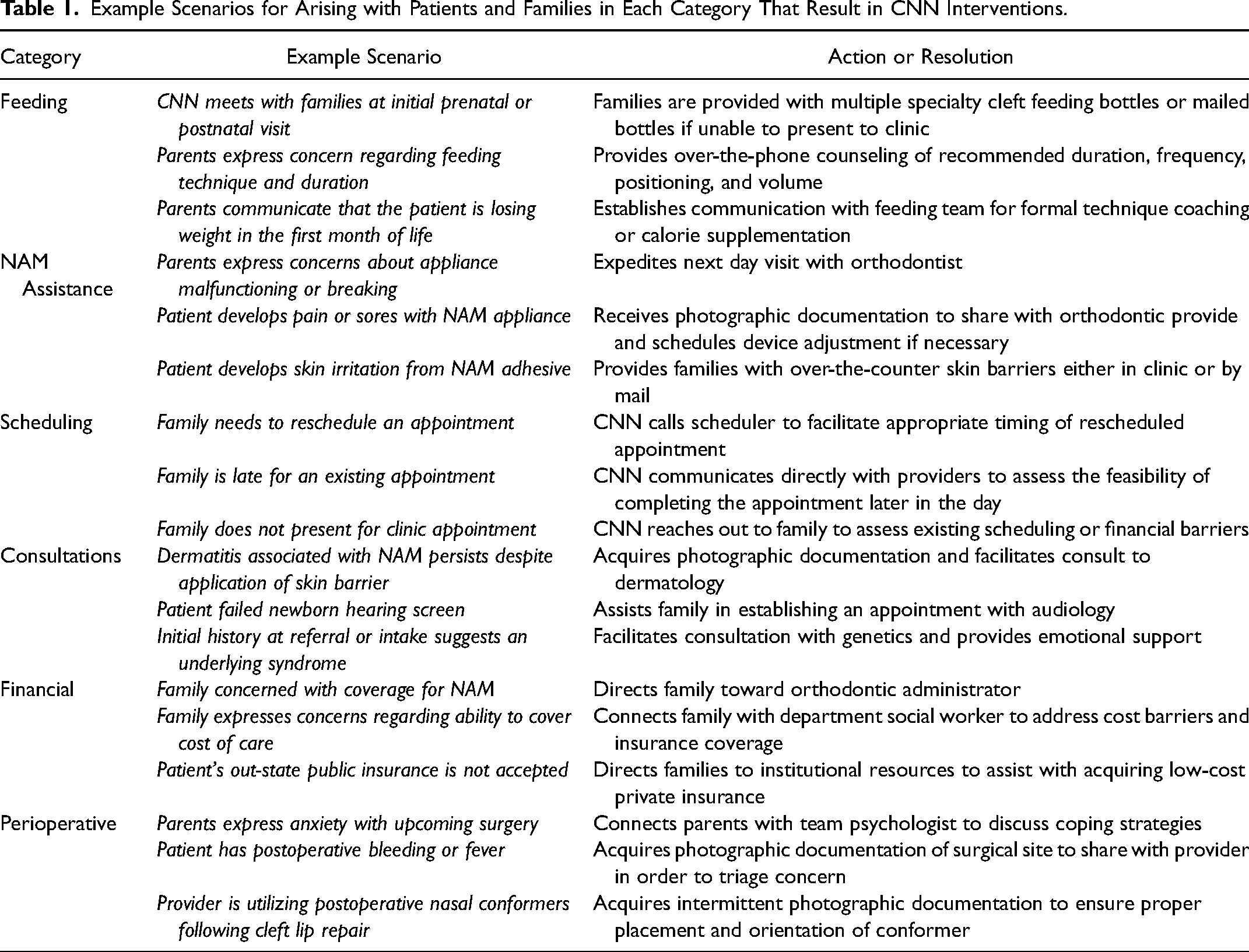
Email, phone, and text conversations between the CNN patient families were systematically analyzed. Patient age, in weeks, at the time of first contact between the CNN and a patient family was recorded, as were prenatal communications. Each interaction was characterized by 1 of 7 categories: feeding support, NAM assistance, appointment scheduling, financial assistance, addressing perioperative concerns, facilitating physician consults, and miscellaneous. Feeding support was defined as documentation of the CNN sending bottle supplies, weight check-ins, and over-the-phone or in-person assistance with feeding technique. NAM assistance included device troubleshooting, orthodontic referrals for dislodged devices or broken devices, and check-ins for adherence. Perioperative support included instructions for preoperative appointments, laboratory testing, and day-of-surgery logistics as well as postoperative counseling related to pain, inflammation, fever, and bleeding. Financial assistance included both helping patients with insurance questions and referrals to social work for payment navigation. Examples of interaction scenarios and resulting CNN actions can be found in Table 1. The date of each intervention and the patient age was recorded. The number of each type of interaction was tabulated for each patient as well as the total cohort.
