
Abstract
Objectives
This study investigated the association of MSX1 gene variants rs3821949 and rs12532 with nonsyndromic cleft lip and/or palate (NSCL/P) in the Pakistani population.
Design
Comparative cross-sectional study.
Methods
One hundred (n = 100) subjects with NSCL/P and n = 50 unrelated healthy controls were enrolled in a multicenter comparative cross-sectional study. A tetra amplification refractory mutation system (ARMS) polymerase chain reaction (PCR) was performed to analyze MSXI gene single nucleotide variants (SNVs).
Results
Among 100 NSCL/P subjects, the majority were males (56%; male: female = 1.27: 1). Most of the cases (74%) had cleft lip and palate (CLP) compared to isolated clefts. Genotyping of MSX1 gene variant rs3821949 showed an increased risk for NSCL/P in various genetic models (P < 0.0001), and the A allele exhibited a more than 4-fold increased risk among cases (OR = 4.22: 95% CI = 2.16–8.22; P < 0.0001). Our investigation found no significant difference between the rs12532 variation and NSCL/P.
Conclusion
Our study findings suggest that MSX1 gene variants may increase predisposition to NSCL/P in the Pakistani population. Further studies comprising large samples are required to identify the genetic aetiology of NSCL/P among our people.
Keywords
Introduction
Cleft lip and palate (CLP) are frequent congenital anomalies due to abnormal growth or fusion of facial prominences during early embryologic development. Though CLP's complex and multifactorial aetiology implicates genetic and environmental factors, its pathophysiology is poorly understood, and several molecular pathways have been linked to its pathogenesis. 1 The incidence of CLP differs by racial, geographic, and socioeconomic factors, where Asian and American Indian populations have shown higher and African people have lower incidence risk.2,3 Orofacial clefting can be characterized as nonsyndromic or an isolated defect, occurring in ∼85% of cleft lip and/or palate cases and approximately 45% of solitary cleft palate cases. Nonsyndromic solitary cleft palate appears in around 1/2500 live births. In contrast, the incidence of nonsyndromic cleft lip and/or palate (NSCL/P) is comparatively higher at about 1/1000 live births and reported as 1.20 in Chinese, 1.18 in Japanese, and 1.22 in other Asian countries. In Pakistan, overall incidence for orofacial clefts is documented to be 1.91 per 1000 births (one per 523 births); however, nonsyndromic orofacial cleft incidence is not reported. Syndromic clefting occurs in about 150 chromosomal syndromes, over 300 Mendelian single-gene disorders, teratogen exposure, antiepileptic medications, and specific uncategorized syndromes.4–7
Numerous genetic and epidemiologic methodologies have been used to find aetiological factors, particularly candidate gene studies, yielding the most intriguing results. The association between the muscle segment homeobox gene (MSX1) with NSCL/P has been repeated the most frequently among these potential genes and has been found as a risk factor for craniofacial anomalies including NSCL/P, NSCLO, and CPO. 8 The MSX1 gene spans chromosome 4p16.2 and consists of two exons; both represent the 5'-and 3'-terminal UTR regions and contain 912 bases that encode 303 amino acids. 9
