
Abstract
Background:
Irreparable peroneus brevis tendon tears are uncommon, and there is scant evidence on which to base operative treatment. Options include tendon transfer, segmental resection with tenodesis to the peroneus longus tendon, and allograft reconstruction. However, the relative effectiveness of the latter 2 procedures in restoring peroneus brevis function has not been established.
Methods:
Custom-made strain gage–based tension transducers were implanted into the peroneus longus and brevis tendons near their distal insertions in 10 fresh-frozen cadaver feet. Axial load was applied to the foot, and the peroneal tendons and antagonistic tibialis anterior and posterior tendons were tensioned to 50% and 100% of physiologic load. Distal tendon tension was recorded in this normal condition and after sequential peroneus brevis-to-longus tenodesis and peroneus brevis allograft reconstruction. Measurements were made in 5 foot inversion/eversion and plantarflexion/dorsiflexion positions.
Results:
Distal peroneus brevis tendon tension after allograft reconstruction significantly exceeded that measured after tenodesis in all tested loading conditions (P ≤ 0.022). With 50% of physiologic load applied, peroneus brevis tension was 1% to 28% of normal (depending on foot position) after tenodesis and 73% to 101% of normal after allograft reconstruction. Under the 100% loading condition, peroneus brevis tension was 6% to 43% of normal after tenodesis and 88% to 99% of normal after reconstruction with allograft. Distal peroneus longus tension remained within 20% of normal under all operative and loading conditions.
Conclusion:
Allograft reconstruction of a peroneus brevis tendon tear in this model substantially restored distal tension when the peroneal tendons and their antagonists were loaded to 50% and 100% of physiologic load. Tenodesis to the peroneus longus tendon did not effectively restore peroneus brevis tension under the tested conditions.
Clinical Relevance:
Because tenodesis was demonstrated to be ineffective for restoration of peroneus brevis function, this procedure may result in an imbalanced foot clinically.
Introduction
Tears of the peroneal tendons are an uncommon but frequently underdiagnosed source of retromalleolar ankle pain.4,6,10 With few exceptions, available clinical data regarding this pathology comprise only case series with limited numbers of patients,1,4,8,9,11,13,17-19,21 expert opinions,3,6,7,10,16,23,24 and case reports.14,15 The lack of clinically relevant information regarding the functional outcome that may be expected with each treatment option has hindered decision making when this diagnosis is encountered. Most often, if more than half of the diseased tendon is deemed compromised during operative evaluation, tenodesis to the remaining healthy peroneal tendon has been advocated somewhat arbitrarily.9,18 However, there is no evidence that biomechanics of the native foot can be approximated by tenodesis. Deep toe flexor tendon transfers have also been recommended, even when peroneal muscle excursion and functionality remain well preserved,8,18 ignoring the value of the peroneal muscle unit. Objective measures of functional outcome after tendon transfer are scant, but there is evidence that neither peak eversion force nor balance can be restored through this operation when there is concomitant peroneus longus and brevis insufficiency. 20
Recently, reconstruction of the affected peroneal tendon using semitendinosus allograft has produced satisfactory clinical results, challenging the tenodesis mindset.11,13-15 Because there is a lack of empirical evidence supporting either of these operative approaches, this study was designed to directly measure and compare distal peroneal tendon tension in response to controlled proximal tendon force application after each of the procedures, in the setting of a degenerative peroneus brevis tendon and normal peroneus longus tendon. We hypothesized that physiologic tension at the insertions of the peroneal tendons after an irreparable tear of the peroneus brevis can only be restored by reconstructing the injured tendon and cannot be reestablished by tenodesis to the healthy peroneus longus tendon.
Materials and Methods
Specimen Preparation
Ten fresh previously frozen lower legs from different donors, sectioned mid-tibia, were used (mean donor age 54, range 35 to 69; 9 male, 1 female). Soft tissues were removed to expose the peroneus longus, peroneus brevis, tibialis anterior, and tibialis posterior tendons, and a stainless steel rod was cemented into the medullary canal of the tibia to allow attachment to the load application device. The skin and subcutaneous tissues overlying the peroneal tendons on the lateral aspect of the foot were removed, as were plantar tissues overlying the region of the insertion of the peroneus longus tendon on the base of the first metatarsal.
