
Abstract

Keywords
The Achilles tendon (AT) is the strongest tendon in the human body, capable of heavy loading. 5 Despite its strength, 17 it is also one of the most commonly injured tendons. 25 The incidence of AT ruptures is between 7 and 37 per 100 000 person-years, 4 with most of these injuries occurring during athletics in men ages 30 to 40 years. 19 The AT reaches maximum tension during the eccentric phase of muscle/tendon action, 26 a mechanism that is associated with basketball, tennis, and football, all of which are sports commonly associated with AT ruptures. 35
Diagnosis
Rupture of the AT is usually considered chronic if left untreated for 4 to 6 weeks. 20 Occasionally, the AT will rupture without the patient noticing the loud “pop” or “snap” commonly associated with this injury, not always initially identifying the injury as significant. Patients may further delay seeking treatment as pain and swelling decrease over time, leading the patient to believe that the injury is minor and improving. 20 In some cases, patients electing nonoperative treatment can develop persistent symptoms of pain, weakness, and dysfunction due to elongation of the tendon during recovery.
In addition to a thorough injury history, diagnosis of chronic AT ruptures should always begin with a physical examination. The calf squeeze test and the knee flexion test are two reliable methods of diagnosis. 12 The calf squeeze test or Thompson test is administered with the patient lying prone with the foot off of the examining table. If the tendon is intact, the ankle will plantarflex when the calf is compressed by the examiner. If the tendon is ruptured, the ankle will remain static (Figure 1). The knee flexion or “extensor lag” test is administered with the patient lying prone with both knees bent at 90°. If the AT is completely disrupted, the affected ankle will fall into a neutral or dorsiflexed position compared with the unaffected ankle. 12 Of note, the palpable gap commonly seen after acute AT ruptures 15 is not always present in the chronic setting.

The Thompson test. Photograph illustrating the absence of plantarflexion with squeezing of the calf in the prone position signifies a rupture of the Achilles tendon.
Ultrasound is an effective imaging method because it correlates well with the histopathologic findings, although it is operator dependent. 24 Magnetic resonance imaging (MRI) should be considered if ultrasound is unavailable or equivocal. MRI provides extensive information on the internal morphology of the tendon and the surrounding structures and is useful in evaluating the various stages of chronic degeneration and in differentiating between peritendinitis and tendinopathy. 24 Areas of mucoid degeneration are shown on MRI as zones of high signal intensity on T1- and T2-weighted images (Figure 2). 24 MRI can also serve as a perioperative guide to surgical planning, as it is easier to visualize the entire tendon length with ultrasound imaging.

Sagittal T2-weighted magnetic resonance imaging.
Treatment of Chronic AT Ruptures
When a chronic AT rupture is identified after appropriate examination and imaging, several treatment options are available. The following sections review evidence-based recommendations (Table 1) for the treatment of chronic AT ruptures. A summary of evidence-based recommendations can be found in Table 2.
Levels of Evidence and Grades of Recommendation.
Summary of Grades of Recommendation.
Nonoperative Treatment
Most patients who seek treatment for chronic AT rupture will require surgical intervention to return to an acceptable range of activities and function. Nonoperative approaches have evolved in the treatment of AT ruptures from casting to functional rehabilitation, with improved results. 27 However, these improved results are likely predicated on detecting and treating the rupture early. As such, functional rehabilitation may have limited benefit for chronic AT ruptures. If nonoperative treatment is necessary, a low-profile brace such as a carbon-fiber ground reaction force ankle foot orthosis should be used.
Operative Treatment
As detailed in the following sections, several surgical options exist to treat chronic AT ruptures. The indications include patients with chronic Achilles ruptures that have failed to improve with conservative treatment measures or who wish to participate in activities that will be made difficult with a chronically lengthened and poorly functioning AT. Regardless of the technique used, pharmaceutical anticoagulation should be considered for repair or reconstruction of chronic AT ruptures, as a significantly higher rate of venous thromboembolism has been shown to occur following surgical intervention for chronic versus acute AT ruptures (P = .048) as well as elective repair of Achilles tendinopathy (P = .0069). 2
The size of the AT defect is an important factor in management. Myerson 29 described a scheme for surgical treatment of chronic AT ruptures on the basis of defect size (Table 3). The outcomes reported on various surgical treatment options for chronic AT ruptures are limited mostly to case series and case reports. For this reason, there is not necessarily a clear and predictable first-line surgical option in patients with this injury. Several factors will contribute to the treatment choice, including patient age, activity level, comorbid conditions, tolerance for surgery and recovery, and the condition of the soft tissue envelope. However, in most patients who undergo surgery, the defect size between the proximal and distal stumps of the AT will dictate which procedures may be successful, as detailed below.