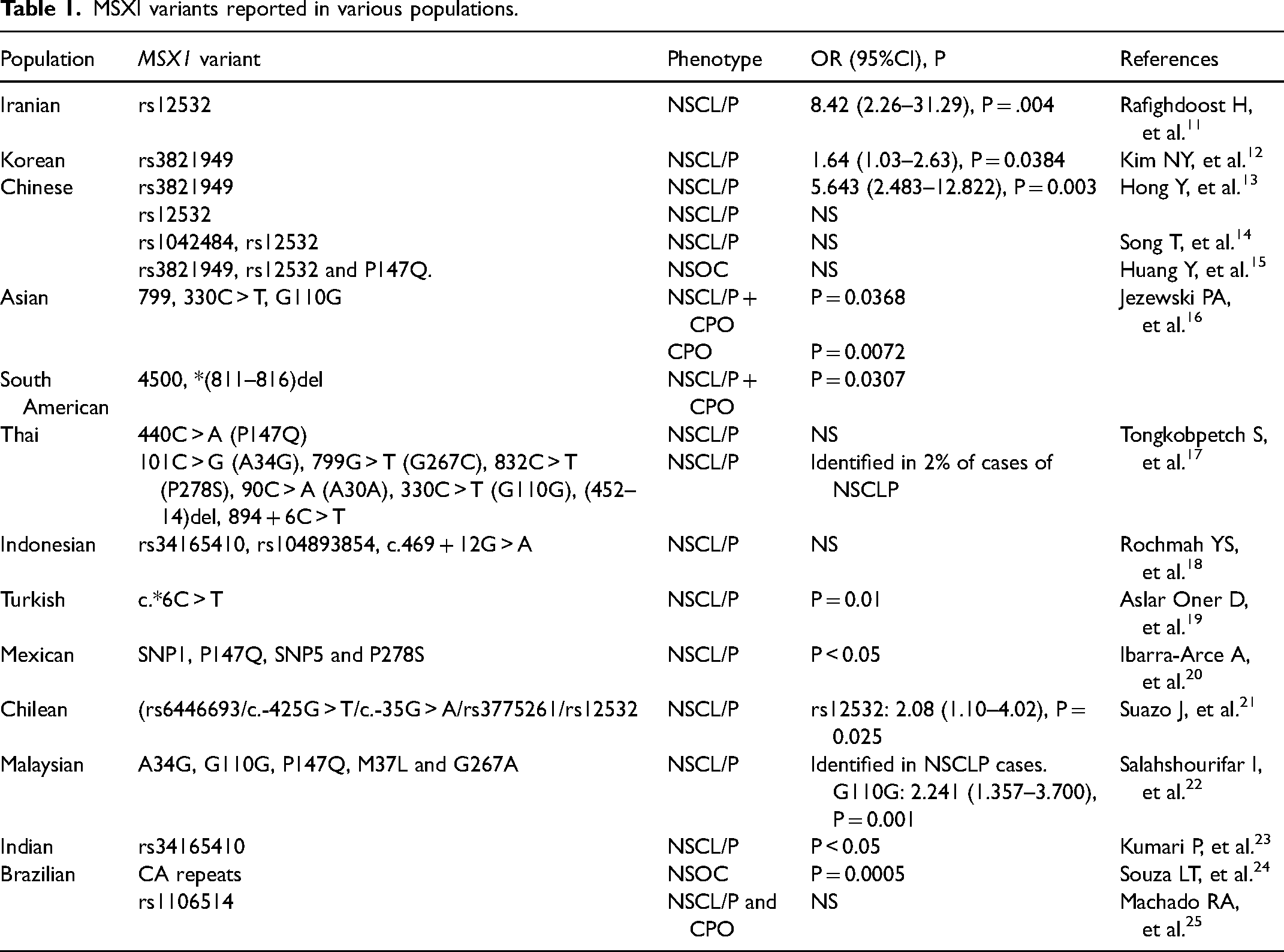
The MSX1 gene is crucial for teeth and craniofacial development. The MSX1 gene knock-out mouse models demonstrated a cleft palate, abnormal maxillary growth, and the absence of an alveolar process. Various studies have shown a link between oral clefts and the MSX1 gene across many populations,1,10 (Table 1). However, this association has yet to be identified among the Pakistani people. The present study investigated MSX1 gene variants rs3821949 and rs12532 to find their association with NSCL/P among the Pakistani population.
MSXI variants reported in various populations.
Materials and Methods
Study Design and Participants
The study was approved by Ethical Review Committee, of the institute. It was a multicenter comparative cross-sectional study; unrelated cases of NSCL/P and healthy controls were recruited from various hospitals of the region. The research was conducted from January 2018 to December 2020 after acquiring written informed consent from the participant's guardians.
Inclusion and Exclusion Criteria
After complete clinical evaluation, plastic surgeons diagnosed the NSCL/P subjects to exclude developmental disorders and syndromes associated with CLP, such as congenital heart defects, congenitally missing teeth, and limb malformations. The healthy controls were of Pakistani origin with no known familial history of the orofacial cleft.
Selection of MSX1 Gene Variants and Sample Size:
Two variants, rs3821949 an intergenic variant (g.chr4:4858675) and rs12532 a 3’-UTR variant (g.chr4:4863419) of gene MSX1 were chosen based on their association with NSCL/P in other populations.12,26,27 As MSX1 gene has been found as a risk factor for NSCL/P, nonsyndromic cleft lip only (NSCLO), and cleft palate only (CPO),16,28,29 all types were included in our study. Secondly, there is limited data on the potential role of genetics aetiology of orofacial clefts in the Pakistani people, and the association of the MSX1 gene has not been investigated previously in our population. According to 1000 Genomes project, the allele frequencies of rs3821949 in South Asian population are G = 0.829 and A = 0.171; whereas for rs12532 allele frequencies in Pakistani Punjabi's are reported as A = 0.74 and G = 0.26. Using the openepi online tool (https://www.openepi.com/), the sample size was calculated based on the incidence reported in previous studies in Pakistan (1.91/1000 births) and Asia (1.33/1000 births).4,30 The parameters for sample size were incidence rate = 1.91, N = 1000, 95% confidence level, and, design effect = 1. The minimum sample size estimated was n = 29; however, to increase the confidence, sample size was increased to n = 150 (n = 100 cases of NSCL/P and n = 50 healthy controls without CLP). This sample size was able to achieve more than 80% power on the minor allele frequency of MSXI variant rs3821949 from our study results (cases = 0.36, controls = 0.12). Power calculation were done on OSSE sample size and power estimator (http://osse.bii.a-star.edu.sg/calculation2.php).
