
Abstract
Objective
Optimal Outcomes Reporting was recently introduced to categorize outcomes after cleft palate repair. We seek to propose an expanded version of Optimal Outcomes Reporting and to determine if correlation exists between the expanded outcomes and persistence with team care follow-up through age 9.
Design
Retrospective cohort study.
Setting
Cleft team at large pediatric hospital.
Patients
Patients with isolated nonsyndromic cleft palate (n = 83) born from 2001-2012.
Main Outcome Measures
Patients who continued to present at age 5 or greater were assessed for optimal outcomes. Optimal outcomes were: surgery - no fistula or velopharyngeal insufficiency; otolaryngology - no obstructive sleep apnea or signs of chronic middle ear disease; audiology - no hearing loss; speech-language pathology - no assessed need for speech therapy.
Results
Of the 83 patients identified, 41 were assessed for optimal outcomes. Optimal outcome in any discipline was not associated with follow-up through age 9 (0.112 ≤ p ≤ 0.999). For all disciplines, the group with suboptimal outcomes had a higher proportion of patients from geographic areas in the most disadvantaged quartile of social vulnerability index, with the strongest association in the group with suboptimal speech outcome (OR 6.75, 95% CI 0.841-81.1).
Conclusions
Optimal outcomes and retention in team clinic were not statistically significantly associated, but clinically relevant associations were found between patients in the most disadvantaged quartile of social vulnerability and their outcomes. A patient-centered approach, including caregiver education about long-term care for patients with cleft palate, would allow for enhanced resource utilization to improve retention for patients of concern.
Introduction
Outcomes after cleft palate repair are reported with significant heterogeneity, 1 in large part due to variation in operative technique and extent of postoperative follow-up. This heterogeneity is a potential limitation to streamlining payment models for cleft-related care. 2 Optimal Outcomes Reporting (OOR) has recently been introduced as a novel quality metric for objective, value-based reporting of outcomes after repair of isolated nonsyndromic cleft palate. 3 In that study, patients achieved optimal outcome at age 5 if they had a single operation resulting in both velopharyngeal competence and no fistula. That study focused specifically on the surgical outcome in cleft palate.
The necessity of multidisciplinary care for children with special health care needs, including orofacial clefting, was established in the United States in 1987 by Surgeon General C. Everett Koop. 4 The American Cleft Palate Craniofacial Association (ACPA) specifies the parameters for multidisciplinary evaluation and treatment of children with clefts and other craniofacial anomalies 5 and certifies teams using their published standards for approval. 6 Prior work evaluating multidisciplinary outcomes in isolated cleft palate demonstrated median follow-up of only 7 years despite significant utilization of speech therapy, audiology, and otolaryngology services after initial palate repair. 7 We propose extending the OOR concept to outcomes specific to several cleft palate team disciplines.
Socioeconomic factors are inextricably tied to health outcomes and to interactions between patients and the healthcare system, including in patients and families managing cleft lip and palate. 8 Despite the essential nature of multidisciplinary care for patients with clefts throughout growth, attrition can be high. In surveys, patients’ families cited cost and lack of perceived benefit to care as the most common reasons for loss to follow-up. In fact, commercially-insured patients may pay hundreds of US dollars in out-of-pocket costs for a single multidisciplinary team visit. 9
The current follow-up protocol for children with cleft lip and/or palate at our institution does not differentiate follow-up interval based on outcome, and it is possible that lack of perceived benefit of team care is felt by families whose children are doing well. The current study aims to define multidisciplinary optimal outcomes in patients with isolated nonsyndromic cleft palate at 5 years of age. In addition, we seek to correlate optimal outcomes with retention to follow-up in team clinic through 9 years of age. Finally, we explore associations between optimal outcomes and demographic and socioeconomic factors.
