
Abstract
Background:
The minimally invasive chevron-Akin (MICA) technique has already demonstrated efficacy compared with other known surgical treatments for mild to moderate hallux valgus (HV). MICA combines percutaneous osteotomies with the benefits of modern, rigid internal fixation. The aim of study was to evaluate the radiographic parameters, clinical improvement, and potential complications in moderate to severe HV cases, operated using the MICA technique.
Methods:
Retrospective study including 70 feet with HV operated using the MICA technique. The AOFAS hallux MTP-IP score and radiographics for HV evaluation were applied preoperatively, and after 6 months, 1 year, and 2 years of follow-up. The following radiographic parameters were measured: metatarsophalangeal hallux valgus angle (HVA), distal metatarsal articular angle (DMAA), interphalangeal angle (IPA), and intermetatarsal angle (IMA).
Results:
The average preoperative VAS pain score was 8.2 ± 1.5, which improved to 1.2 ± 2.2 at 24 months. The mean preoperative IMA was 14.8 ± 3.6 degrees compared with a mean of 7.5 ± 2.1 degrees (P < .01) at 24 months. The preoperative HVA value averaged 30.4 ± 9.8 degrees and at 6 months postoperatively 11.1 ± 6.8 degrees (P < .01), which remained stable until measured at 24 months. The mean preoperative DMAA was 16.3 ± 8.6 degrees and at the 6-month follow-up was 7.8 ± 5.4 degrees (P < .01). The mean preoperative IPA was 7.63 ± 4.4 degrees compared with a mean of 6.28 ± 3.5 degrees (P > .05) at 24 months. Complications included painful hardware (14.28%), neuropathic pain (2.85%), and loss of correction (4.28%).
Conclusion:
In this retrospective review from a single center, we found the MICA technique to be an effective procedure for correcting moderate to severe HV, with a low rate of recurrence and an acceptable rate of complications. Patients undergoing the surgical procedure in our series showed a significant reduction in radiographic parameters and a significant improvement in clinical scores, maintaining these results over time.
Level of Evidence:
Level IV, retrospective study.
Introduction
There is growing interest in the use of minimally invasive surgical techniques (MIS) for the treatment of hallux valgus (HV), with an increasing number of published studies including clinical series, radiologic validations, cadaveric studies, comparative studies, and technical reports on MIS techniques.1,4,8-10,15-21,23,26-36,39-43,45,55,59-64,66,70 Five recent systematic reviews concluded that MIS is a safe and reliable technique for hallux valgus correction.6,11,28,44,65
Among the procedures to treat HV, the distal chevron metatarsal osteotomy was first described in 1962 and remains a widely accepted technique. It is indicated in the treatment of mild and moderate HV deformities, with satisfactory results in adult individuals of all age groups.2,3,9,58
In 2011, Vernois and Redfern described the minimally invasive chevron-Akin (MICA). This technique combines percutaneous osteotomies with the benefits of modern rigid internal fixation. 67 In addition, it minimizes soft tissue and vascular disruption while allowing a lateral translation of the metatarsal head to nearly 100%. This is possible by maintaining only the medial cortical contact of the head with the lateral cortex of the metadiaphyseal region (Figure 1). This procedure can be indicated for symptomatic mild to moderate HV deformity, and with experience, severe deformity corrections can be corrected using nearly 100% displacement of the osteotomy.54,55,67

Intraoperative image of the first metatarsal showing the contact of the medial cortex of the head with the lateral cortex of the metaphyseal region.
The objective of the present study is to evaluate the radiographic parameters, clinical improvement, and potential complications in cases of moderate and severe hallux valgus operated on at our institution using the MICA technique. We hypothesized that the MICA technique would be able to maintain clinical and radiographic improvement in a minimum 2-year follow-up.
Materials and Methods
Patient Demographic Data
Between January 2017 and December 2020, a total of 47 consecutive patients (39 females and 8 males) with a mean age of 55.9 years (range, 21-77 years; SD, 13 years) underwent primary MICA. All patients in this retrospective study were treated by 2 fellowship-trained foot and ankle orthopaedic surgeons with > 7 years of experience at an academic institution. A total of 70 feet (59 females and 11 males) were treated. Twenty-four patients underwent simultaneous bilateral corrections. 12.9% of the patients were smokers and 21.4% had diabetes. The minimum follow-up was 24 months (average of 31.6 months and maximum of 42.3 months).
Study Design
This study is a single-center, retrospective study that included patients with moderate to severe HV defined as an intermetatarsal angle (IMA) of 15 to 20 degrees and/or hallux valgus angle (HVA) of 21 to 40 degrees for moderate HV and, severe deformity corresponds to an HVA >40 degrees and/or an IMA >20 degrees, who underwent surgical correction using the MICA technique. The standard radiographic cutoff was HVA <15 degrees and an IMA <9 degrees.36,38,49,56
The indications for surgery were painful HV with failed conservative management. The exclusion criteria were rheumatoid arthritis, severe vascular disorders, neuromuscular disease, and patients with recurrent HV after prior surgery.
The study was designed and conducted in accordance with the Declaration of Helsinki and the Guidelines on Good Clinical Practice.24,69 The Research Ethics Platform approved the study protocol and written informed consent was obtained from all patients prior to the study. Power analysis and necessary sample size computation were performed using G*Power 3.1.9.
The sample size calculation was based on the American Orthopaedic Foot & Ankle Society (AOFAS) hallux metatarsophalangeal-interphalangeal (MTP-IP) questionnaire. The following assumptions were made: difference between comparisons of 5 points with an SD of 10.5. In addition, the following statistical parameters were used: normal distribution, type I error (alpha) of 0.05, bilateral test, and type II error (beta) of 0.2. Thus, to obtain the 0.8 power, it was necessary to include 70 cases in this study.
The AOFAS hallux MTP-IP score for HV evaluation and weightbearing anterior to posterior radiographic views were obtained in each case, preoperatively, after a follow-up period of 6 months, after 1 year of follow-up and after 2 years of follow-up, and visual analog scale (VAS) was applied preoperatively, after 1 year of follow-up and after 2 years of follow-up. Preoperative and postoperative VAS measurements were used to assess pain, ranging from 0 to 10 points (with 0 indicating no pain and 10 denoting disabling pain by the procedure performed).
The following radiographic parameters were measured: intermetatarsal angle (IMA) between the first and second metatarsals, metatarsophalangeal HVA, distal metatarsal articular angle (DMAA), and interphalangeal angle (IPA). All radiographic parameters were measured by 2 fellowship-trained orthopaedic foot and ankle surgeons with >7 years of experience.
Interrater reliabilities for continuous data were performed using interclass correlation coefficients.
All complications defined as any deviation from the normal postoperative course (using the Clavien-Dindo Classification of Surgical Complications) were reported descriptively along with the respective form of treatment. 14 We analyzed whether complications had any interference in the AOFAS hallux MTP-IP score and radiographic outcome.
For inferential analysis, the distribution of continuous data was tested by the Shapiro-Wilk test and the distribution was not symmetric. To compare the measurements over time, the test for paired samples, Friedman test was used, and when appropriate, multiple pair tests were performed with Bonferroni correction. The value of P <.05 was considered to be statistically significant.