Sample Collection, DNA Extraction and Tetra-ARMS PCR Analysis:
Peripheral blood (5 mL) was collected from NSCL/P subjects and controls. DNA was extracted by inorganic process, as reported by Waryah AM et al. 31 DNA concentration and purity were determined by spectrophotometer and agarose gel electrophoresis.
Tetra primers for amplification refractory mutation system (ARMS) polymerase chain reaction (PCR) were designed (Supplemental Table 1) for genotyping MSX1 gene variants (rs3821949 and rs12532) using the online tool Primer 1 (http://primer1.soton.ac.uk/primer1.html). The specificity was validated by the UCSC tools In-Silico PCR and Blat (https://genome.ucsc.edu/). The PCR master mix (20 μL) contained genomic DNA (2 μL), MgCl2 buffer (2 μL) 2.5 mM for rs12532 and 2.0 mM for rs3821949, 0.125 mM dNTPs (2 µL), a pair of outer primers (1 µl), pair of inner primers (2 µl), Taq Polymerase (0.6 µL) and deionized distilled water (7.4 µL). The PCR program encompassed initial denaturation at 95 °C for 2 min, denaturation (30 cycles) at 95 °C for 30 sec, annealing (62 °C for rs12532 and 67 °C for rs3821949) for 40 sec, extension at 72 °C for 50 s and a final extension at 72 °C for 5 min. The products were separated on a 2% agarose gel and visualized on the Bio-Rad gel documentation system (Figures 1 and 2).
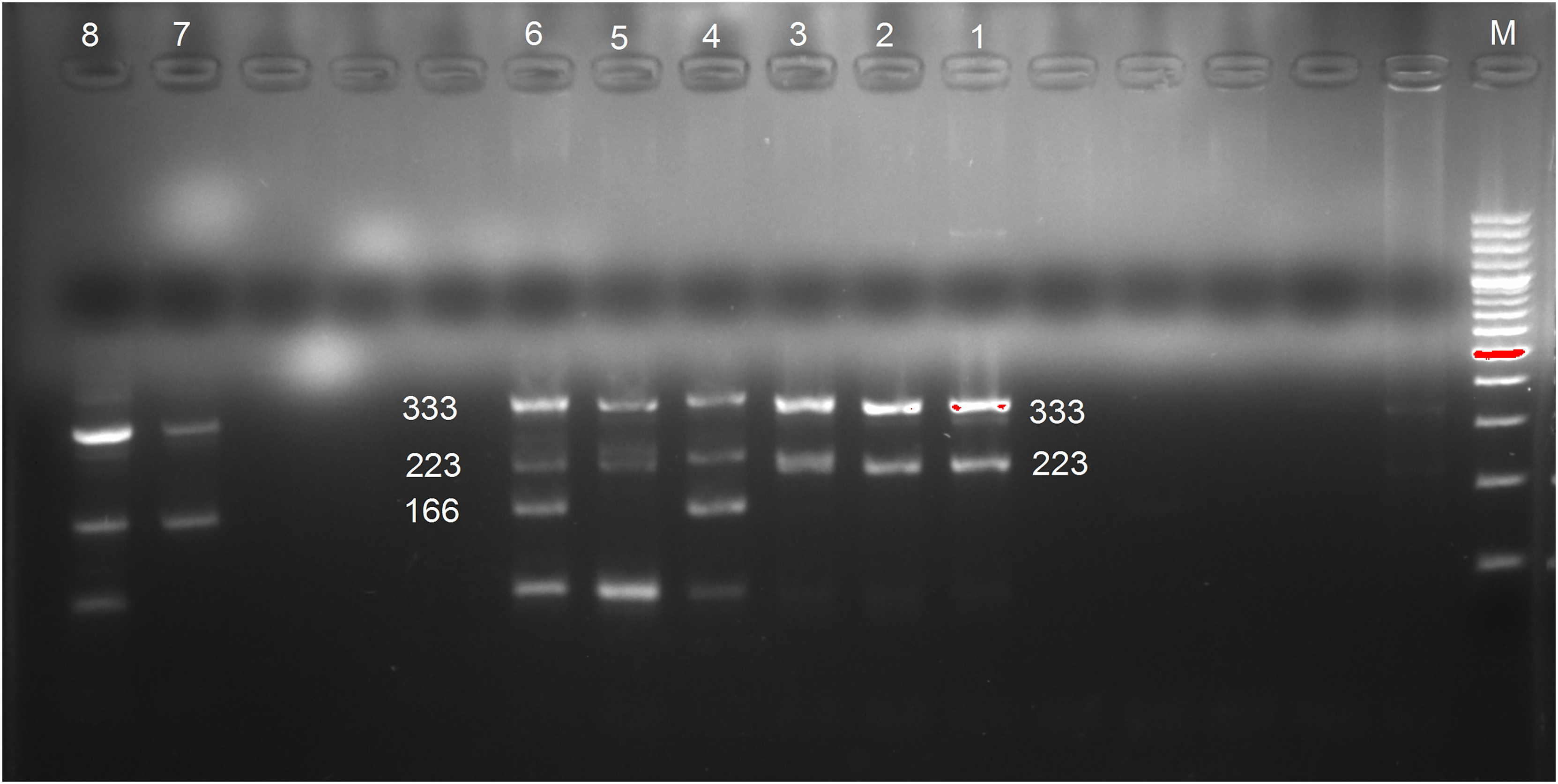
Gel images of Tetra ARMS PCR products of MSX1 gene variant rs3821949 showing Homozygous AA, two bands at 333 and 166 (lanes 7 and 8); Heterozygous AG, three bands at 333, 223 and 166 (lanes 4 and 6); Homozygous GG, two bands at 333 and 223 (lanes 1, 2, 3 and 5).
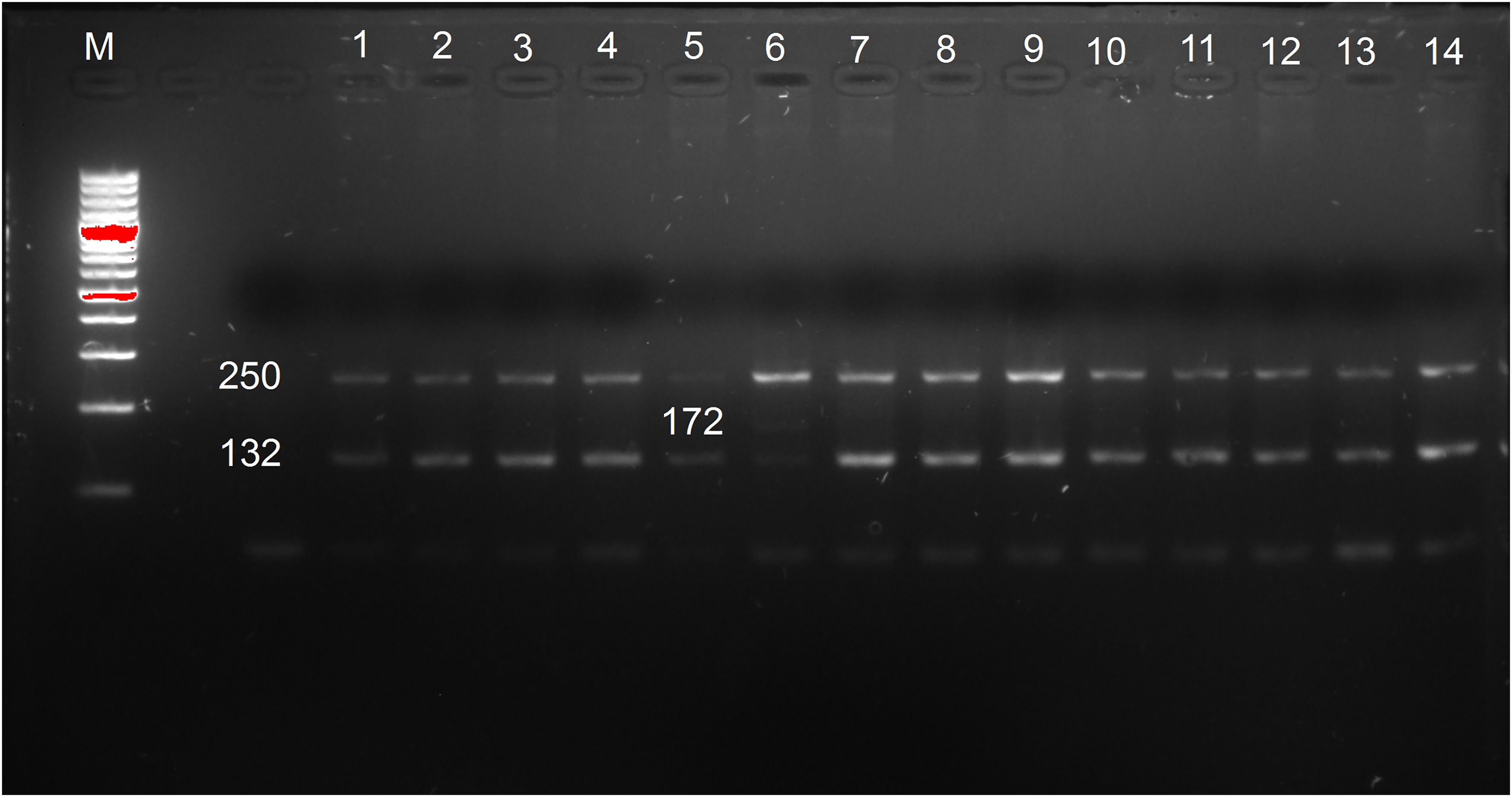
Gel images of Tetra ARMS PCR products of MSX1 gene variant rs12532 showing Heterozygous AG, three bands at 250, 172 and 132 (lane 6); Homozygous AA, two bands at 250 and 132 (lanes 1–5 and 7–10).
