
Abstract
Background:
Multimodal postoperative analgesia employs multiple medications given perioperatively to block the generation and perception of pain at different points in the nociceptive pathway. This retrospective study examines its effect on the length of stay for patients undergoing hindfoot and ankle fusions.
Methods:
All patients operated upon by the senior authors between 2007 and 2011, inclusive, underwent ankle fusion, subtalar fusion, pantalar arthrodesis, triple arthrodesis, or combined ankle/subtalar fusions. The perioperative pain management was either the “traditional” method (patient-controlled-analgesia–delivered parenteral narcotics beginning immediately postoperatively) or the multimodal pain protocol (pre- and postoperative oral administration of opioids, celecoxib, pregabalin, acetaminophen, and prednisone). The choice of pain protocol was up to the surgeons, without any exclusion criteria. Physical therapy protocols were not changed during the study. The study included 220 patients; 175 received the multimodal protocol and 45 received traditional management. Multimodal protocol patients were younger (53.9 vs 59.7 years; P < .003), but there were no other differences between the groups with respect to gender, obesity, body mass index, tobacco use, alcohol use, or comorbidities. Complex cases (revision surgeries, Charcot joint surgeries, multiple concurrent procedures, etc) were equally represented in both groups.
Results:
Multimodal protocol patients had lower lengths of stay (2.5 days; 95% confidence interval [CI], 1.4-3.7) than traditional pain management patients (4.2 days; 95% CI, 2.7-5.7; P < .001). This was also true for both complicated and uncomplicated surgeries when considered separately.
Conclusion:
This study provides the first evidence that multimodal therapy reduces the length of stay for patients undergoing major hindfoot or ankle fusion surgery, regardless of surgical complexity.
Level of Evidence:
Level III, comparative series.
Background
Multimodal postoperative analgesia, 3 which relies on the use of multiple medications given perioperatively to block the generation and perception of pain at different points in the nociceptive pathway, has been used extensively since it was first proposed in 1993 by Kehlet and Dahl. 3 Various iterations of the oral medications employed in multimodal therapy have included COX-2 inhibitors (which inhibits peripheral nerve stimulation and may inhibit central brain perception to pain), gabapentinoids (which inhibit transmission of pain in the dorsal ganglia of the spinal cord), acetaminophen (which has a central inhibitory effect), and opioids (which act in the dorsal ganglia and centrally).8,13 The proposed theory is that blocking the pain generation mechanism at several different stages in the pathway is more effective than blocking it at a single point.5,8,11-13 Intraoperatively, some investigators specify the use of spinal or regional anesthesia, some use supplemental peripheral blocks, and many of the arthroplasty studies include an injected cocktail that includes long-acting local anesthetic, morphine, and steroid into the surgical wound.1,4,5,7-9,11,12,14
There is a single study involving foot and ankle surgery that examined the role of multimodal therapy, 14 in which all surgeries were performed under regional anesthesia with popliteal blocks administered for postoperative pain control. In that study, the only variable examined was influence of the use of pregabalin on postoperative pain and opioid use. It was reported that pregabalin had no effect on these parameters.
In the author’s institution, multimodal therapy was introduced on the joint reconstruction service and was found to effectively reduce postoperative pain and length of stay (LOS). It was then instituted on the foot & ankle service using the same protocol in mid-2008. The current retrospective study was undertaken to test the hypothesis that the use of multimodal therapy similarly decreases the LOS for a specific group of patients. The group chosen for the comparison was those undergoing hindfoot and ankle fusions, so as to limit the study to a relatively homogeneous group of patients having procedures performed on the foot and ankle that were typically done on an inpatient basis.
Methods
The patients studied comprised those operated upon by attendings in the Foot & Ankle Section in the Department of Orthopaedics and Rehabilitation at a tertiary care center between January 1, 2007, and December 31, 2012. The inclusion criteria were that the patients underwent 1 of the following surgeries: ankle fusion, subtalar fusion, pantalar arthrodesis, triple arthrodesis, or combined ankle and subtalar fusions. All patients having these surgeries were identified and selected using billing records (both departmental and hospital) and the electronic medical record (EMR) system (Epic Systems, Inc, Verona, WI). The latter was an integrated system that incorporated all inpatient and outpatient patient care activities. All operative notes, discharge summaries, and clinic notes were captured in this system, as were all lab results, medications (either used in the hospital or prescribed), allergies, and problem lists. All notes were stored in the clinical database as plain text. All other data were coded as discrete data elements.
The perioperative pain management was by 1 of 2 methods. The “traditional” method was the use of patient-controlled analgesia (PCA)-delivered parenteral narcotics (either morphine or dilaudid) that was begun immediately postoperatively. Patients were then weaned to oral medications as quickly as possible. The multimodal pain protocol (Table 1) was adopted for use on the foot & ankle service in mid-2008 after its utility was demonstrated on the joint reconstruction service. The protocol consisted of preoperative oral administration of long-acting oxycodone (10 mg), celecoxib (200 mg), pregabalin (75 mg), acetaminophen (1 g), and prednisone (40 mg). Postoperatively, patients were begun on oral long-acting oxycodone (10 mg every 12 hours), celecoxib (200 mg every 12 hours), and acetaminophen (1000 mg every 6 hours). Short-acting oxycodone (5-20 mg every 4 hours) was provided for breakthrough pain. If this did not control the pain, then patients were offered parenteral narcotics. Steroids were not used in diabetic patients. Due to several instances of hyperglycemia in nondiabetic patients, the use of steroids in all patients was curtailed in mid-2009. Patients were discharged with prescriptions for 2 days of long-acting oxycodone, 2 weeks of celecoxib, and 2 weeks of short-acting oxycodone. Because of insurance limitations that evolved over the duration of the study, long-acting morphine was substituted for long-acting oxycodone. Patients whose outpatient prescription plan would not pay for celecoxib after discharge were placed on naproxen. The choice of pain management protocol was left to the surgeons. There were no exclusion criteria for use of the multimodal management protocol based on age, procedure, or comorbidities. Alterations due to drug allergies or sensitivities were made as needed. Standard order sets existed for both protocols to reduce the variability of implementation. Prior to the use of multimodal pain protocol, perioperative blocks were routinely used for postoperative pain control. These were rarely used once the new protocol was instituted, and only used when pain control was inadequate immediately after surgery. All surgeries were performed under spinal or general anesthesia, which were chosen without regard to the pain management used. There were no other systematic alterations in postoperative care during the study period, including physical therapy regimens. Inpatients were seen the day after surgery for crutch, walker, or wheelchair training, as deemed appropriate by the therapist. Discharge was based on achieving adequate pain control and passing the physical therapist’s training criteria.
