
Abstract
Objective
To compare osteomeatal complex (OMC) anatomical variations and nasal cavity airway volume between individuals with cleft lip and palate (CLP) and healthy controls using cone beam computed tomography (CBCT).
Design
Retrospective, cross-sectional study.
Setting
Department of dentomaxillofacial radiology.
Patients/Participants
CBCT images of 200 individuals were evaluated: 100 patients with CLP (mean age 13.64 ± 4.32 years) and 100 age- and sex-matched controls (mean age 13.67 ± 4.32 years). Patients with syndromes, maxillofacial trauma, prior orthognathic surgery, or inadequate image quality were excluded.
Main Outcome Measures
Presence of OMC anatomical variations and nasal cavity airway volume.
Results
Agger nasi cells were the most common anatomical variation and hypertrophic turbinates were the most frequent pathology in both groups. Haller cells (p = 0.006) and nasal septal pneumatization (p = 0.001) were more prevalent in controls. In contrast, paradoxical middle turbinate (p = 0.015), nasal septal deviation (p = 0.001), and mucosal thickening (p = 0.001) were more frequent in CLP. Total nasal cavity airway volume did not differ significantly between groups.
Conclusions
Individuals with CLP exhibit distinct OMC anatomical patterns compared with controls; however, total nasal cavity volume is not significantly altered. These findings indicate that regional OMC alterations and overall nasal cavity volume represent related but distinct anatomical constructs.
Introduction
Osteomeatal complex (OMC), which is a key location in the drainage and ventilation of frontal, maxillary and anterior ethmoid air cells, consists of the middle turbinate, the hiatus semilunaris, the maxillary sinus ostium, the infundibulum, the ethmoid bulla and the frontal recess.1-3 Some of the anatomical variations seen in this strategic area may impair mucociliary clearance by interfering with airflow and drainage. It has been stated that concha bullosa, over-pneumatized ethmoid bulla, paradoxical turbinate, Haller cells and Agger Nasi cells are among these anatomical variations that cause stenosis and obstruction, thus creating a suitable basis for the formation of infections and pathologies in the middle meatus. 4 Some studies also suggest that anatomical variations, depending on their size, location or the amount of mucosal contact may play an important factor in the development of pathologies such as chronic sinusitis.5,6
Endoscopic sinus surgery is frequently performed in the treatment of sinusitis cases, one of the leading chronic infections. However, there is a high risk of complications during the surgical procedure due to the very complex and sensitive nature of the region and surrounding important anatomical structures. 7
Studies performed on individuals with cleft lip and cleft palate (CLP), which is one of the leading craniofacial anomalies and can present in various forms (unilateral, bilateral, complete, incomplete), have reported decreased airway dimensions and nasal deformities.8-10 These structural alterations may influence sinonasal anatomy; however, the extent to which CLP is associated with OMC variations and related pathologies remains unclear. While numerous studies have evaluated OMC anatomy in healthy populations1,2,11-30 investigations specifically focusing on the OMC region in individuals with CLP are limited.3,31
Individuals with CLP generally need maxillofacial correction surgery to ensure physiological function. The risk of complications will increase in surgeries performed on patients with CLP due to the altered anatomical structures of the defect regions. To avoid possible complications, it is important to evaluate the defect area with three-dimensional (3D) imaging methods that prevent loss of information due to superpositions, instead of two-dimensional (2D) conventional radiographs. 3D imaging methods such as computed tomography (CT) or cone beam computed tomography (CBCT) help to provide clear information for preoperative evaluation of both the mentioned area, drainage, and ventilation routes. 32 However, CBCT is more advantageous compared to CT due to shorter irradiation time and less radiation dose. 33
This retrospective cross-sectional study aimed to compare the incidence of OMC anatomical variations and pathologies, as well as nasal cavity airway volume, between individuals with CLP and age- and sex-matched healthy controls using CBCT. In addition, we explored whether the presence of OMC variations and pathologies was associated with differences in total nasal cavity volume across the study sample.
Materials and Methods
The study protocol was reviewed and approved by an institutional ethics committee, and the study was conducted in accordance with ethical standards. All individuals with CLP registered in the institutional hospital information and management system were identified. Of 444 registered CLP patients, 151 had CBCT scans including the OMC within the field of view (FOV). After applying exclusion criteria (n = 47) and excluding four scans due to insufficient diagnostic quality, the final CLP cohort consisted of 100 patients. Isolated cleft lip or isolated cleft palate cases were not included. The same exclusion criteria were applied to the healthy control group. About 100 CBCT scans with sufficient diagnostic image quality were selected to achieve age and sex distributions comparable to the CLP group.