In general, the annealing temperature range falls between 55°C and 72°C. However, the higher GC content requires higher melting and annealing temperatures due to the stronger three hydrogen bonds in the G-C pair, as opposed to only two hydrogen bonds in the A-T pair. 32 In the current study, the %G∼C content of rs3821949 variant primers is 50%, which may account for the high amplification temperature. A lower annealing temperature led to nonspecific amplification or no PCR products, while an optimized temperature of 67°C provided good discrimination. Random representative samples were Sanger sequenced by using the outer primers to check the validity of the newly developed tetra primer ARMS assay. And the results of both were 100% concordant. Reactions were successfully genotyped with a genotype call rate of 100%. The method's reproducibility was determined by running a few samples in three independent PCR reactions on different days, and complete concordance between each test was observed. If the genotyping results were ambiguous, the samples were re-tested in duplicates until a precise genotype was determined. During the process of cross-validation, no errors in genotyping were detected.
Statistical Analysis:
Frequency/percentage of categorical variables (age, gender, alleles, and genotypes) and Chi-square were analyzed by using IBM SPSS v.23.0. The Hardy-Weinberg equilibrium (HWE) and haplotype frequencies were estimated. The association of MSX1 gene variants with NSCL/P was determined under different genetic models. The odds ratio (OR) and 95% confidence interval (CI) were determined under a logistic regression model to observe the association of genotypes and haplotypes with NSCL/P by using the online software SNPStat. 33 Taking into account the number of comparisons conducted, Bonferroni correction was used to account for statistically significant values. The Bonferroni correction reduces P-value to 0.00357 (0.05/14 comparisons). To assess the false positive association, 1,000,000 Permutations P* value was calculated by Haploview v.4.2 software.
Results:
Socio-Demographic and Clinical Characteristics
The mean age of the mothers of NSCL/P subjects at the time of pregnancy was 29.7 ± 5.9 years; n = 52 (52%) were between 20 and 30 years of age, n = 43 (43%) were between 31 and 40 years of age, n = 4 (4%) were more than 40 years old and only one was below 20 years of age. In our study, CLP was the more frequent n = 74 (74%) type compared to the isolated cleft lip n = 15 (15%) and isolated cleft palate n = 11 (11%). The gender distribution among NSCL/P subjects showed that n = 56 (56%) were males and n = 44 (44%) were females (male: female = 1.27: 1). The gender distribution and cleft types showed no association (P = 0.50). Among 100 subjects of NSCL/P, the majority (31%) were second-born, 28% had a fourth or more birth order, followed by first-born (21%) and third-born (20%).
Genotype and Allele Distribution of MSX1 Gene Variants
The allele and genotype distribution of the MSX1variants rs3821949 and rs12532 are shown in Table 2. The HWE was estimated for the genotype distributions of the two SNVs, and no deviation was observed in both group (P > 0.05).
Allele and genotype frequencies of MSX1 variants and their association with nonsyndromic cleft lip and/or palate.