Pain Protocol Schema.
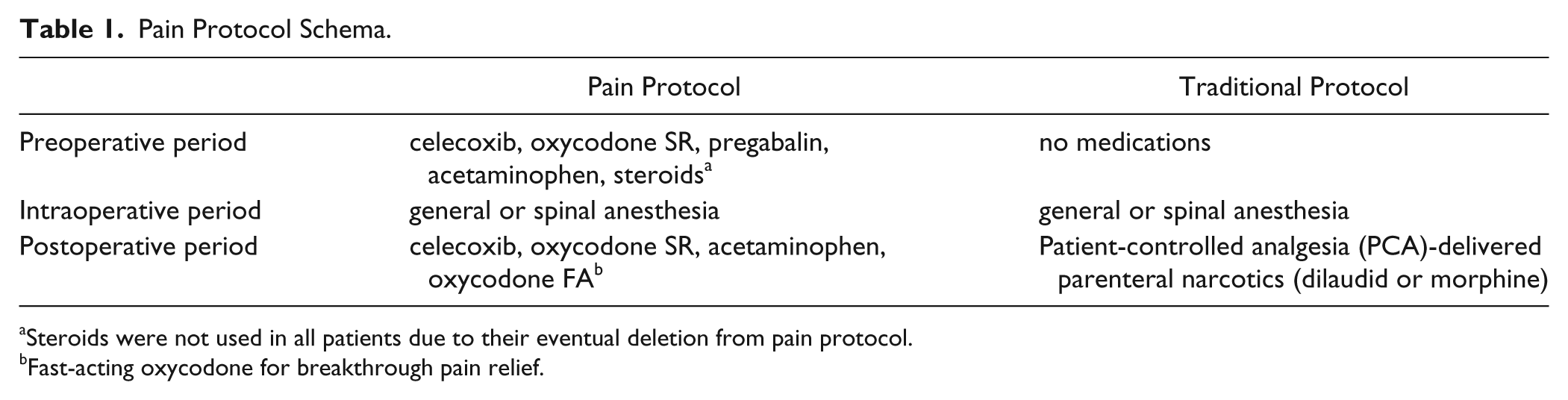
Steroids were not used in all patients due to their eventual deletion from pain protocol.
Fast-acting oxycodone for breakthrough pain relief.
Selection of Data Elements
All text notes, including operative summaries, operative notes, clinic notes, and discharge summaries, for each patient identified were collected. Discrete perioperative laboratory data elements collected included serum glucose and hemoglobin (Hgb) A1c. For glucose, the maximum value during the treatment encounter was used in the analysis. For the Hgb A1c, the preoperative value was selected.
Discrete demographic data collected included body mass index (BMI), age, gender, medications administered or prescribed, medical problems (captured in a patient-centric longitudinal problem list based on ICD9 coding), alcohol use, and tobacco use. The last 2 parameters were routinely collected and recorded as part of all inpatient and outpatient history and physical examinations.
All operative and postoperative notes were manually reviewed to determine the specific procedure performed. Discharge summaries and EMRs were used to determine admission and discharge dates. This was verified by comparing these dates with those obtained from the hospital billing records. The billing records for the hospital and department were reviewed to ascertain the billed charges and actual payments received by the hospital and orthopaedic provider for each surgical episode. The hospital charges included all hospital-associated costs, including medication.
Data Analysis
All data elements were downloaded into an Excel spreadsheet using masked patient medical record numbers that would prevent identification of individual patients while still permitting the longitudinal tracking of each patient’s notes, labs, medications, and other associated data.
Categorical data were assessed using chi-square tests or Fisher’s exact test. Due to the skewed distribution of most of the continuous data (age, BMI, financial data, laboratory data), the Wilcoxon rank test comparison was used for these parameters. In all instances, 2-sided testing was performed, with a significance level (P value) set at .05. All statistics were performed using SPSS (version 12.0; IBM Corporation, Armonk, NY).
This study was carried out with approval from the institutional review board.
Results
Two hundred twenty patients underwent fusion surgery of the hindfoot or ankle between January 1, 2007, and December 31, 2011, by the senior authors (J.D.M. and M.D.C.). Of these, 175 received the multimodal pain protocol and 45 did not. The demographic profile of the population is seen in Table 2. Patients receiving isolated subtalar joint fusions were more likely to have received the pain protocol than other patients (34/35, 97.1% vs 141/185, 76.2%; P < .003 by Fisher’s exact test), while those getting pantalar fusions were less likely to have been treated using the pain protocol (11/19, 57.9% vs 164/201, 81.6%; P < .031). The latter observation was not due to a higher prevalence of diabetes in the pantalar population (4/19 vs 54/202, P > .5). Outpatient surgeries were performed using only the pain protocol (24/24), whereas this had not been possible while using the traditional pain management regimen. No outpatient surgical patients were readmitted due to uncontrolled pain. On the other hand, complex cases (defined as revision surgeries, Charcot joint surgeries, multiple concurrent procedures, or otherwise complicated) were no more likely to receive the pain protocol than routine pain management.