All images were obtained with the Planmeca® Promax 3D Mid (Planmeca Oy, Helsinki, Finland, 2012) CBCT device operating at 90 kVp and 10 mA with a reconstructed voxel size of 0.403 mm with two consecutive separate 36 s irradiations, and a FOV area of 16×9 cm2. All images were then combined with the Romexis® software program (Planmeca Oy, Helsinki, Finland) and reconstructed a FOV area of 16×16 cm2. The resulting images were saved in the Digital Imaging and Communications in Medicine (DICOM) format and were directly assessed on a monitor screen ((14 bit, 24-inch, NEC MD 242C2, 1920 ×1200 resolution) (Dell Technologies, Round Rock, TX, ABD)). As this was a retrospective study based on routine clinical imaging, all CBCT scans were obtained using the institution's standardized positioning protocol. Patients were positioned in an upright posture with the Frankfort horizontal plane parallel to the floor and the midsagittal plane perpendicular to the floor.
Anatomical variations of OMC such as ethmoid cell variations (Agger Nasi cell (ANC), Haller cell (HC), over-pneumatized ethmoid bulla (OPEB)), conchae variations (conchae bullosa (CB), paradoxical middle conchae (PMC), second middle conchae (SMC), bifid conchae (BC)), uncinate process variations (uncinate bulla (UB), bifid uncinate process (BUP), uncinate process orientation type (UPOT)), nasal septum variations (deviation (NSD) and pneumatization (NSP)), pathologies of OMC (hypertrophic conchae (HTC), mucosal thickening (MT)) and localization of CLP (unilateral or bilateral) were the parameters evaluated in this study. Representative CBCT examples of HC and NSD are presented in Figure 1.
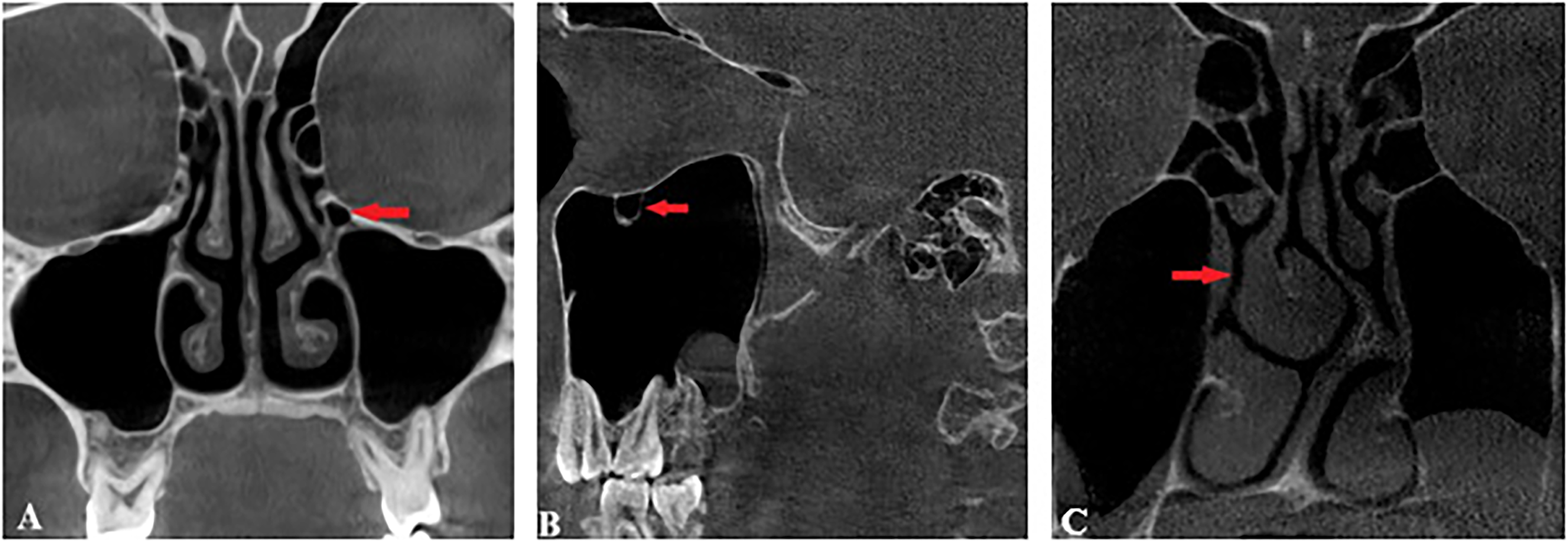
Representative CBCT images demonstrating HC and NSD. (A) Coronal view showing HC (arrow). (B) Sagittal view confirming HC (arrow). (C) Coronal view showing Mladina type 7 NSD to the left with right middle turbinate hypertrophy.