Scheme for the Surgical Treatment of Chronic Achilles Tendon Ruptures on the Basis of Gap Size a .
From Myerson. 29
Primary Repair
Primary repair is an option in cases of chronic AT ruptures with less than 2 cm of retraction or in those cases in which the tendon has healed in an elongated position, resulting in laxity that reduces power and alters gait (Figure 3). In the latter scenario, a section of tendon (often there is a section of abnormal or degenerative tendon substance) must be removed to recreate the normal length and tension of the tendon prior to performing the primary repair. It is also important to release adhesions between the tendon and sheath and free up the gastrocnemius and soleus to ensure that the triceps surae moves freely following repair. Rehabilitation proceeds similar to primary repair, with early functional range of motion and protected weight bearing. 33 In a prospective case series (Level IV evidence) of 30 consecutive patients with delays in diagnosis of AT rupture of more than 4 weeks, Yasuda et al 40 performed resection of scar tissue (15-50 mm in length) between the healed stumps of the tendon prior to performing direct repair of the tendon using Krackow stitches with No. 2 nonabsorbable polyfilament in each tendon stump. Mean American Orthopaedic Foot & Ankle Society (AOFAS) scores increased from 82.8 points preoperatively to 98.1 points postoperatively. Mean postoperative Achilles Tendon Total Rupture Score was 92.0 points. At latest follow-up, none of the patients had experienced tendon reruptures or difficulty walking or climbing stairs. In addition, all athletes had returned to their preinjury levels of sports participation.
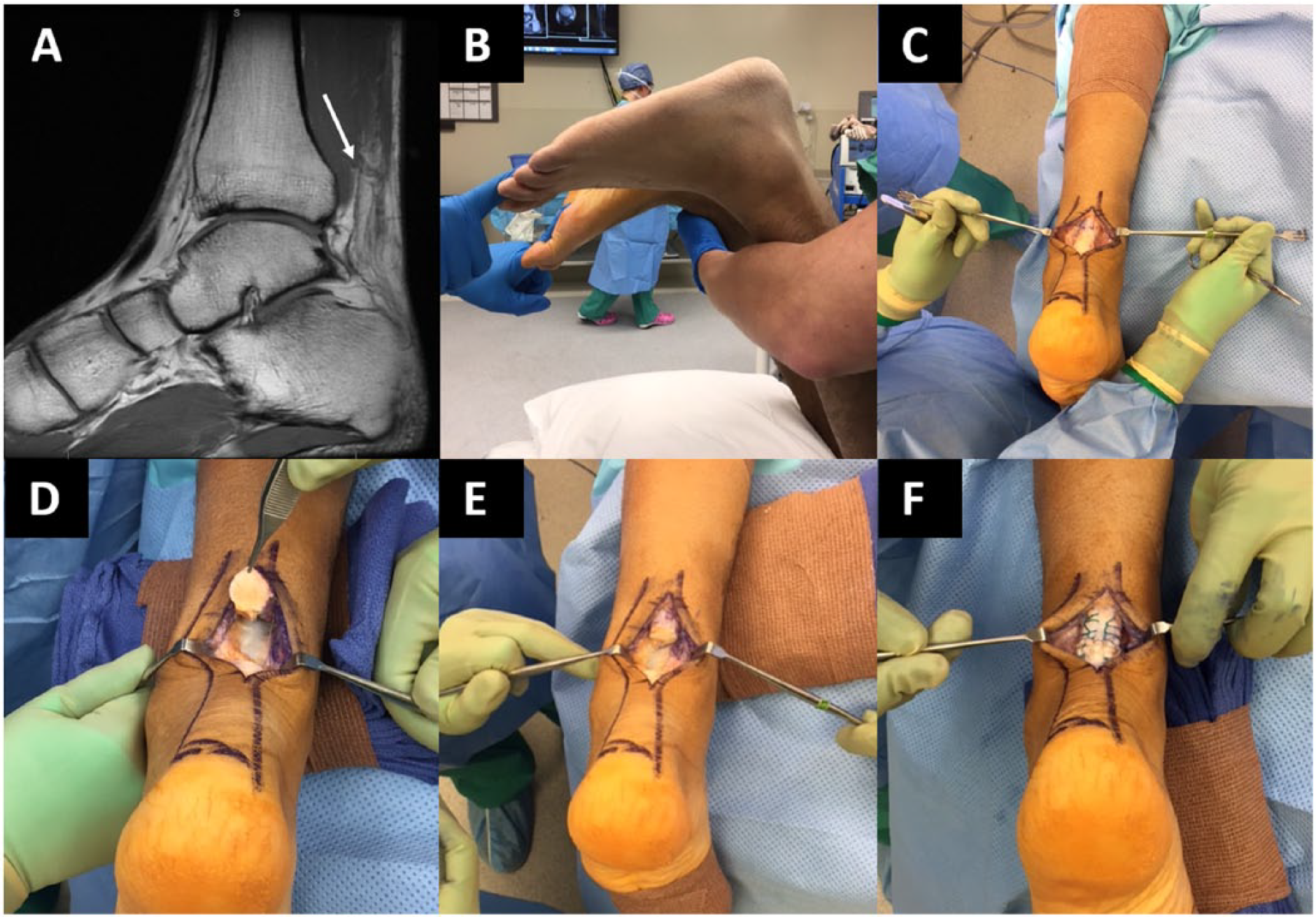
Primary repair of a chronic Achilles tendon rupture. (A) Preoperative T1-weighted sagittal magnetic resonance imaging of the left ankle in a 31-year-old man demonstrating healing (arrow) of an 11-week-old Achilles tendon rupture with laxity at the distal portion of the tendon. (B) Preoperative operating room image demonstrating left ankle extensor lag of approximately 15° compared with the contralateral side. (C) Intraoperative image demonstrating no residual tear. (D) The tendon was cut near the site of injury, with degenerative tissue shown within the tendon. (E) After resection of scar tissue between the two healed tendon stumps. (F) Following primary repair with Krackow sutures.
V-Y Tendon Plasty
V-Y tendon plasty is typically performed in cases of medium-sized (2-5 cm) defects. This procedure is performed by incising an inverted V on the proximal stump of the AT, with the apex of the V at the tendinous portion of the myotendinous junction of the AT and gastrocnemius muscle. 8 The arms of the V are made such that their length is each approximately 1.5 times that of the defect size.8,13 With larger defects (>5 cm), the arms of the V should be twice the defect size. 8 With the foot held in plantarflexion, the proximal stump of the AT is pulled carefully and slowly such that the myotendinous junction is stretched but not torn to allow reapproximation and suture repair of the two segments.