Demographics of Study Population.
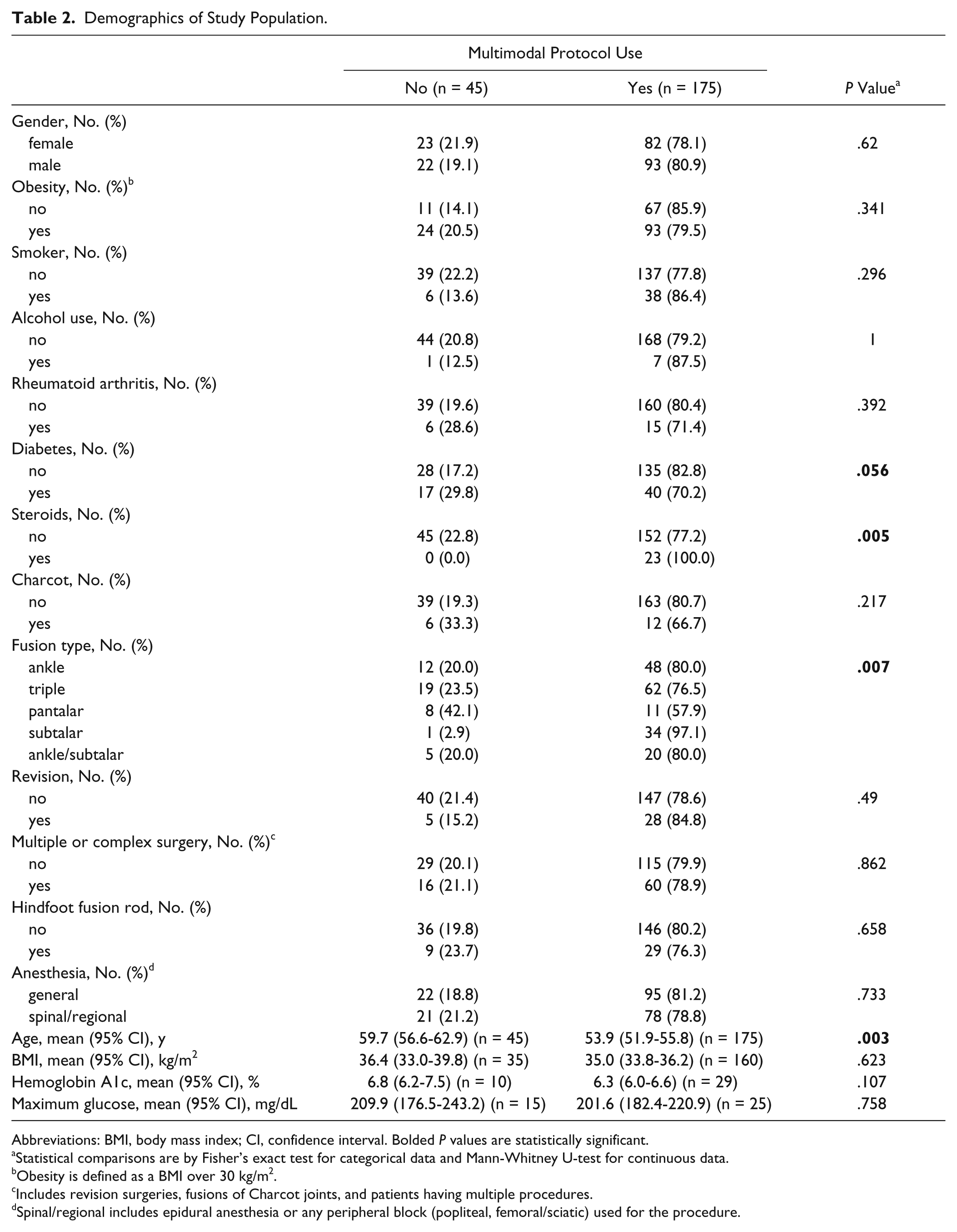
Abbreviations: BMI, body mass index; CI, confidence interval. Bolded P values are statistically significant.
Statistical comparisons are by Fisher’s exact test for categorical data and Mann-Whitney U-test for continuous data.
Obesity is defined as a BMI over 30 kg/m2.
Includes revision surgeries, fusions of Charcot joints, and patients having multiple procedures.
Spinal/regional includes epidural anesthesia or any peripheral block (popliteal, femoral/sciatic) used for the procedure.
Although patients receiving the pain protocol were younger (53.9 years; 95% confidence interval [CI], 51.9-55.8 vs 59.7 years; 95% CI, 56.6-62.9; n = 45; P < .003 by Mann-Whitney U-test), there were no other significant differences between the 2 groups with respect to gender, obesity, BMI, tobacco use, alcohol use, or prevalence of rheumatoid arthritis. There was borderline lower use of the pain protocol in diabetic patients (40/57, 70.2% vs 135/163, 82.8%; P < .056), and they were more likely to have been administered steroids during their admission (Table 2). However, the prevalence of surgery for Charcot joints was similar in both groups. There was no significant difference in the type of anesthesia used (general vs spinal/epidural/regional block) between the 2 groups (Table 2). Although only available for a small number of patients, hemoglobin A1c levels were not different between the 2 groups, nor were the maximum perioperative glucose levels.