NSD was classified according to the Mladina classification, which categorizes septal deformities into seven types based on characteristic vertical and horizontal patterns observed on CBCT. Type 1 represents a vertical deviation that does not reach the nasal dorsum and does not affect nasal valve function. Type 2 extends to the nasal dorsum within the nasal valve region and may impair valve function. Type 3 corresponds to a vertical deviation reaching the superior portion of the middle turbinate, typically presenting as a C-shaped deformity. Type 4 represents an S-shaped deformity involving both sides. Type 5 describes a horizontal deviation with a septal spur on one side and a straight septum on the other. Type 6 is characterized by a horizontal deformity with a deep anterior groove and an intermaxillary bony crest. Type 7 includes combined deformities involving two or more of the above types. 34
NSP was assessed according to the classification proposed by Mureșan et al., based on its anatomical origin: Type 1 indicates absence of pneumatization; Type 2 originates from the crista galli; Type 3 arises from septal extensions of the frontal sinus; Type 4 represents posterior septal pneumatization of sphenoidal origin; and Type 5 corresponds to pneumatization of the perpendicular plate originating from the ethmoid. 35
Evaluation of nasal cavity volume was calculated by using Mimics® (Research 20.0.0.691, Materialize NV technologielaan 15 3001 Leuven, Belgium) software program. Glupker et al. 36 was taken as a reference when determining the lines for nasal cavity boundaries. The area between the reference lines in axial, sagittal, and coronal sections was calculated as the nasal cavity volume.
This study was conducted within the framework of a postgraduate thesis. Prior to data collection, the observer and a supervising dentomaxillofacial radiologist jointly reviewed representative CBCT scans to standardize the identification criteria for OMC anatomical variations and to define nasal cavity boundaries. Discrepancies were discussed until consensus was achieved. Following this calibration phase, all evaluations were performed by a single observer to ensure methodological consistency across the dataset. Therefore, inter-observer reliability was not calculated. Intra-observer reliability was assessed on 20 randomly selected scans after a two-week interval and demonstrated almost perfect agreement (κ = 0.82), supporting the reliability of the measurements.
A priori power analysis (G*Power) indicated that a total sample of 200 participants (100 per group) would provide >80% power to detect medium effect sizes (w = 0.3) for chi-square comparisons at α = 0.05. SPSS (Statistical Package for Social Sciences) for Windows 20.0 program was used for statistical analysis. Mean and standard deviation values were used as descriptive statistics. Chi-Square and Fisher's exact test were used for the comparisons between groups for qualitative data, and Independent Sample T-test was used for the comparisons between normally distributed groups for quantitative data. Statistical significance was set at p < 0.05 for two-category comparisons and p < 0.01 for chi-square tests involving more than two categories.
Results
CBCT images of a total of 200 individuals, 100 patients with CLP (43 females and 57 males, mean age 13.64±4.315 years) and 100 healthy controls (45 females and 55 males, mean age 13.67±4.318 years) were evaluated.
Among the 100 CLP patients, 73% presented with unilateral clefts and 27% with bilateral clefts. Within the unilateral subgroup, 26% had right-sided clefts and 74% had left-sided clefts.
The most common anatomical variation in both groups was ANC, and the most frequent pathology was hypertrophic turbinates. The frequencies of OMC variations and pathologies in CLP and healthy control groups are summarized in Table 1. Among the statistically significant differences, NSD, MT, and PMC were more prevalent in the CLP group, whereas HC and NSP were more frequently observed in controls.
Comparison of OMC Anatomical Variations and Pathologies Between Groups.