In what was defined as a retrospective comparative study (Level III evidence), Guclu et al 13 performed V-Y tendon plasty with fascia turndown in 17 patients with chronic AT rupture. However, the outcomes of these patients were not directly compared with those of another cohort, and therefore this study might be considered a case series (Level IV evidence). The patients in that study had a mean defect size of 6 cm (range, 4.5-8 cm), and the mean time from injury to operation was 7 months (range, 4-12 months). V-Y tendon plasty was performed as described above, with the repair performed using 1-0 nonabsorbable polyester suture with a modified Kessler method. In addition, a flap was prepared from the gastrocnemius aponeurosis distal to the V recession. The flap was inverted, and the anastomosis was reinforced with the flap using 2-0 absorbable polyglactin interrupted sutures. The defect between the gastrocnemius aponeurosis was repaired with 0 absorbable polyglactin running sutures. At a mean follow-up of 195 months (range, 158-226 months), no reruptures had occurred. The AOFAS score improved from a preoperative mean of 64 to 95 at latest follow-up (P < .01). All patients could perform a single-leg heel raise at follow-up. Interestingly, defect size, calf atrophy, and increased time from injury to surgery were significantly associated with decreased plantarflexion peak torque at follow-up but did not affect AOFAS scores.
In another case series (Level IV evidence) of 15 consecutive patients with missed or neglected AT ruptures, Elias et al 8 described the outcomes of V-Y lengthening and flexor hallucis longus (FHL) tendon transfer. The average time from injury to operation was 17.3 weeks (range, 1-57 weeks), and therefore not all patients included in this study had chronic AT ruptures. The authors performed V-Y tendon plasty similar to the techniques described above, though prior to repair of the stump ends, an FHL tendon transfer was performed similarly to that technique described by Elgohary et al. 7 Following repair of the proximal and distal segments using heavy nonabsorbable suture, the muscle belly of the FHL was sutured to the back of the AT at the level of the repair using absorbable suture. This was performed to create a vascular bed at the dysvascular site of the rupture. AOFAS scores improved from a mean score of 58.4 preoperatively to 94.1 at a mean follow-up of 106 weeks (P < .001). Compared with the healthy, contralateral side, 22.3% loss of plantarflexion torque was demonstrated at 60°/s (P < .01), and 13.5% loss of plantarflexion torque was demonstrated at 120°/s (P < .01) at latest follow-up. Eleven of the 15 patients (73%) were aware at the time of follow-up that the hallux interphalangeal joint no longer flexed, though this did not result in any deleterious effect on gait or function.