Example Scenarios for Arising with Patients and Families in Each Category That Result in CNN Interventions.
Weight Gain and Timing of Care Outcomes
Patient weights were recorded biweekly starting at two weeks for the first 3 months of life, as well as recordings at 6 months and 1 year. Weight-for-age z-scores as determined by growth charts were obtained to determine growth percentiles. Patients were retrospectively flagged for poor weight gain if they recorded a z-score below −2.0 in the first year of life. All dates of cleft lip and palate surgeries were recorded as well as patient age at surgery.
Statistical Analysis
All data analysis was conducted using JASP (Version 0.16.3; JASP Team, 2020). Demographic variables were assessed using descriptive statistics. Nurse navigator interactions with patient families were tabulated by patient and across the total cohort in order to calculate the proportional contribution of each interaction type. The proportion of patients receiving each category of interaction and the average timing of each intervention were assessed with descriptive statistics. Distribution of CNN interactions were assessed between publicly and privately insured patients as well as between white and nonwhite patients with the chi-square test. Weight z-scores at each time point and surgical timing for cleft lip and palate repair were compared between demographic groups with unpaired t-tests. CNN interactions were compared between patients flagged for poor weight gain and those who were not with the chi-square test.
Results
One hundred two patients presented for cleft lip and/or palate care in the study period, of whom 69 met inclusion criteria. Thirteen patients were excluded for Pierre-Robin sequence, 6 for syndromic diagnoses, 2 for Tessier facial clefts, 4 for late presentation, 7 for undergoing prior cleft surgery at an outside institution, and 1 for a submucous cleft palate. The cohort was 46% female, 77% white, and 80% privately insured. Thirty patients (43%) had a diagnosis of cleft lip only, 21 (26%) had both cleft lip and palate, and 18 (30%) had cleft palate only.
There was a total of 639 interactions between the CNN and patient families and 97% of patient families had interactions with the CNN throughout the observation period. Median age at first contact was 1 week (range: 22 weeks gestation-14 weeks). Thirty-nine percent of patients were seen prenatally after ultrasound diagnosis. The most common CNN interactions were appointment scheduling (30%), addressing perioperative concerns (22%), and feeding support (20%). Across the categories of interventions, feeding support was on average provided earliest in life (median 3 weeks, IQR 1-8), followed by NAM assistance (median 5 weeks, IQR 2-11) and appointment scheduling (median 6.5 weeks, IQR 1-19, Table 2). Feeding and NAM-assistance were heavily distributed in the first 3 months of life compared to after 3 months of life (P < .001 for both, Figure 1).