Surgical Technique
The surgical technique adopted was modified from the MICA procedure as described by Joel Vernois and David Redfern (Figure 2). 55
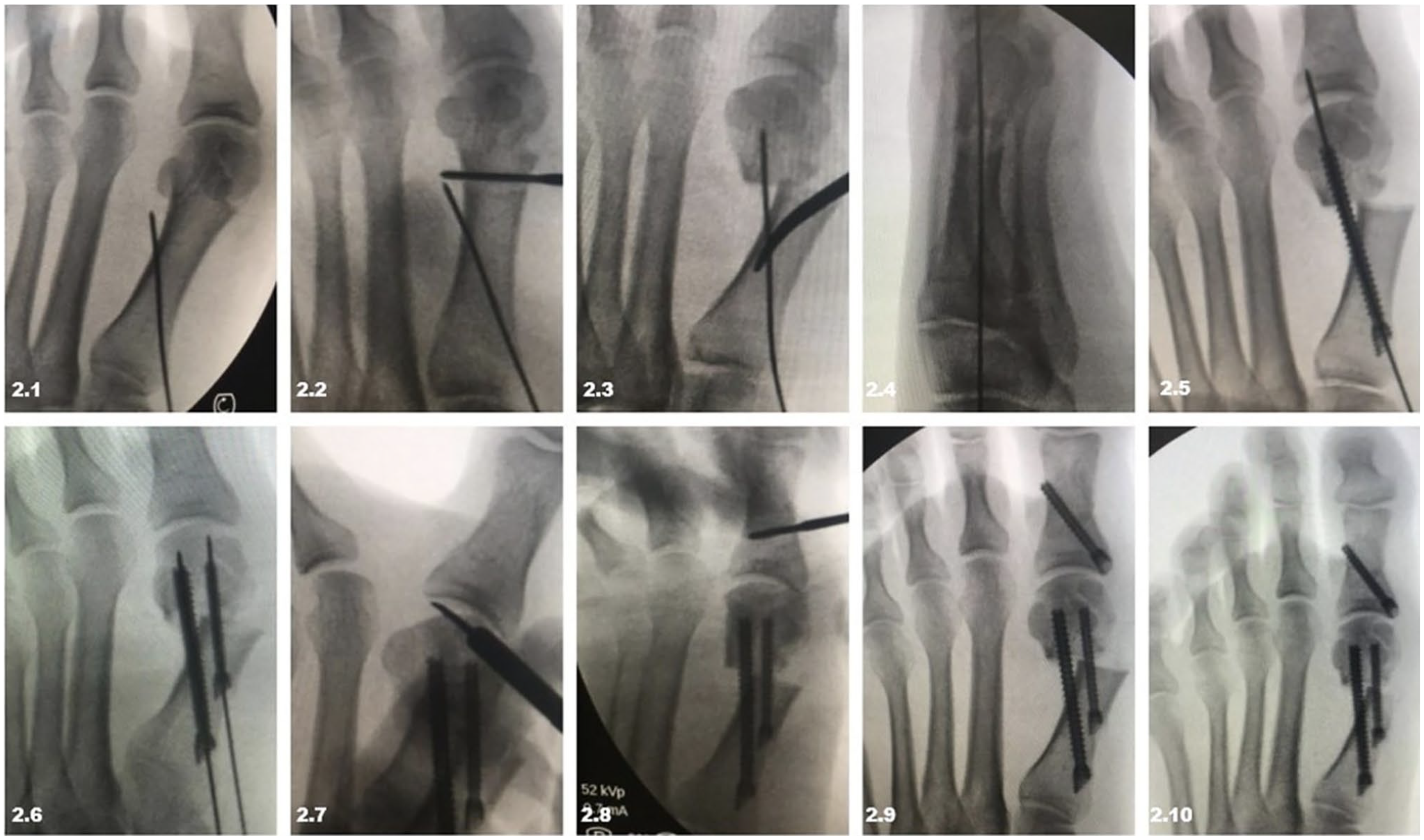
Intraoperative sequence showing surgical technique: (2.1) positioning of the first guidewire, (2.2) insertion of the Shannon burr and chevron osteotomy, (2.3, 2.4) displacement of the metatarsal head and fixation with the first guidewire, (2.5, 2.6) fixation with the first and second screw, (2.7) hallux abductor tenotomy, (2.8-9) Akin osteotomy and fixation with screw, and (2.10) final appearance.
The appropriate instrumentation for MIS was used in the surgical procedure. Burrs attached to Implant Micromotor System (SurgicPro Model, NSK/Nakanishi, Japan) with speed governor (300-500 rpm, minimum torque 50-80 Ncm) and continuous saline irrigation were used to cut the bone.39,55 Exostectomies were performed with 12×3.1-mm Wedge burrs, the chevron osteotomies were performed with 20×2-mm Shannon burrs. Akin osteotomies were performed with 12×2-mm Shannon burrs. Osteotomies were fixated using cannulated 3.0-mm threaded screws or with 4.0-mm headless screws with double compression.
Percutaneous tenotomy of the hallux adductor and lateral capsulotomy of the metatarsophalangeal joint were performed in cases of severe deformity when soft tissue contracture and limited passive reduction of the hallux valgus deformity persisted after the metatarsal osteotomy was fixated (Figure 2.7).
An Akin osteotomy was routinely performed using the Vernois and Redfern technique (Figure 2.8 and 2.9). 55
Lastly, the medial spike of bone at the metatarsal remaining after the shift was resected using the 2×12-mm burr. Final fluoroscopic images were then obtained (Figure 2.10).
In the postoperative period, immediate full weightbearing was permitted with the use of a hard-soled orthopaedic shoe; this protection was maintained for 6 weeks. After the initial 6 weeks, patients were released from shoe wear restrictions and were instructed to return to the use of conventional footwear.
Results
Clinical Results
Preoperative VAS scores averaged 8.24 ± 1.51 in the preoperative period and decreased to 1.37 ± 2.27 after 1 year and to 1.19 ± 2.23 after 2 years (P < .01) (Table 1).
Descriptive Statistics of the Studied Population.
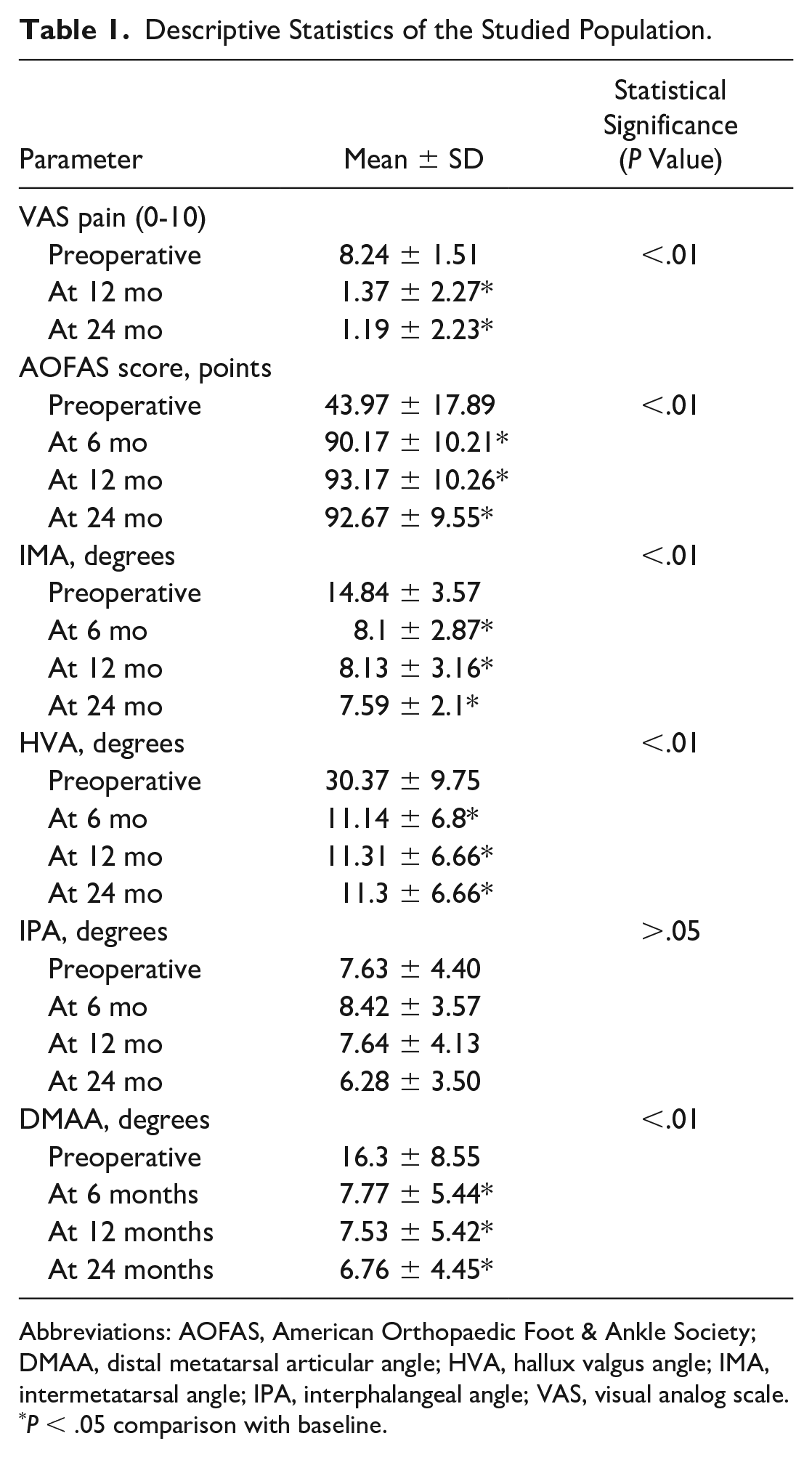
Abbreviations: AOFAS, American Orthopaedic Foot & Ankle Society; DMAA, distal metatarsal articular angle; HVA, hallux valgus angle; IMA, intermetatarsal angle; IPA, interphalangeal angle; VAS, visual analog scale.