Patients receiving the pain protocol had a lower overall LOS (2.5 days; 95% CI, 1.4-3.7) compared to those treated by conventional pain management (4.2 days; 95% CI, 2.7-5.7; P < .001). There were no significant differences in the professional or hospital-based payments received for treatment between the groups (Table 3A). The LOS was also analyzed by the status of patients with respect to diabetes or neuropathy (as reflected by the diagnosis of a Charcot joint) (Table 3B). The presence of diabetes did not alter the observation that pain protocol use was associated with reduced LOS. For patients with neuropathy (Charcot joints), this was not true, as the use of the pain protocol did not influence their LOS (2.8 days; 95% CI, 1.3-4.4 vs 2.5 days; 95% CI, 1.3-3.7; P = .557). The data were also reanalyzed without the subtalar joint fusion patients, who predominantly had outpatient surgery. There was no difference in the results, with the LOS being lower in pain protocol patients than in conventionally treated patients (2.9 days; 95% CI, 1.5-4.3 vs 4.2 days; 95% CI, 2.7-5.8; P < .001).
Impact of Multimodal Pain Protocol on Admission Status and Treatment Costs.
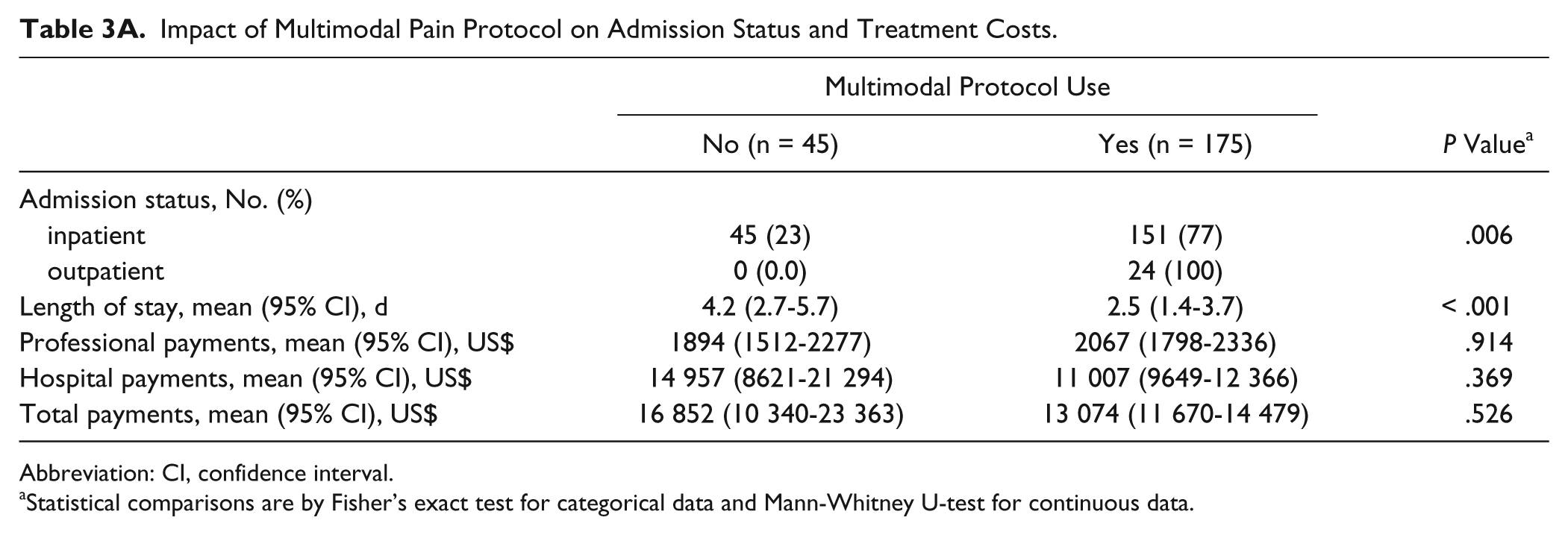
Abbreviation: CI, confidence interval.
Statistical comparisons are by Fisher’s exact test for categorical data and Mann-Whitney U-test for continuous data.
Influence of Diabetes and Neuropathy on Length of Stay.
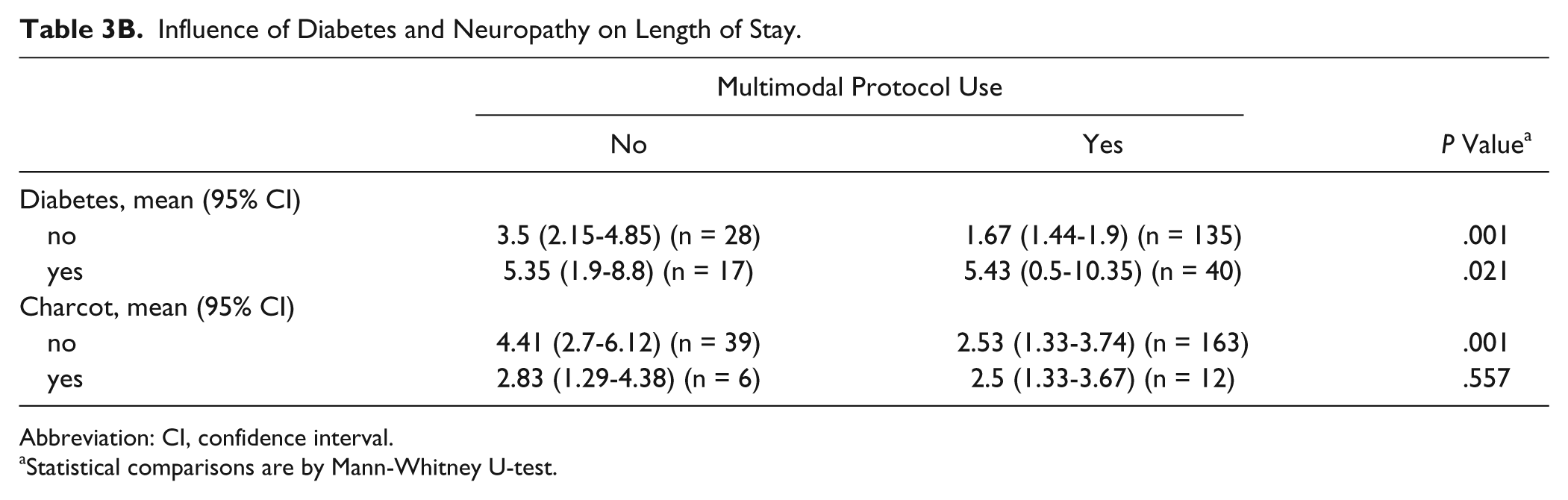
Abbreviation: CI, confidence interval.