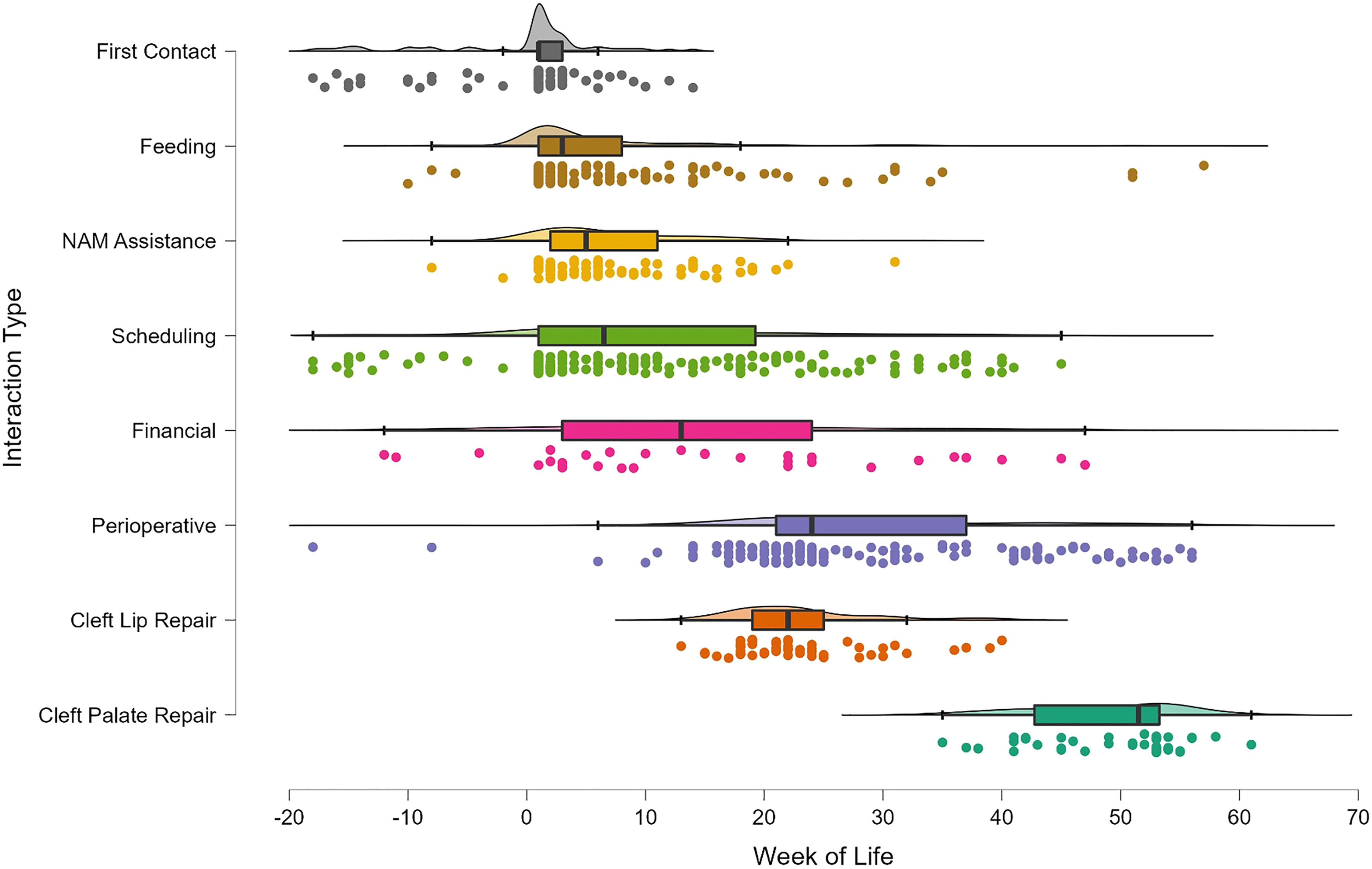
Distribution of cleft nurse navigator interventions as well as timing of cleft lip and cleft palate repair across the first year of life.
Total Number, Median age, and Number of Patients for Each Type of Nurse Navigator Interaction Recorded During the Study Period.