Methods
Institutional Review Board approval (Washington University IRB #201810044) was obtained prior to the study, and patient/caregiver informed consent was not required for this study. Children born with isolated nonsyndromic cleft palate from years 2001–2012 were identified in a prospectively maintained cleft team database. All patients underwent primary palatoplasty by 1 of 5 pediatric plastic surgeons at our institution at approximately 10–12 months of age. The date of birth range was chosen to ensure follow-up data through age 9 was available for all included patients. For all patients, demographic data including home address and insurance status was recorded. Patients who were retained to follow-up through age 5 or greater were assessed for optimal outcomes. Patients lost to follow-up between cleft palate repair and age 5 were excluded from further analysis. Optimal outcomes defined as: surgery - no fistula or velopharyngeal insufficiency (as previously defined by Meara 3 ); otolaryngology - no obstructive sleep apnea or signs of chronic middle ear disease; audiology - no hearing loss; speech-language pathology - no assessed need for speech therapy. The team visit used to capture optimal outcome data took place within 1 year of the patient's fifth birthday.
After optimal outcome for each discipline was assessed, each patient was assessed for retention to follow-up through age 9. Our protocol recommends 6 team clinic visits between cleft palate repair and age 9. For this analysis, patients with at least 4 team clinic visits in the time between their initial cleft palate repair and age 9 were considered retained to follow-up, and patients with fewer than 4 team clinic visits were considered lost.
Further analysis was performed to identify socioeconomic and other potential barriers to team care, based on the patient's last known home address. Road distance from the patients’ home address to the team clinic was calculated with Google Maps (Google, Mountain View, California, United States). Socioeconomic status was approximated using the 2010 Social Vulnerability Index (SVI). SVI uses United Status census data on poverty, lack of vehicle access, and crowded housing, among others, in each census tract to determine vulnerability and need for resource allocation after natural disasters. 10 SVI as a marker for neighborhood disadvantage has been previously used to demonstrate disparities in trauma outcomes, 11 cardiovascular disease prevalence, 12 and cancer mortality. 13 SVI includes a total of 4 themes contributing to an overall ranking. The overall ranking was used, and patients were grouped into SVI quartiles for this analysis. A similar measure of neighborhood disadvantage, Area Deprivation Index (ADI), has also been described. However, since this analysis included patients born 2001–2012 and ADI data is not available prior to 2015, ADI was not used in this analysis.
Statistical analysis was performed with GraphPad Prism (San Diego, California, United States). Social vulnerability index values range from 0 to 1, with higher values corresponding to greater neighborhood disadvantage. For comparison, patients were split into 2 groups based on SVI - those in the most disadvantaged quartile (SVI 0.750-SVI 0.999), and those in the remaining 3 quartiles (SVI 0.001–0.749). All patients had either Medicaid or commercial insurance. Discrete variables, including outcomes, follow-up status, and insurance status, were compared with Fisher's exact test. Distance from team clinic was compared with the Mann-Whitney U test. A p-value <0.05 was considered statistically significant. Odds ratios are presented with 95% confidence intervals.