Given the paucity of evidence, provided by two Level IV studies, a Grade C recommendation is indicated for the use of a V-Y tendon plasty in treatment of chronic AT ruptures.
Tendon Transfer
Compared with acute AT ruptures, chronic ruptures are typically more difficult to repair, as the tendon ends are usually retracted. 21 To compensate for this, tendon transfers are a common treatment option in this scenario. An FHL tendon transfer is most commonly used,7,31,34,38,39 though a peroneus brevis tendon transfer has also been described.18,21,22
In a case series (Level IV evidence), Elgohary et al 7 described the outcomes of 19 patients (mean age, 47 years) treated for chronic AT rupture with FHL tendon transfer with concomitant gastrocnemius recession. The mean duration between injury and surgery was 16 weeks (range, 8-26 weeks). To perform the FHL tendon transfer, the FHL was divided distally, with the distal segment of the tendon sutured to the adjacent flexor digitorum longus tendon of the second toe. The remaining segment of the FHL tendon was retracted through a proximal incision and weaved through the distal AT stump in 14 cases. In the remaining 5 patients, a transverse tunnel was created in the calcaneus near the insertion of the AT. The FHL tendon was passed through the tunnel in a medial-to-lateral direction. After passing through the tunnel, the FHL tendon was woven through the proximal AT stump and tenodesed to itself. The ruptured ends of the AT were then sutured to the FHL tendon and muscle. In this case series, 7 the AOFAS score improved significantly from a mean score of 65 (range, 52-72) preoperatively to 94 (range, 76-100) at a mean follow-up of 29 months (range, 13-52 months) (P < .001). At latest follow-up, no patients had sustained rerupture, none had a dorsiflexion deficit of more than 10°, and only 1 patient had a plantarflexion deficit of more than 10°. All patients were able to perform a single-leg heel raise, compared with none of the patients preoperatively.
In a case series (Level IV evidence) of 11 patients with chronic AT ruptures, Wegrzyn et al 39 described the outcomes of a modified FHL tendon transfer procedure. Following fibrosis debridement, the average defect size was 7.4 cm (range, 2.5-10 cm). The authors’ surgical technique was similar to that described by Elgohary et al. 7 At an average follow-up of 79 months (range, 48-81 months), no reruptures had occurred. The AOFAS score improved from a preoperative mean score of 64 to 98 (range, 90-100) at latest follow-up (P < .0001). Patients returned to sports activities at an average 10 months (range, 6-18 months) postoperatively, though all at a lower level of sports than preinjury. Average ankle range of motion at latest follow-up was 12° of dorsiflexion and 45.5° of plantarflexion.
In a retrospective case series (Level IV evidence), Maffulli et al 21 performed peroneus brevis tendon transfer in 17 patients with chronic AT rupture. Intraoperatively, an ostectomy of the posterosuperior corner of the calcaneus was performed with an oscillating saw without disturbing the AT insertion site. This was performed to prevent impingement of the AT on the calcaneus and also allowed placement of the peroneus brevis tendon closer to the insertion site of the AT. The distal 3 cm of the peroneus brevis tendon was detached and passed through the proximal incision. The calcaneus was then drilled with a Beath pin from dorsal to plantar at an angle of approximately 45° to the plantar surface of the heel, and the peroneus brevis tendon was passed through and secured with a metallic or bioabsorbable interference screw. The peroneus brevis tendon was then tenodesed to the distal stump of the AT with 2.0 Vicryl sutures. No patients were lost to follow-up at a mean 4.6 years (range, 2-7 years). All patients were able to perform at least 10 single-leg heel lifts on the affected limb, though the mean peak force of the operated limb was significantly lower than that of the contralateral limb (244.6 vs 289.7 N, P < .0001). The mean Achilles Tendon Total Rupture Score had improved from 58 points (range, 35-68 points) preoperatively to 91 points (range, 75-97 points) at most recent follow-up (P = .0001). Using the Boyden classification system, 6 patients had excellent results, 10 had good results, 1 had a fair result, and none had poor results. All patients returned to their preinjury occupations at a mean of 9 weeks postoperatively, and all 13 patients who were involved in high-impact sports prior to injury were able to return to these recreational activities at a mean 6.8 months postoperatively.