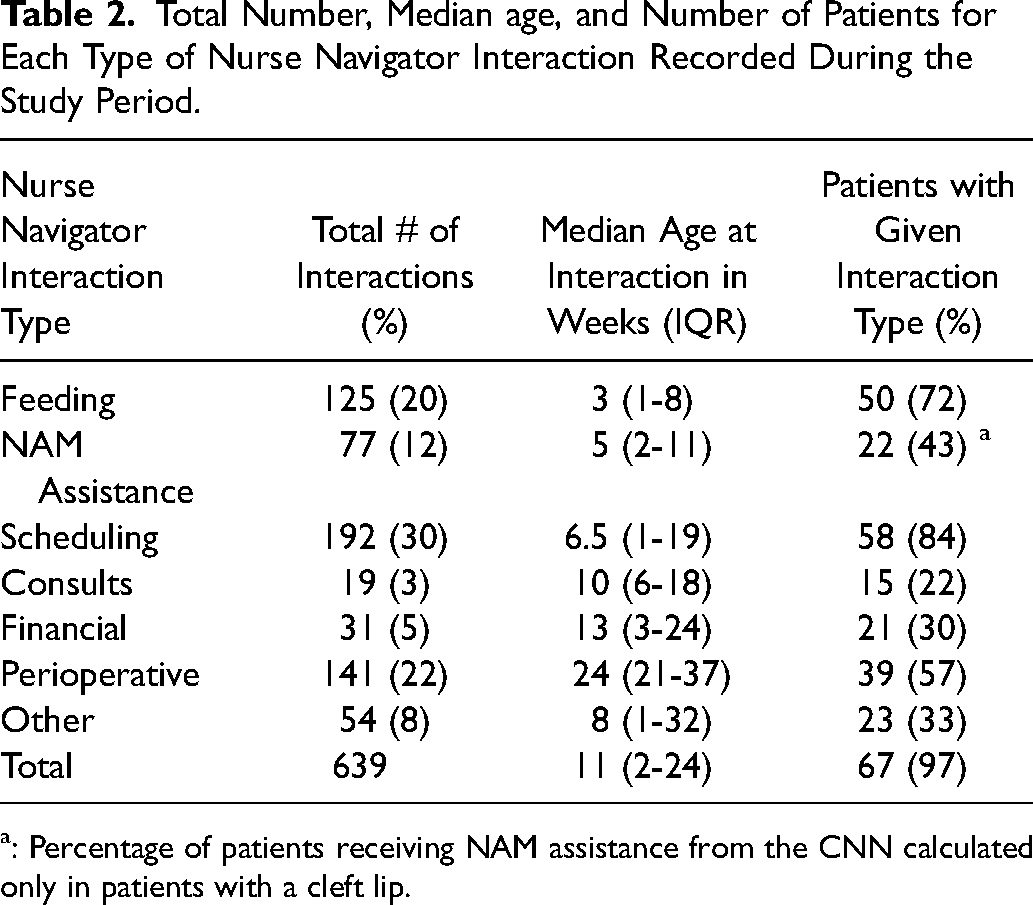
: Percentage of patients receiving NAM assistance from the CNN calculated only in patients with a cleft lip.