P < .05 comparison with baseline.
When we compared the evolution of the VAS score separately for moderate and severe cases, we found that the preoperative VAS for moderate patients was 8.9 ± 6.32, higher than the severe group, which was 8.61 ± 1.64. This difference did not achieve statistical significance (P = .072). When comparing the VAS score changes over time during the 12-month postoperative period, the moderate group improved to 2.71 ± 4.65 whereas the severe group improved to 2.75 ± 3.07; this does demonstrate a statistically significant difference between the groups (P = .002). A similar pattern is seen when comparing scores at 24 months, where the VAS score is 2.57 ± 4.64 for moderate cases and 2.32 ± 2.84 for severe cases (P = .003) (Table 2).
Impact of Severity and Complications on the VAS pain, AOFAS Score, IMA, HVA, DMAA, and Their Persistence Over Time.
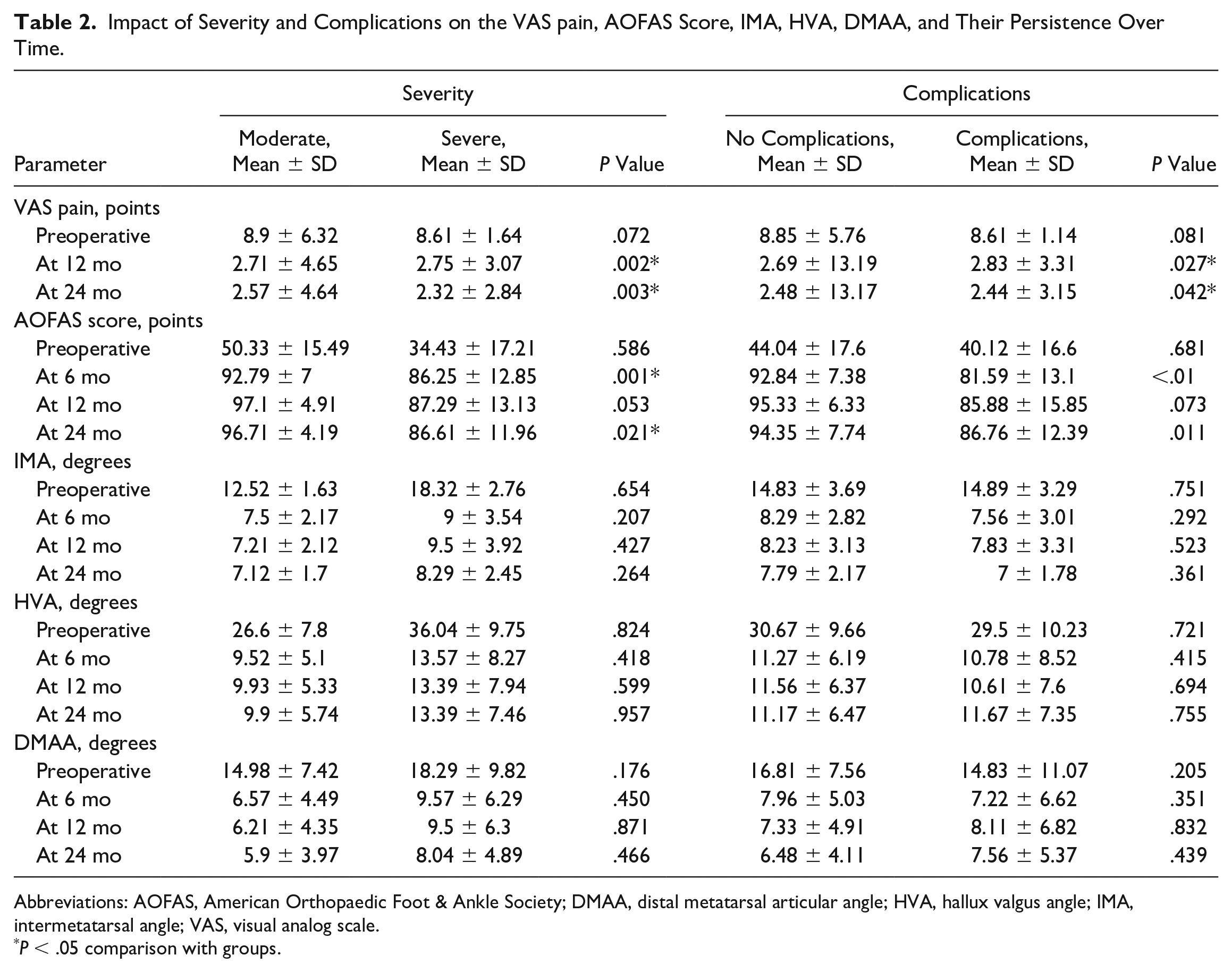
Abbreviations: AOFAS, American Orthopaedic Foot & Ankle Society; DMAA, distal metatarsal articular angle; HVA, hallux valgus angle; IMA, intermetatarsal angle; VAS, visual analog scale.
P < .05 comparison with groups.
The average preoperative AOFAS hallux MTP-IP score was 43.97 ± 17.89 and demonstrated a positively satisfactory variation when compared to the AOFAS hallux MTP-IP score measured in the 6-month postoperative period, which was 90.17 ± 10.21 (P < .01). This score was maintained in subsequent postoperative periods of 12 and 24 months (Table 1, Figure 3).
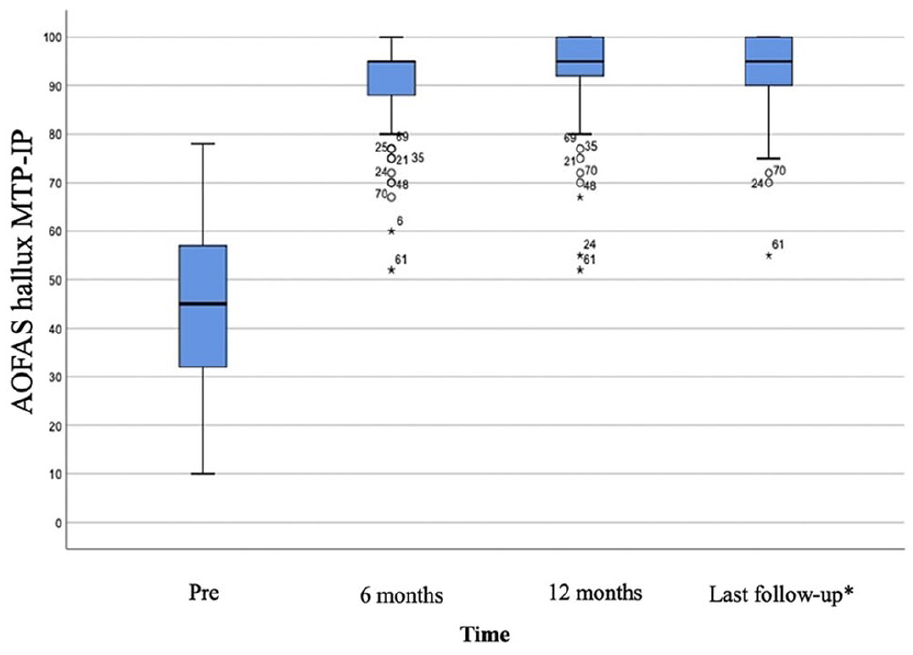
The AOFAS hallux MTP-IP score outcome over time. *Minimum of 24 months of follow-up.