Statistical comparisons are by Mann-Whitney U-test.
Anesthesia type affected the LOS. Patients receiving general anesthesia had higher LOS than those having spinal, epidural, or regional blocks in the overall population (4.1 days; 95% CI, 2.0-6.1 vs 1.9 days; 95% CI, 1.5-2.3; P = .001) and among those who were administered the multimodal pain protocol (3.9 days; 95% CI, 1.4-6.4 vs 1.4 days; 95% CI, 1.2-1.7; P < .001). Controlling for inpatient/outpatient status and comorbidities did not alter this finding.
Since the payments were significantly higher in complicated cases (P < .011) (Table 3C), the lack of payment differences seen could be due to that factor. The analysis was therefore re-run stratifying cases based on the complexity of the case (revision, Charcot joint, multiple procedures, etc). In uncomplicated patients (Table 4A), the patients were younger (54.2 years; 95% CI, 51.9-56.5 vs 61.2 years; 95% CI, 57.1-65.4; P < .002), were more likely to have outpatient procedures (P < .042), were likely to be given steroids (P < .024), and had lower LOS (1.6 days; 95% CI, 1.4-1.9 vs 3.2 days; 95% CI, 2.5-3.9; P < .001) if the pain protocol was used. Professional or hospital payments were not different. In complicated cases (Table 4B), while patient ages were not different between the groups, the LOS was reduced with the use of the pain protocol (4.2 days; 95% CI, 1.0-7.5 vs 6.1 days; 95% CI, 1.9-10.2; P < .007), but professional or hospital payments were not different. The distribution of diabetic patients between the treatment groups was not significantly different when controlling for the performance of either the uncomplicated or complicated surgeries.
Impact of Surgical Complexity on Length of Stay and Treatment Costs.
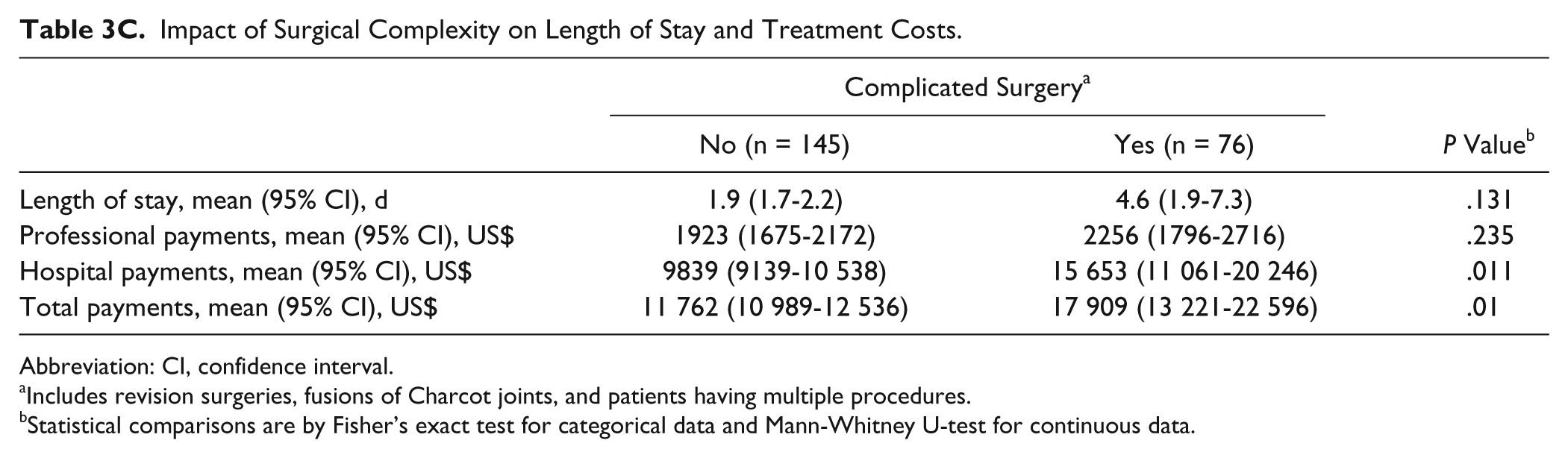
Abbreviation: CI, confidence interval.
Includes revision surgeries, fusions of Charcot joints, and patients having multiple procedures.
Statistical comparisons are by Fisher’s exact test for categorical data and Mann-Whitney U-test for continuous data.