Results
Optimal Outcomes at Age 5
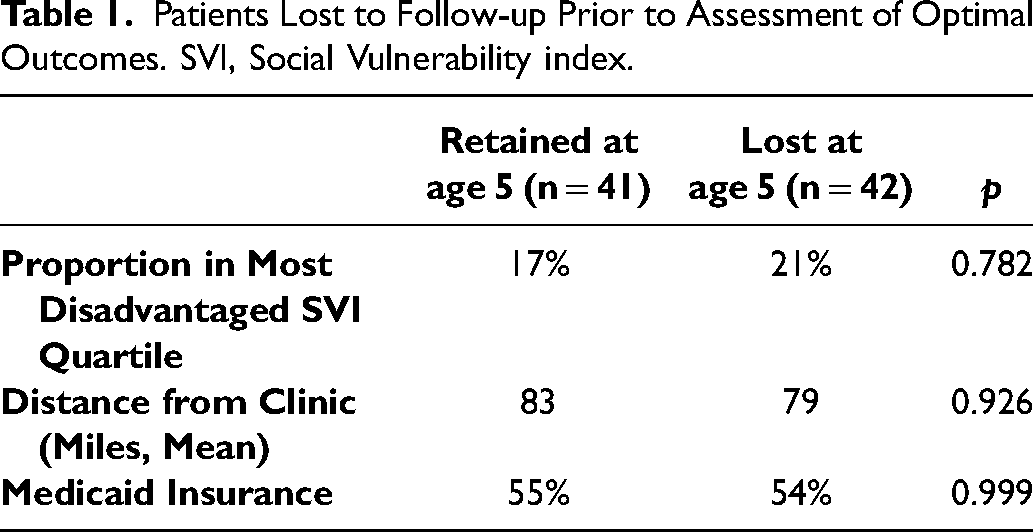
A total of 83 patients born between 2001–2012 with isolated nonsyndromic cleft palate who underwent repair were identified. Of these, 41 had follow-up through the year of their fifth birthday and were able to be assessed for optimal outcomes (Figure 1). The 42 patients lost to follow-up prior to age 5 did not differ from those retained in regard to SVI, distance from clinic, or insurance status (Table 1).
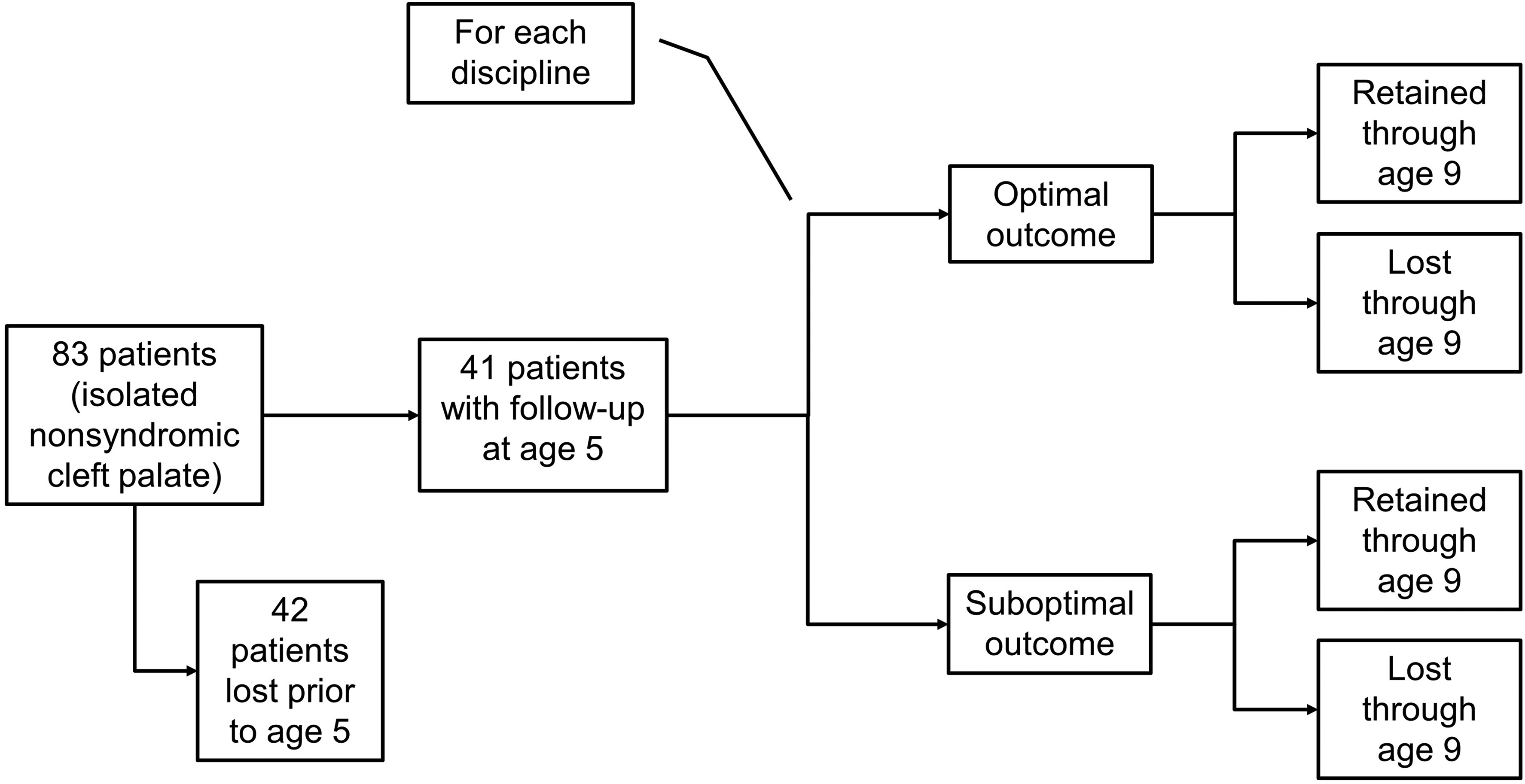
Patients, optimal outcomes, and follow-up retention in isolated nonsyndromic cleft palate.
Patients Lost to Follow-up Prior to Assessment of Optimal Outcomes. SVI, Social Vulnerability index.
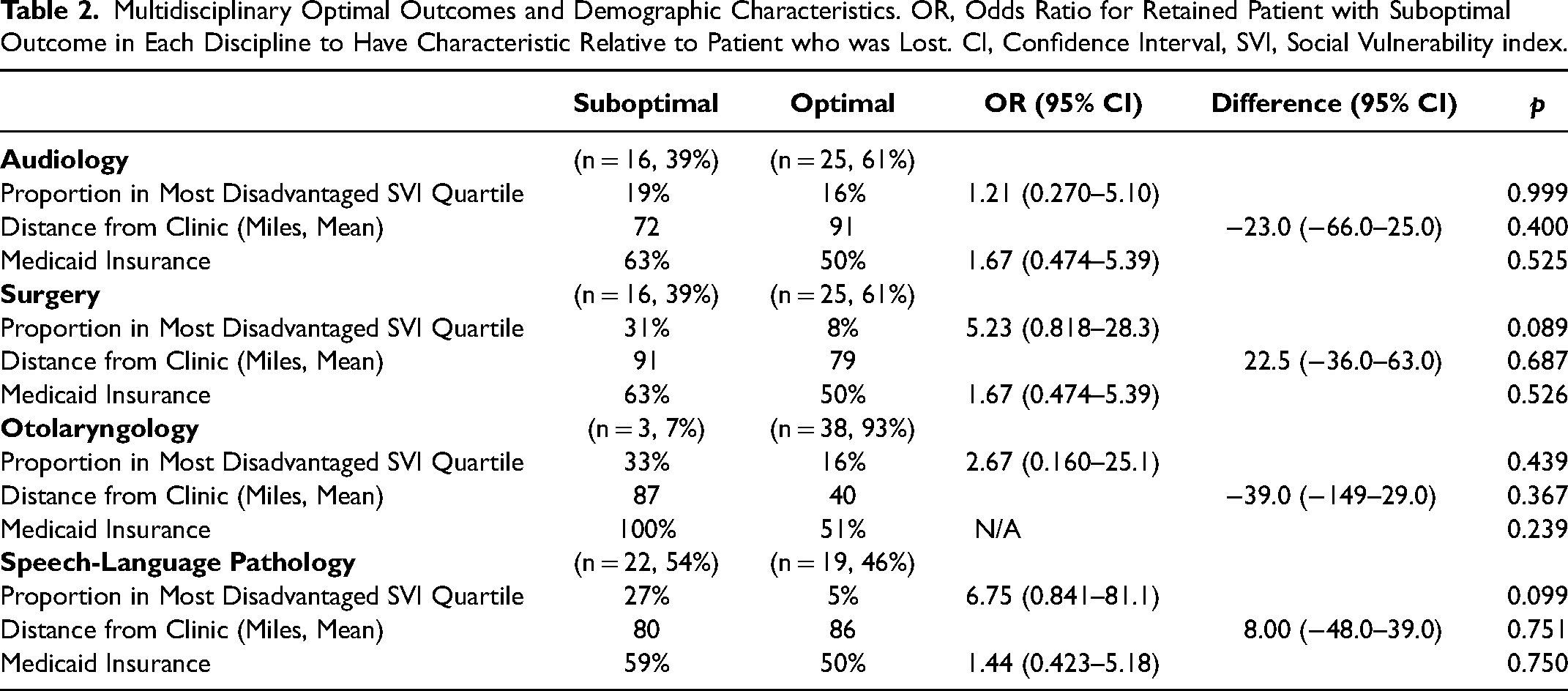
Optimal outcome achievement by discipline ranged from 46%-93% (Figure 2). In all 4 disciplines, the group of patients with suboptimal outcomes had both a higher proportion of patients in the most disadvantaged quartile of SVI and a