When we compared the evolution of the AOFAS hallux MTP-IP score separately for moderate cases and for severe cases, we found that the preoperative AOFAS hallux MTP-IP for moderate patients was 50.33 ± 15.49, higher compared with the severe group, which was 34.43 ± 17.21, though this difference did not achieve statistical significance (P = .586). When comparing the AOFAS hallux MTP-IP score changes over time, however, at the 6-month postoperative period, the moderate group improved to 92.79 ± 7 whereas the severe group improved only to 86.25 ± 12.85; this does demonstrate a statistically significant difference between the groups (P < .01). A similar pattern is seen when comparing scores at 24 months, where the AOFAS hallux MTP-IP score is 96.71 ± 4.19 for moderate cases and 86.61 ± 11.96 for severe cases (P = .021) (Table 2, Figure 4).
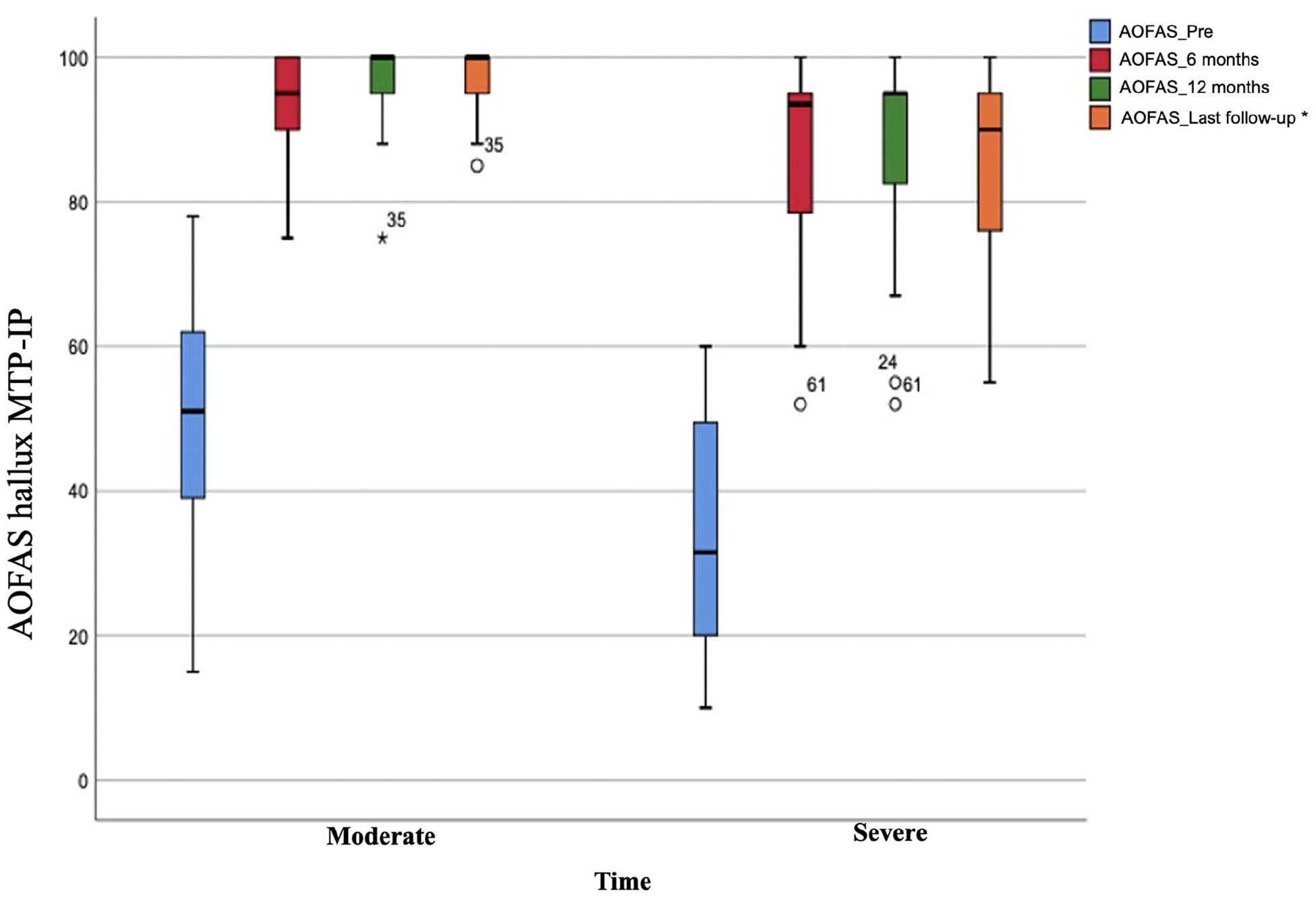
The impact of hallux valgus severity on AOFAS hallux MTP-IP score outcome over time. *Minimum of 24 months of follow-up.
Radiographic Results
Regarding the radiographic criteria for the severity of the cases, 42 feet (60%) were considered moderate and 28 feet (40%) severe.
All radiographic parameters were measured by 2 fellowship-trained orthopaedic foot and ankle surgeons with >7 years of experience. The deformities were measured preoperatively and then postoperatively (Table 1).
The intraobserver and interobserver agreement and consistency for measurements assessed by interclass correlation coefficient demonstrated excellent reliability for HVA, IMA, and IPA and proved good for DMAA (Table 3).
Intraobserver and Interobserver Agreement and Consistency Angles Measurements Assessed by ICC. a
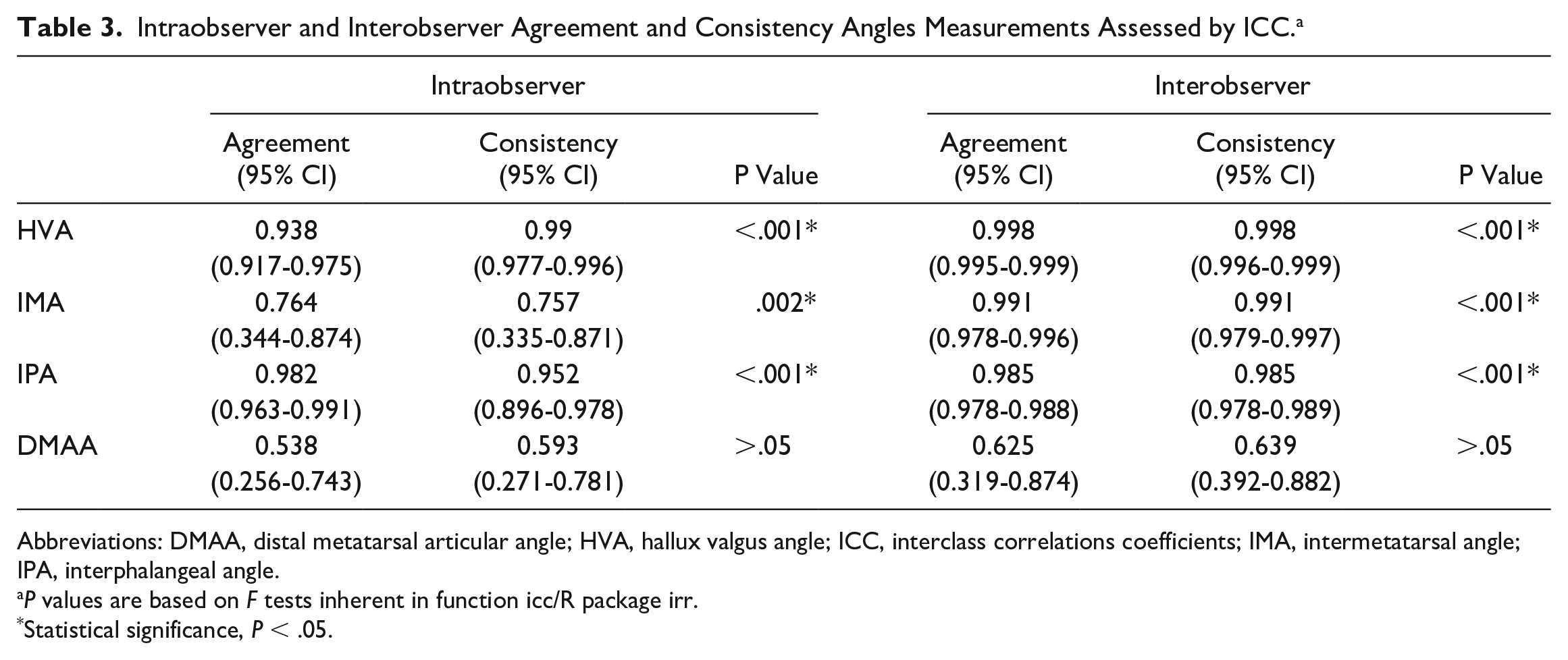
Abbreviations: DMAA, distal metatarsal articular angle; HVA, hallux valgus angle; ICC, interclass correlations coefficients; IMA, intermetatarsal angle; IPA, interphalangeal angle.