Demographics and Outcomes in Patients Having Uncomplicated Surgeries.
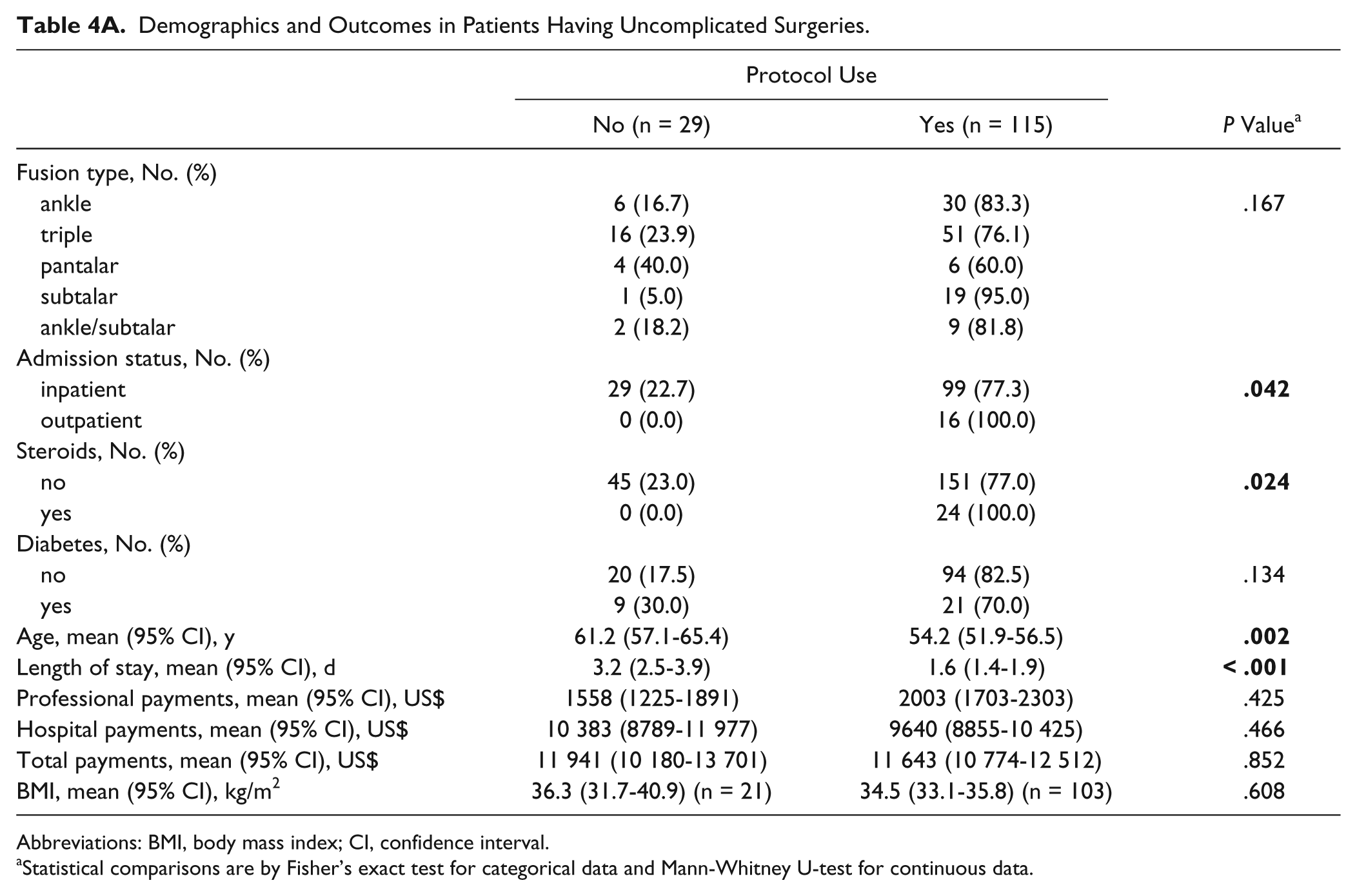
Abbreviations: BMI, body mass index; CI, confidence interval.
Statistical comparisons are by Fisher’s exact test for categorical data and Mann-Whitney U-test for continuous data.
Demographics and Outcomes in Patients Having Complex Surgeries.