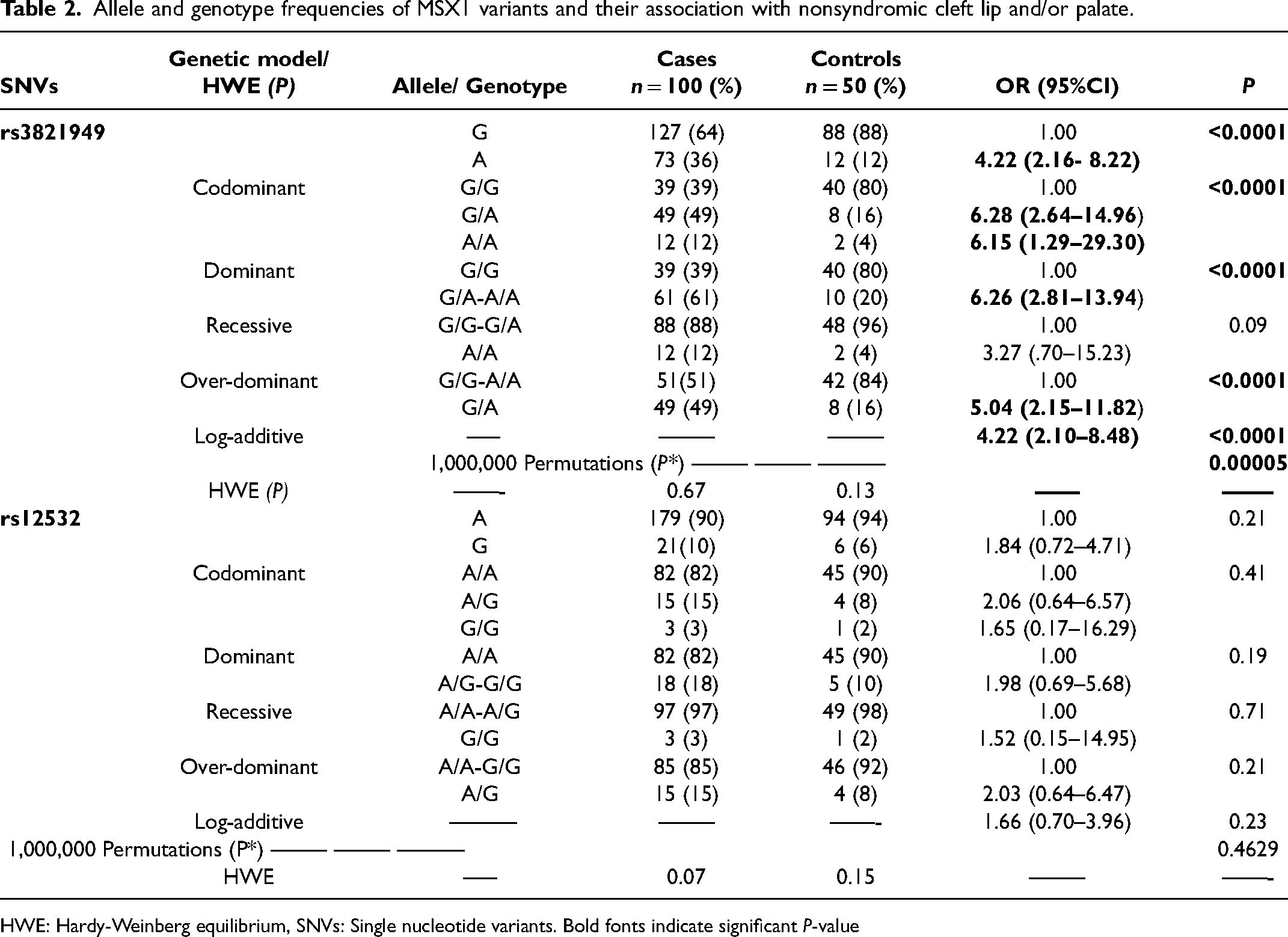
HWE: Hardy-Weinberg equilibrium, SNVs: Single nucleotide variants. Bold fonts indicate significant P-value
The rs3821949 variant frequency distribution for genotypes was 39% homozygous for the G allele, 49% heterozygous, and 12% homozygous for the A allele. The A allele of the rs3821949 variant exhibited increased risk for NSCL/P (OR = 4.22: 95% CI = 2.16–8.22; P < 0.0001). The rs3821949 variant showed a significant association with NSCL/P. It increased the risk under codominant (GA/GG: OR = 6.28, 95% CI = 2.64–14.96, AA/GG: OR = 6.15, 95% CI = 1.29–29.30; P < 0.0001), dominant (OR = 6.26, 95% CI = 2.81–13.94; P < 0.0001), over–dominant (OR = 5.04, 95% CI = 2.15–11.82; P < 0.0001) and log-additive (OR = 4.22, 95% CI = 2.10–8.48; P < 0.0001) genetic models (Table 2). The rs3821949 variant remained significantly associated with NSCL/P after applying Bonferroni correction and, 1,000,000 Permutations test.
For rs12532, the frequency distribution for AA, AG, and GG genotypes among cases was 82%, 15%, and 3%, respectively. We did not find any significant association of the rs12532 variant with NSCL/P in our population. The A-A haplotype of MSX1 rs3821949 and rs12532 SNVs are significantly associated with NSCL/P. It increased the risk by more than 3-fold (OR = 3.52, 95% CI = 1.74–7.15, P = 0.0006) (Table 3).