P values are based on F tests inherent in function icc/R package irr.
Statistical significance, P < .05.
The IMA initially presented a mean value of 14.84 ± 3.57 (range, 11-24) degrees. A significant decrease in this value was noted when the patient was reevaluated in the 6-month postoperative period, with a mean value of 8.1 ± 2.87 (range, 2-19) degrees (P < .01). In the period between the 6-month and 24-month postoperative evaluations, the values of the IMA continued to show a slight decrease in the mean values (P < .05) (Table 1, Figure 5A).
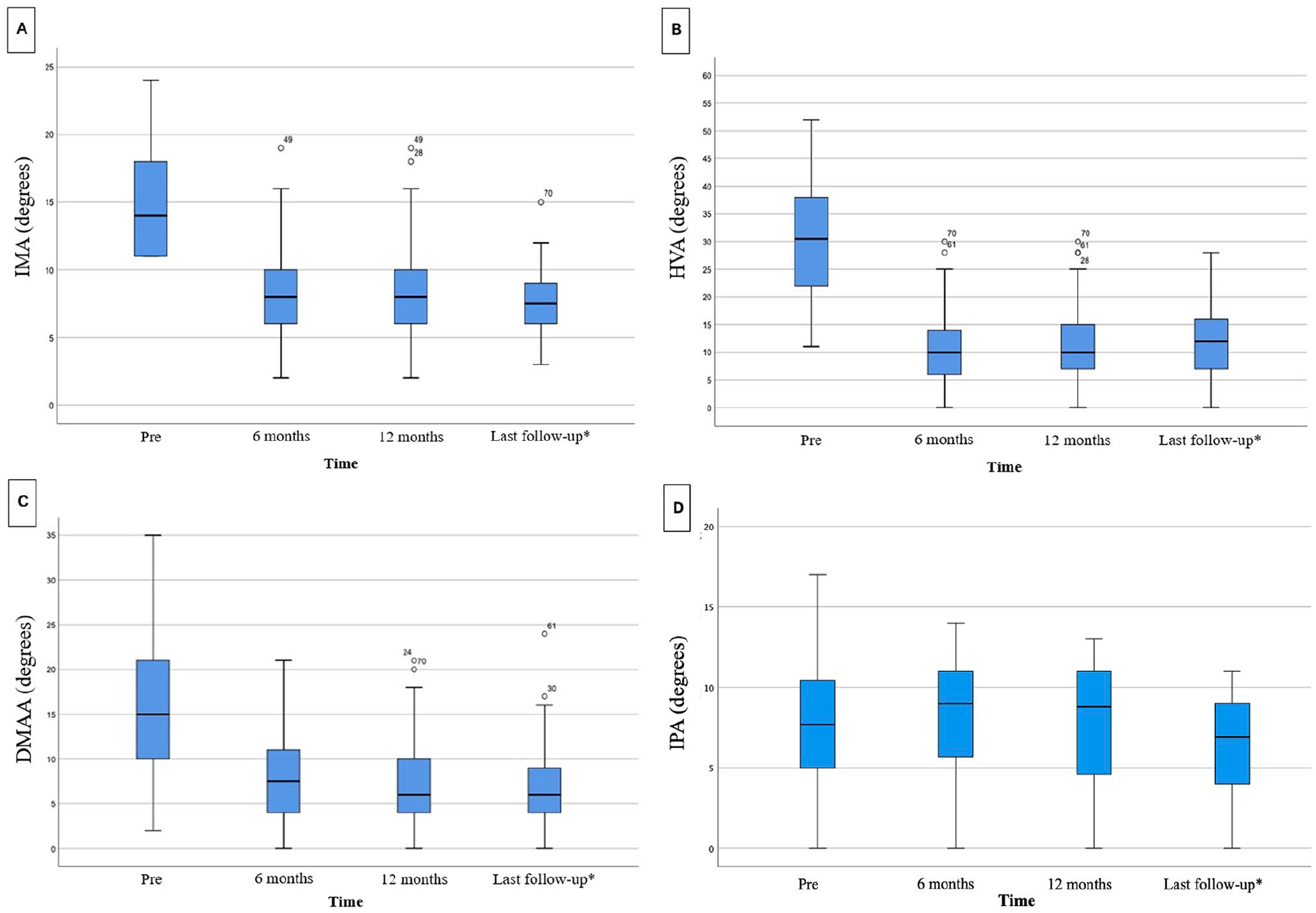
Impact of follow-up time on (A) intermetatarsal angle (IMA), (B) metatarsophalangeal hallux valgus angle (HVA), (C) distal metatarsal articular angle (DMAA), and (D) interphalangeal angle (IPA). *Minimum of 24 months of follow-up.
The HVA showed a mean value of 30.37 ± 9.75 (range, 11-52) degrees preoperatively followed by a mean value of 11.14 ± 6.8 (range, 0-30) degrees (P < .01) at 6 months postoperatively, remaining stable in the postoperative evaluations at 12 and 24 months (Table 1, Figure 5B).
The DMAA started with a mean of 16.3 ± 8.55 (range, 2-47) degrees preoperatively and presented a significant drop (P < .01) in the 6-month assessment, with a mean of 7.77 ± 5.44 (range, 0-21) degrees. Like the IMA, the DMMA continued to show decreased values until the 24-month evaluation (P < .05) (Table 1, Figure 5C). The IPA showed a mean value of 7.63 ± 4.40 (range, 0-17) degrees preoperatively followed by a mean value of 6.28 ± 3.50 (range, 0-11) degrees (P > .05) at 24 months postoperatively (Table 1, Figure 5D).
Over the 2 years of follow-up, the radiographic improvement did not change. The 6-month radiographic data were not significantly different compared to the 24-month data.
When comparing the radiographic evolution separately for moderate and severe cases (Figure 6) or when comparing the radiographic evolution with complications (Table 2), we noticed that both severity and the presence of complications did not influence the outcome at the end of 2 years of follow-up.