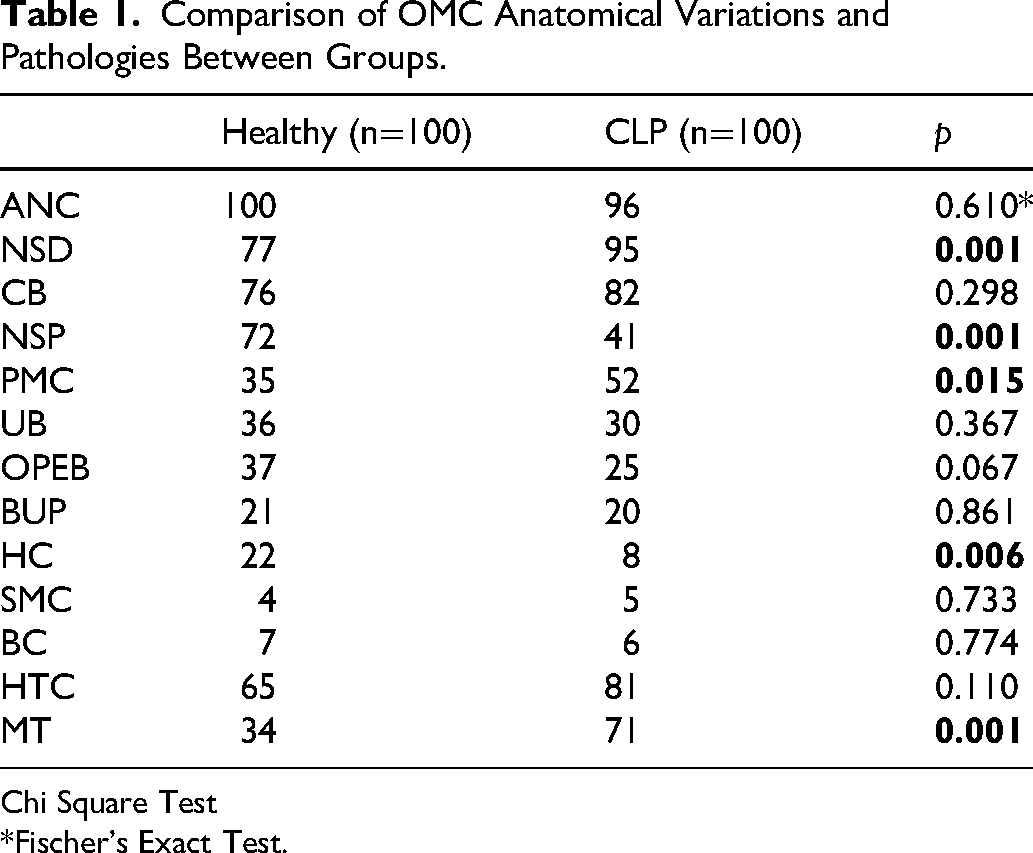
Chi Square Test
*Fischer's Exact Test.
NSD type 7 was the most common septal deviation pattern in both groups, observed in 31% of controls and 71% of individuals with CLP. In the control group, NSD types 1 and 3 were significantly more frequent, whereas NSD type 7 and type 2 were markedly more prevalent in the CLP group (p < 0.001). Regarding NSP, type 1 was significantly more common in controls, while types 4 and 5 were more frequently observed in individuals with CLP (p < 0.001). The distribution of NSD and NSP types is presented in Table 2.
Evaluation of the NSD and NSP Types.
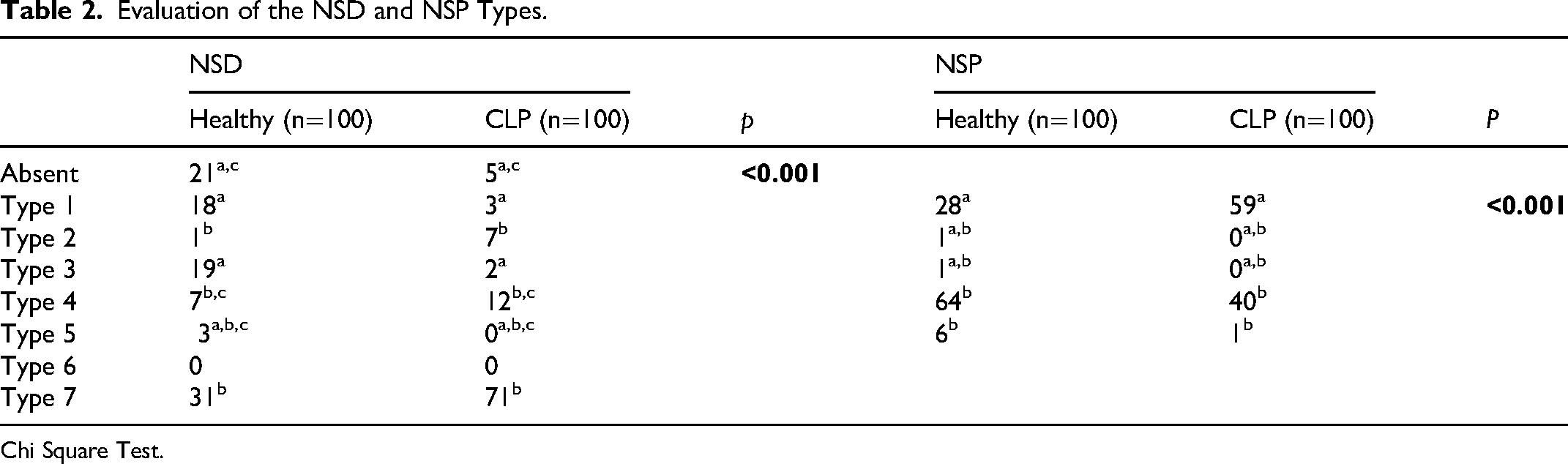
Chi Square Test.
A statistically significant association was found between the septal deviation side and cleft laterality, with septal deviation occurring predominantly on the same side as the cleft (p < 0.001) (Table 3).
Evaluation of the Relationship Between NSD and the Localization of HT and CLP Line.

Chi Square Test.