Tendon force transducers
A 20-mm-long slit was created in the substance of the peroneus longus and brevis tendons adjacent to their insertions on the first and fifth metatarsal bases, respectively, using a blunt probe. A custom-made strain gage-based tension transducer was inserted into each slit and secured using small suture loops to maintain alignment with the tendon axis. Each transducer was fabricated from a thin, contoured stainless steel plate to which a foil strain gauge (EA-06-062AQ-350/LE, Vishay Precision Group, Inc, Wendell, NC) was bonded (Figure 1). The strain gauge was aligned with the longitudinal axis of the transducer body, and the gauge and connecting wires were sealed with polyurethane sealant (M-Coat A, Vishay Precision Group). The transducer was shaped such that, when inserted into the tendon and secured with the suture loops, any tensile loading subsequently experienced by the tendon elastically deformed the transducer body, the deformation was sensed by the strain gauge, and its amplified output was recorded.
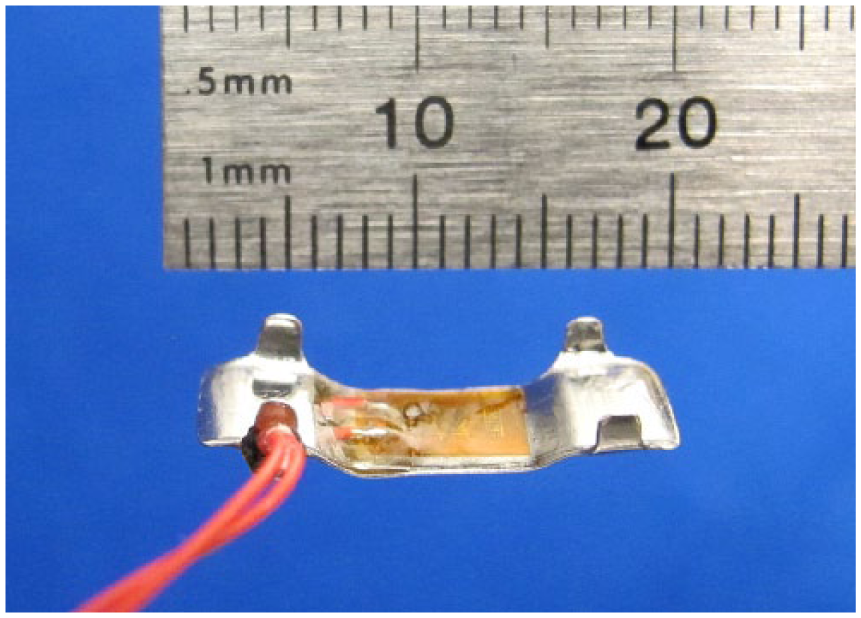
Custom-made tendon force transducer. A strain gauge senses deformation of the transducer body as the tendon is loaded. Integral tabs and suture tacks maintain sensor alignment with the tendon axis.
At the conclusion of testing of each specimen, the first and fifth metatarsals and the associated peroneal tendons and implanted transducers were dissected free and the tendons were subjected to stepwise tensile loading in 2-N increments using a servohydraulic materials testing machine. The transducer outputs at each increment of tension were documented and the resulting second or third-order polynomial best-fit calibration curves were used to convert the transducer signals recorded during the experiment into units of force (newtons) (Figure 2).