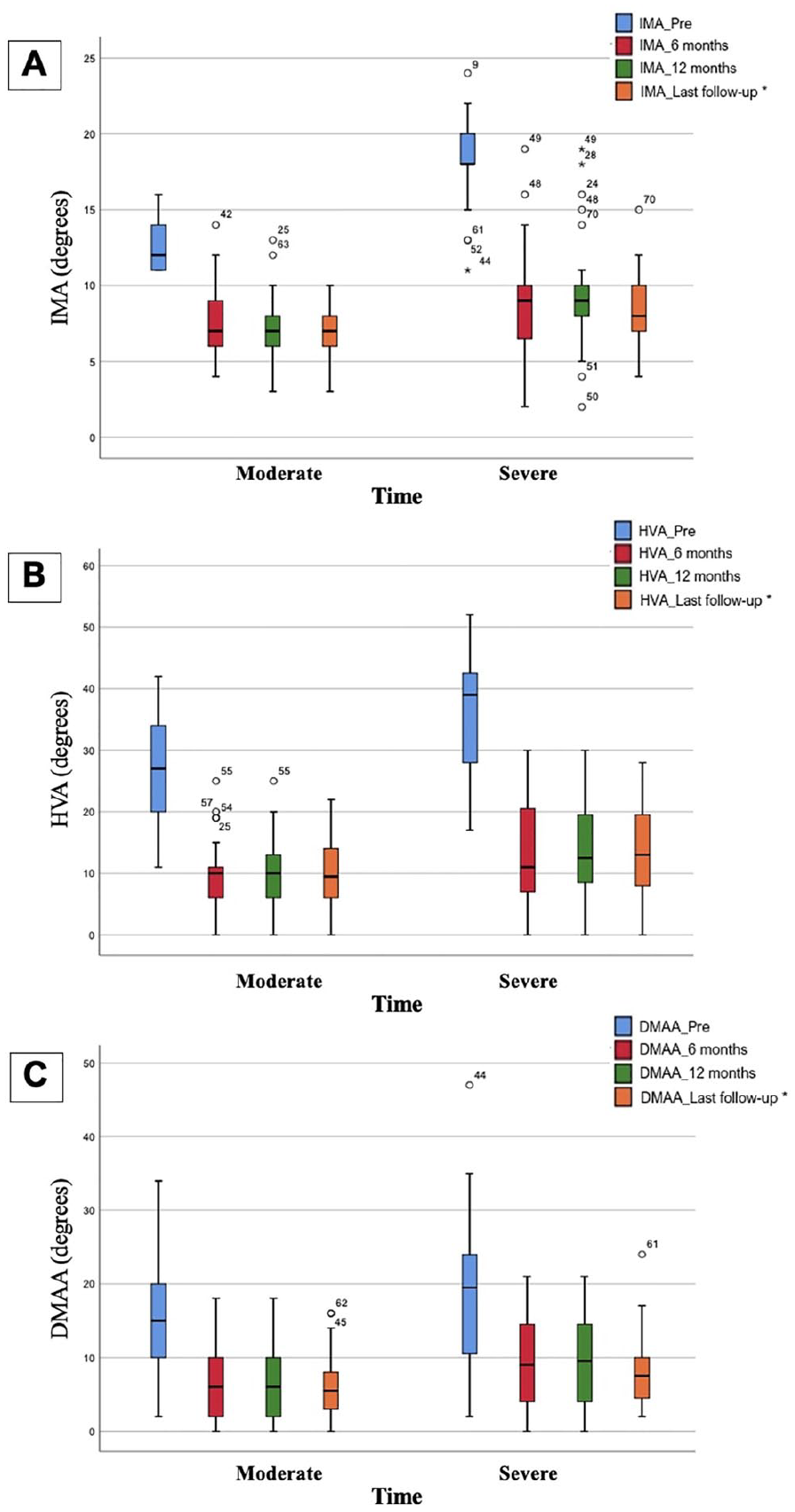
The Impact of HV severity on (A) intermetatarsal angle (IMA), (B) metatarsophalangeal hallux valgus angle (HVA), and (C) distal metatarsal articular angle (DMAA) outcome over time. *Minimum of 24 months of follow-up.
Complications
Complications included painful hardware, irritation of the dorsomedial digital nerve, and loss of correction. Pain due to prominent hardware at the screw heads in the first metatarsal occurred in 14.28% of the cases (10 feet; 9 feet with nonbeveled screw vs 1 foot with beveled) (47 patients had conventional headless screws and 23 patients had headless beveled screws). In all cases, screw removal (Grade III-a) resulted in complete resolution of pain. Hardware pain complaints were eliminated when we switched to using bevel screws instead of head screws; however, there was no significant difference between the groups (P = .392). Moderate nerve-related symptoms occurred in 2 cases (2.85%) in the territory of the dorsomedial digital nerve. These patients were treated with pregabalin 75 mg, 1 capsule, every 12 hours, for 3 months with resolution of symptoms after 3 months (Grade II). In 1 case (1.42%), 1 screw in the first metatarsal broke without loss of alignment or migration of the screw (Grade I). Significant loss of alignment in the chevron osteotomy occurred in 3 (4.28%) severe cases (HVA > 40), and 2 of these cases required revision surgical fixation (Grade III-a). Finally, in a single case (1.42%), the lateral screw migrated distally in the metatarsal head, but the patient remains asymptomatic without pain or motion restriction (Grade I) at 32 months postoperatively (Figure 7.5 and 7.6). The comparative analysis showed that patients with complications had a less favorable positive evolution of the AOFAS hallux MTP-IP outcome compared to those who had no complications at the 6- and 24-month follow-up (P < .05). Complications did not influence the radiographic outcome for the IMA, HVA, and DMAA over time (P > .05) (Table 2).

Outcome sequence showing surgical complications: (7.1-7.3) clinical follow-up images pre-, intra-, and postoperation at 36 months, respectively; (7.4) radiographic images preoperation; (7.5) radiographic images intraoperation with initial screw position (yellow balloon); (7.6) radiographic images postoperation At 36 months with migration from screw to proximal (yellow balloon) and screw model initially used with wide head that caused discomfort in patients (green balloon). [See online article for color figure.]
Discussion
We performed a retrospective study to evaluate radiographic parameters, clinical improvement, and potential complications in cases of moderate and severe hallux valgus operated by the MICA technique. Both cases showed significant improvement in clinical and radiographic parameters, maintaining them throughout the 2 years of follow-up. The most prevalent complication was pain around the hardware in the region of the screw head in the first metatarsal. These complications influenced the clinical results but did not influence the radiographic result.
Interest in minimally invasive HV surgery among foot and ankle surgeons is rapidly increasing. However, there remain concerns regarding the information provided by the available publications, although there has recently been an increase in the level of evidence presented.
Despite the growing number of studies on MIS, one of the criticisms of the studies is that they rarely talk in detail about the complications that have occurred. Our study tried to identify the complications that occurred and discuss their impact and how they were treated.
Clinical Outcomes
In our study, we found that the MICA technique showed a significant improvement in the clinical parameters measured. These advances were identified by the first 6 months postoperative and remained stable throughout the remainder of the follow-up for a minimum of 24 months. Ferreira et al, 22 in a recent systematic review and meta-analysis comparing the open technique with the MICA technique, demonstrated a similar pattern of pain and function between the open and percutaneous techniques after a 6-month follow-up. However, the authors highlighted that the short follow-up time of the studies might influence the risk of bias and lead to erroneous conclusions. 22 Few studies have been able to report on clinical outcomes using the MICA technique with a follow-up of more than 24 months.12,37,38
We present similar results regarding the AOFAS hallux MTP-IP and VAS scores to the studies carried out by Nunes et al 52 in a recent study with 25 patients with a mean follow-up of 14.6 months, Chan et al 12 with a series of cases of 13 feet but with an average follow-up of 48 months. and Holme et al 25 in a study with 40 patients and a 12-month follow-up.
However, in our sample of patients with moderate and severe deformity, we further delineated our results and compared the evolution of the VAS score and AOFAS hallux MTP-IP score separately for moderate cases and for severe cases.
The VAS score showed a positive evolution over time for both moderate and severe cases, and we observed that the severity of the cases influenced the final result VAS score. When the cases were compared, there was a difference in the final VAS outcome at 12 months and at 24 months (P < .05).
The difference in the AOFAS hallux MTP-IP scores in moderate cases compared with severe cases is not unexpected. A lower initial score in more severe cases is likely related to several factors including greater severity of the deformity, greater pain, presence of articular stiffness, and the presence of plantar calluses, among other factors. The lower postoperative scores may be related to the lesser degree of angular improvement compared with moderate cases secondary to the limitations of the correction, sesamoid and metatarsal phalangeal joint degeneration, and soft tissue contractures.