Despite these structural differences, total nasal cavity airway volume did not differ significantly between the CLP and control groups (p = 0.219). In contrast, across the entire sample, males exhibited significantly larger nasal cavity volumes than females (p = 0.009) (Table 4).
Comparison Nasal Cavity Airway Volume According to CLP Presence and Sex.
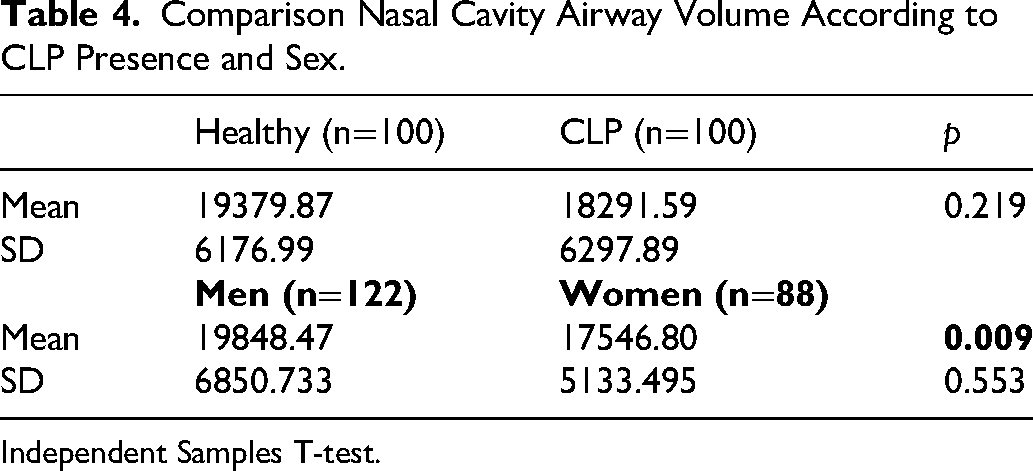
Independent Samples T-test.
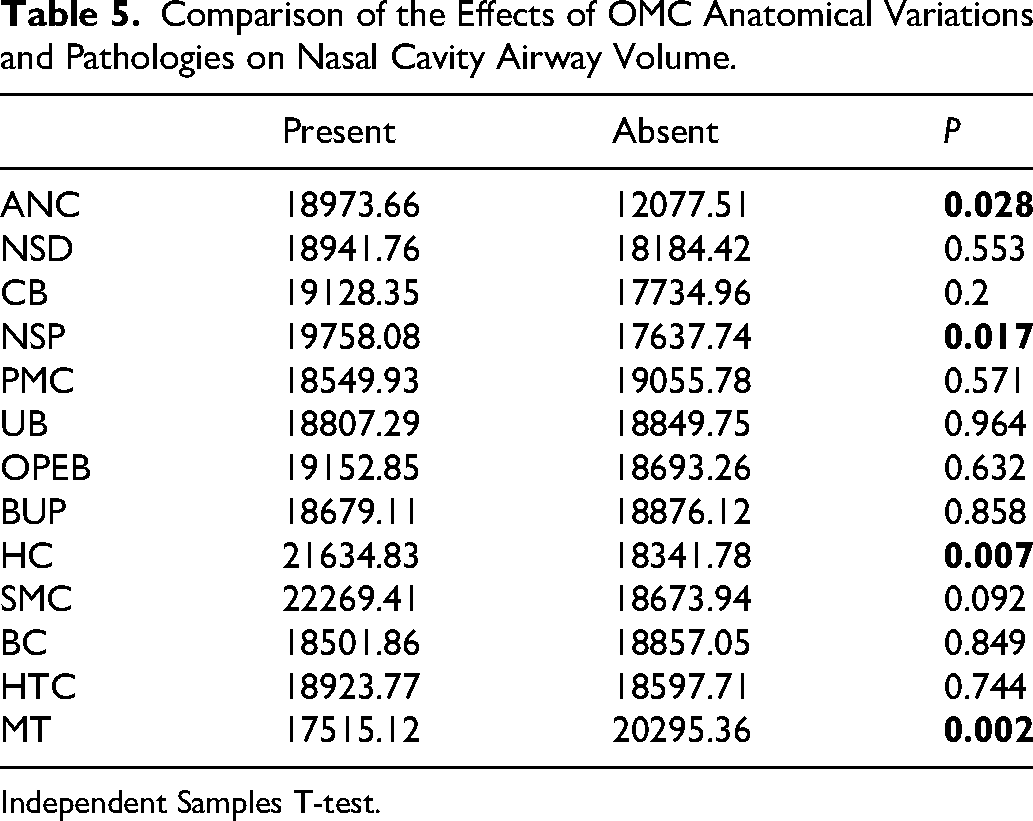
The associations between individual OMC variations and pathologies and nasal cavity volume are summarized in Table 5. Among these variables, HC, NSP, and MT demonstrated statistically significant associations with nasal cavity volume; however, the magnitude of these differences should be interpreted cautiously.
