
Abstract

INTRODUCTION
Foreign bodies within the hands and feet are common clinical problems, and most of these become symptomatic as a result of their location in the palmar or plantar soft tissues. Foreign bodies within the bone are distinctly more unusual and can pose significant diagnostic challenges as illustrated in this case report.
CASE REPORT
A 23-year-old man presented with progressively worsening symptoms of pain and swelling of the left foot over a 3-month period. He denied any history of recent injury or systemic illness. Physical examination revealed mild tenderness and slight enlargement over the dorsolateral aspect of the midfoot region of his left foot, just overlying the cuboid. There was skin discoloration but no erythema or cellulitis. Range of motion of the patient's ankle was satisfactory. There was mild restriction of hindfoot motion, lacking a little less than 10 degrees combined inversion and eversion, compared to the contralateral foot.
Before his initial visit, the patient was seen in another city where he was diagnosed as having a solitary bone cyst of the left cuboid. This was confirmed on CT, the report of which described a “well-circumscribed lucent lesion of the cuboid.” The study noted communication of the lesion plantarly into the subjacent abductor digiti minini muscle. Most notable was the “cortical fragment within a large lucent lesion… compatible with the fallen fragment sign.”
Upon further questioning, the patient recalled what he believed to be an unrelated history of injury four years before onset of symptoms. He jumped into the Connecticut River from an overhanging tree branch, where the water was shallower than anticipated, sustaining a stellate laceration of the plantar surface of his foot, which was sutured at the local emergency room. Three weeks later, the wound dehisced and drained a small amount. Healing occurred over several weeks after a course of oral antibiotics and wound soaks. He had no subsequent symptoms and subsequently participated in collegiate athletics, as well as numerous running sports after graduation.
Radiographs
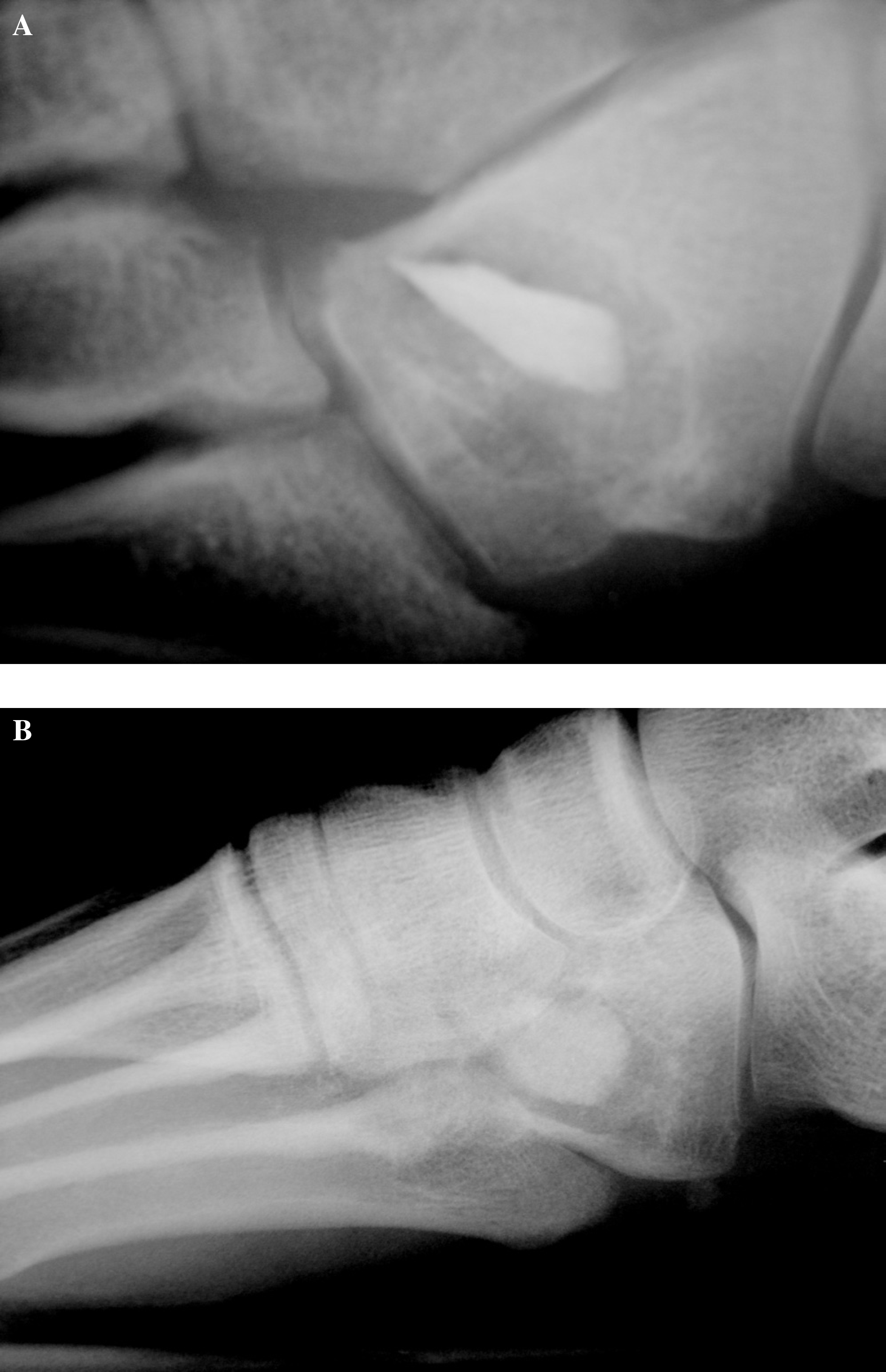
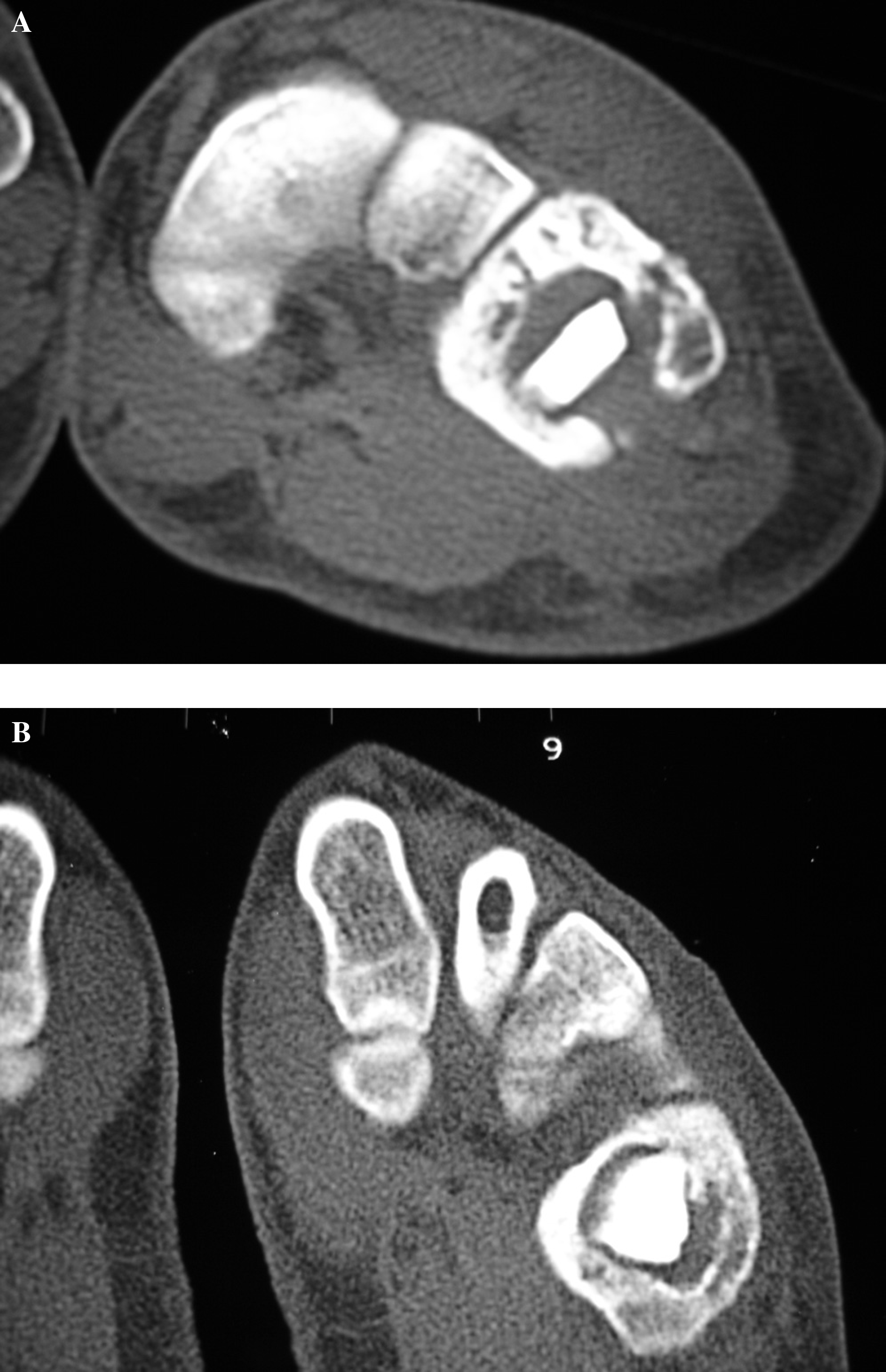
Review of standing anteroposterior, lateral, and oblique radiographs of the foot and ankle showed a lytic lesion of the cuboid, which occupied 50% of the volume of the bone and contained a hyperdense zone (Figure 1, A and B). Destruction of the inferior cortex of the cuboid by the expansile cystic lesion was noted. The zone of transition between the osteolysis and the normal bone appeared narrow and demonstrated a thin zone of sclerosis. Review of the outside CT scan brought by the patient revealed hyperdense material, inconsistent with bone and suggestive of a foreign body within the cystic zone of the cuboid (Figure 2, A and B).
Operative Treatment