In another case series (Level IV evidence) of 20 patients (mean age at operation, 43 years) undergoing peroneus brevis tendon transfer for chronic AT ruptures, Kosaka et al 18 had no reruptures at an average follow-up of 164 months. The mean AOFAS score at follow-up was 86.9, though preoperative scores were not available for comparison. Six patients (30%) returned to competitive sports, while 10 patients (50%) returned to recreational activities.
On the basis of the overall positive results demonstrated in several case series, a Grade B recommendation is indicated for the use of a tendon transfer in repair of a chronic AT rupture.
Turndown Flap
A turndown flap may be performed in cases of attempted primary repair in which a small defect still remains following approximation and suturing of the tendon ends (Figure 4). In a case series (Level IV evidence) of 10 patients with a neglected AT rupture, Esenyel et al 11 described the outcomes of a gastrocnemius fascial flap. Patients underwent surgery at a mean of 1.9 months (range, 1-3 months) following injury. The mean age at surgery was 41 years (range, 38-45 years). Intraoperatively, the tendon stumps were trimmed and repaired using No. 2-0 Ethibond thread (Ethibond, Somerville, NJ) with the ankle at maximum plantarflexion. After the tendon ends were approximated and sutured, the average remaining defect size was 3 cm (range, 2-4 cm). A 10-mm-wide central gastrocnemius aponeurosis flap was cut and freed from 3 to 4 cm proximal to the suture line. This flap was twisted 180°, drawn downward, and fixed in the distal stump with interrupted sutures. The tendon flap was then surrounded by a knitted mesh (Hyalonect; Fidia Advanced Biopolymers, Abano Terme, Italy). At a mean follow-up of 43.2 months, no reruptures were reported, and all patients returned to sports activities at their preinjury levels. The AOFAS score improved from a mean of 64.8 preoperatively to 97.8 at latest follow-up (P < .0001). No significant difference was found in dorsiflexion or plantarflexion range of motion at follow-up between the surgically repaired and healthy ankles. All patients were able to complete at least 25 heel raises.
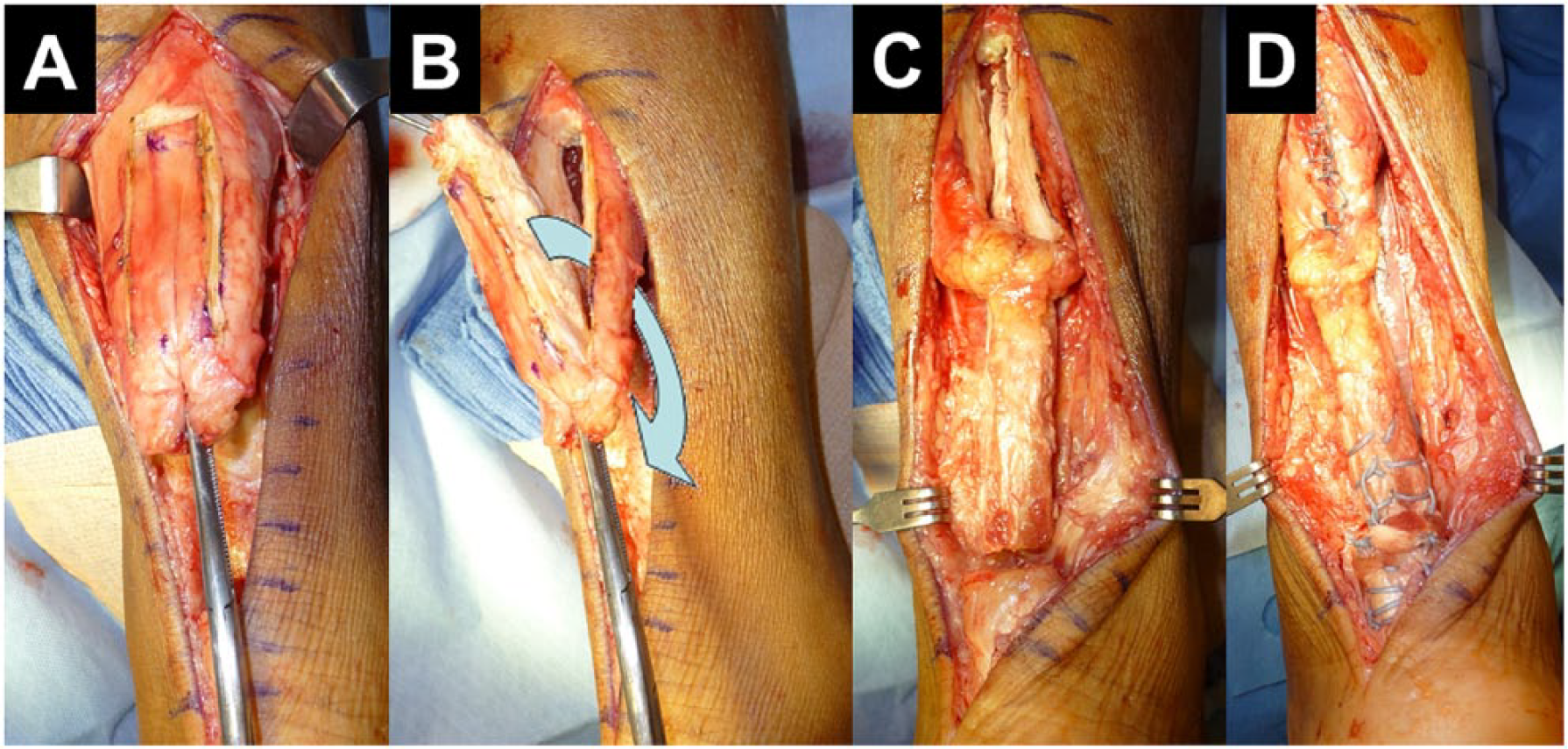
Turndown flap. (A) A central gastrocnemius aponeurosis flap is cut and freed. (B) This flap is twisted 180° (arrow), (C) drawn downward, and (D) fixed to the distal stump with sutures with closure of the gastrocnemius defect.