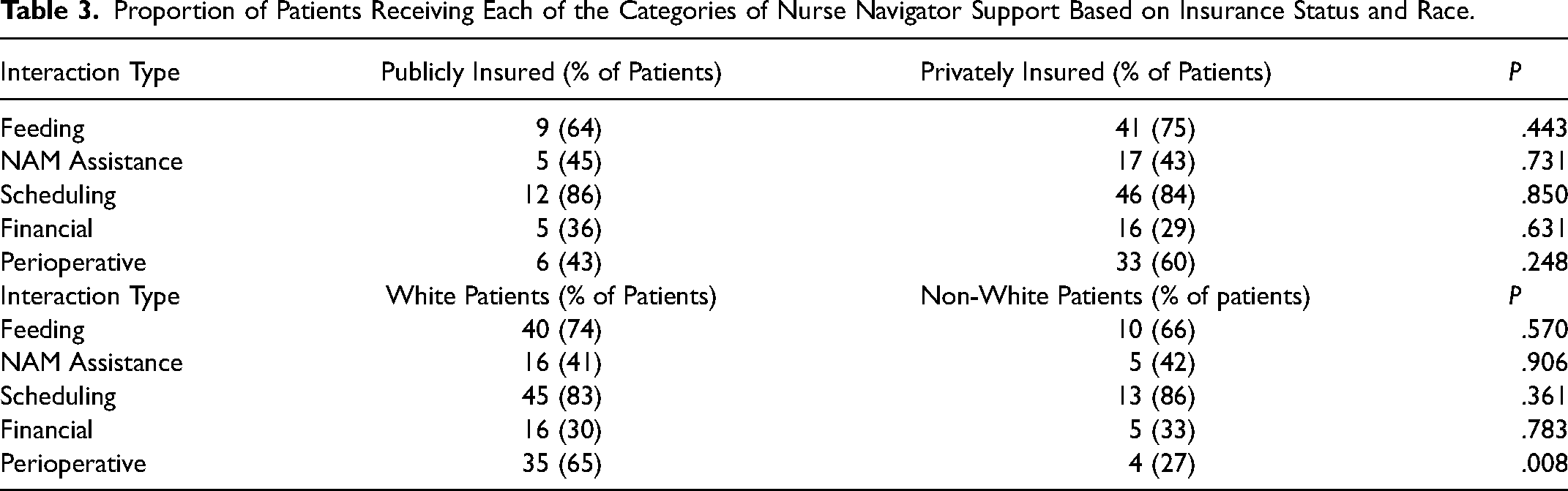
There was no difference in the proportion of families receiving feeding support (P = .443), NAM assistance (P = .731), scheduling assistance (P = .850), financial resources (P = .631), or perioperative assistance (P = .248) from the CNN on the basis insurance payor status (Table 3). A similar trend was observed for white and nonwhite patients, with the exception that fewer perioperative concerns were addressed with the CNN in nonwhite patients as compared to white patients (27% vs 65%, P = .008, Table 3).
Proportion of Patients Receiving Each of the Categories of Nurse Navigator Support Based on Insurance Status and Race.
There were no differences in mean weight z-score at any time point between white and nonwhite patients and between privately and publicly insured patients in the cohort (P > .05 for all, Table 4). Seventy-one percent (12/17) of patients flagged for poor weight gain received CNN feeding support compared to 72% (35/48) of patients without (P = .854). The average number of feeding support interactions also did not vary between patients flagged for poor weight gain and those who were not (2.6 ± 3.6 vs 1.6 ± 1.8, P = .125).
Weight z-Scores Throughout the First Year of Life for White and Nonwhite Patients as Well as Publicly Insured and Privately Insured Patients.
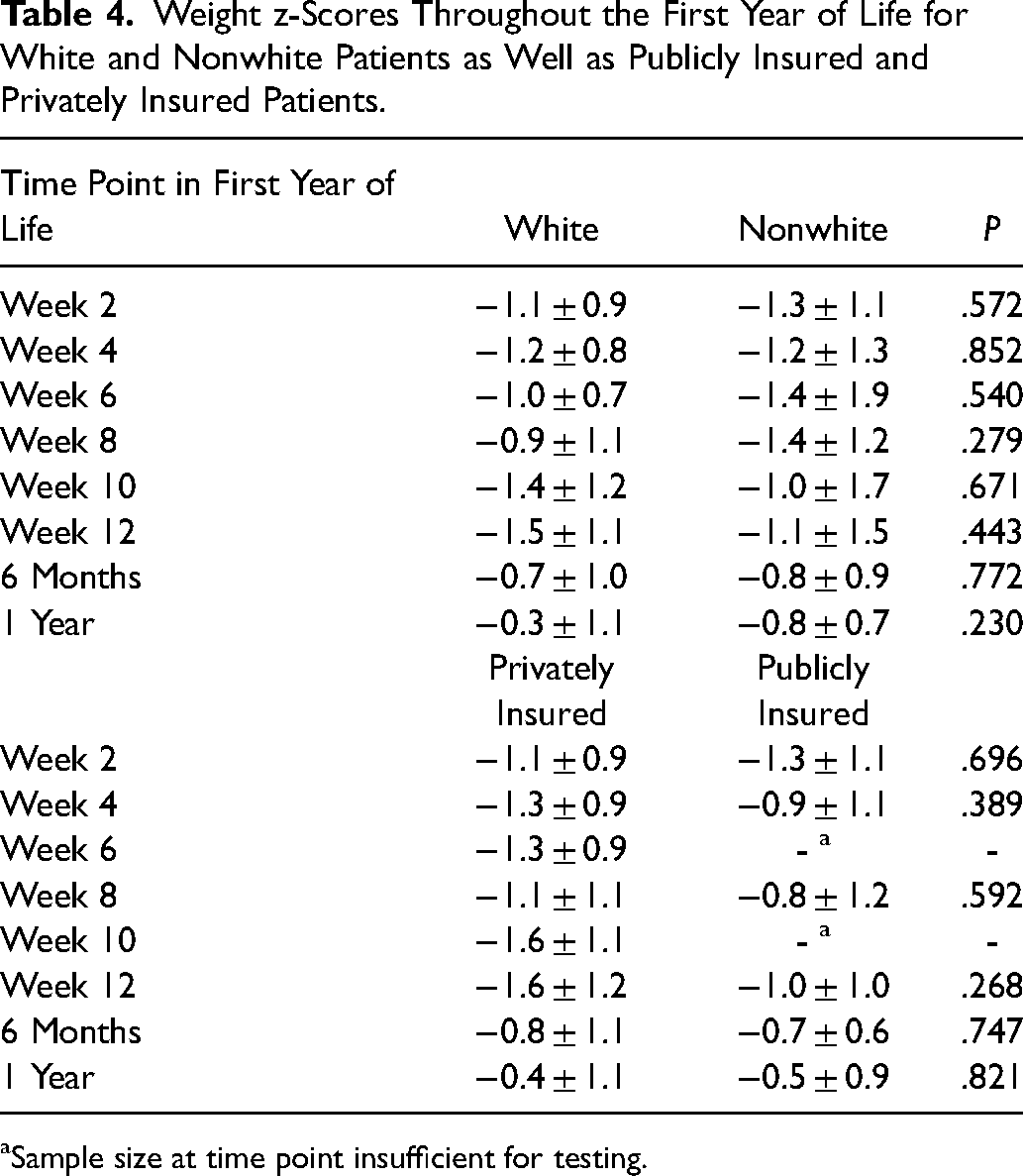
Sample size at time point insufficient for testing.
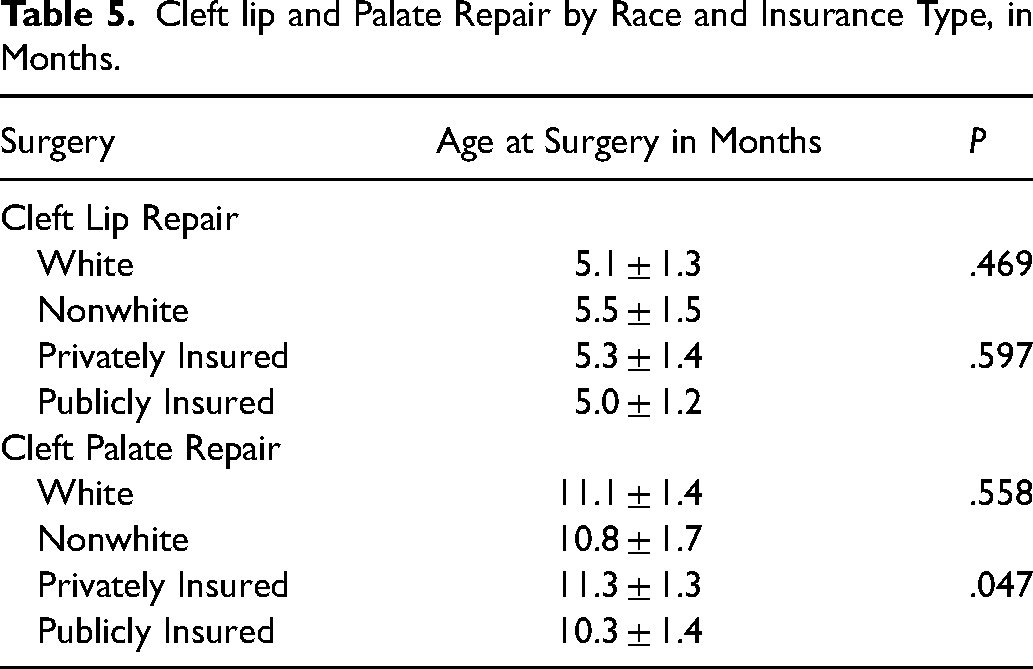
No patient in the cohort underwent tongue-lip adhesion. Average age at cleft lip repair was 5.2 ± 1.4 months. There was no difference in cleft lip repair timing on the basis of race (P = .469) or insurance status (P = .597, Table 5). Patients with public insurance underwent palate repair earlier than privately insured patients (10.3 ± 1.4 months vs 11.3 ± 1.3 months, P = .047). There was no difference in the timing of palate repair between white and nonwhite patients (P = .558, Table 5).