We did not find studies in the literature evaluating clinical results for the MICA technique using VAS and AOFAS hallux MTP-IP scores over time in moderate and severe cases. Mikhail et al, 46 in a study with 248 patients who underwent the MICA technique with a mean follow-up time of 12.9 months (range, 6-30 months), used the Foot Function Index (FFI) part A (pain) to follow postoperative outcomes. They found a significant improvement in patients postoperatively (FFI score 18) compared to preoperatively (FFI score 48). Biz et al 7 published a recent study using a different technique, the Minimally Invasive Intramedullary Nail Device (MIIND), to correct moderate and severe hallux valgus, and demonstrated similar results in the evolution of the AOFAS hallux MTP-IP score over time. Our clinical results compared positively with previous studies in the literature in the initial postoperative scores and show that good results are maintained in the long term when compared to studies with long follow-up.7,12,25,37,52,63
Radiologic Outcomes
One of the major criticisms of previous studies that aim to deal with the MICA technique is that most studies refer only to the radiographic evolution of IMA and HVA, not measuring and evaluating the evolution of DMAA and IPA. Our study performed a complete radiographic evaluation of these angles, adding information that to our knowledge has not been reported previously.
In our study, intraobserver and interobserver agreement and consistency for HVA, IMA, and IPA demonstrated excellent reliability, similar to the results found by Chi et al 13 for HVA and IMA, and to the results found by Khademi et al 32 for IPA. We found good intraobserver and interobserver reliability for DMAA, different from the results presented by Vittetoe et al, 68 who obtained excellent intraobserver reliability and poor interobserver reliability, and the results presented by Lalevée et al, 34 who obtained excellent intraobserver and interobserver reliability.
We presented an average correction of 7.25 degrees for the IMA, 19.07 degrees for the HVA, 9.54 degrees of correction for the DMAA, and 1.35 degrees of correction for the IPA. Similar results were found by Miranda et al 47 in a recent systematic review. The mean values of preoperative IMA and HVA and correction of postoperative deformity in this study were comparable to studies carried out in other studies (Table 4).7,10,23,25,29,41,46,50,52
Radiographic Outcomes (Minimum 12 Months) From Other Studies Investigating Third-Generation Minimally Invasive Osteotomies for Hallux Valgus Correction.
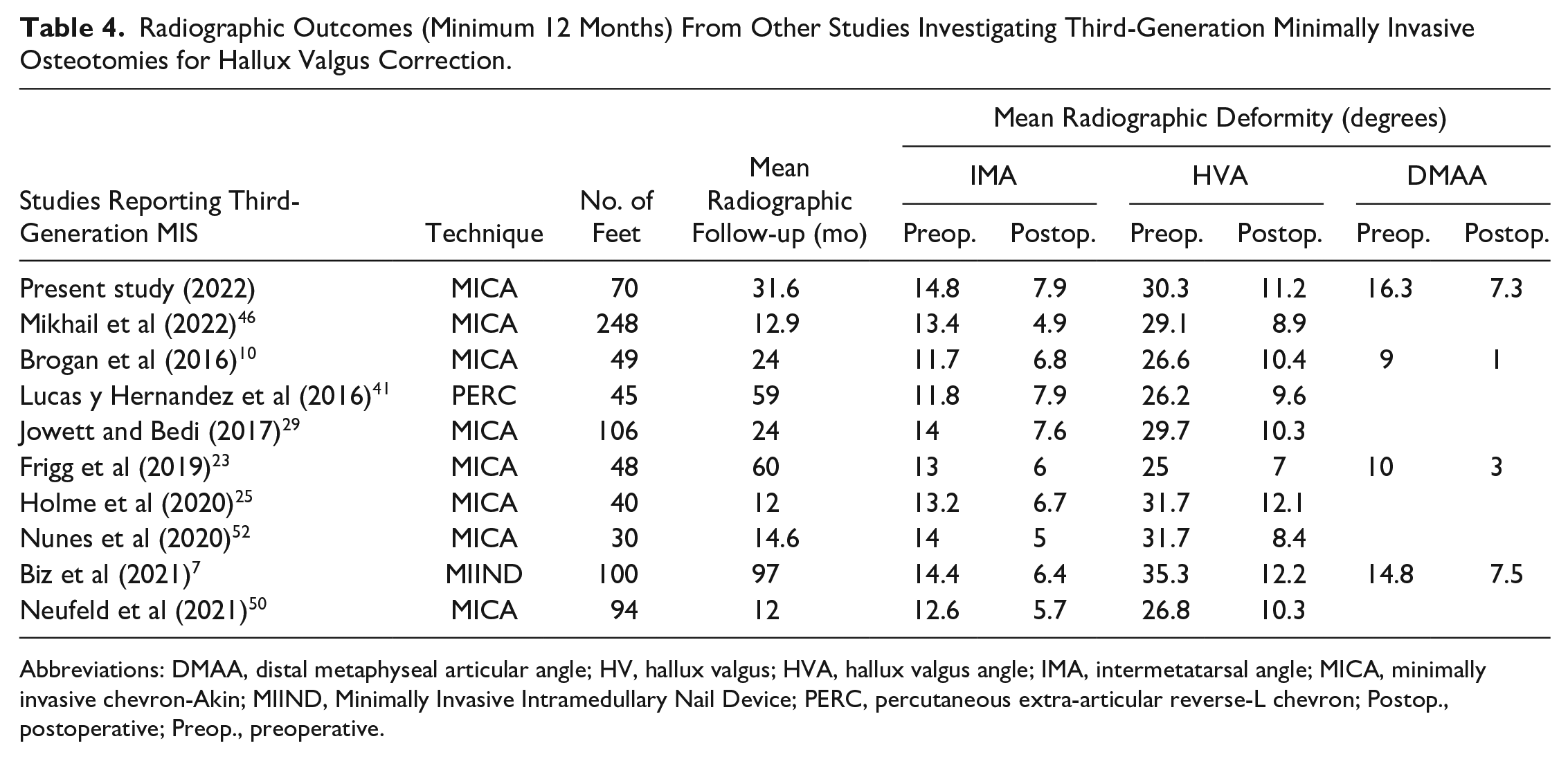
Abbreviations: DMAA, distal metaphyseal articular angle; HV, hallux valgus; HVA, hallux valgus angle; IMA, intermetatarsal angle; MICA, minimally invasive chevron-Akin; MIIND, Minimally Invasive Intramedullary Nail Device; PERC, percutaneous extra-articular reverse-L chevron; Postop., postoperative; Preop., preoperative.
Although other studies evaluating the radiographic correction using the MICA technique only followed patients for 6 months at most, our study presents a minimum radiographic follow-up of 24 months, and in some cases 42 months. Over time, both moderate and severe cases maintained similar radiographic corrections (P < .01) (Tables 1 and 2, Figure 6).
In our series, we presented 28 severe cases (HVA >40 degrees and/or IMA >16 degrees) and obtained similar results (IMA: preoperative 18.2; postoperative 8.2 and HVA: preoperative 36.1; postoperative 13.4) to Lewis et al. In their recent study of 50 patients with severe HV undergoing the MICA technique, patients demonstrated improvement (P < .001) in both IMA (preoperative 17.5; postoperative 5.1) and HVA (preoperative 44.1; postoperative 11.5) after surgery. 38
DMAA is recognized as an indicator of surface lateralization of the first metatarsal joint. We know that when we measure DMAA, we do not necessarily measure where the cartilage edges are and that a change in rotation can affect the appearance of plain radiographs. We are unaware of a study that has evaluated the possible causes of the decrease in DMAA after percutaneous chevron osteotomy. Unlike the biplanar chevron osteotomy, where we have a medialization of the surface of the first metatarsal joint with a consequent natural decrease in DMAA, in the percutaneous chevron osteotomy, the lateralization of the head of the first metatarsal occurs without medialization of the articular surface. 48 However, this decrease in DMAA could be explained by the change in the anatomical axis of the first metatarsal preoperatively to the mechanical axis of the postoperative period. 61 This change in the first metatarsal axis, despite not generating a change in the position of the surface of the first metatarsal joint, creates a smaller angular measurement and, potentially will alter accurate measurement of the DMAA.