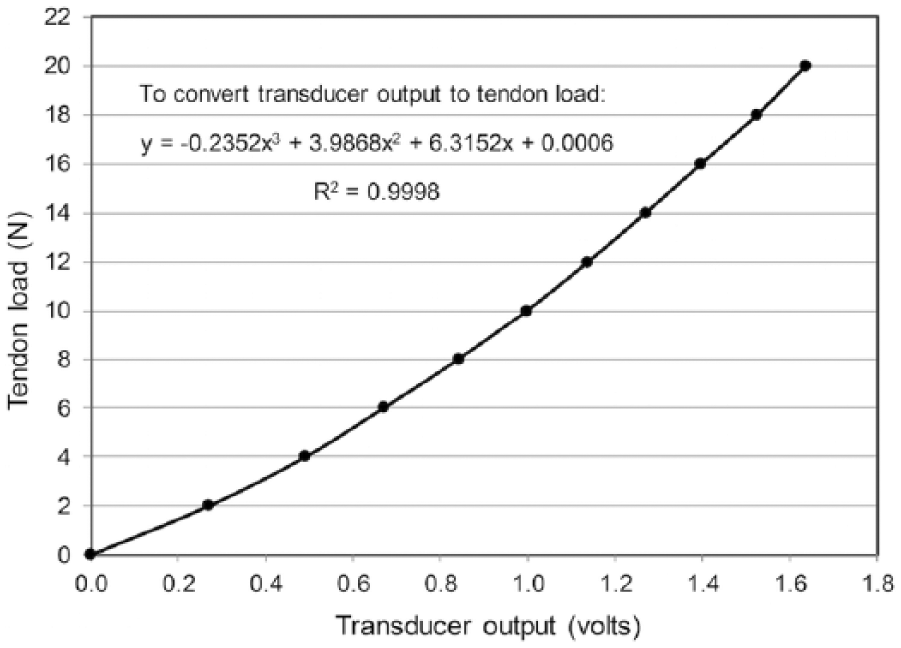
Representative calibration curve relating transducer response to applied tendon loads.
Load application
Each specimen was mounted in a loading device incorporating a vertical linear bearing carriage to which the tibia was fixed and through which compressive axial loading was applied to the foot using a cable, pulleys, and a 25-kg weight (Figure 3). The axial load applied during all measurements was the sum of the mass of the 25-kg weight plus the mass of the foot and the bearing carriage, totaling approximately 28 kg or 275 N. This load countered the tensile forces applied to the tendons and maintained firm contact between the sole of the foot and the testing device’s base plate.
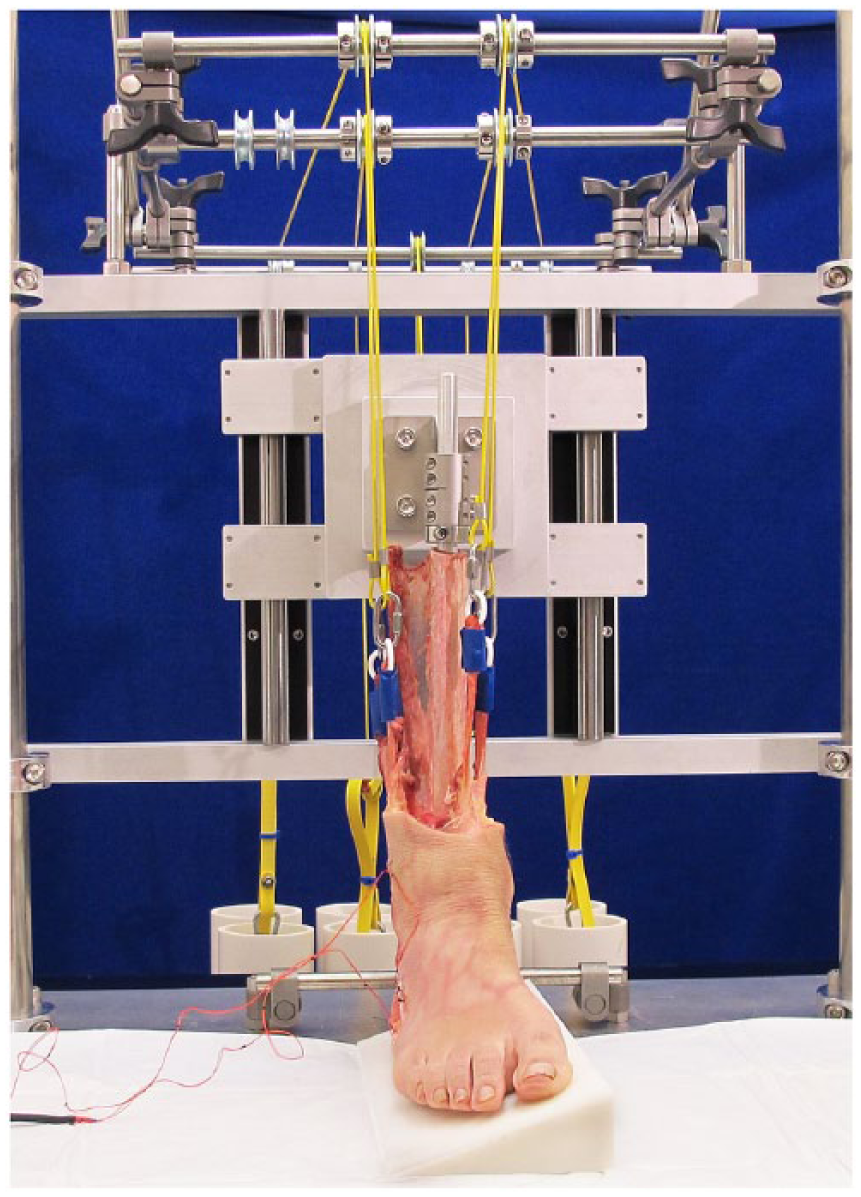
Specimen loading apparatus. Tendon tensile loads and compressive axial foot load were applied using weights and cables. In this image, the foot has been placed in 20 degrees of inversion using a wedge beneath the sole of the foot.
The proximal ends of the peroneal tendons and tibialis anterior and posterior tendons were connected to a system of cables, pulleys, and weights allowing simultaneous application of tensile loads to each. Two tendon loading levels were applied, approximating 50% and 100% of the load experienced by each tendon in vivo at the midstance phase of gait.5,12 For 50% loading, these loads were 10, 25, 31, and 35 N for the peroneus brevis, peroneus longus, tibialis anterior, and tibialis posterior, respectively, and the load magnitudes were doubled to achieve 100% loading. The weights were raised and lowered as needed to unload and load the tendons using a modified hydraulic motorcycle jack.
Distal tendon force measurements were obtained with the foot oriented sequentially in 10 degrees of eversion, neutral, 20 degrees of inversion, 10 degrees of plantarflexion, and 10 degrees of dorsiflexion. These positions were achieved by interposing wedge-shaped blocks between the plantar surface of the