In a case series (Level IV evidence) of 9 patients with chronic AT ruptures, Tay et al 37 performed two turndown flaps with concomitant FHL tendon transfer. The mean patient age was 59.5 years (range, 54-75 years), and the mean duration from injury to operation was 6.3 months (range, 1-12 months). Unlike the study by Esenyel et al, 11 the authors did not initially perform primary repair of the two tendon stumps. Rather, dual 1-cm-wide turndown flaps were created from the proximal tendon and were sutured to the distal stump as described above. In addition, the FHL tendon was passed medial to lateral through the distal AT, with slack from the FHL tendon tenodesed to the lateral turndown flap and the FHL muscle belly myodesed to the medial turndown flap. The mean defect size in 9 patients was 5.6 cm (range, 4-7 cm). Six patients were available at 2-year follow-up, at which the mean AOFAS score was 94.2, though no preoperative scores were obtained for comparison. A visual analog score for pain was assessed and found to be 0 in all but 1 patient. Four patients rated the overall results of their treatment as excellent, 1 as very good, and 1 as good (none as fair, poor, or terrible).
Given the paucity of evidence, provided by two Level IV studies, a Grade C recommendation is indicated for the use of a turndown flap in treatment of chronic AT ruptures.
Allograft Reconstruction
Allograft reconstruction may be used for the surgical management of chronic AT ruptures with large defects (>3 cm) (Figure 5). This procedure is performed most commonly with the use of an AT allograft.3,14,16,30,32 The literature on allograft reconstruction is limited mostly to case reports, though Hollawell et al 16 performed a retrospective case series (Level IV evidence) of 4 patients with chronic (8-16 weeks) AT ruptures. All patients underwent tendon reconstruction with the use of an AT allograft and xenograft combination. After debriding the torn tendon stumps, the proximal and distal ends of the stumps were incised transversely to create a separation of anterior and posterior ends, into which the AT allograft was seated and sutured with 2-0 FiberWire (Arthrex, Naples, FL) with the ankle slightly plantarflexed. Next, an Inforce Reinforcement Matrix (Integra Life Sciences, Plainsboro, NJ) xenograft was cut to approximately 3 cm2 and sutured to the proximal and distal repair sites using 4-0 loop FiberWire in a running, locking fashion. In this case series, the median gap length was 4.75 cm. At a median follow-up of 37 months, the mean Foot and Ankle Outcomes Instrument core scale score was 97, and the Foot and Ankle Outcomes Instrument shoe comfort core scale score was 100. All patients were able to return to all preinjury activities at a median of 14.5 weeks postoperatively.