Comparison of the Effects of OMC Anatomical Variations and Pathologies on Nasal Cavity Airway Volume.
Independent Samples T-test.
Discussion
The literature shows that anatomical variations of OMC from reported prevalence rates vary widely across studies. For example, the incidence of paradoxical turbinate has been reported to vary widely from 3% to 42% across different studies.2,3,11,13,17,21,23,25,27,31 The reason for the difference is thought to be the use of different definitions, patients of different ethnic origins, and different imaging techniques and imaging parameters.
Kennedy and Zinreich 1 considered air spaces protruding below the ethmoid bulla in the orbital floor at the opening of the maxillary sinus as HC and observed HC in 10% of cases in their study. Pérez-Piñas et al. 37 reported the presence of HC according to the same criterion, and detected HC in 2.7% of cases. However, Bolger et al. 11 defined HC as including any cell located between the ethmoidal bulla, the orbital lamina of the ethmoid bone, and the orbital floor; using this definition, Pérez-Piñas et al. 37 found the prevalence increased to 45% in the same study.
A review of the literature reveals significant differences in the definition of the ANC among researchers. Pratt and Pratt 38 defined the ANC as a projection located just above and anterior to the attachment point of the middle concha. Mosher 39 positioned this structure near the most anterosuperior end of the middle concha, describing its inner boundary as the uncinate process and its outer boundary as the inner surface of the superior process of the maxilla. Bolger et al. 11 described the ANC as the most anterior ethmoidal cell. Jacobs et al. 40 defined the ANC as a small bony projection on the lateral nasal wall, located just anterior and superior to the anterior attachment of the middle turbinate. Marquez et al. 41 suggested that the term agger nasi should be reserved for the superficial projection anterior to the middle turbinate attachment, whereas the term ANC should be used exclusively for the ethmoid air cells responsible for pneumatization of this projection.
These differences in the anatomical definitions of both HC and ANC significantly contribute to the wide ranges in prevalence rates reported in previous studies. Non-standardized diagnostic criteria make comparisons between studies difficult and highlight the need for consistent, reproducible anatomical definitions in radiological research.
In a study conducted in the United States, Joe et al. 13 reported the prevalence of PMC as only 3%. Wani et al., 17 evaluating an Indian population, reported a prevalence of 9.33%, whereas Çalışkan et al. 25 found a significantly higher prevalence of PMC in the Turkish population (21.8%). Although PMC was defined consistently across these studies as medial orientation of the convex surface of the middle concha opposite to its normal direction, its prevalence varied markedly among different populations. This wide variability despite a uniform definition suggests that ethnic differences and population-specific anatomical variations may play an important role.
While the prevalence of CB was reported as 45.4% in Kaygusuz et al. 21 and 25.8% in Orhan et al. 23 in studies using CT, these rates increased markedly to 92% in Göksel and Özcan 3 and 87.5% in Dedeoğlu et al. 31 in studies using CBCT. Kar and Altıntaş 42 retrospectively analyzed paranasal sinus tomography images and reported that concha bullosa was detected in 44.74%. In all of these studies, CB was defined according to the same anatomical criteria, and evaluations were performed within the same ethnic population. Despite this, significant differences in prevalence rates were reported. This variability observed despite the same definition and population indicates that the prevalence of concha bullosa largely depends on the sensitivity of the imaging method used.
Studies conducted on healthy individuals1,2,11-30 have suggested that the presence of CLP-related deformities in the oral and nasal cavities by creating some changes in the OMC and nasal cavity, paving the way for more variation and pathology formation. Studies comparing variations and pathologies of OMC in healthy individuals and individuals with CLP are quite limited in the literature3,31 and our study has attempted to address this area.
Göksel and Özcan 3 observed a significantly higher incidence of paradoxical middle concha (PMC) in individuals with CLP (58%) compared to healthy individuals (42%) (p = 0.024). Dedeoğlu et al. 31 reported no statistically significant difference in PMC incidence between healthy individuals (38%) and individuals with CLP (46%) (p > 0.05). In this study, in line with Göksel and Özcan, 3 PMC was statistically significantly higher in individuals with CLP (p = 0.015).
No statistically significant difference in the incidence of HC was reported by Göksel and Özcan
3
and Dedeoğlu et al.