foot and the testing device’s base plate. After documenting tendon forces with the foot in its native condition, the complete series of measurements was repeated after tenodesis of the peroneus brevis tendon to the peroneus longus tendon and after allograft reconstruction of the peroneus brevis tendon.
Operative technique
To approximate a frequent clinical scenario, we simulated an irreparable tear of the peroneus brevis tendon behind the lateral malleolus in the region in which the avascular zone of the tendon is located. 22 With the foot in neutral position and the foot and tendons loaded as described for the 50% loading condition, the desired proximal and distal extents of the tendon defect were marked with ink 5 cm distal to the tip of the fibula and extending 8 cm proximally to avoid fibular impingement. 3 The peroneus brevis tendon was sutured to the adjacent peroneus longus tendon at the marked locations using no. 2 FiberWire suture (Arthrex, Naples, FL), and the intervening 8-cm tendon segment was resected, resulting in a standardized peroneus brevis-to-longus tenodesis. Distal peroneus brevis and peroneus longus tendon tensions were then documented under each of the loading conditions and foot orientations described above.
After completion of the tendon force measurements in the tenodesed condition, specimens were again loaded to the 50% level and a 2-cm longitudinal midsubstance incision was created in each stump of the remaining peroneus brevis tendon to incorporate an allograft. Peroneal allografts obtained from other fresh-frozen cadaver specimens were then woven through the incisions using a Pulvertaft technique and secured using FiberWire suture (Figure 4). 2 The entire range of distal tendon force measurements was then repeated.

Lateral aspect of the foot after performing peroneus brevis reconstruction using a tendon graft. The peroneus brevis tendon force transducer is partially visible near the tendon’s insertion on the base of the fifth metatarsal.