In our study, the vast majority of patients had normal IPA (<10 degrees). Although they underwent Akin’s osteotomy for hallux valgus correction, we did not find a significant decrease between the pre- and postoperative periods. Although not yet discussed in the literature, we can infer the low power of correction of isolated percutaneous Akin osteotomy with a 2-mm burr, since, according to a study by Nguyen et al, 51 we need to remove a 3-mm wedge in the Akin osteotomy to obtain a 10-degree correction of the interphalangeal angle.
Complications
Complications in surgeries that use minimally invasive techniques are often associated with a significant learning curve. The percutaneous technique requires a different skill set than surgeons are typically exposed to during their early training.5,33 In centers where minimally invasive surgery is performed exclusively, the learning process can occur relatively quickly and efficiently, after performing 20 to 50 cases.5,33,47,53 In a study that evaluated the learning curve, Jowett et al 29 reported a 40% complication rate in a subgroup with the first 60 procedures performed by the author during the learning curve and obtained a 26% complication rate when evaluating the learning procedures from 61 to 120, performed by the same author. In our study, we presented a total rate of complications of 24.2% (Table 5). If we remove the prominent hardware requiring removal, the complication rate is 10%. Based on the studies above, we can infer that with 70 cases we were within the field of the learning curve.
Complications and Screw-Removal Rates From Other Studies Investigating Third-Generation Minimally Invasive Osteotomies for Hallux Valgus Correction
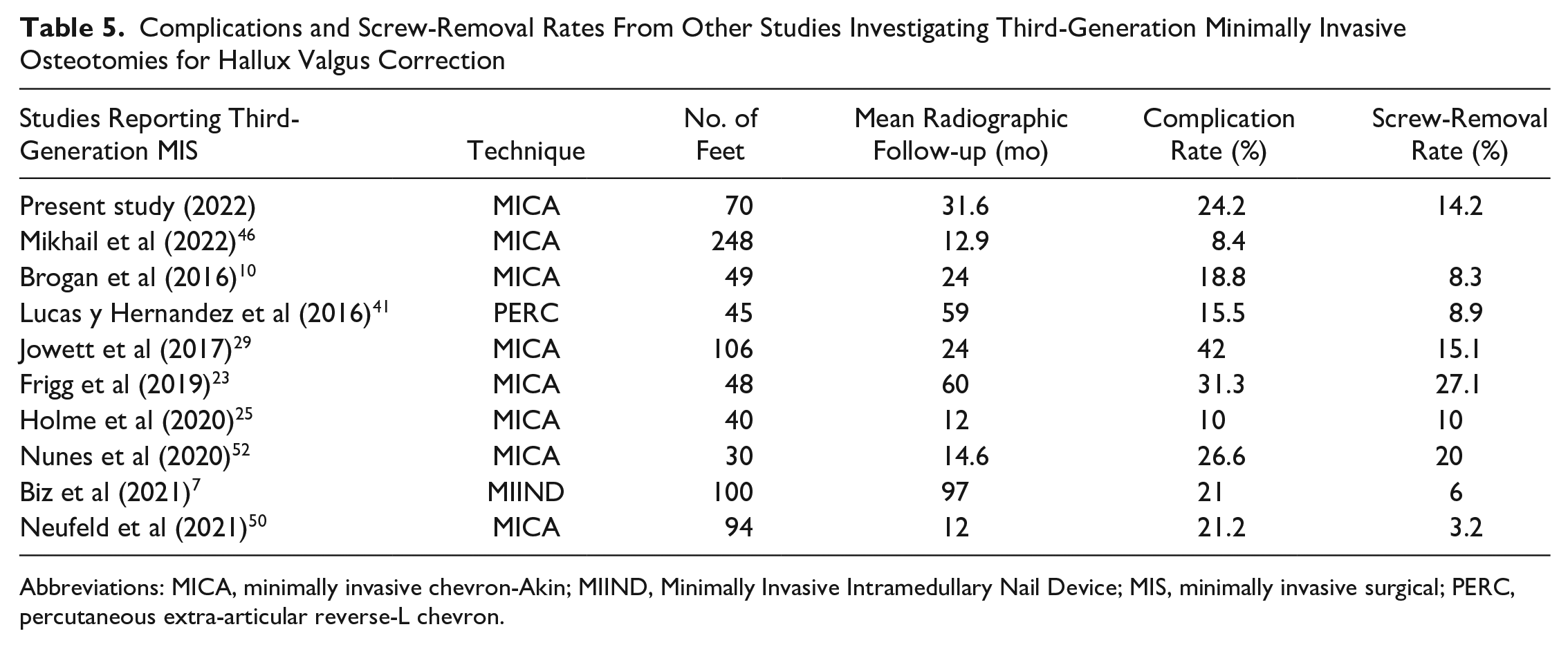
Abbreviations: MICA, minimally invasive chevron-Akin; MIIND, Minimally Invasive Intramedullary Nail Device; MIS, minimally invasive surgical; PERC, percutaneous extra-articular reverse-L chevron.
In our study, the most prevalent complication was pain around the hardware in the region of the head of the screws in the first metatarsal (Figure 7) when wearing shoes. In 14.28% of the cases (10 feet), it was necessary to remove the painful screws in the first 6 months after surgery, with complete resolution of pain after the removal procedure. This same type of complication was reported by Nunes et al 52 and Robinson and Lam. 57 with removal of the painful hardware allowing complete improvement of the clinical condition.
In our cases, we observed that hardware pain complaints were eliminated when we changed to beveled screw heads. These screws sit flush against the bone (Figure 2), reducing the likelihood of irritation of the soft tissues and allowing the surgeon to verify proper screw position against the medial cortex using intraoperative fluoroscopy.25,52,55,57
Moderate neuropathic pain was seen in 2 cases (2.85%) but resolved by 3 months with oral pregabalin treatment. The medication was discontinued once the pain resolved. This complication is similar to that found in the literature. 52
We presented 3 cases (4.28%) of loss of reduction at the chevron osteotomy, and in 2 of these cases there was a need for surgical revision, a similar rate when compared with minimally invasive osteotomies of the third-generation minimally invasive techniques reported.7,29
Finally, we did not present any cases of skin infection, osteomyelitis, pseudoarthrosis, or osteonecrosis of the metatarsal head as previously reported in the literature.
Strengths and Weaknesses
The major weakness of this study is the lack of a comparable control group. In addition, we did not exclude cases where additional procedures, such as hammer toe corrections or metatarsal osteotomies, were performed. As our cohort included moderate to severe HV, these cases tend to have associated lesser toe deformities and concomitant procedures are commonly performed with HV correction. The radiographic parameters were measured by 2 fellowship-trained orthopaedic foot and ankle surgeons who participated in all surgeries, which could bias the results.
Conclusion
Our hypothesis that the MICA technique would be able to maintain clinical and radiographic improvement in a minimum follow-up of 2 years was confirmed. This study, unlike the previous ones, details more comprehensively the clinical and radiographic variables and the possible complications related to the MICA technique. The findings suggest that in our hands the MICA technique has been a relatively safe and effective procedure for correcting moderate to severe HV, with a low rate of recurrence and an acceptable rate of complications. In our series, the patients showed a significant improvement in clinical outcomes and showed significant improvement in radiographic parameters, maintaining these results over the follow-up period of this study. The minimum 2-year good results of this study justify the continued use of the technique and suggest the need to compare the outcomes prospectively with a matched open comparison group.
Supplemental Material
sj-pdf-1-fai-10.1177_10711007221114123 – Supplemental material for Minimally Invasive Chevron-Akin for Correction of Moderate and Severe Hallux Valgus Deformities: Clinical and Radiologic Outcomes With a Minimum 2-Year Follow-up
Supplemental material, sj-pdf-1-fai-10.1177_10711007221114123 for Minimally Invasive Chevron-Akin for Correction of Moderate and Severe Hallux Valgus Deformities: Clinical and Radiologic Outcomes With a Minimum 2-Year Follow-up by Kepler Alencar Mendes de Carvalho, Andre Donato Baptista, Cesar de Cesar Netto, Anne H. Johnson and Miki Dalmau-Pastor in Foot & Ankle International
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Anne H. Johnson, MD, reports Novastep: royalities and consulting fees, Patents planned, issued or pending. ICMJE forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.