31
when comparing healthy individuals (30% and 18%, respectively) and individuals with CLP (42% and 24%, respectively) (
Göksel and Özcan 3 reported a statistically significant difference in the presence of NSD at 80% in healthy individuals and at 92% in the CLP group (p < 0.05) using Earwaker classification. 12 The present study adds additional data on NSD in individuals with CLP based on the Mladina classification and also found a statistically significant difference in prevalence of NSD between healthy individuals and individuals with CLP (p = 0.001). In their studies on only healthy individuals according to the Mladina classification, Wee et al. 18 reported the prevalence of NSD types as follows: type 1, 35.4%; type 2, 27.9%; type 3, 8.8%; type 4, 17%; type 5, 6.8%; type 6, 4.1%; and type 7, 0% in 488 of 970 patients. Prasad et al. 22 reported type 1 in 21%, type 2 in 27.1%, type 3 in 14.9%, type 4 in 14.9%, type 5 in 9.6%, type 6 in 7.89%, and type 7 in 4.38% of 114 patients. Similarly, Moshfeghi et al. 29 reported type 1 in 19.4%, type 2 in 6.2%, type 3 in 20.7%, type 4 in 5.4%, type 5 in 4.4%, type 6 in 0.3%, type 7 in 30.3%, and no NSD in 13.2% of 386 patients. In our study, both healthy individuals and individuals with CLP groups, the prevalence of NSD types was found to be statistically significant different (p < 0.001).
Previous studies have demonstrated a significant association between cleft laterality and the direction of NSD. Suzuki et al. 44 reported that the nasal septum was predominantly convex toward the cleft side in patients with unilateral clefts, revealing a strong correlation between cleft side and deviation direction (p < 0.001). Similarly, Dinç et al. 45 observed ipsilateral septal deviation in 80% of right-sided clefts and in all left-sided clefts, confirming a significant association between cleft laterality and septal deviation direction. In agreement with these findings, the present study also demonstrated that NSD occurred predominantly on the same side as the cleft (p < 0.001). These consistent results suggest that unilateral cleft formation leads to asymmetric nasal and maxillofacial development, resulting in septal displacement toward the cleft side.
Göksel 46 reported the presence of NSP at 69% in healthy individuals and at 50% in the CLP group. Comparing healthy individuals (72%) and individuals with CLP (41%), the prevalence of NSP was found to be statistically significantly different (p < 0.001) in this study.
Mureşan et al. 35 evaluated the images of 190 healthy individuals and classified NSP according to their anatomical localization. According to this classification, the most common type of NSP was found to be type 4 as 71%. In the present study, using the classification proposed by Mureşan et al., 35 type 4 was also the most common NSP pattern in healthy individuals (64%). But in the CLP group, lack of pneumatization of the NS (type 1) was most observed at rates of 59%. The prevalence of NSP types was found statistically significantly different in both healthy individuals and individuals with CLP groups (p < 0.001).
Two theories have been proposed to explain the relationship between HC and NSD in the literature. The first and most widely accepted theory states that hypertrophy of the contralateral turbinate occurs as a compensatory reaction to NSD. The second theory proposes that unilateral nasal turbinate growth results from genetic causes or early-life trauma, which creates pressure on the nasal septum as it grows throughout childhood and adolescence, leading to its deviation toward the contralateral side.47-49 Demir et al. 50 evaluated the relationship between NSD and middle turbinate hypertrophy and reported statistically significant middle turbinate hypertrophy on the non-NSD side compared to the NSD side. In this study, the hypertrophy of the middle turbinate on the non-NSD side was found to be statistically significant (p < 0.001).
Mølsted and Dahl, 51 Kolbenstvedt et al., 52 Suri et al., 53 and Starbuck et al. 54 concluded that the nasal septum significantly deviates to the same side in patients with unilateral CLP (UCLP). This study reached the same conclusion as previous studies that found the CLP line and the NSD line to be on the same side (p < 0.001).
Loftus et al. 55 conducted a study examining 62 healthy individuals and found that intranasal cavity volume increased with age and men having larger intranasal cavity volumes than women. Previous studies have found that age and sex have a significant effect on nasal cavity volume. In this study, sex also affects the nasal airway volume significantly. Therefore, while determining the study population, healthy individuals were selected as close in age as possible and with the most equal gender distribution with CLP group.
Farzal et al. 56 evaluated 30 individuals (10 healthy individuals, 10 with UCLP and 10 with bilateral CLP (BCLP)) and reported that nasal cavity volume was lower in individuals with UCLP and BCLP compared with healthy controls. In contrast, Ertaş and Ataol 57 evaluated nasal airway volumes in 16 individuals with UCLP and a skeletal Class III relationship and 16 healthy individuals with a skeletal Class III relationship, reporting significantly larger nasal airway volumes in the CLP group. In the present study, nasal cavity volumes in individuals with CLP and healthy individuals were calculated using the anatomical boundaries defined by Glupker et al. 36 Unlike the findings of Farzal et al. 56 and Ertaş and Ataol, 57 no statistically significant difference was observed between the nasal cavity volumes of individuals with CLP and healthy individuals.