Statistical Analysis
After completion of all measurements and calibration of the tendon force transducers as described above, the distal tendon tensions measured after each operative procedure were expressed as percentages of normal and compared using paired Student t tests.
Results
Under 50% of stance-phase tendon load, peroneus brevis tendon tension adjacent to its insertion on the base of the fifth metatarsal ranged from 1% to 28% of normal, depending on the foot position, after peroneus brevis-to-longus tenodesis. After reconstruction of the peroneus brevis with allograft, tension in the region of its insertion increased from 73% to 101% of normal. Tension in the peroneus longus tendon near its insertion site was 102% to 117% of normal after tenodesis, and 84% to 93% of normal after allograft reconstruction of the peroneus brevis. For both tendons, the treatment outcomes differed significantly in each evaluated foot position, with P values ≤.022 (Tables 1 and 2).
Tension at Distal Peroneus Brevis Tendon Under 50% of Physiologic Midstance-Phase Tendon Loading Condition, Expressed as Percentage of Normal ± SD.
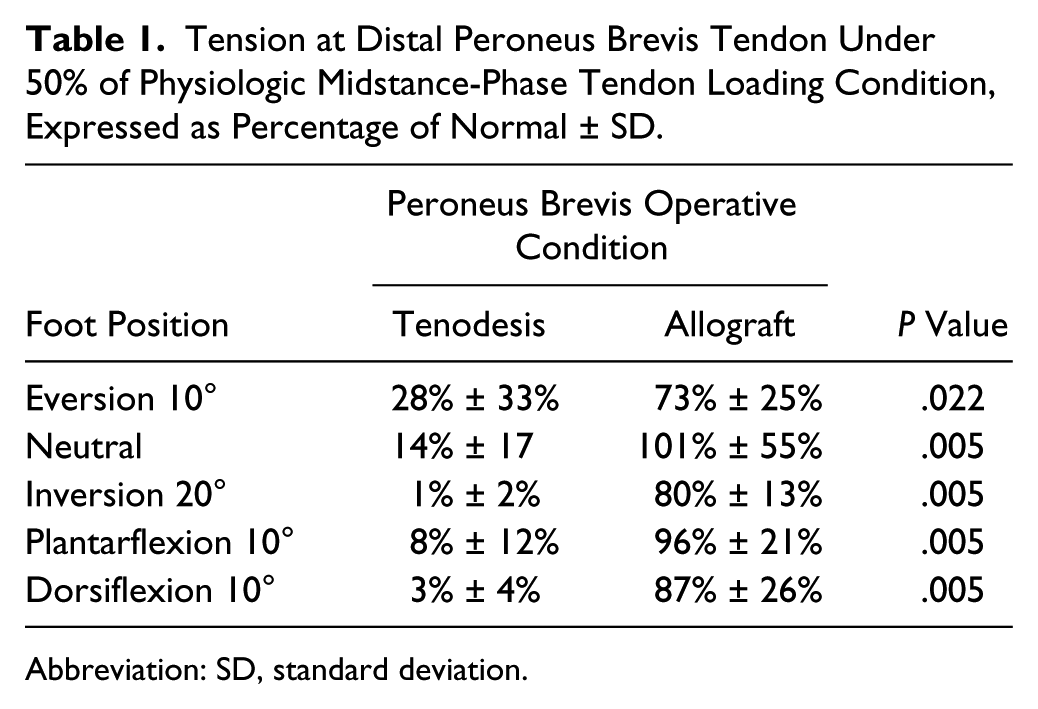
Abbreviation: SD, standard deviation.
Tension at Distal Peroneus Longus Tendon Under 50% of Physiologic Midstance-Phase Tendon Loading Condition, Expressed as Percentage of Normal ± SD.