higher proportion of patients with Medicaid insurance than the group with optimal outcomes (Table 2). However, none of these differences reached statistical significance.
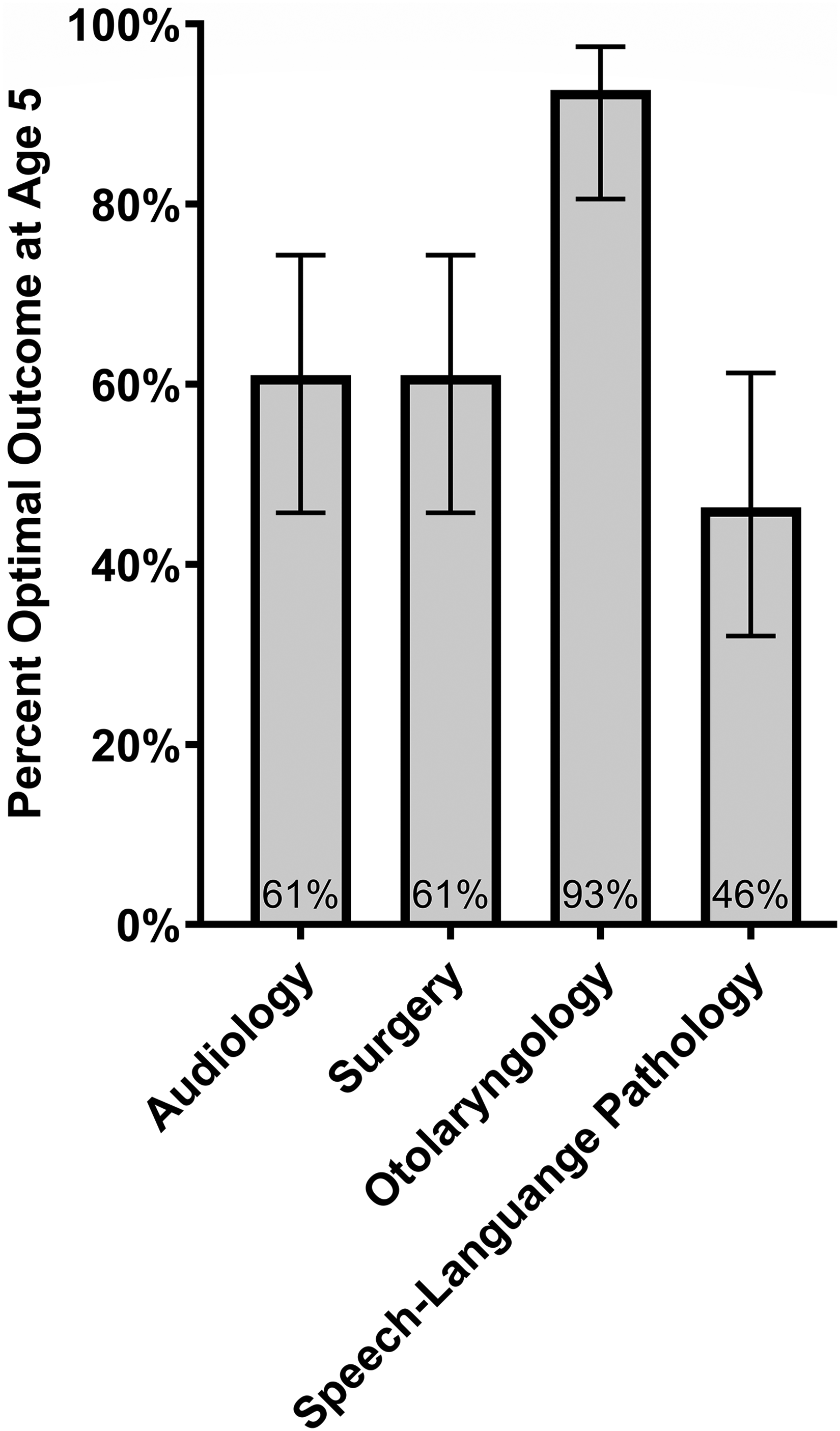
Achievement of multidisciplinary optimal outcomes at age 5. Error bars include 95% confidence interval.
Multidisciplinary Optimal Outcomes and Demographic Characteristics. OR, Odds Ratio for Retained Patient with Suboptimal Outcome in Each Discipline to Have Characteristic Relative to Patient who was Lost. CI, Confidence Interval, SVI, Social Vulnerability index.
Follow-Up at Age 9
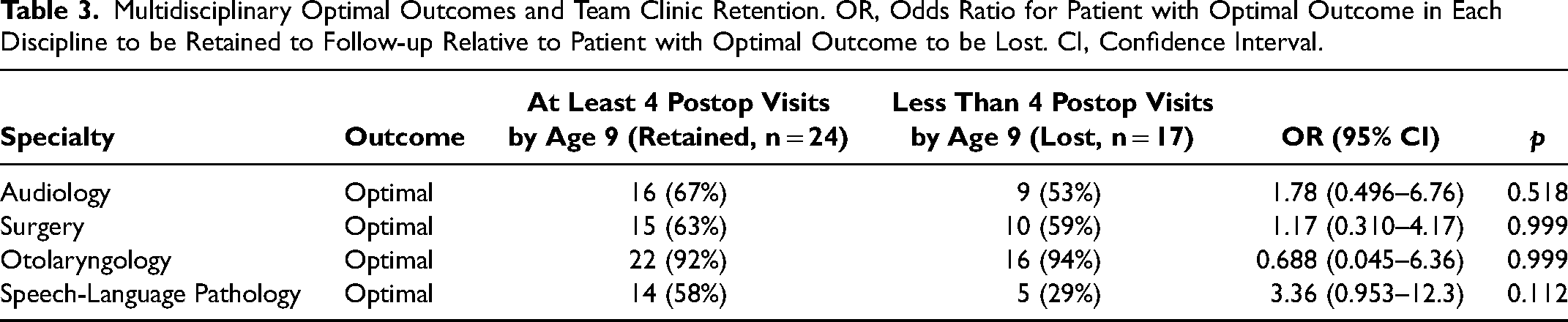
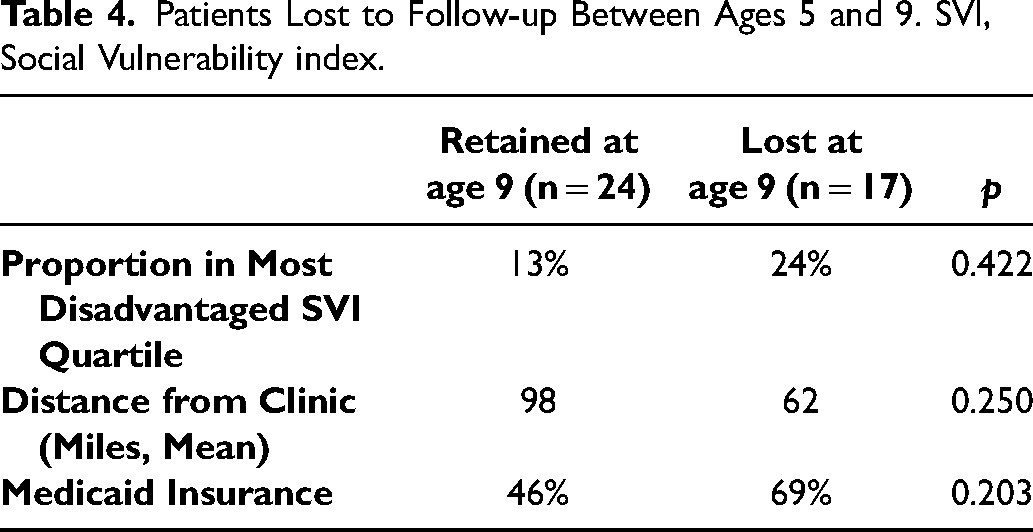
Optimal outcome in any discipline at 5 years of age was not associated with team clinic follow-up through age 9 (0.112 ≤ p ≤ 0.999, Table 3). Overall, patients who were retained at age 9 were more likely to have commercial insurance and not to be in the most disadvantaged quartile of SVI, although these differences were not statistically significant (Table 4).