Although a potential relationship between OMC variations and nasal cavity volume could be anticipated, our findings did not demonstrate a significant association between these parameters. Despite the increased prevalence of several OMC variations and pathologies in individuals with CLP, total nasal cavity volume remained comparable between groups. This finding suggests that regional anatomical alterations within the OMC do not necessarily translate into measurable differences in global airway dimensions.
Another important consideration is that unilateral and bilateral CLP cases were analyzed together in the present study. Given the known asymmetry and side-specific anatomical variations in unilateral CLP, pooling these subgroups may have influenced the interpretation of anatomical patterns and potentially masked subtype-specific differences. Therefore, future studies evaluating unilateral and bilateral cleft phenotypes separately may provide more detailed insight into subtype-specific OMC morphology.
In this retrospective observational study, selected OMC anatomical variations and pathologies were significantly more prevalent in individuals with CLP compared with healthy controls, whereas total nasal cavity volume did not differ significantly between groups. These findings suggest that OMC anatomy and total nasal cavity volume represent related but distinct anatomical constructs. While the OMC primarily reflects regional drainage and ventilation pathways, overall nasal cavity volume appears to be influenced by broader craniofacial morphology and growth patterns in CLP. Therefore, structural variations within the OMC should not be assumed to proportionally alter global airway dimensions. Moreover, nasal airflow is a dynamic physiological process regulated not only by static anatomical dimensions but also by nasal valve mechanics, mucosal congestion, and autonomic control of the venous sinuses. As described by Eccles, 58 total nasal resistance is largely determined at the level of the nasal valve and may fluctuate over time independently of global nasal cavity volume. Accordingly, static volumetric measurements obtained from CBCT represent morphologic parameters and cannot fully capture the functional behavior of the nasal airway. Although several anatomical variations demonstrated statistically significant differences between groups, statistical significance does not necessarily imply direct clinical impact. Variations such as NSD, PMC, NSP, or mucosal thickening may influence regional airflow dynamics or sinus drainage; however, without objective functional assessment or symptom correlation, the magnitude of their clinical relevance remains uncertain. Future prospective studies integrating morphologic imaging with functional airflow assessment and patient-reported outcomes are required to better clarify the clinical implications of these anatomical findings.
Clinical Implications
From a cleft care perspective, identification of OMC variations has practical implications for preoperative planning and multidisciplinary management. Patients with CLP frequently undergo secondary rhinoplasty, septoplasty, alveolar bone grafting, or orthognathic procedures.
32
Altered intranasal anatomy in these individuals may increase surgical complexity and influence intraoperative orientation. Recognition of septal deviation patterns, turbinate hypertrophy, and infraorbital ethmoid cells on preoperative CBCT imaging may support anatomic mapping and preoperative team communication. However, because symptom severity, objective functional airflow measures, and surgical outcomes were not assessed in this study, these radiologic findings should not be interpreted as direct indicators of functional impairment or operative risk. Although global nasal cavity volume was not significantly altered, the higher prevalence of selected OMC variations suggests that localized anatomical differences should be carefully evaluated in cleft patients on an individual basis. Therefore, review of the OMC region on preoperative CBCT
Limitations
One limitation of this study is that unilateral and bilateral CLP cases were pooled in the primary analyses to preserve statistical power, given the relatively smaller bilateral subgroup. While these subtypes may exhibit distinct anatomical patterns, the primary objective was to evaluate the overall impact of cleft presence on OMC morphology and nasal cavity volume rather than subtype-specific differences. Future studies with larger and more balanced cleft subgroups are warranted to further explore potential anatomical distinctions between unilateral and bilateral cleft phenotypes. Additionally, functional airway assessments and symptom-based evaluations were not included, which limits direct clinical interpretation of the anatomical findings.
Conclusion
Within the limitations of this retrospective CBCT study, individuals with CLP demonstrated a distinct pattern of OMC anatomical variations compared with healthy controls, while total nasal cavity volume did not differ significantly between groups. These findings highlight the importance of distinguishing regional osteomeatal anatomy from global airway dimensions in cleft populations and may assist clinicians in preoperative radiologic assessment and surgical planning.
Footnotes
Acknowledgments
The authors thank Asst. Prof. Şükrü Can Akmansoy for his contribution to the statistical analysis.
Ethical Approval and Informed Consent
This retrospective study was approved by the Marmara University Faculty of Medicine Non-invasive Clinical Research Ethics Committee (Project No: 09.2023.710). All procedures were performed in accordance with the guidelines of the Declaration of Helsinki.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated and analyzed during the current study are not publicly available due to ethical and privacy considerations but are available from the corresponding author on reasonable request.
Anonymity Statement
All identifying information related to the authors, institutions, ethics committees, and funding sources has been included only on the title page to ensure anonymity during the peer review process.