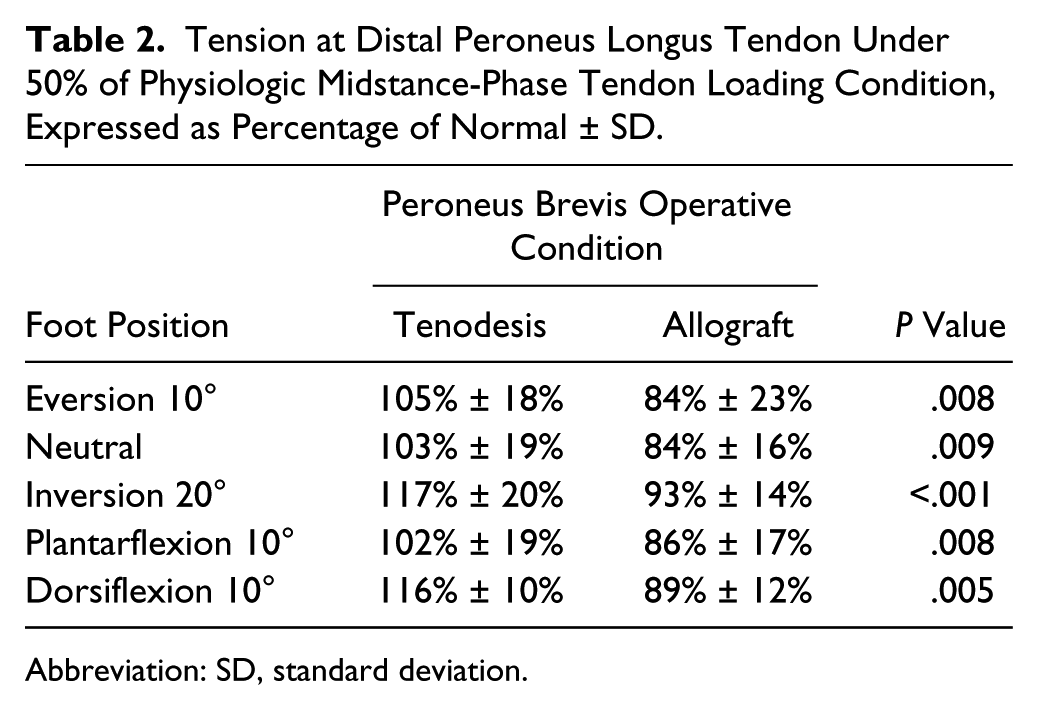
Abbreviation: SD, standard deviation.
Under the 100% loading condition, tension in the distal peroneus brevis tendon ranged from 6% to 43% of normal after tenodesis and from 88% to 99% of normal after repair with allograft, depending on the foot position. Tension in the distal peroneus longus tendon was 101% to 120% of normal and 94% to 101% of normal after tenodesis and peroneus brevis allograft reconstruction, respectively. For both tendons the treatments differed significantly, withP values ≤.022, in all comparisons except for peroneus longus tension in everted and neutral foot positions (Tables 3 and 4).
Tension at Distal Peroneus Brevis Tendon Under 100% of Physiologic Midstance-Phase Tendon Loading Condition, Expressed as Percentage of Normal ± SD.