Cleft lip and Palate Repair by Race and Insurance Type, in Months.
Discussion
The introduction of a cleft nurse navigator at our institution has brought about improved equity in the distribution of care services and has been shown to be particularly beneficial to patients and families in marginalized populations. Here, we sought to further describe the specific interventions employed by the CNN which have mediated these trends. The results show the overwhelming majority of patients are assisted early in the first year of life, and that interventions including appointment scheduling and rescheduling, feeding support, and NAM assistance represent the predominant forms of interaction between families and the nurse navigator. Critically, these services were distributed equitably across sociodemographic groups.
By systematically characterizing the family interactions with the CNN, the mechanisms by which minority and publicly insured patients have experienced improved care can be more clearly defined. First, scheduling assistance was the predominant manner by which the nurse navigator interfaced with families. This is notable given prior research showing that patients who are Black or who receive Medicaid insurance have demonstrates higher rates of missed appointments. 22 The stability of a family's social background plays an outsized role in the difficulty of organizing care for patients with cleft conditions, thus the appointment flexibility facilitated by the nurse navigator provides an emotional and functional benefit to families at risk for missing appointments.
Feeding support was another intervention provided by the nurse navigator which is posited to benefit disadvantaged groups, as lower household income has been associated with chronic malnutrition in patients with cleft lip and palate. 38 Previous data from our institution has suggested that initiation of the CNN program brought about improvements in weight gain over the first three months of life, particularly for Black patients and patients on Medicaid. 37 Here, we have noted that weight check-ins and bottle supply shipments by the CNN were equitably distributed between sociodemographic groups, and that over 70% of all patients have interactions with the CNN related to feeding. Further, the prenatal period is an important time for the nurse navigator to provide anticipatory feeding guidance, and 39% of families were seen prenatally. These findings align with a previous report which showed that a quality improvement initiative including patient tracking and increased interim contact decreased the rate of failure to thrive by 10% in patients with cleft lip and palate. 39 Assistance with early feeding technique is particularly important when considering that malnutrition is a risk factor for fistula formation following cleft surgery. 40 While this analysis failed to demonstrate that patients flagged for poor weight gain by z-score received preferential feeding support from the CNN, we were likely underpowered to detect a difference given the overall high rate of feeding support. While this study specifically addressed feeding support in nonsyndromic patients, it warrants mention that syndromic patients and patients with Pierre-Robin sequence are at high risk for feeding difficulties and failure to thrive.41,42 These patients were excluded from analysis because many receive support with inpatient feeding teams. Still, the CNN routinely assists families of patients with milder presentations, and these are particularly important groups to follow given the elevated risk.