Multidisciplinary Optimal Outcomes and Team Clinic Retention. OR, Odds Ratio for Patient with Optimal Outcome in Each Discipline to be Retained to Follow-up Relative to Patient with Optimal Outcome to be Lost. CI, Confidence Interval.
Patients Lost to Follow-up Between Ages 5 and 9. SVI, Social Vulnerability index.
Discussion
Our population of patients with nonsyndromic isolated cleft palate showed significant heterogeneity in outcomes. Our population had a similar rate of optimal surgical outcome (61%) to the isolated cleft palate population (72%) previously published by Meara using the same definition. 3 The incidence of chronic middle ear disease and obstructive sleep apnea (ie, suboptimal otolaryngology outcome) was rare in this cohort. The absence of conductive hearing loss (61%, optimal audiology outcome) was less common than the optimal otolaryngology outcome (93%), suggesting a contribution of chronic Eustachian tube dysfunction in some patients not captured in the otolaryngology optimal outcome. Approximately half (46%) of patients avoided need for speech therapy at age 5. The incidence of speech therapy and conductive hearing loss are similar to previously published series.14,15
Previous work has suggested that patients who require dental, psychological, or speech services are more likely to be retained to multidisciplinary follow-up. 7 In this study, outcome at age 5 was not associated with retention or loss to follow-up at age 9. The approximately 50% loss of follow-up by age 5, with about 40% of the remaining patients lost by age 9, is significant attrition that is not explained by optimal outcomes in this population. Likewise, there was not a clear demographic (distance from clinic, SVI, or insurance status) association with loss to follow-up at either time point. The high overall rate of attrition suggests a need for multiple approaches to optimize care delivery. The concept of “minimally disruptive medicine” 16 for patients with complex conditions certainly applies to families navigating management of children with a cleft palate. A core tenet of this concept is individualizing delivery of this care. While team clinic follow-up guidelines offer a guideline for each condition, outcomes and other individual needs may necessitate different frequencies of follow-up. The optimal outcomes concept may allow triage of some patients to 1) more or less frequent follow-up or 2) more or less intensity of follow-up to promote perceived value of team care to families. In addition, continued adoption of telemedicine (which was not offered during the time period of this study) could remove some transportation or childcare barriers to multidisciplinary care. Future work could include patient surveys to elucidate the specific medical, social, and environmental challenges faced by families living in the most disadvantaged areas followed by outreach targeted to SVI.