Haplotype frequencies of MSX1 gene variants and linkage disequilibrium analysis.
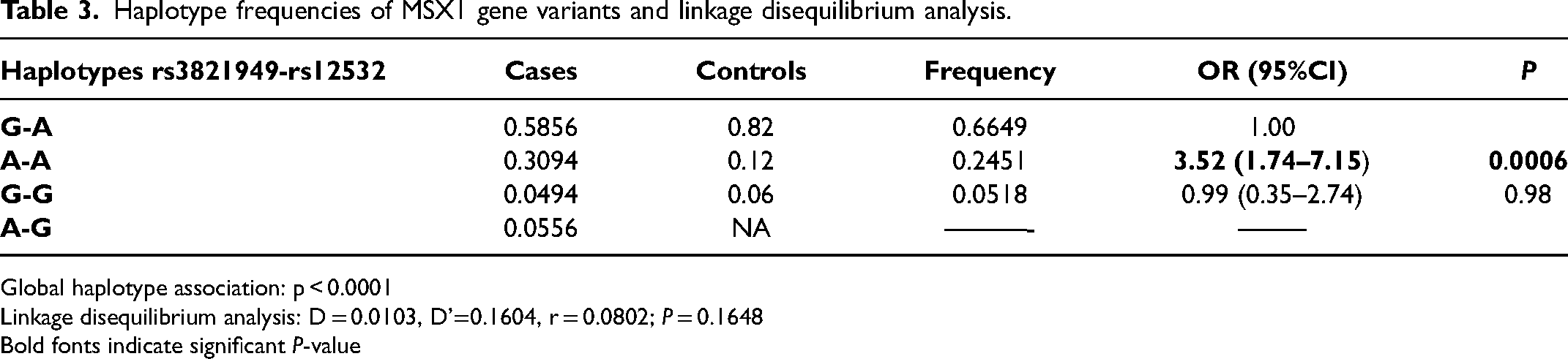
Global haplotype association: p < 0.0001
Linkage disequilibrium analysis: D = 0.0103, D’=0.1604, r = 0.0802; P = 0.1648
Bold fonts indicate significant P-value
Discussion
The ecto-mesenchymal interactions with the series of transcription factors are essential for forming craniofacial structures. MSX1 and MSX2 belong to the homeobox MSX gene family with partially overlapping expression patterns in the embryonic craniofacial area. MSX1 is important to palatogenesis and odontogenesis due to its role as a transcriptional repressor. Furthermore, it is responsible for the growth of limbs, the neurological system, and the inhibition of tumor growth. MSX1 variants in humans exhibit pleiotropic phenotypes related to NSCL/P, nonsyndromic tooth agenesis, and Witkop and Wolf-Hirschhorn syndrome.34,35
The genetic diversity of the Pakistani population has made it an outstanding resource for studying the relationship between genes and disorders. The Pakistani population is comprised of over 18 ethnicities and 60 languages. All the ethnic groups have different genetic lineages, resulting in genetic heterogeneity. Among the major ethnicities, Punjabis have a complex admixture of South Asian, East Asian, and West Eurasian lineages; Pathans, Baloch, and Sindhis share alleles with Greeks and Georgians, and Urdu speakers have heterogeneous Indian ancestry. Thus, genetic variations in the Pakistani population show significant differences in the risk of developing various disorders and disease progression.36,37 Despite numerous genetic studies in various populations,14,38,39 no study in the Pakistani population has identified the association between the MSX1 gene variants and NSCL/P. The MSX1 gene is a putative candidate gene implicated in the processes that cause orofacial clefts. The single nucleotide variations of this gene are linked to the etiopathogenesis of 2% of all nonsyndromic clefts. The MSX1 gene is mainly responsible for secondary palate formation, and variations within the gene cause isolated cleft palates. But due to the complex aetiology and gene-to-gene interaction, the influence may rise to more than 9-fold, resulting in almost 20% of the causes of clefts.40,41 In the present study, we found an association of MSX1 SNV rs3821949 with NSCL/P in Pakistani cases. This variant raised the risk of NSCL/P more than 6-fold in cases.
In contrast, the A-A haplotypes of the selected variants increased the risk by more than 3-fold in cases compared to controls. Our results agree with the study conducted among the Korean population that exhibited a positive association between rs3821949 and cleft of the nose, lip, and palate. 12 Fallen MD et al. 37 revealed a noticeable linkage between MSX1 variants and oral clefts. Furthermore, Hong et al. 13 estimated a noticeable difference in genotypes for rs3821949 between NSCL/P cases and controls. Still, the variation was not significant for rs12532.