It is of note that a category where CNN services were not observed to be equitably distributed was in addressing the perioperative concerns of families. As mentioned, this category included preoperative instructions for when and where to present on the day of surgery as well as postoperative counseling related to pain, inflammation, fever, and bleeding. This may be explained both by documented trends in the treatment of postoperative pain among minority patients and by provider trust dynamics. Recent evidence supports the idea that both patient and provider factors contribute towards the reduced treatment of postoperative pain among Black and Hispanic patients, with these patients less likely to receive opioids. 43 Additionally, a study has shown that both white and Black laypersons perceive that white patients are more pain sensitive and more likely to report pain than Black patients. 44 Certainly, these implicit and explicit biases impact providers at all levels. Moreover, racial disparities in postoperative care are observed in other areas of pediatric surgery including appendectomy, cholecystectomy, and fracture treatment.45,46 Finally, patient-provider trust may be underlying this trend. Patient-provider trust is multifaceted and is particularly influenced by continuity-of-care. 47 We have previously reported that the CNN program has both increased and consolidated the communication between our cleft team and parents, which is hypothesized to increase patient-provider trust. 37 The observation that perioperative concerns are not equally addressed between demographic groups, however, complicates this. While this is not intentional, it serves as a powerful reminder of both distrust in the medical system and historic lack of outreach to marginalized populations. It is clear there is work yet to be done in ensuring equity in the attention afforded to patients of all backgrounds in the postoperative period.
Still, across appointment scheduling, feeding support, NAM assistance, financial assistance, and consult facilitation, CNN services are equitably distributed between demographic groups. Additionally, weight gain measured through biweekly z-scores and surgical timing were equal between groups in the present cohort, with publicly insured patients even experiencing earlier palate repair than privately insured patients. This provides additional evidence that care coordination services can be distributed equally yet preferentially benefit disadvantaged groups. This idea has been previously supported in literature assessing patient navigation programs for cancer centers and in disease-specific screening efforts.48,49
It is of critical importance to not only describe but also to reduce sociodemographic disparities in cleft and craniofacial surgery. In a systematic review covering health disparities research in plastic surgery through 2019, Baxter et al. noted that nearly 90% of existing literature is in either the detecting or understanding phase. Likewise, in craniofacial surgery most published research has sought to identify delays in care or increases in complications for patients, with a relative scarcity of studies evaluating interventions to address these disparities.37,50 Going forward, it would be of benefit to marginalized populations to continue rigorously assessing and describing interventions aimed at surgical equity. Enhanced recovery after surgery (ERAS) programs, for example, have been shown to eliminate disparities in postoperative length of stay in Black patients undergoing colorectal surgery. 51 ERAS protocols for cleft palate surgery have also demonstrated decreased length of stay and postoperative analgesia, 52 and may show similar promise towards this goal. Further, we will continue to utilize the best possible evidence to optimize our nurse navigator program to offer equitable outreach, family-assistance, and clinical follow-up for all patients.
This work is not without its limitations. First, this study is retrospective, and we are unable to infer direct connections between CNN interventions and patient outcomes. The inclusion criteria was intentionally narrowed to nonsyndromic cleft lip and palate and excluded multiple comorbidities such as Pierre-Robin sequence so as to better capture a normalized timeline of interventions for a specific group of patients. This may limit generalizability of the findings. Finally, due to institutional policy regarding phone data storage, available text communications between the CNN and patient families were limited to August 2020 and beyond, limiting the sample size of available patients and thus statistical power. Still, assessing patients across a single year yielded over 600 interactions and interventions. This was adequate for descriptive purposes and provided a detailed characterization of the CNN program.
Conclusions
At our institution, the initiation of cleft nurse navigator program has improved surgical health equity for patients with cleft lip and cleft palate. We report that the predominant forms of interactions include assistance with scheduling, feeding, NAM, and perioperative concerns. These interventions were to a great extent distributed equally across sociodemographic groups, and likely mediate the improved equity in weight gain and surgical timing amongst patients with cleft lip and palate at our institution. The results also provide direction for future improvement, particularly toward ensuring that all populations of patients have their needs addressed in the perioperative period.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.