There was a clinically significant association in this population between speech outcomes and living in an area in the most disadvantaged quartile of SVI. Of patients with optimal speech outcome, 5% lived in a highest-quartile SVI, most disadvantaged area, and of patients with suboptimal outcome, 27% lived in a highest-quartile SVI, most disadvantaged area (OR 6.75, 95% CI 0.841–81.1). Differences in language skill of young children in different family income levels have been published previously. 17 There was a similarly clinically significant association between surgical outcome and living in an area in the most disadvantaged quartile of SVI. Of patients with optimal surgical outcome, 8% lived in a highest-quartile SVI, most disadvantaged area, and of patients with suboptimal surgical outcome, 31% lived in a highest quartile SVI, most disadvantaged area (OR 5.23, 95% CI 0.818–28.3). The need for secondary velopharyngeal surgery and the need for speech therapy may be related. This SVI discrepancy in outcome in patients receiving presumably identical surgical care is dramatic. Outcome differences related to socioeconomic status in cleft care have been noted previously, even in a country with universal health care.8,18
Meara defined Optimal Outcomes Reporting in a population of patients with nonsyndromic isolated cleft palate. 3 By restricting the population to isolated nonsyndromic cleft palate, they minimized the variability introduced by known genetic syndromes, as well as the subjectivity involved in additional surgery for cleft lip and nose revision. However, limiting the included subjects to this subpopulation of patients decreased the sample size for the analyses in this study, and this is also the main limitation of the current work. Additionally, while isolated cleft palate is a good starting point to limit variables for optimal outcomes, it is a largely invisible condition to parents (compared to other craniofacial differences), and this may present an area of particular challenge for follow-up retention in team clinic. While our multidisciplinary team attempts to follow patients with clefts through skeletal maturity, age 9 was chosen as the cutoff to measure follow-up retention in this study. This allowed inclusion of as many patients as possible in the subpopulation of patients with isolated nonsyndromic cleft palate. This limitation, where up to approximately 20 years is necessary to know the “final” outcome of an intervention beyond skeletal maturity, is inherent to the cleft literature. Each multidisciplinary outcome is a cumulative outcome at age 5, but outcomes beyond age 5 are not included in this analysis. It is likely that some patients developed need for speech therapy or VPI, chronic middle ear disease, or hearing loss after age 5. In addition, while patients who requested transfer of their care to another team were excluded from this analysis, it is possible that a suboptimal outcome was diagnosed by an outside provider for an included patient and was not captured in this analysis.
Future related work will focus on defining and studying optimal outcomes for other craniofacial differences, including cleft lip and palate and craniosynostosis. This will necessitate inclusion of outcomes related to psychology, neurosurgery, dentistry, and orthodontics. The need to standardize patient outcome measurements is necessary to promote care that is valuable to patients. 19 Furthermore, this work calls for development of novel strategies to promote equitable cleft care outcomes in patients with different socioeconomic realities, 20 especially as data suggests an association between lower socioeconomic status and increased incidence of clefting. 21
Conclusion
Although associations between optimal outcomes and demographic characteristics were not statistically significant, clinically relevant associations with social vulnerability are present in our population. In an environment with low overall follow-up retention in team clinic for isolated cleft palate, characterizing patients with cleft palate by optimal outcomes may allow resources to be directed to improve delivery of care for patients with the most need.
Footnotes
Acknowledgments
None.
Prior Meeting Presentation
Presented at the 14th International Cleft Congress, Edinburgh, Scotland, July 15, 2022.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.