Irrigation and debridement of the cuboid was done through a longitudinal lateral incision. At surgery, there was chronic thickening of the overlying soft tissue and periosteum. This layer contained granulomatous tissue and a small amount of what appeared to be purulent material. There was granulomatous-appearing material inside the bone. Cultures of both the soft tissue and of the bone itself were taken for aerobic, anaerobic, fungal, and acid-fast organisms.
The breach in the plantar-lateral cortex of the cuboid was widened for debridement and revealed a large foreign body, consisting of a 15 × 20 × 4 mm piece of stone (Figures 3 and 4). There were multiple smaller pieces of the same slategray material within the bone. The cuboid was extensively debrided with osteotomes, curettes, and rongeurs. Because the lesion extended into the distal articular cartilage of the cuboid, a large portion of the distal subchondral bone and cartilage had to be removed to achieve adequate debridement.
Once all the cultures were taken, the patient was given 1 gram of intravenous cefazolin, and the wound was irrigated with 6 liters of antibiotic solution using a pulsing lavage system. The wound was packed open. Three days later, the patient underwent repeat debridement, irrigation with the pulsing lavage system, and wound closure.
Pathologic Findings
Histologic examination revealed an osseous foreign body, mild chronic, nongranulomatous inflammation within the fibroconnective tissue, and extensive marrow fibrosis with “prominent inflammation as aggregates of lymphocytes and plasma cells” mixed with the bone fragments.