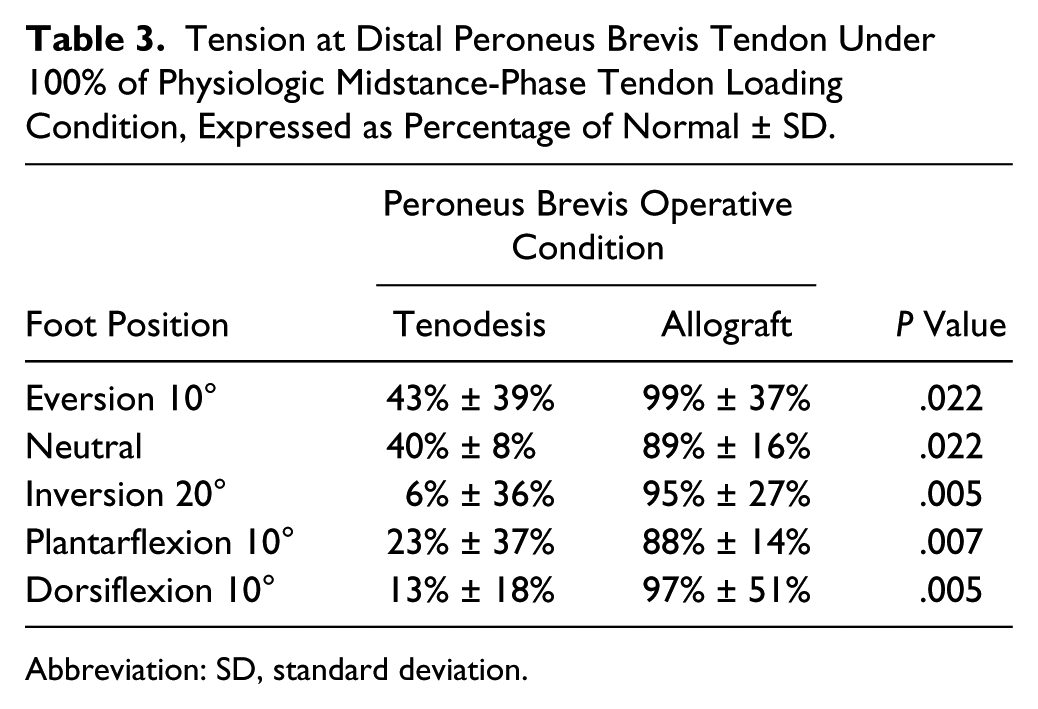
Abbreviation: SD, standard deviation.
Tension at Distal Peroneus Longus Tendon Under 100% of Physiologic Midstance-Phase Tendon Loading Condition, Expressed as Percentage of Normal ± SD.
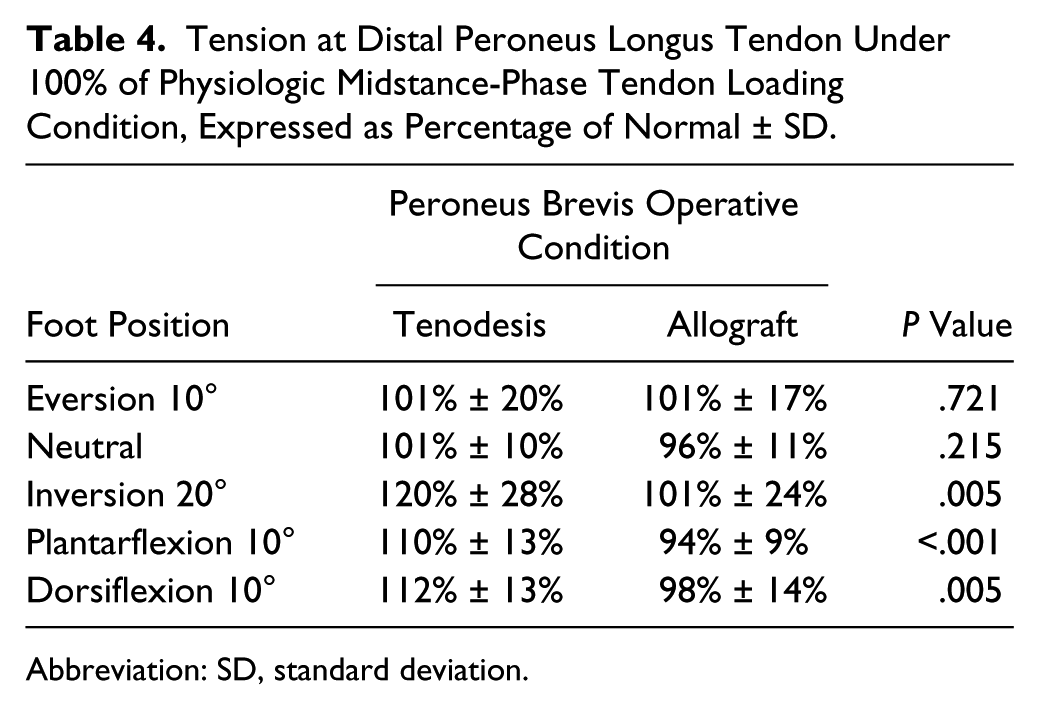
Abbreviation: SD, standard deviation.