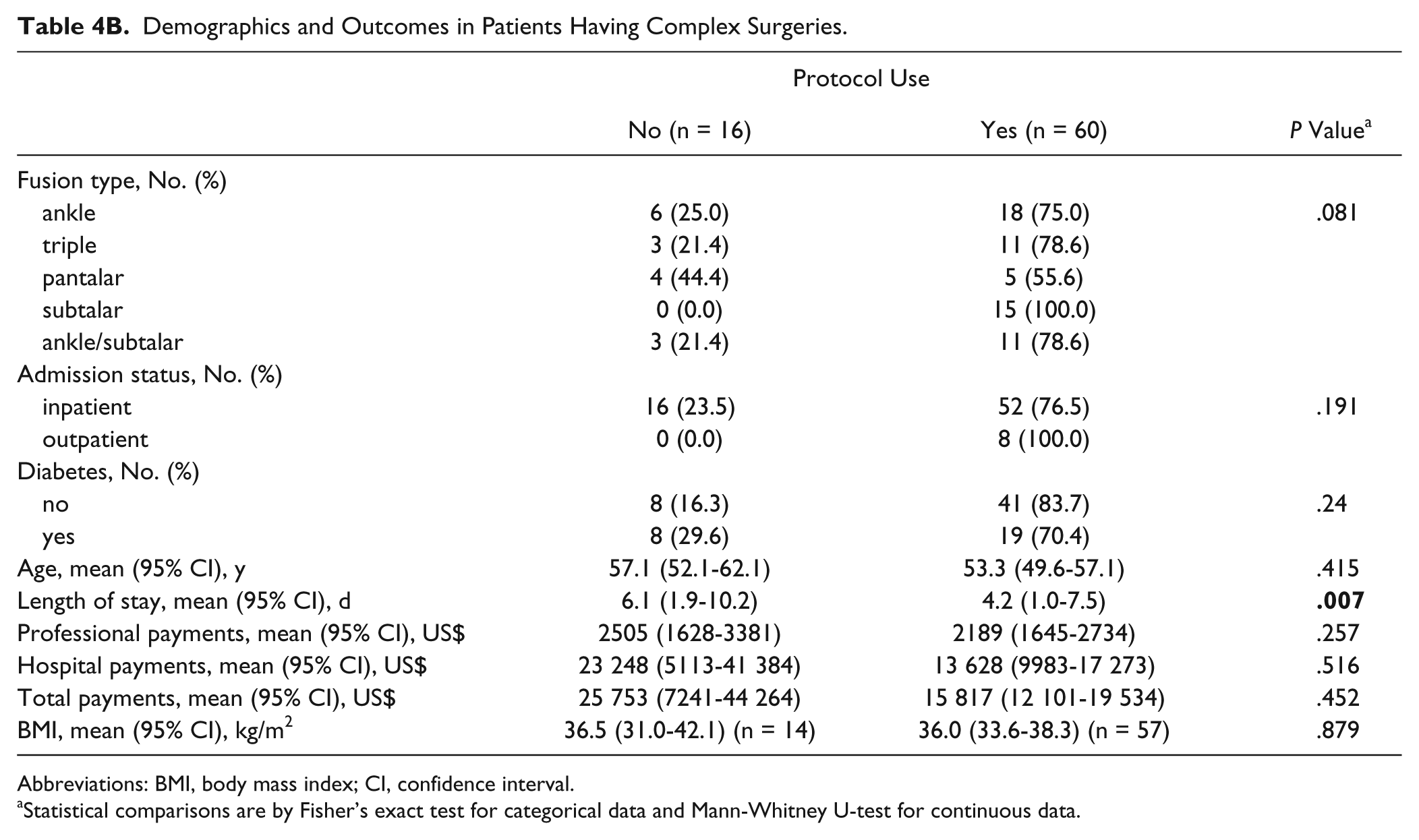
Abbreviations: BMI, body mass index; CI, confidence interval.
Statistical comparisons are by Fisher’s exact test for categorical data and Mann-Whitney U-test for continuous data.
Steroids were used in 23 patients as part of the pain protocol. There were no significant differences with respect to gender, age, BMI, diabetes, or type of surgery performed between those who did or did not receive steroids. The LOS or payments were not different based on the use of steroids. Patients on the multimodal pain protocol were more likely to have received steroids (Table 2).
Discussion
The underlying concept of multimodal postoperative analgesia 3 is that the interdiction of the pain generation mechanism at several different points in the pathway is more effective than relying on a single locus of intervention.5,8,11-13 By blocking pain generation and perception through multiple pathways, the multimodal protocol serves to potentiate the effect of each 1 individually. Peripherally, inhibition of inflammatory and pain generation is achieved through nonsteroidal anti-inflammatories, specifically the COX-2 inhibitors. More proximally in the pathway, in the dorsal horn ganglia of the spinal cord, excitation of the pain transmitting neurons is inhibited by gabapentinoids (gabapentin and pregabalin) as well as by opioids. Centrally, within the brain, inhibition of the perception of pain is provided by acetaminophen, opioids, and possibly COX-2 inhibitors. The main goal of therapy is to improve patient recovery while reducing the need for opioids, thereby decreasing unwanted side effects such as nausea, vomiting, sedation, and respiratory depression.
The general structure of multimodal therapy revolves around specific medications given preoperatively, intraoperatively, and postoperatively. Preoperative medications (gabapentin/pregabalin, long-acting opioid, steroid, acetaminophen, COX-2 inhibitor) are directed at all aspects of the pain generation pathway, with the intent being to prevent or minimize the initiation of pain. Intraoperative treatment includes the use of spinal or regional anesthesia, employment of supplemental peripheral blocks, and in many of the arthroplasty studies, an injected cocktail that includes long-acting local anesthetic, morphine, and steroid into the surgical area. Postoperatively, the medications used include COX-2 inhibitors, a scheduled long-acting opioid, scheduled acetaminophen, and added short-acting opioid as needed for breakthrough pain. The majority of studies reserve parenteral narcotics for failure of pain control using the oral protocol. There is considerable variability in the implementation of multimodal therapy, primarily surrounding the use of steroids and the postoperative use of gabapentin/pregabalin.
The most common metrics used to measure the efficacy of multimodal therapy are opioid use, patient-centered pain ratings, functional recovery after surgery, and postoperative complications. Most studies have demonstrated an opioid-sparing effect of multimodal therapy following total joint replacement,5,9 spine surgery, 10 and shoulder surgery. 2 However, a prospective randomized study of 56 patients undergoing ankle surgery did not see a decrease in opioid use postoperatively. However, this study did not use the postoperative component of the protocol, as everyone received PCA with oral opioid/acetaminophen as needed. 14 Similarly, postoperative pain scores are generally decreased in patients receiving multimodal therapy following total joint replacement,4,7,9 spine surgery, 10 and shoulder surgery, 2 although this was not found in the only study involving ankle surgery. 14 Consistent with these findings of diminished pain, patients have been found to have quicker return of function, as measured by procedure-specific physical therapy measures.1,2,4,7,9,10 Also commensurate with the opioid-sparing effects of multimodal therapy, several narcotic-related complications (nausea, altered mental status, etc) have sometimes been found to be less frequent.7,10
Notwithstanding the previous studies that demonstrated the opioid-sparing effects of multimodal therapy, there remain concerns over the potential for overprescription of narcotics postoperatively. None of the patients in the current study required treatment for overnarcotization, as measured by the use of Narcan. In addition, the use of long-acting oxycodone, which is most highly associated with narcotic abuse, was limited to 48 hours, specifically to minimize the potential for abuse.