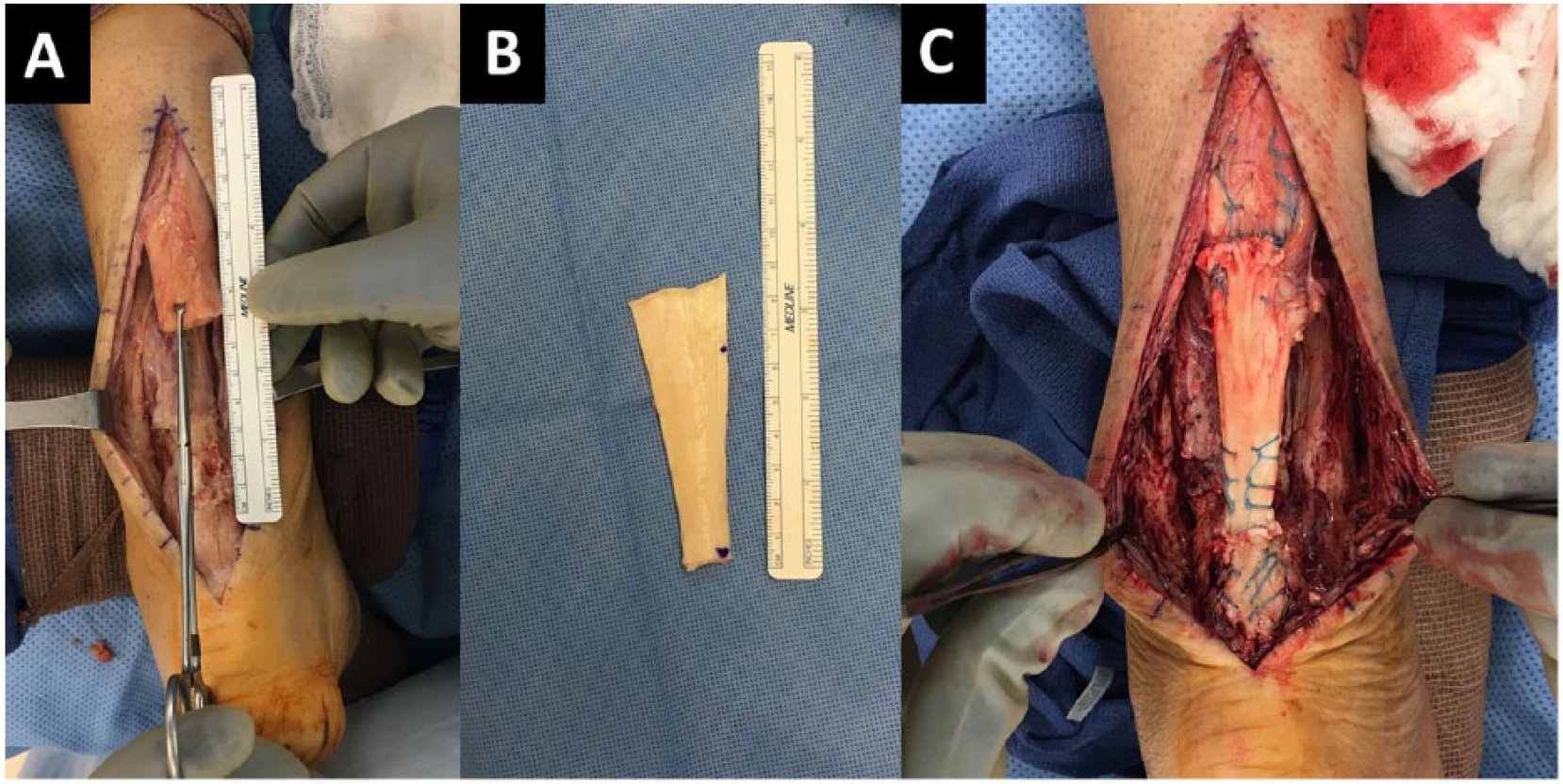
Allograft reconstruction. (A) Measurement of the defect size. (B) Achilles tendon allograft prepared on the back table. (C) Following suture repair of the Achilles tendon defect with the allograft.