Discussion
Tenodesis of peroneus brevis tendon stumps to the adjacent healthy peroneus longus tendon after excision of a degenerative segment is commonly performed based on the unsubstantiated belief that this will restore normal peroneus brevis tension at its insertion on the fifth metatarsal without affecting the tension in the distal peroneus longus tendon. Our findings, based on direct measurement of distal peroneal tendon tension, indicate that this is not the case. However, the empirical data demonstrated that the more obvious direct approach of peroneus brevis reconstruction by means of an allograft can reestablish substantially normal function of the peroneus brevis musculotendinous unit with minimal negative influence on the healthy peroneus longus tendon.
According to our findings, peroneus brevis-to-longus tenodesis may contribute to an imbalanced foot condition. Because the peroneus brevis is one of the main dynamic stabilizers of the normal ankle joint and since chronic lateral ankle instability and degenerative tears of the peroneal tendons often coexist, 4 the striking reduction in peroneus brevis force transmission by more than 90% documented with the foot inverted and the reduction of 60% or more measured in neutral inversion/eversion may have a particularly negative effect on efforts to achieve frontal plane ankle stability.
In addition to the likely unbalancing effects of markedly diminished peroneus brevis effectiveness, peroneus brevis-to-longus tenodesis altered the tension measured in the peroneus longus tendon near its insertion on the base of the first metatarsal. Increased tension ranging from 1% to 20%, depending on foot position and proximal tendon load, was documented, which was unsurprising given that the peroneus brevis muscle force was directly transferred to the peroneus longus tendon proximal to the defect location. Although the clinical effects of sustained increased plantarflexion force on the first ray are unknown, it is possible that it may drive the hindfoot into varus, further weakening ankle eversion power and potentially leading to further peroneal tendon degeneration.6,9 This may be of particular concern in patients presenting with both an irreparable peroneus brevis tendon tear and cavus foot morphology.
According to our results, the potentially deleterious changes in tendon tension associated with peroneus brevis-to-longus tenodesis may be avoided by reconstructing the degenerative peroneus brevis tendon, assuming that the peroneus brevis muscle itself is normal. Interestingly, both distal peroneus brevis force and distal peroneus longus force were slightly reduced after this procedure compared with their normal, preoperative magnitudes. We attribute this phenomenon to increased resistance to tendon gliding resulting from weaving and suturing of the allograft to the stumps of the peroneus brevis, and to alterations in the normal soft tissue anatomy resulting from accessing the tendons operatively.
As with most laboratory studies, there are limitations associated with the methodology used in this investigation. The novel tendon force transducers integral to the study were designed to self-align with the tendon when inserted into a longitudinal slit, and they were secured with small sutures. However, their outputs may have been affected by subtle changes in their alignment relative to the tendon axis during the course of testing each specimen, as well as by incidental contact with adjacent soft tissues. Additionally, because of their proximity to the tendon insertion sites, they were sensitive to the tendon’s spatial orientation relative to the metatarsal base during calibration, which may have introduced slight error. Further, we recognize that the static loading to which the foot and tendons were subjected during the experiment was a gross simplification of dynamic physiologic loading. Finally, there is no doubt that the results of both tenodesis and allograft reconstruction are technique and healing dependent. While controlled constant tension was applied to both the peroneus brevis and the peroneus longus tendons during the operative procedures in our study, the tension applied clinically is variable, unquantified, and likely to affect the result.
In summary, allograft reconstruction of a peroneus brevis tendon tear in this model substantially restored distal tension when the peroneal tendons and their antagonists were loaded to 50% and 100% of physiologic load. Tenodesis to the peroneus longus tendon did not effectively restore peroneus brevis tension under the tested conditions. Because tenodesis was demonstrated to be ineffective for restoration of peroneus brevis function, this procedure may result in an imbalanced foot clinically.
Footnotes
Acknowledgements
The authors acknowledge Anatomy Gifts Registry for procurement of anatomic specimens used in this study.
Author Note
The investigation was performed at Duke University Medical Center, Durham, NC.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.