The outcome metric used in the present study, length of stay following surgery, has been less commonly reported. In total joint arthroplasty, 2 studies reported a decrease in LOS when using multimodal therapy in retrospective studies.7,9 Pagnano et al, 7 using a protocol that included peripheral nerve blocks for postoperative analgesia, found a decrease in LOS from 5.0 days to 2.8 days in patients undergoing total hip and knee arthroplasties when compared to historical controls. Using controls drawn from the period just prior to the implementation of multimodal therapy, Peters et al 9 reported decreased LOS for total hip patients from 3.7 days to 2.5 days and for total knee patients from 3.1 days to 2.5 days. However, 2 other studies did not have such findings.4,6 In a prospective randomized study examining the effects of pregabalin and dexamethasone on postoperative pain following total hip arthroplasty in 120 patients, Mathiesen et al 6 did not find any differences in LOS, although they did observe an opioid-sparing effect in the study protocol. In another prospective randomized study of 60 patients undergoing total hip arthroplasty, Lee et al 4 also did not find any difference in LOS in the multimodal protocol group, although both study groups received the same intraoperative wound injection regimen.
The main limitation of the current study is that it is a retrospective comparison study of concurrent nonrandomized patients undergoing major hindfoot or ankle fusion surgery either with or without the benefit of multimodal analgesic therapy. Since the period included in the study extended before the time of our institution’s having an integrated electronic medical record, it was not possible to accurately measure either opioid administration or pain scores for the entire study group. However, administrative data were available to permit precise determination of LOS for all patients, and all clinical notes were obtainable for manual review to determine comorbidities. Although not methodologically pure as a randomized prospective study, it does provide the first evidence in this population of patients that the use of multimodal therapy reduced the LOS. This was observed in patients undergoing uncomplicated hindfoot/ankle fusions (1.6 days LOS; 95% CI, 1.4-1.9 vs 3.2 days LOS; 95% CI, 2.5-3.9; P < .001) and those having revision or otherwise complicated procedures (4.2 days LOS; 95% CI, 1.0-7.5 vs 6.1 days LOS; 95% CI, 1.9-10.2; P < .007). The use of spinal anesthesia or other regional blocks did not decrease the LOS, which suggests that its use alone does not confer partial benefits of multimodal pain management. As might be expected in a payment system that is based on fixed payments centered on diagnostic related groups (DRGs), the use of multimodal therapy did not result in any difference in reimbursement for either the surgeon or the hospital. However, it seems reasonable to infer that the decreased LOS associated with multimodal therapy would improve the net financial balance for the hospital since overall hospital expenditures decrease per episode of care as the LOS is reduced. In a hospital that consistently runs a very high census, such as ours, reducing LOS also has the added advantage of freeing up hospital beds for additional patients to be admitted.
Patients with Charcot joints undergoing ankle/hindfoot fusions did not have any significant reduction in their LOS associated with use of the pain protocol. Whether this is due to the inherent decrease in postsurgical pain due to their neuropathy or related to their more complicated comorbidities cannot be ascertained from this study. The rationale for keeping this group of patients in the study is the observation that not all neuropathic patients with Charcot joints are the same with respect to the degree of their neuropathy. For instance, not all patients with Charcot joints lack protective sensation to Semmes-Weinstein monofilament 5.07. Since there is no universally accepted way to identify the neuropathic patients who might feel enough postoperative pain to benefit from the pain protocol, they were included in the study but stratified for analysis.
There were several limitations to the current study. As noted, this was a nonrandomized retrospective study, which entailed all the disadvantages of such analyses. Although the patients receiving the pain protocol were younger than the control group (53.9 vs 59.7 years; P < .003), there were no differences in the known comorbidities between the groups. However, in the complex surgery group in which no age difference existed between the pain treatment groups, the significant LOS difference persisted. The selection of patients for receiving the pain protocol was left to the surgeon’s discretion. As it became clear that patients were doing better using the pain protocol (primarily the surgeons’ perception of less pain in their patients the day after surgery), it was used more consistently for major hindfoot/ankle fusions. Based on the initial iteration of the pain protocol in our department, it was thought that steroids were essential to the success of the protocol. Since there was a reluctance to use the protocol in diabetic patients perioperatively due to the potential for hyperglycemia, it was infrequently used. However, once steroids were removed from the pain protocol secondary to a department-wide re-evaluation of the pain protocol, it became routinely used in diabetic patients. This change is supported by the current analysis stratified based on steroid use, which did not reveal any significant differences in LOS, as has been noted previously. 6 Other reports also demonstrated that steroids are not universally employed in multimodal therapy for total joint arthroplasty4,7-9 or ankle surgery. 14
In conclusion, the use of multimodal therapy for perioperative pain control was shown to be associated with reduced hospital stays for patients undergoing ankle or hindfoot fusions. This was seen regardless of the degree of surgical complexity or presence of specific comorbidities such as diabetes or rheumatoid arthritis. The use of steroids as a component of multimodal therapy did not appear to be critical to the reduction in hospital length of stay.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.