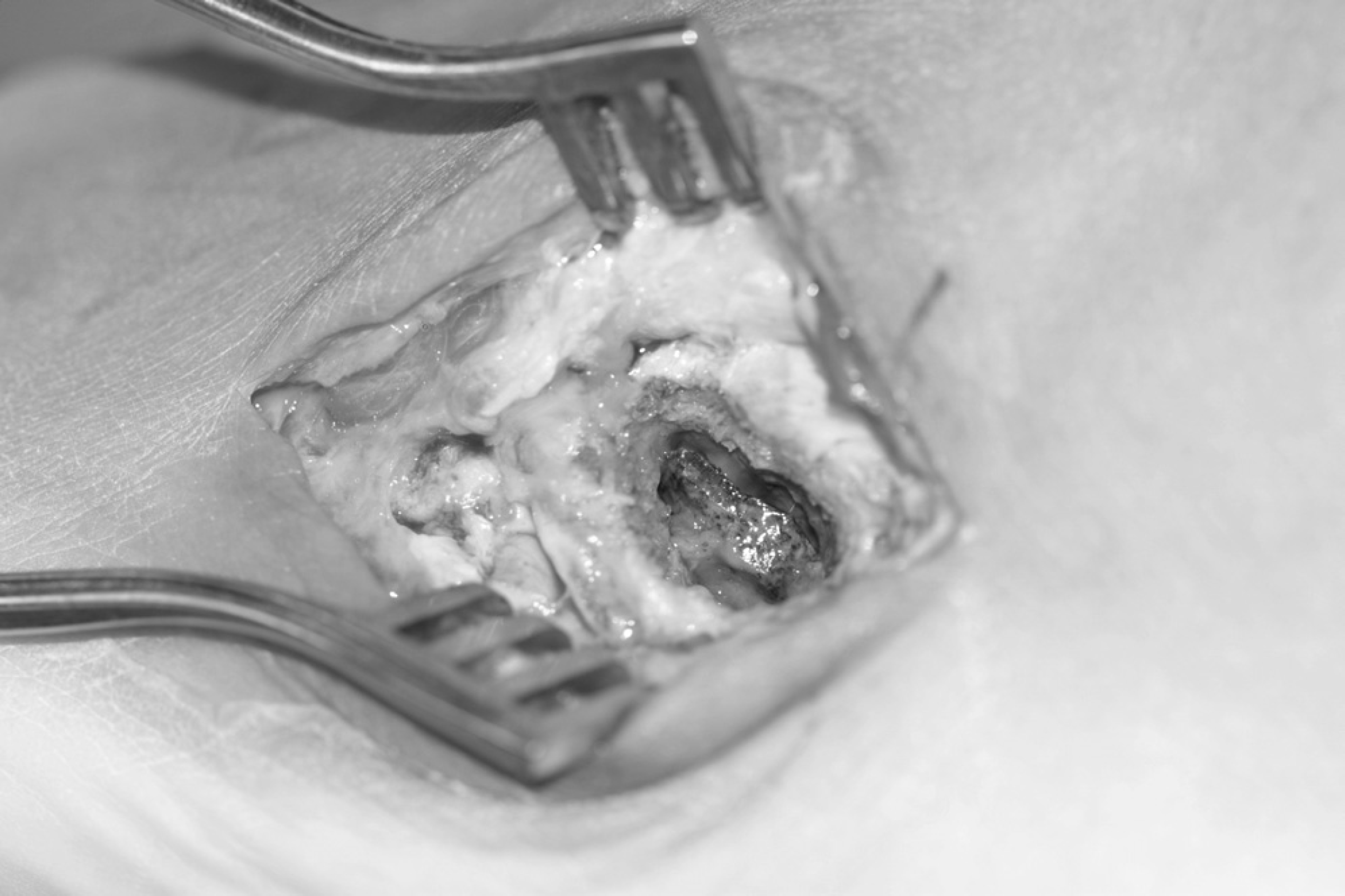
Intraoperative photograph demonstrating the petrous foreign body through a lateral window in the cuboid bone.
Microbiology reported presumptive clostridium species from both the soft tissue and the bone. Operative cultures were negative for aerobes, acid-fast bacilli, and fungi. The infectious diseases consultant prescribed intravenous piperacillin/tazobactam (Zosyn® Wyeth, Philadelphia, PA) while the patient was in the hospital, and the patient was discharged on an outpatient intravenous regimen with this medication.

The rock, to scale, after removal.
Complications
Five days after the peripherally inserted central catheter (PICC) line was placed in the left arm, the patient was readmitted to the hospital with fever and chills. He was found to have a DVT in his left upper extremity associated with the intravenous line. He was treated with enoxaparin sodium (Lovenox®, Sanofi-Aventis, Bridgewater, NJ) for two days, and the PICC line was removed. Despite placement of a new PICC line in the patient's right arm, he had persistent fever, which was ultimately attributed to the medication by the infectious diseases consultant. The patient was changed from piperacillin/tazobactam to intravenous ertapenem sodium (Ivanz®, Merck, West Point, PA), with prompt resolution of the fever. The patient completed a 6-week regimen of 1 g ertapenem sodium daily.
After surgery, there was primary wound healing without complications. The patient experienced no wound dehiscence or drainage at any time after the second surgical procedure. There were no clinical signs of recurrent infection. The patient was prescribed a molded accommodative insole for his shoe. He was advised to modify his athletic activity to tolerance and to observe the foot for a minimum of 6 months before the planned secondary reconstruction.