Autograft Reconstruction
Autograft reconstruction of a chronic AT rupture has also been described with the use of a hamstring6,9,10,23,36 or quadriceps tendon1,28 autograft. As with allograft reconstruction, the use of an autograft may be indicated particularly in patients with large defects. In a retrospective case series (Level IV evidence) of 35 patients with symptomatic chronic AT ruptures of more than 6 weeks’ duration, Dumbre Patil et al 6 performed tendon reconstruction using a semitendinosus autograft. After debriding the frayed AT ends and removing the calcified and hard tendon, the authors measured the defect size between stumps, and if the defect size was greater than 5 cm, the authors placed traction on the proximal stump for 5 minutes before attempting end-to-end opposition. If end-to-end contact was not possible with the ankle in 10° to 20° of plantarflexion, the semitendinosus tendon was harvested. A guidewire was placed through the calcaneus approximately 1.5 cm below the native AT insertion site to create a tunnel through which the autograft was passed. The two autograft ends were then sutured together and to the proximal stump of the native tendon using Vicryl No. 2-0 sutures with the ankle in neutral position. In this case series, 6 defect sizes ranged from 5 to 9 cm. At an average follow-up of 30.7 months, no reruptures had occurred, and all patients had returned to their prerupture daily activity. Weight-bearing manual muscle testing improved from 2/5 preoperatively to 4/5 or 5/5 at latest follow-up.
In a prospective case series (Level IV evidence) of 15 patients, El Shazly et al 10 performed endoscopic-assisted reconstruction of chronic AT ruptures of at least 6 weeks’ duration using a semitendinosus autograft. Four portals were placed, with 2 superior portals located on each side 3 cm above the palpable gap of the torn AT. The inferior portals were placed 1 cm above the native AT insertion site. Hindfoot endoscopy was performed for debridement of scar tissue in the retrocalcaneal space. Using the inferolateral portal, a calcaneal tunnel was created 10 mm anterior to the AT insertion. The semitendinosus autograft was placed through the superior portals and through the proximal stump of the AT. Next, the graft ends were retrieved through the corresponding inferior portals and through the calcaneal tunnel. A biodegradable interference screw was used to fix the graft distally to the calcaneal tunnel with the ankle in neutral position. In this case series, 10 the mean gap size on preoperative MRI was 49 ± 9 mm. At a mean follow-up of 27 months, the mean AOFAS score increased from 32.6 preoperatively to 90.8 at latest follow-up (P < .05). The mean time to return to daily activities (excluding running and other sports) was 12.6 weeks. At follow-up, a nonsignificant deficit (<10%) was found using isokinetic testing between the involved and uninvolved plantar- and dorsiflexors with regard to peak torque, average power, and total work.
In a case series (Level IV evidence) of 21 patients, Maffulli et al 23 performed AT reconstruction with the use of a gracilis tendon autograft at a mean of 4.8 ± 3.3 months following injury. Prior to the procedure, an average gap of 6.8 ± 3.7 cm was present between the proximal and distal AT stumps with maximum plantarflexion and traction applied to both stumps. Following gracilis tendon harvest, the graft was passed through a small incision in the substance of the distal stump of the AT in a medial-to-lateral direction, and then through the substance of the proximal stump in a lateral-to-medial direction. The graft was then fastened to the AT at each entry and exit point with use of 3-0 Vicryl sutures. In 4 cases, the plantaris tendon was harvested, left attached distally, and used to reinforce the reconstruction. At a mean follow-up of 10.9 years (range, 8-12 years), 15 of the 21 patients (71%) were available for clinical and functional assessment. There were 2 excellent, 11 good, 2 fair, and 0 poor results. All patients were able to perform at least 10 single-leg heel lifts on the affected side, and 8 patients were able to perform at least 60 single-leg heel lifts on the affected side. All 15 patients had returned to their preinjury occupations. The mean Achilles Tendon Total Rupture Score at the time of the latest follow-up was 90.1 ± 5.8.
On the basis of the overall positive results demonstrated in several case series, a Grade B recommendation is indicated for the use of autograft reconstruction of chronic AT ruptures.
Summary
For patients who wish to return to preinjury activity, operative treatment is often preferred for chronic AT rupture.
Various operative treatments exist for repair of chronic AT ruptures, and defect size between the proximal and distal healthy tendon stumps is a general guide to the appropriate option(s) for any particular patient.
The current literature on surgical management options for chronic AT ruptures is limited primarily to Level IV studies and case reports. The highest grade of recommendation for any one of these techniques is a Grade B recommendation for the use of autograft reconstruction of the AT or a tendon transfer using FHL or peroneus brevis tendon.
Patient factors and surgeon experience with techniques are important considerations when considering surgical intervention for these injuries.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.