In contrast to our study findings, Hong et al. did not demonstrate a haplotype association of both variants with NSCL/P in an Uyghur population of China. An isolated cleft lip was associated with MSX1 gene variants, and the study showed an increase in cleft susceptibility due to gene-gene interaction among the South American population. 40 The findings of Song T et al. 14 supported the genetic association of candidate genes, paired box 9 (PAX9) and interferon regulatory factor 6 (IRF6) among NSCL/P Chinese cases. Still, they ruled out the role of MSX1 gene variants.
Our population did not detect a significant association between NSCL/P and the rs12532 variant. Huang YQ et al. 15 reported concordant results and showed that the rs12532 variant and NSCL/P are not associated. As opposed to our findings, the rs3821949 variant was not related to NSCL/P in the Han Chinese population of Western China; conversely, the P147Q MSX1 gene variant was significantly associated with the disease; suggesting the potential role of the MSX1 gene in the etiopathology of NSCL/P. On the contrary, Hooshang et al. 11 showed a significant association of rs12532. They found a more than 2-fold risk for NSCL/P in the Iranian population with the AG genotype and more than 8-fold with the GG genotype. In that study, the gene MSX1 rs3775261 variant was not found as a risk factor. The disparities between the findings show that gene variations among different ethnicities may influence the susceptibility to NSCL/P.
Increasing maternal age might be attributed to NSCL/P causation.42,43 However, in our study, most mothers (52%) were between the ages of 20 and 30. In comparison, 43% were between the ages of 31 and 40 during the time of their affected child's pregnancy. In the present study, the frequency of NSCL/P was 56% and 44% in males and females, respectively, with a male-to-female ratio of 1.27: 1. Previous studies also suggested a higher frequency of NSCL/P among males as compared to females.44,45 The frequency of CLP was higher (74%) as compared to the solitary cleft lip (15%) or cleft palate (11%) in our study. The distribution of orofacial clefts showed that the majority of the Asian population has NSCL/P with a greater frequency compared to other types. NSCL/P was found in 77.89% of Malay patients, followed by isolated cleft palate (12.87%) and isolated cleft lip (9.8%). Among Chinese, the distribution was NSCL/P (76%), followed by isolated cleft palate (17.3%), and isolated cleft lip (6.5%); and among Indians, NSCL/P (76.92%), isolated cleft palate (23%), and isolated cleft lip (0%). 46 Barbosa Martelli DR et al. 45 reported the more frequent type as CLP (53.4%), followed by isolated cleft lip (26.2%) and isolated cleft palate (20.4%). The study reported the more frequent occurrence of isolated cleft palate among females. In contrast, the CLP and isolated cleft lip were dominated among the male gender. However, we did not find any significant differences. A meta-analysis revealed an association between birth order and CLP. It noted a higher birth order of 3 or more increased the likelihood of the occurrence of clefts, 47 though our study negated the findings.
The present study has certain limitations, including small sample size, and another limitation was recruiting participants from the Sindh province of Pakistan only. As we could not find any genetic study on the MSX1 gene conducted in association with orofacial clefts in the Pakistani population, its comparison with other studies in our population was not possible. Therefore, large-scale studies in other provinces and with other genes are required to investigate the genetic basis of orofacial clefts in the Pakistani people.
Conclusion:
In conclusion, we found that MSX1 gene variant rs3821949 is strongly associated with NSCL/P. The haplotype association further provided strong evidence of genetic etiology among NSCL/P subjects in the Pakistani population. Further investigations comprising large samples are required to validate our findings.
Supplemental Material
sj-docx-1-cpc-10.1177_10556656231185218 - Supplemental material for Association of MSX1 Gene Variants with Nonsyndromic Cleft Lip and/or Palate in the Pakistani Population
Supplemental material, sj-docx-1-cpc-10.1177_10556656231185218 for Association of MSX1 Gene Variants with Nonsyndromic Cleft Lip and/or Palate in the Pakistani Population by Anny Memon, Feriha Fatima Khidri and Yar Muhammad Waryah, Roohi Nigar, Munir Ahmad Bhinder, Ahmed Muhammad Shaikh, Hina Shaikh, Ali Muhammad Waryah in The Cleft Palate Craniofacial Journal
Footnotes
Acknowledgment
The authors thank the research participants, healthcare personnel, and LUMHS Hospital, Jeejal Maa Hospital, Maaji Hospital, and Paretabad Hospital, Hyderabad, for their assistance in collecting samples.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received financial support for the research, authorship, and/or publication of this article: This project was funded by LUMHS Jamshoro, and LUMHS provided all equipment and laboratory supplies Liaquat University of Medical and Health Sciences, Jamshoro, Pakistan.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.