At 8 months after the completion of his antibiotic regimen, the patient had moderate residual pain over the lateral midfoot and a mild sensation of instability in the region (Figure 5). Reconstructive surgery was done, including repeat wound debridement and cultures and concomitant arthrodesis between the cuboid and lateral two metatarsals and between the bases of the fourth and fifth metatarsals. Proximal tibial bone graft was used to fill the osseous defects and to augment the arthrodesis sites.
After surgery, the patient was maintained in a nonweight-bearing cast for 3 months, followed by a walking cast for 3 weeks. The patient was then prescribed a cushioning insole with an underlying carbon fiber stiffening device in his shoe.
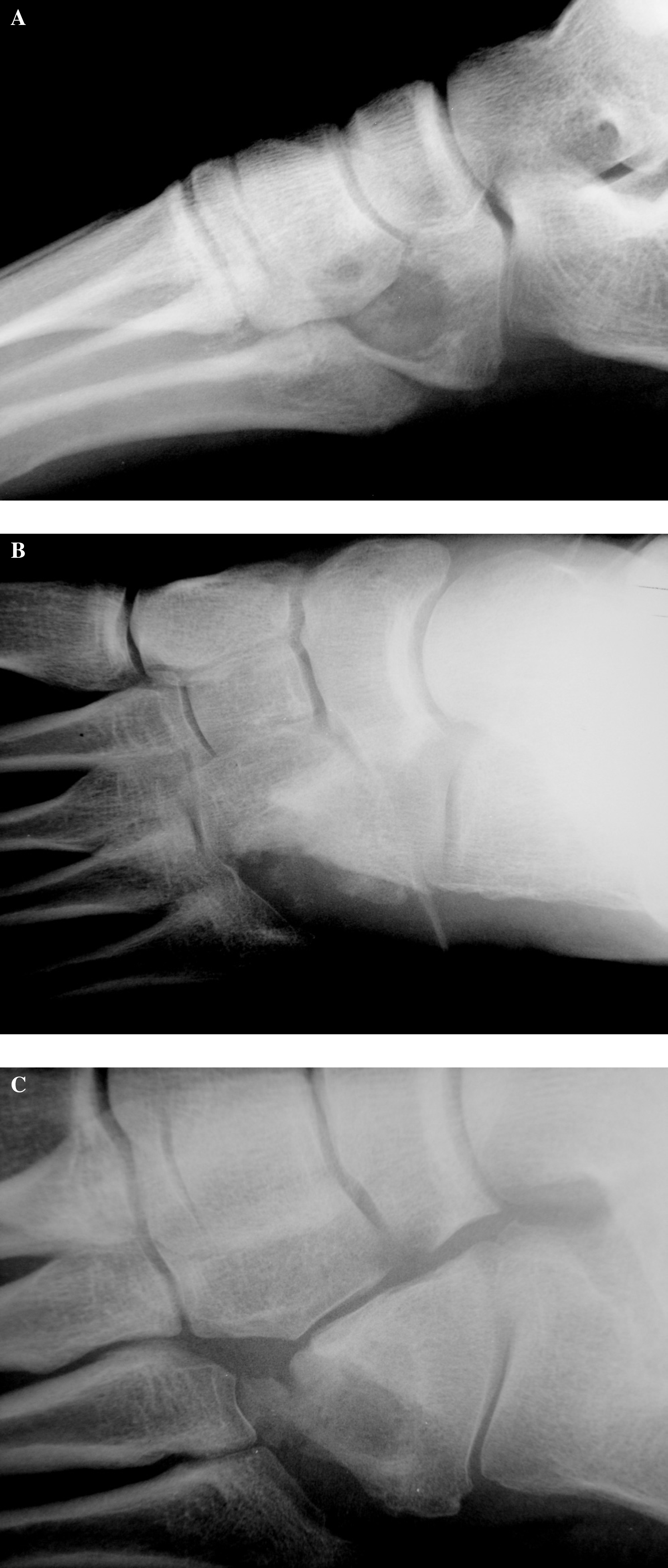
Lateral

Anteroposterior
Followup
At last followup, 2 years after surgery, the patient reported no significant pain or limitation of daily or exercise activities, with the exception that he was no longer jogging. On examination, the patient had excellent hindfoot, midfoot, and forefoot alignment. He had 5/5 muscle strength in all planes and could perform resisted hindfoot eversion with no pain. Dorsalis pedis and posterior tibial pulses were 2+. Radiographic examination demonstrated complete consolidation of the arthrodesis sites (Figure 6).
DISCUSSION
As common as the diagnosis of imbedded foreign body in the foot may seem, foreign bodies frequently pose dilemmas, either of diagnosis, treatment, or both. Radiopaque materials typically are certain kinds of glass or metal, although other unusual radiopaque materials have been reported. 8 Metallic ones, while easy to see, can be hard to remove operatively if they are in an unusual or sensitive location. Several authors have reported metallic foreign bodies embedded in the bones of the foot. 10,15,16 The more common dilemma is the difficulty of diagnosis, specifically of finding nonmetallic or radiolucent foreign bodies in the soft tissues. 2,6,11
However, most unusual are the radiolucent foreign bodies within bone, because of the greater trauma required and the rarity of radiolucent objects that are rigid enough to penetrate osseous structures. Gerbert et al. 4 reported one example. Of the many foreign bodies reported in the literature, Durr et al. 3 noted that “only 31 cases of thorn, wood, or plant-splinter induced lesions of bone have been reported in the English language literature to our knowledge.” These authors noted that foreign bodies may cause changes of osteolysis or periosteal reaction that may simulate tumors such as in our patient, although most produced granulomatous reaction in the soft tissue.
Foreign bodies within bone may produce significant osseous reaction, resulting in the so-called foreign body granuloma or a post-traumatic bone cyst. 5 Both lesions typically manifest as a lytic osseous lesion with well-defined or sclerotic margins. Absorbable orthopaedic implants can produce similar histologic and radiographic findings as traumatic foreign bodies within the bone. 1,9 Foreign bodies can migrate within the associated post-traumatic bone cyst, giving a clue to this entity. 13 The inciting foreign material may be radiopaque, as in this patient, or radiolucent as with most organic material such as thorns or branches. 14 The foreign body granulomatous response can be difficult to distinguish from a primary benign or malignant osseous lesion, such as a unicameral cyst, giant cell tumor, enchondroma, sarcoma, or a metastatic lesion.
In most cases, the presence of nonaggressive features such as a narrow zone of transition or sclerotic rim together with visualization of the foreign body and history of penetrating trauma are the keys to the diagnosis. Ultimately, histologic evaluation can definitively confirm the diagnosis, especially in the absence of a history of penetrating trauma.
The ease of visualization of soft tissue or intra-osseous foreign bodies depends not only on the inherent density of the foreign material but also on the size of the object. 12 Materials having a density closer to soft tissue may require advanced imaging modalities such as CT, MRI, or ultrasound because of their superior contrast resolution among materials of similar density or architectural composition. 7
Some patients also present after considerable time has elapsed from the inciting injury. In fact, the history of penetrating injury often is deemed insignificant because of the delayed onset of symptoms.
This case was unusual in several ways. The intra-osseous location and unusual size and inert nature of the foreign bodies presumably accounted for the long interval between injury and symptoms.
This case also posed the inverse of the usual dilemma of a foreign body in the foot: the difficulty of finding a foreign body that was large, obvious, and radiopaque rather than the usual problem of a foreign body that is small, occult, and radiolucent. A routine radiograph in the emergency department would have revealed the foreign body. The original history failed to identify the plantar laceration as a penetrating wound, despite the foreign matter found in the soft tissue. Once the lesion finally became symptomatic, it was misinterpreted as a neoplasm of the bone and the foreign body as a “fallen fragment” of bone.
In retrospect, the rock must have penetrated the plantar surface of the cuboid at the time of injury, and the limited extent of the infection was presumably due to the containment of the foreign body within the bone rather than in the soft tissue. The cystic reaction and dense foreign body simulated a cystic neoplasm with an internal cortical bone fragment. While differential considerations include chronic osteomyelitis, benign primary osseous lesions of chondroid or fibrous histology, large intraosseous ganglion or subchondral cyst, most malignant lesions would be expected to generate a wider zone of transition without sclerosis.